HIGH SARS-COV-2 VIRAL LOAD IN URINE SEDIMENT CORRELATES WITH ACUTE KIDNEY INJURY AND POOR COVID-19 OUTCOME
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BASIC RESEARCH www.jasn.org
High SARS-CoV-2 Viral Load in Urine Sediment
Correlates with Acute Kidney Injury and Poor
COVID-19 Outcome
Paulo S. Caceres,1,2 Gina Savickas,1,2,3 Shannon L. Murray,3 Kausik Umanath,4,5
Junior Uduman,4 Jerry Yee,4,5 Tang-Dong Liao,1 Steven Bolin ,6 Albert M. Levin,7,8
Moomal N. Khan,3 Sarah Sarkar,3 Jamie Fitzgerald,9 Dipak Maskey,1 Adrian H. Ormsby,10
Yuvraj Sharma,4 and Pablo A. Ortiz1,2,3
Due to the number of contributing authors, the affiliations are listed at the end of this article.
ABSTRACT
Background AKI is a complication of coronavirus disease 2019 (COVID-19) that is associated with high mor-
tality. Despite documented kidney tropism of the severe acute respiratory syndrome coronavirus 2 (SARS-
CoV-2), there are no consistent reports of viral detection in urine or correlation with AKI or COVID-19 severity.
Here, we hypothesize that quantification of the viral load of SARS-CoV-2 in urine sediment from patients with
COVID-19 correlates with occurrence of AKI and mortality.
Methods The viral load of SARS-CoV-2 in urine sediments (U-viral load) was quantified by qRT-PCR in 52
patients with PCR-confirmed COVID-19 diagnosis, who were hospitalized between March 15 and June 8,
2020. Immunolabeling of SARS-CoV-2 proteins Spike and Nucleocapsid was performed in two COVID-19 kid-
ney biopsy specimens and urine sediments. Viral infectivity assays were performed from 32 urine sediments.
Results A total of 20 patients with COVID-19 (39%) had detectable SARS-CoV-2 U-viral load, of which 17
(85%) developed AKI with an average U-viral load four-times higher than patients with COVID-19 who did
not have AKI. U-viral load was highest (7.7-fold) within 2 weeks after AKI diagnosis. A higher U-viral load cor-
related with mortality but not with albuminuria or AKI stage. SARS-CoV-2 proteins partially colocalized with
the viral receptor ACE2 in kidney biopsy specimens in tubules and parietal cells, and in urine sediment cells.
Infective SARS-CoV-2 was not detected in urine sediments.
Conclusion Our results further support SARS-CoV-2 kidney tropism. A higher SARS-CoV-2 viral load in urine
sediments from patients with COVID-19 correlated with increased incidence of AKI and mortality. Urinary viral
detection could inform the medical care of patients with COVID-19 and kidney injury to improve prognosis.
JASN 32: 2517–2528, 2021. doi: https://doi.org/10.1681/ASN.2021010059
The novel severe acute respiratory syndrome coro- addressing viral presence in target organs in rela-
navirus 2 (SARS-CoV-2) emerged in late 2019, and tion with COVID-19 complications. One of the
the associated coronavirus disease 2019 (COVID- most common complications of COVID-19 is
19) rapidly became a pandemic.1 Patients with
severe COVID-19 present with dyspnea and hyp- Received January 16, 2021. Accepted May 23, 2021.
oxemia, leading to respiratory failure. However, Published online ahead of print. Publication date available at
SARS-CoV-2 does not exclusively infect respira- www.jasn.org.
