HIV AND AIDS IN SPAIN, 2001
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
HIV AND AIDS
IN SPAIN, 2001
MINISTERIO
DE SANIDAD
Y CONSUMO
SUBSECRETARÍA DE
SANIDAD Y CONSUMO
MINISTERIO DIRECCIÓN GENERAL DE
DE SANIDAD SALUD PÚBLICA Y CONSUMO
Y CONSUMO
SECRETARÍA DEL PLAN
NACIONAL SOBRE EL SIDAHIV AND AIDS I N S PA I N , 2 0 0 1
Edited and distribuyed by: © MINISTERIO DE SANIDAD Y CONSUMO CENTRO DE PUBLICACIONES Paseo del Prado, 18. 28014 Madrid NIPO: 351-02-027-7 Depósito Legal: M-24045-2002 Printed: Rumagraf, S.A. Avda. Pedro Díez, 25. 28019 Madrid Printed in Spain O.T. 31484
HIV AND AIDS IN SPAIN, 2001 3 BACKGROUND Spain is a country in southern Europe with a population of about 40 million inhabitants. In the 1990s, it was the European country most heavily affected by the HIV/AIDS epidemic, but this situation has changed in recent years, as great progress has been made in controlling HIV transmission, and AIDS incidence and mortality rates have been substantially reduced. The epidemiological situation of HIV infection and AIDS in Spain at the start of the 21st century is the result of a process of over 20 years, which can be briefly summarized in three major events:1 The rapid spread of HIV during the 1980s. During this decade HIV infection spread widely among a large number of injecting drug users (IDUs)2,3 in Spain, making this mechanism of transmission responsible for more than two-thirds of cases. HIV also spread among homosexual men, although much less abruptly.4,5 The high number of HIV-infected IDUs, most of them sexually active young adults, led to secondary transmission of HIV by the heterosexual and perinatal route. At the start of the 1990s, more than 100,000 HIV infections had already occurred,6 and AIDS-related mortality ranked first among the major causes of potential years of life lost in Spain.8 The progressive control of HIV transmission since the beginning of the 1990s. The seriousness of the situation alerted society. New prevention programs were started and existing programs intensified, which helped to reduce risk practices. The number of young people in the next generations started intravenous drug use gradually decreased,9 resulting in a gradual aging of the IDU group. Added to this was a trend to replace the intravenous route of drug use by the inhaled or smoked route.9,10 These trends led to a marked reduction in the rate of occurrence of new HIV infections, as has been shown by serial studies of HIV seroprevalence in IDUs,11-12 homosexual men3,5 and women who engage in sex work.13-14 The spread of highly active antiretroviral therapies since 1997. By the mid-nineties, the highest point in the epidemic in terms of morbidity and mortality was reached, with more than 7,000 new AIDS diagnoses and more than 5,000 deaths annually.3 Since highly active antiretroviral therapies were introduced at the end of 1996, there has been a considerable improvement in the immune status and prognosis of HIV-infected persons.15 This resulted in a rapid reduction in AIDS incidence of over 60% in the next four years, and a decline in mortality of 67% in just two years.3
4 HIV AND AIDS IN SPAIN, 2001
STATUS OF THE EPIDEMIC IN SPAIN AT THE BEGINNING
OF THE 21ST CENTURY
• HIV TRANSMISSION Figure 1. Time trend of HIV diagnosis in several
European countries.
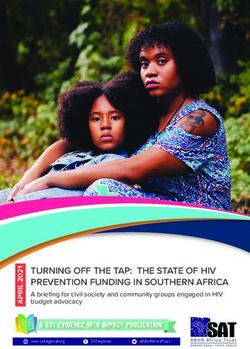
General trend
Diagnosis of HIV-infection per million
250 Spain*
The various sources of information Belgium
Germany
available agree in pointing out a steady 200 Ireland
decline in HIV transmission rates
inhabitants
Switzerland
in Spain over recent years.4-5,11-14 150 United Kingdom
However, the number of new HIV
100
diagnoses is still high, and the
possibility of new increases in 50
transmission rates cannot be ruled
out.16 In autonomous communities in 0
which epidemiological data on newly 1994 1995 1996 1997 1998 1999 2000 2001
diagnosed cases of HIV infection is Year
available, a reduction of over 70% has *Three regions.