tory tract cells, as documented in recent studies Correspondence: Dr. Pablo A. Ortiz, Hypertension and Vascular
in enterocytes, endothelial cells, and kidney Research Division, Department of Internal Medicine, Henry Ford
cells.2–5 It is not clear to what extent this multior- Hospital, 6135 Woodward Ave., Detroit, MI 48202. Email:
portiz1@hfhs.org
gan tropism contributes to poor COVID-19 out-
come, mainly due to lack of conclusive studies Copyright ß 2021 by the American Society of Nephrology
JASN 32: 2517–2528, 2021 ISSN : 1533-3450/1046-2517 2517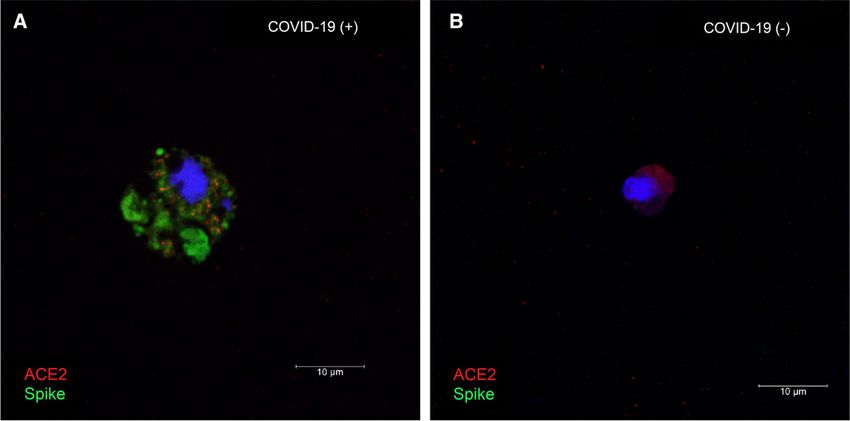
BASIC RESEARCH www.jasn.org
AKI, which occurs in up to 49% of patients, with higher rates
Significance statement
in minority groups,6–11 and is linked to poor COVID-19
prognosis and mortality.12–14 Despite the documented pres- AKI has been recognized as a common complication of coronavi-
ence of SARS-CoV-2 in kidney tissue,2–5,15,16 efforts to detect rus disease 2019 (COVID-19) and is associated with disease sever-
ity and mortality. The mechanisms behind these associations
viral genetic material or infective particles in urine have been
remain obscure, due, in part, to unsuccessful attempts to consis-
inconclusive. Most studies reported an absent or very low tently detect the novel severe acute respiratory syndrome corona-
detection rate of viral genetic material in whole urine, and virus 2 (SARS-CoV-2) in urine, despite evidence of kidney tropism.
only few laboratories have examined the presence of infective This study consistently quantifies the SARS-CoV-2 genome via
SARS-CoV-2.17–21 This lack of in-depth urine analysis has quantitative RT-PCR in cells of urine sediments from patients
with COVID-19. It was found that viral load in urine sediment
prevented the establishment of an association between urine
was higher within 2 weeks of the AKI event among patients with
SARS-CoV-2 load and kidney injury, precluding us from tak- COVID-19, and it correlated with increased risk of death. Quanti-
ing advantage of an easily accessible, noninvasive sample as a fication of viral load in urine sediment offers a noninvasive
diagnostic tool for patients with COVID-19. It is unclear why approach that could help identify and care for those patients
virus detection in urine is so challenging. Possible reasons with COVID-19 who are at higher risk of kidney injury and poor
outcome.
could be related to variability in urine volume, incomplete
replication or release by infected kidney cells, or virus
destruction in urine by excreted proteases and RNAses. All in the following weeks after an AKI episode (up to 8 weeks).
of these factors could be minimized using detection method- Only one patient in the cohort was not available for specimen
ologies with increased sensitivity that measure the presence collection after the AKI episode and was excluded from the
of SARS-CoV-2 directly in cells of renal origin, such as the quantitative RT-PCR (qRT-PCR) analysis.