been noted since the early 1990s.17
In spite of this large decrease, an overall total of 60 new HIV infections per million inhabitants were
diagnosed in these communities in 2001, a figure that is still very high in comparison with other
European countries (Figure 1).7
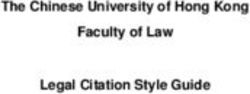
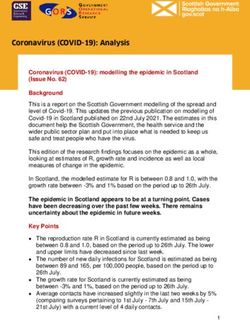
The risk of HIV infection is Figure 2. New diagnosis of HIV-infection, according
distributed very heterogeneously in to transmission category in three Spanish regions.
the population. In Spain, the
situations associated with the 800
highest risk of infection are, in order 700
Injecting drug users
Number of HIV diagnosis
of importance, parenteral drug use, 600
Sexual transmission
homosexual practices between men 500
and heterosexual contact with an 400
infected partner. In spite of this, 300
risky sexual relations have been the
200
leading cause of new infections in
100
recent years, which is explained by
the fact that it is the most 0
1986 1988 1990 1992 1994 1996 1998 2000
widespread exposure to risk in the
Year
population (Figure 2).18HIV AND AIDS IN SPAIN, 2001 5
Injecting drug users
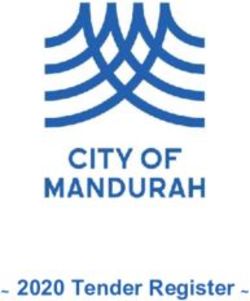
Large changes have occurred in this group over the years, which have led to a rapid and marked
reduction in the number of new HIV infections.9,11-12 Of these, the most important change has
been a steady decline in the number of youths starting intravenous drug use and, consequently, in
the risk of infection by this route.19-20 In parallel to this, some former IDUs, mostly heroin users,
have stopped consuming and many
others have switched either partly
Figure 3. Main route of drug administration among
or totally from the injected to the
persons first time attended for heroine or cocaine
inhaled route (Figure 3).21 This
dependence.
process has not occurred
simultaneously or with the same
80 Injected Smoked/inhaled Sniffed
intensity throughout Spain.10,21 The
70
risk of HIV infection continues to be
60
very high among persons who inject
Percentage
50
drugs, although various studies have
40
found moderate reductions in
30
prevalence (Figure 4), 10-12,22
20
probably contributed to by the
10
spread of methadone maintenance
0
and needle exchange programs.9,23
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Elaborated from Treatment indicator of the Spanish Observatory on Drugs. DGPNSD.
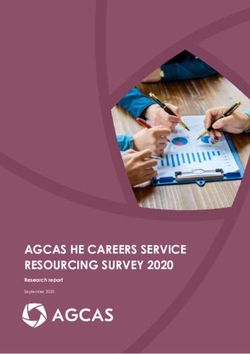
Men who have sex with men
Figure 4. HIV infection among injecting drug users European statistics on AIDS cases
who were voluntarily tested. show that Spain is one of the
countries with the highest rates in
45 Prevalence (%) Nº of HIV+ 350 homo/bisexual men.7 HIV
38,4
40
300 seroprevalence in homo/bisexual
33,1
35 30,7 men declined in the first half of the
250
Number of HIV+
28,9 27,9 28,2
Prevalence (%)
30 1990s, but subsequently has
23,9 25
25 22,2 200
remained stable at around 10%
20 150 (Figure 5).4-5,24 In other European
15 countries, there have been recent
100
10 reports of increases in risk
5 50
practices,25 incidence rates of
0 0
sexually transmitted diseases,26 and
1992 1993 1994 1995 1996 1997 1998 1999 2000
the incidence of HIV in homosexual
Year
The EPI-VIH Study. men.27 This new trend may also be6 HIV AND AIDS IN SPAIN, 2001
occurring in Spain, as reflected by a Figure 5. HIV infection among homo/bisexual men
recent study in Madrid, which found voluntarily tested.
an upward trend in HIV transmission
since 1997 in a cohort of men with 25 Prevalence (%) Nº of HIV+ 250
homosexual practices.16 19,6
20 200
Number of HIV+
Recent studies have found that men 15,6
Prevalence (%)
15 13 150
who have sex with men, male sex 11,1
10 10,3 10,4
workers and transvestites are 10 8,8 8,3 100
groups especially susceptible to HIV;
furthermore, it is worth noting that 5 50
nearly half of the men in these
groups are of Latin American 0 0
origin.28-30 1992 1993 1994 1995 1996 1997 1998 1999 2000
Year
The EPI-VIH Study.
Heterosexual transmission of HIV
HIV transmission through heterosexual contacts has remained an endemic phenomenon in Spain,
without appreciable changes. However, the level of endemicity has been relatively high compared
to other European countries, as is revealed by comparison of the AIDS rates in this transmission
category.7
The marked decrease in other mechanisms of HIV transmission in Spain has caused heterosexual
transmission to become the leading cause of infections in recent years, although this does not
imply an increase in the number of infections by this route.
The heterosexual population is very heterogeneous in terms of the risk of HIV infection. The
data that probably best summarize this situation are those for seroprevalence in women
delivering a liveborn child, which ranges from 1 to 3 per 1000, although there are differences
between autonomous communities.24,31 Among persons who only have heterosexual exposure,
the highest risk of HIV infection is found in those with an infected sexual partner, most of which
are IDUs or ex-IDUs. Over the years, this group has shown infection prevalence rates of over
5%, with no clear signs of a decrease (Figure 6).32
In women engaging in sex work, HIV seroprevalence has fallen below 2% (Figure 7), and
intravenous drug use has become an uncommon practice.13,14,32 A massive influx of immigrant
women from Latin America, sub-Saharan Africa and Eastern Europe has occurred in recent
years in this group; however, an increase in levels of infection has not been observed to
date.28,32HIV AND AIDS IN SPAIN, 2001 7
Figure 6. HIV seroprevalence among persons New diagnoses of HIV infection
with HIV infected heterosexual partner. reflect moderate decreases in the
number of infections from
14
12,4
heterosexual transmission,17 which
12 10,6 10,6
agrees with the lower frequency of
10,5 10,3
9,9 sexual risk behaviors in the Spanish
10 9,3
Prevalence (%)
8,5
8
7,9 population compared to other
countries,33 and the continuous
6
decrease in the incidence of sexually
4
transmitted diseases during the
2
1990s.34
0
1992 1993 1994 1995 1996 1997 1998 1999 2000
Year
Mother-to-child transmission
The EPI-VIH Study.
Spain was the European country
with the highest incidence of AIDS
through mother-to-child transmis-
Figure 7. HIV seroprevalence among female sex sion.7 The high effectiveness of
workers voluntarily tested. antiretroviral therapy in reducing
10
the rate of mother-to-child HIV
8,4 TOTAL transmission led to it being
8 Non injecting drug users proposed as a goal to virtually
eliminate infections transmitted by
Prevalence (%)
6 this mechanism, for which early
5
4 diagnosis of infection in all pregnant
4
2,5 2,4
2,8 women is a prerequisite. In recent
2 1,4 1,3 1,3
1,8
1,3 1,3
years, between 500 to 1000 HIV-
1 0,9 0,8 0,7
0,6 0,3 infected women have delivered a
0 liveborn child in Spain but, thanks to
1992 1993 1994 1995 1996 1997 1998 1999 2000 new treatments, it is estimated that
Year
the number of children born with
The EPI-VIH Study. HIV infection is well below 40.31 The
number of HIV infections and AIDS
cases in children of infected mothers has been markedly reduced (Figure 8),3 but still shows that
there is a long way to go for complete control of this mechanism of transmission.8 HIV AND AIDS IN SPAIN, 2001
HIV infection and immigrants Figure 8. Mother-to-child transmitted AIDS
cases in Spain.
Of the AIDS cases diagnosed in
Spain up to 2001, less than 3% AZT recomendation to
HIV-infected pregnant women
were persons from other countries 100
of origin, which reflects the fact
No. of new AIDS cases
80
that AIDS epidemic has mainly Proteasa inhibitors
affected the national population.3 In 60
recent years, progressive control
40
of HIV transmission in the Spanish
population, together with a 20
growing influx of immigrants to 0
Spain, has caused this characteristic 1985 1987 1989 1991 1993 1995 1997 1999 2001
of the HIV epidemic to be Year
reversed. The fact that some
immigrants come from countries
where HIV/AIDS is highly endemic may have some impact, but it is likely that adverse social
conditions, leading to situations of greater vulnerability to HIV infection, such as prostitution
or drug use, and greater difficulty to access prevention measures and health services, play a
more important role.35-36
As was previously described for other countries in Europe, the growing importance of immigrant
populations in the HIV epidemic has also started to become evident in Spain. In all autonomous
communities that have data on newly diagnosed AIDS cases, over 20% of the persons diagnosed
with HIV infection in 2001 were
immigrants, a percentage which has
Figure 9. Number and percentage of AIDS cases in
doubled in just two years. 37
Spain in persons from other countries of origin.