cells shed in urine sediments. Here, we tested the hypothesis
that the viral load of SARS-CoV-2 can be quantified in urine Urine Sediment Specimen Collection
sediment and that it correlates with occurrence of AKI and Urine samples were obtained as spontaneously voided or
risk of death among patients with COVID-19. A better bladder-catheterized specimens, and only included in the
understanding of the effect of SARS-CoV-2 presence in the study if fresh urine sample could be obtained and processed
kidney, its detection in urine, and its relationship to kidney immediately by study staff. Urine sediments were obtained
damage could better inform medical decisions to treat within 2–4 hours of sampling by centrifugation at 1000 3 g
patients with COVID-19. for 10 minutes, followed by two washes with cold PBS
buffer. All samples were handled in a biosafety level 2 labo-
ratory after approval from the internal Institutional Recom-
METHODS binant DNA and Biosafety Committee. Viral RNA was
extracted by resuspending urine sediments in lysis buffer
Patients from the viral RNA extraction kit (Takara Bio USA, Ann
During the time frame of our study, 1320 patients were Arbor, MI), following the manufacturer’s instructions.
admitted to the Henry Ford Hospital in Detroit, Michigan, RNA was quantified in a Qubit 4 Fluorometer using the
with a clinical diagnosis of COVID-19. Between March 15 Qubit RNA High Sensitivity Assay Kit (Thermo Fisher Sci-
and June 8, 2020, a cohort of 652 patients enrolled in the entific, Waltham, MA). To estimate RNA sample purity, the
Translational and Clinical Research Center biobank at the
ratios of the absorbance at 260 nm and 280 nm were mea-
Henry Ford Hospital. From our biobank, 52 patients were
sured by NanoDrop (Gen5 Synergy H1 plate reader; BioTek,
enrolled with a COVID-19 diagnosis confirmed by labora-
Winooski, VT) in separate aliquots of ten samples of the
tory RT-PCR of nasopharyngeal swabs or tracheal aspirates.
highest RNA concentration, and were determined to be,
Clinical history, course of COVID-19, and clinical chart diag-
on average, 2.360.3.
nosis of AKI were abstracted from the electronic medical
record. Subsequently, the presence of AKI, its Kidney Disease
Improving Global Outcomes stage, and the presence of RRT Real-Time RT-PCR for SARS-CoV-2 in Urine Sediments
was adjudicated by two independent and blinded nephrolo- Viral RNA was extracted from urine sediments using a com-
gists. Any discrepancy was reconciled by a third nephrologist. mercial kit (Takara Bio USA). Between 10 and 500 ng of RNA
The results of the adjudication were used for all analyses were reverse transcribed using SuperScript III Reverse Tran-
reported (Figure 1). The institutional review board at Henry scriptase (Thermo Fisher Scientific) and random hexamers.
Ford Health System approved specimen collection and bio- Of the resulting cDNA from this reaction, 5 ml were used
banking. Each patient, or their legal representative, provided for real-time PCR in a ViiA 7 Real-Time PCR System
informed consent before participation, and only deidentified (Applied Biosystems, Foster City, CA). The cDNA was diluted
data were analyzed. Urine specimens were collected from at 1:10, 1:20, or 1:50 to ensure the measurements were within
14 consented, healthy, control volunteers; 18 patients with the linear range of the standard curve (Supplemental Figure
COVID-19 who had no AKI; and 33 patients with COVID-19 1). Oligonucleotide primers specific for the SARS-CoV-2
2518 JASN JASN 32: 2517–2528, 2021www.jasn.org BASIC RESEARCH
Participant enrollment in TCRC
Enrollment Biobank between 4/15/2020 and
06/08/2020 (N=652)
Excluded (N=560)
● Unable to produce urine at time of Collection
● Anuric Patients
● Processing limitations
Initial inclusion (N=92)
Inclusion ● Urine sedimentatiom conducted
within 4 hours of collection
● Administrative diagnosis of AKI
Excluded from analysis SARS-Cov-2 PCR positive diagnosis (N=52)
Blinded
Adjudication ● SARS-CoV-2 PCR negative ● Administrative diagnosis of AKI (N=42)
● Clinically suspected (N=40) ● No administrative diagnosis of AKI (N=10)
Analysis COVID-19 positive with AKI COVID-19 positive without presence of AKI
(N=34) (N=18)
Figure 1. Study design and inclusion criteria. Flowchart showing the exclusion and inclusion criteria used in this study to select the study
population of patients with COVID-19 who did or did not have AKI during their COVID-19–related hospital stay. TCRC, Translational and
Clinical Research Center.