Nevertheless, HIV prevalence rates
in immigrants who underwent Number of AIDS cases Percentage of all AIDS cases 10
150
voluntary testing have not been
higher than those found in a Spanish 8 Percentage of all cases
Number of AIDS cases
population of similar characteristics, 100
except in women from sub-Saharan 6
Africa and men from Latin 4
America.28 50
2
This new trend has begun to have 0 0
impact on the number of AIDS cases
89
90
91
92
93
94
95
96
97
98
99
00
01
19
19
19
19
19
19
19
19
19
19
19
20
20
(Figure 9), in which there is an
increasing proportion of persons YearHIV AND AIDS IN SPAIN, 2001 9
with a country of origin other than Spain, mainly Africa, Latin America and Portugal.3 Diagnosis
of HIV infection and AIDS in persons from other countries does not mean that they were
already infected when they arrived; as at least a third of immigrants diagnosed with AIDS in
Barcelona may have acquired the infection in Spain.38
• NUMBER AND CHARACTERISTICS OF PERSONS LIVING
WITH HIV INFECTION
The key feature of the current situation of the epidemic in Spain is the existence of a high
number of persons living with HIV infection (Table 1). Advances in antiretroviral therapy have
improved survival considerably, but have been unable to achieve a cure, making HIV infection a
chronic disease. New therapies have improved the quality of life of HIV-infected persons,
although, once started, treatment must be maintained on an indefinite basis.
HIV prevalence in the general population is approximately 3 infections per one thousand
inhabitants, increasing to 6 per thousand in the 20 to 39 years age group.6,39 In line with the
general pattern of the epidemic, seroprevalence in men is three times higher than in women. In
mothers of newborns, i.e., in sexually active women of childbearing age, seroprevalence rates
range from 1 to 3 per thousand in most autonomous communities.24,31
Table 1. End-2001 estimates of the HIV/AIDS epidemic in Spain.
Persons living with HIV infection 110,000 – 150,000
Prevalence of HIV infection (rate per 1000 inhabitants) 2.7 – 3.8
Probable mechanism of infection in persons living with HIV
Injecting drug users 50% - 60%
Men with homosexual practices 15% - 25%
Heterosexual risk 20% - 30%
Characteristics of persons living with HIV
Men 75% - 80%
Women 20% - 24%
Children (under 13 years) < 1%
Persons developing AIDS since the start of the epidemic* 65,000 – 75,000
New AIDS diagnoses in 2001* 2,500 – 3,000
AIDS incidence rate in 2001 (per 100,000 inhabitants)* 6.3 – 7.5
HIV/AIDS deaths since the start of the epidemic* 40,000 – 50,000
Persons living with HIV-hepatitis C coinfection 60,000 – 80,000
* Estimates take into account underreporting.10 HIV AND AIDS IN SPAIN, 2001
Based on this seroprevalence data, Figure 10. Estimated time trends of HIV epidemic in
there are an estimated 110,000- Spain.
150,000 persons living with HIV
infection in Spain, although probably 140000 Persons newly infected with HIV
more than a quarter of them have HIV related deaths
120000 Persons living with AIDS
not yet been diagnosed (Figure 10).
100000
No. of persons
In recent years, the population of
persons living with HIV infection has 80000
remained relatively stable, since 60000
both the number of new infections 40000
and the number of deaths in infected
20000
persons have fallen to low levels.40
0
1982 1984 1986 1988 1990 1992 1994 1996 1998 2000
The epidemiological characteristics
of these persons depend less on Year
new infections than on those that
have accumulated over the course of the epidemic. These characteristics can be approximated
by studying the number of AIDS cases diagnosed in recent years3 or the number of patients with
HIV infection reported in hospital surveys, as both figures arise directly from the population of
persons living with HIV infection. Based on either of these sources, we can estimate that a little
more than half (50-60%) of HIV-infected living persons acquired the infection by sharing
parenteral drug injection equipment, 20-30% from unprotected heterosexual practices and 15-
25% are men who became infected through unprotected homosexual practices. The proportion
of men to women is approximately 4:1, and the average age of these persons is from 35 to 40
years, with a progressive trend toward aging.