Spike (S) and Nucleocapsid (N) genes were previously devel- SARS-CoV-2 Infectivity Assay
oped. The S primer set22 had the following sequences: Virus infectivity was assessed at a biosafety level 3 facility at
forward, 59 -CAATGGTTTAACAGGCACAGG-39 ; reverse, Michigan State University Veterinary Diagnostic Laboratory.
59 -CTCAAGTGTCTGTGGATCACG-39 . The N primers cor- African green monkey Vero E6 cells (ATCC, Manassas, VA)
responded to the N2 set developed by the Centers for Disease were grown at 80% confluency in Medium 199 with Earle
Control (CDC; https://www.cdc.gov/coronavirus/2019-ncov/ Balanced Salts (MilliporeSigma, St. Louis, MO) supple-
downloads/rt-pcr-panel-primer-probes.pdf). All primers were mented to 6% US origin FBS (Millipore Sigma). Urine sedi-
synthetized by Eurofins Genomics (Louisville, KY). Real- ment lysate was brought to 1 ml with Bovarnick buffer (pH
Time SYBR Green PCR mix was from Bio-Rad (Hercules, 7.0), and then centrifuged at 8,000 3 g for 5 minutes to pellet
CA). Urine sediments from 14 healthy, nonsymptomatic, con- debris. The clarified liquid was passed through a 0.22-mm
trols, with no history of COVID-19 or AKI, were analyzed to syringe filter directly onto cell cultures. Cells were cultured
establish background RT-PCR signal. Viral RNA copies were and monitored daily for cytopathic effects for up to 10
quantified with a standard curve of heat-inactivated SARS- days. At the end of this period, RNA was extracted and
CoV-2 complete genome (catalog number NR-52347, lot num- real-time qRT-PCR was performed for SARS-CoV-2 genes
ber 70033926; National Institutes of Health [NIH], National N and S to confirm presence or absence of viral replication.
Institute of Allergy and Infectious Diseases, BEI Resources,
Manassas, VA). The number of viral copies per nanograms Immunofluorescence and Confocal Microscopy
of RNA was calculated as: viral copies3PCR dilution factor/ Kidney biopsy sample slides were obtained from two patients
nanograms RNA. with RT-PCR–confirmed COVID-19 and two patients nega-
The intra- and interassay coefficients of variation were tive for COVID-19 (negative controls) by the Translational
0.9%60.1% and 1.8%60.3%, respectively, as determined by and Clinical Research Center. Biopsies were indicated for
triplicates that were run in parallel and sequentially. Single- unexplained nephrotic-range proteinuria with clinical concern
band amplification was verified by gel electrophoresis. for rapidly progressing GN in patients with COVID-19.