The high frequency of intravenous drug use among persons living with HIV in Spain explains why
more than half of them are also infected by hepatitis C virus.
• REDUCTION OF HIV/AIDS MORBIDITY AND MORTALITY
Most persons with HIV infection will tend to progress to AIDS if the natural course of the
disease is allowed to go unchecked, resulting in high levels of morbidity and mortality from AIDS.
Highly active antiretroviral therapies have changed this situation, dramatically improving the
prognosis for infected persons.41 Following their introduction in 1997, they caused very sharp
decreases in the incidence of AIDS and mortality (Figure 11). In recent years, these decreases
have become less pronounced, which leads us to suspect that the ceiling for their effectiveness
may have been reached.3 In 2001, the lowest AIDS rates in the last ten years were recorded in
Spain (5.8 new AIDS cases per 100,000 inhabitants), but despite this significant advance, theyHIV AND AIDS IN SPAIN, 2001 11
Figure 11. Time trend in AIDS incidence and were still high compared to other
mortality in Spain. European countries, making Spain
the second ranking country in the
Expanded AIDS case definition AIDS incidence rate, only surpassed
8000 Highly active by Portugal.7
New AIDS cases antiretroviral therapy
AIDS deaths
Antiretroviral therapies currently
Number of persons
6000
play a fundamental role in continuing
4000 to reduce morbidity and mortality
from HIV/AIDS and in preventing
2000 AIDS incidence and mortality from
recovering past levels, since the
0 number of HIV-infected living
1985 1987 1989 1991 1993 1995 1997 1999 2001 persons is still very high. The main
Year factors hindering greater impact of
antiretroviral therapies are: late
diagnosis of AIDS leading to delays in the start of treatment,42 lack of patient compliance with
treatment, the emergence of resistance to antiretroviral drugs and adverse reactions requiring
prescribed treatments to be withdrawn or changed.
Delayed diagnosis of HIV infection has been shown to be an important factor in reducing the
impact of antiretroviral therapies,42,43 and probably of preventive measures as well.44 Its
importance is illustrated by the fact that of all persons diagnosed with AIDS since 1998, over
a third did not know they were infected by HIV, and this proportion exceeds 50% in AIDS
cases due to sexual transmission
(Figure 12).
Figure 12. AIDS cases unaware of their HIV
infection up to AIDS diagnosis, 1998-2001. Improved life expectancy in HIV-
infected persons is providing the
Heterosexual
opportunity for other late-
59
category developing health problems to
appear. The most notable case of
Homo/bisexual
men 56,3 this is infection by hepatitis C virus,
the high frequency of which in HIV-
Injecting drug infected persons is leading to an
users 17,3
increasing incidence of chronic liver
disease and cirrhosis.
TOTAL 35,6
0 10 20 30 40 50 60 70
%12 HIV AND AIDS IN SPAIN, 2001
KEY FACTORS IN THE FUTURE OF THE EPIDEMIC
The HIV/AIDS epidemic is Spain is showing a favorable course and appears headed toward
progressive control of the epidemic. However, there are various factors that could mark the
course of the epidemic in the near future.
– The risk of HIV infection in the population through known transmission mechanisms persists.
A relaxation in healthy behaviors could cause new upturns in the epidemic at any time.
– Some HIV transmission categories, such as men with homosexual practices and persons with
HIV-infected partners, continue to have a less favorable course and have even shown recent
increases.
– The existence of a considerable proportion of HIV-infected persons who have not been
diagnosed has various implications for the course of the epidemic. They may play a significant
role in HIV transmission and also do not benefit from antiretroviral therapies, with the
consequent adverse effects on AIDS incidence and mortality.
– Treatment of HIV infection is continually evolving and changes may occur which differ in their
impact on the epidemic, such as the spread of resistant viral strains or the introduction of
new drugs that improve on and complement previous existing drugs.
– The demographic and social changes that are occurring in Spain as a result of immigration
introduce new elements to be taken into account for prevention and control of the epidemic.
– The principal element of uncertainty about the epidemic comes from the global environment,
where HIV is very widespread and continues to progress.45 Geographical barriers do not
prevent the spread of HIV, so while an effective vaccine remains unavailable, control of the
epidemic will only be possible through close international cooperation.HIV AND AIDS IN SPAIN, 2001 13 HIV AND AIDS IN SPAIN, 2001 – KEY POINTS. HIV transmission • HIV transmission is much lower than it was in the past, but is still high. • The number of new infections through sexual transmission has decreased less and currently surpasses parenteral transmission. • Injecting drug use, homosexual relations between men and having an infected sexual partner are, in order of importance, the situations associated with the highest risk of infection. • Promotion of HIV testing in pregnant women helps to reduce infection through vertical transmission. People living with HIV infection • In spite of new treatments, there is still no cure for HIV infection. • There are approximately 120,000 infected persons, a figure that has remained relatively stable in recent years. • Over half of these persons acquired the infection through injecting drug use, and most have hepatitis C virus coinfection. Reduction of morbidity and mortality • AIDS incidence and mortality decreased markedly following the introduction of highly active antiretroviral therapies. • This trend has recently slowed even though the incidence of AIDS is still high. • Persons who do not know they are infected cannot benefit from treatment, which is why early diagnosis of infection is so important. • AIDS is still a significant cause of mortality in young adults in Spain. Principal uncertainties in the near future • Difficulties in maintaining protective behaviors over the long term. • Advances and possible problems modifying the effectiveness of antiretroviral therapy. • Influence of migratory movements of the population on HIV infection in Spain.
14 HIV AND AIDS IN SPAIN, 2001
REFERENCES
1. Castilla J, Bolea A, Suárez M, de la Fuente L. Spain. In McElrath K. HIV and AIDS: A World View.
Westport, CT: Greenwood Press, 2002,
2. Fernández Sierra MA, Gómez Olmedo M, Delgado Rodríguez M, et al. Infección por el virus de la
inmunodeficiencia humana en la población española (II). Metaanálisis de las tendencias temporales y
geográficas. Med Clin (Barc) 1990;95:366-71.
3. Centro Nacional de Epidemiología. Vigilancia Epidemiológica del Sida en España. Situación a 31 de
diciembre de 2001. Bol Epidemiol Semanal 2001; 10: 1-4.
4. Del Romero J, Castilla J, García S, et al. Evolución de la prevalencia de infección por el virus de la
inmunodeficiencia humana en un colectivo de varones homo/bisexuales de Madrid (1986/1995). Med
Clin (Barc) 1997;110:209-12.
5. Centre d’Estudis Epidemiològics sobre la Sida de Catalunya. Monitoratge de la prevalença i del nivell
de prevenció de la infecció per l’HIV en la comunitat d´homes homosexual i en usaris de drogues per
via parenteral. Document tecnic nº 11. Barcelona: Departament de Sanitat i Seguretat Social, 2000.
6. Downs AM, Heisterkamp SH, Brunet JB, Hamers FF. Reconstruction and prediction of the HIV/AIDS
epidemic among adults in European Union and low prevalence countries of central and eastern
Europe. AIDS 1997;11:649-662.
7. European Centre for the Epidemiological Monitoring of AIDS. HIV/AIDS surveillance in Europe. End-
year report 2001. Saint-Maurice: Institut de Vielle Sanitaire, 2001, No. 66. (http://www.eurohiv.org)
8. Castilla J, Martínez de Aragón MV, Gutiérrez A, Llácer A, Belza MJ, Ruiz C et al. Impact of HIV
mortality among young men and women in Spain. Int J Epidemiol 1997;26:1346-51.
9. Plan Nacional sobre Drogas. Memoria 2000. Madrid: Delegación del Gobierno para el Plan Nacional
sobre Drogas, 2001.
10. De la Fuente L, Bravo MJ, Lew C, et al. Prevalencia de infección por el virus de la inmunodeficiencia
humana y de conductas de riesgo entre consumidores de heroína en Barcelona, Madrid y Sevilla: un
ejemplo de centrar los estudios en consumidores y no sólo en usuarios por vía intravenosa. Med Clin
(Barc) 1999;113:646-51.