JASN 32: 2517–2528, 2021 Urine SARS-CoV-2 and Kidney Injury 2519BASIC RESEARCH www.jasn.org
Formalin-fixed, paraffin-embedded slices were first deparaffi- rank correlations. All statistical analyses were performed
nized with xylene and then rehydrated gradually through using GraphPad Prism 8.2.1 (GraphPad Software, San Diego,
100% ethanol to distilled water. Slides were incubated for 10 CA), with the exception of the analysis for inpatient mortal-
minutes with 0.05% Triton X-100 at room temperature (RT) ity. The association between the viral load of SARS-CoV-2 in
for permeabilization followed by antigen retrieval using citric urine sediments (U-viral load) and inpatient COVID-19
acid buffer (10 mM, pH 6.0). Slides were then blocked with 5% mortality was performed using the Fine and Gray competing
BSA to block nonspecific binding. Slides were incubated with risk model with the R statistical programming language pack-
primary antibodies, either a 1:200 dilution of SARS-CoV-2 age “cmprsk.” In this analysis, inpatient mortality was mod-
spike mAB (clone 1A9; Gentex, Irvine, CA) or SARS-CoV-2 eled as the primary hazard, and alive at hospital discharge
nucleocapsid antibody (clone 6H3; Gentex), at 4 C overnight. was modeled as the secondary hazard. Patients who were still
This was followed by 1:100 of Alexa Fluor 647 donkey anti- in the hospital and alive as of June 8, 2020 were censored. To
mouse IgG (Molecular Probes, Eugene, OR) for 1 hour at account for multiple admissions, the total number of inpa-
RT. To label angiotensin-converting enzyme 2 (ACE2), slides tient days across all admissions for a patient was considered
were then incubated with a 1:50 dilution of ACE2 rabbit mAB the inpatient time to event. Hazard ratios (HRs) and 95% CIs
(clone EPR4435; Abcam, Cambridge, MA) after blocking with for the association of U-viral load with mortality were calcu-
1% BSA, followed by incubation with 1:100 Cyanine3 donkey lated both unadjusted and adjusted for age, sex, and Black
anti-rabbit IgG (Jackson ImmunoResearch, West Grove, PA) race/ethnicity. P values ,0.05 were considered statistically
for 1 hour at RT. Finally, slides were counterstained with significant.
49 ,6-diamidino-2-phenylindole at a dilution of 1:2000 for 5
minutes at RT. Controls for nonspecific secondary antibody
binding were performed without primary antibodies, and RESULTS
were completely negative. COVID-19–negative and COVID-
19–positive slides were imaged the same day, with identical SARS-CoV-2 Detection in Urine Sediments from
settings, using a Leica TCS SP8 MP confocal/multiphoton Patients with COVID-19 and AKI
microscopy system (Leica Microsystems, Wetzlar, Germany), The baseline characteristics of our study cohort of 52 patients
with a 633/1.40 oil CS2 Harmonic Compound Plan Apochro- with a confirmed COVID-19 diagnosis are summarized in
mat lens. We also tested antibodies against SARS-CoV-2 Table 1. The mean6SD follow-up time from COVID-
nucleocapsid protein (A50, 1:250; Rockland Antibodies, Lim- 19–related admission was 53.7617.9 days. Two SARS-CoV-
erick, PA) or SARS-CoV-2 membrane protein (A55, 1:200; 2 genes (S and N) were successfully detected by RT-PCR
Rockland Antibodies).23 All of these antibodies have recently and quantified by extrapolation to a standard curve of the
SARS-CoV-2 genome (Supplemental Figure 1). A mean6SD
been used by other investigators to detect SARS-CoV-2 in
U-viral load of 17306344 copies/ng RNA was measured in
respiratory tissue and placenta,5,24 and in human liver duct
non-AKI COVID-19 specimens (NS versus background in
organoids.25
COVID-19–negative controls, P50.38; Figure 2A). In speci-
mens from patients with COVID-19 who developed AKI, the
Albumin-Creatinine Ratio U-viral load was 3.9-times higher (P50.001; mean6SD,