11. Hernández-Aguado I, Aviñó MJ, Pérez-Hoyos S, et al. Human immunodeficiency virus (HIV) infection
in parenteral drug users: evolution of epidemic over 10 years. Int J Epidemiol 1999;28:335-340.
12. Sopelana P, Carrascosa C, García-Benito P. Evolución de la prevalencia de la infección por el VIH-1 en
los drogodependientes de la Comunidad de Madrid (1985-1996). Med Clin (Barc) 1998;111:257-8.
13. Ballesteros J, Clavo P, Castilla J, et al. Low seroincidence and decrease in seroprevalence among
female prostitutes in Madrid [letter]. AIDS 1999; 13:1143-4.
14. Vioque J, Hernández-Aguado I, Fernández García E, et al. Prospective cohort study of female sex
workers and risk of HIV infection in Alicante, Spain (1986-1996). Sex Transm Inf 1998;74:264-88.HIV AND AIDS IN SPAIN, 2001 15
15. GEMES (Grupo Español Multicéntrico para el Estudio de Seroconvertores). El periodo de incubación
del sida en España antes de la terapia antirretroviral de alta eficacia. Med Clin (Barc) 2000;115:681-686.
16. Del Romero J, Castilla J, García S, Clavo P, Ballesteros J, Rodríguez C. Time trend in HIV
seroconversion incidence among homosexual men repeatedly tested in Madrid, 1988-2000. AIDS
2001;15:1319-1321.
17. Moreno C, Huerta I, Lezaun ME, et al. Evolución del número de nuevos diagnósticos de infección por
el VIH en Asturias, Navarra y La Rioja. Med Clin (Barc) 2000;114:653-5.
18. López de Munain J, Cámara MM, Santamaría JM, Zubero Z, Baraia-Etxaburu J, Muñoz J. Características
clínicoepidemiológicas de los nuevos diagnósticos de infección por el virus de la inmunodeficiencia
humana. Med Clín (Barc) 2001;117:654-656.
19. Castilla J, Pollán M, López-Abente G. The AIDS epidemic among Spanish drug users: a birth-cohort
associated phenomenon. Am J Public Health 1997;87:770-774.
20. Gómez-Lázaro R, del Romero J, Castilla J, et al. Categorías de exposición y seroprevalencia del VIH en
adolescentes que se realizaron voluntariamente la prueba. Madrid, 1986-2000. Gac Sanit 2001;15:202-
208.
21. De la Fuente L, Barrio G, Royuela L., Bravo MJ and the Spanish Group for the Study of the Route of
Heroin Administration. The Transition from injecting to smoking heroin in three Spanish cities.
Addiction 1997; 92:1733-1744
22. Bravo MJ, Bario G, de la Fuente L, Royuela L, Colomo C, Rodríguez MA et al. Evolución de la
prevalencia de infección por VIH y de prácticas de inyección entre inyectores de drogas infectados o
no por el VIH de tres ciudades españolas. Rev Clin Esp 2000; 200:355-59.
23. Secretaría del Plan Nacional sobre el Sida. Plan de movilización multisectorial frente al VIH/SIDA,
España 1997-2000, Evaluación. Madrid: Ministerio de Sanidad y Consumo, 2001.
24. Centre d’Estudis Epidemiològics sobre la Sida de Catalunya. Sistema integrat de vigilància
epidemiològica del VIH/sida a Catalunya (SIVES). Informe anual 2000. Barcelona: Departament de
Sanitat i Seguretat Social, 2001.
25. Dodds JP, Nardone A, Mercey DE, Johnson AM. Increase in high risk sexual behaviour among
homosexual men, London 1996-8: cross-sectional, questionnaire study. BMJ 2000, 320:1510-1.
26. Goulet V, Sednaoui P, Laporte A Billy C, Desenclos JC. The number of gonococical infections
identified by RENAGO network is increasing. Eurosurveillance Weekly 2000; 5:2-5.
27. Suligoi B, Giuliani M, Galai N, Balducci M and the STD Surveillance Working Group. HIV incidence
among repeat HIV testers with sexually transmitted diseases in Italy. AIDS 1999; 13:845-850.
28. The EPI-VIH Study Group. HIV infection among persons of foreign origin voluntarily tested in Spain. A
comparison with national subjects. Sex Transm Inf 2002 (in press).
29. Belza MJ, Llácer A, Mora R, Morales M, Castilla J, de la Fuente L. Sociodemographic characteristics and
HIV risk-behaviour patterns of male sex workers in Madrid (Spain). AIDS Care 2001;13:677-682.16 HIV AND AIDS IN SPAIN, 2001
30. Belza MJ, Llácer A, Mora R, et al. Características sociales y conductas de riesgo para el VIH en un
grupo de travestis y transexuales masculinos que ejercen la prostitución en la calle. Gac Sanit
2000;14:330-7.
31. Noguer I, García-Saiz A, Castilla J et al. Evolución de la seroprevalencia de VIH en madres de recién
nacidos entre 1996 y 1999. Med Clin (Barc) 2000;115:772-774.
32. Grupo para el Estudio Anónimo no Relacionado de Seroprevalencia de VIH en Consultas de ETS.
Seroprevalencia de infección por el VIH en pacientes de consultas de enfermedades de transmisión
sexual, 1998-2000. Med Clin (Barc) 2002; (en prensa).
33. Castilla J, Barrio G, de la Fuente L, Belza MJ. Sexual behaviour and condom use in the general
population of Spain, 1996. AIDS Care 1998; 10:667-676.
34. Centro Nacional de Epidemiología. Comentario epidemiológico de las enfermedades de declaración
obligatoria y Sistema de Información Microbiológica. España. Año 2001. Bol Epidemiol Semanal 2002;
10:49-54. (http://cne.isciii.es)
35. Secretaría del Plan Nacional sobre el Sida. Prevención del VIH/sida en inmigrantes y minorías étnicas.
Madrid: Ministerio de Sanidad y Consumo, 2001. (http://www.msc.es/sida).
36. Llácer A, del Amo J, Castillo S, Belza MJ. Salud e inmigración: a propósito del SIDA. Gac Sanit
2001;15:197-99
37. Castilla V, Alberdi JC, Barros C, Gómez J, Gaspar G, Sanz J. Cohorte multicéntrica de pacientes con
infección VIH de la corona metropolitana sur-este de Madrid (COMESEM): Fundamentos,
organización y resultados iniciales. Rev Clin Esp 2002 (in press).
38. García de Olaya P, Lai A, Jansá JM, Bada JL, Caylà JA. Características diferenciales del sida en
inmigrantes extranjeros. Gac Sanit 2000;14:189-94
39. Castilla J, Pachón I, González MP, et al. Seroprevalence of HIV and HTLV in a representative sample of
the Spanish population. Epidemiol Infect 2000; 125:159-62.
40. Castilla J, de la Fuente. Evolución del número de personas infectadas por el VIH y de los casos de sida.
España, 1980-1998. Med Clin (Barc) 2000; 115:85-9.
41. García de Olalla P, Caylà JA, Brugal MT et al. Evolución de la mortalidad y supervivencia del SIDA en
Barcelona (1981-1997). Med Clin (Barc) 1999;113:169-70.
42. Castilla J, Noguer I, Belza MJ, del Amo J, Sánchez F, Guerra L. ¿Estamos diagnosticando a tiempo a las
personas infectadas por el VIH?. Atención Primaria 2002;29:20-25.
43. Castilla J, Sobrino P, de la Fuente L, Noguer I, Guerra L, Parras F. Late diagnosis of HIV infection in the
era of highly active antiretroviral therapy: Consequences on AIDS incidence. AIDS 2002 (in press).
44. Janssen RS, Holtgrave DR, Valdiserri RO, Shepherd M, Gayle HD, De Cock KM. The serostatus
approach to fighting the HIV epidemic: prevention strategies for infected individuals. Am J Public Health
2001;91:1019-24.
45. ONUSIDA. La epidemia de SIDA. Situación en diciembre de 2001. Geneva: UNAIDS, 2001.
(http//www.unaids.org).HIV AND AIDS
IN SPAIN, 2001
MINISTERIO
DE SANIDAD
Y CONSUMO
SUBSECRETARÍA DE
SANIDAD Y CONSUMO
MINISTERIO DIRECCIÓN GENERAL DE
DE SANIDAD SALUD PÚBLICA Y CONSUMO
Y CONSUMO
SECRETARÍA DEL PLAN
NACIONAL SOBRE EL SIDAYou can also read