Spontaneously voided or bladder-catheterized urine samples 677961479 copies/ng RNA) compared with background in
were obtained from hospitalized patients and briefly centri- COVID-19–negative controls (Figure 2A). In patients where
fuged (1000 3 g, 10 minutes) to eliminate particulate mate- urine was collected within the first 2 weeks after an AKI epi-
rial. Supernatants were used for determination of urine sode, the U-viral load was significantly higher (13,26663033
albumin (catalog number ab108788; Abcam) and creatinine copies/ng RNA, P50.004 versus non-AKI; Figure 2B),
(BioAssay, Hayward CA) concentration with ELISA kits. returning to levels comparable with non-AKI after 2 weeks
The measured urine albumin and creatinine concentrations (32126897 copies/ng RNA, P.0.99 versus non-AKI). To
were used to calculate the albumin-creatinine ratios (ACRs) assess the prevalence of high U-viral titers among patients
in milligrams per gram. with AKI, we set a threshold of three SDs of the background
signal from noninfected controls. Approximately half of the
Statistical Analyses patients with AKI had U-viral loads above this threshold,
For descriptive purposes, continuous variables were summa- compared with only three out of 18 (17%) of the non-AKI
rized using means and SDs, and categoric variables are group (P50.02; Figure 2C), indicating a larger proportion
summarized using frequency counts and percentages. of patients with AKI who had a higher SARS-CoV-2 viral
Between-group differences in continuous variables were load in urine sediments. The amount of RNA purified from
assessed using the nonparametric Kruskal–Wallis test. For patients with COVID-19 with or without AKI was not signif-
categoric variables, between-group frequency differences icantly different (P.0.99; Supplemental Figure 2) and there
were assessed using the Fisher exact test. Correlations was no correlation between U-viral load and starting amount
between continuous variables were tested using Spearman of RNA in the RT-PCR reaction (Spearman r correlation
2520 JASN JASN 32: 2517–2528, 2021www.jasn.org BASIC RESEARCH
Table 1. Baseline characteristics of the study cohort
Characteristics COVID-19 COVID-19 and AKI COVID-19 and No AKI P Value
Total 52 (100) 34 (65.4) 18 (34.6)
Age (years) 62613 64612 58615 0.24
Sex, n (%) 0.02
Male 30 (57.7) 24 (80.0) 6 (20.0)
Female 22 (42.3) 10 (45.5) 12 (54.5)
Race, n (%) 0.42
Black 37 (71.2) 23 (62.2) 14 (37.8)
White 11 (21.2) 8 (72.7) 3 (27.3)
Hispanic 2 (3.8) 2 (100) 0
Asian 1 (1.9) 1 (100) 0
Unknown 1 (1.9) 0 1 (100)
Height (m), mean6SD 1.7260.11 1.7560.09 1.6760.09 0.008
Weight (kg), mean6SD 94.9626.4 97.1625.3 90.9628.7 0.34
BMI (kg/m2), mean6SD 32.0468.65 31.4766.98 33.11611.30 0.90
Comorbidities, n (%)
Hypertension 41 (33.1) 28 (68.3) 13 (31.7) 0.48
Heart Failure 12 (9.7) 6 (50.0) 6 (50.0) 0.30
Diabetes 27 (21.8) 21 (77.8) 6 (22.2) 0.08
COPD 9 (7.2) 5 (55.6) 4 (44.4) 0.70
CKDa 35 (28.2) 28 (80.0) 7 (20.0) 0.004
Urine volume (ml), mean6SD 55.2624.3 55.0617.6 55.7634.2 0.66
Serum creatinine (mg/dl), mean6SD 1.961.8 2.261.8 1.762.0 0.02
Albuminuria (ACR.30 mg/g), n (%) 33 (63.5) 20 (60.6) 13 (39.4) 0.38
CRP .3 mg/L (34 on record; 65.4%), n (%) 23 (67.6) 15 (65.2) 8 (34.8) 0.46
Urinary tract infection, n (%) 12 (23.1) 8 (66.7) 4 (33.3) .0.99
Catheterized, n (%) 27 (51.9) 22 (81.5) 5 (18.5) 0.02
Blood in urine, n (%) 12 (23.1) 8 (66.7) 4 (33.3) .0.99
On ventilator, n (%) 30 (57.7) 25 (83.3) 5 (16.7) 0.003
Mortality, n (%) 12 (23.1) 10 (83.3) 2 (16.7) 0.18
Continuous variables are summarized as means6SDs. P values were calculated using the Kruskal–Wallis test (for continuous variables) or the Fisher exact test (for
categoric variables). BMI, body mass index; COPD, chronic obstructive pulmonary disorder; CRP, C-reactive protein.
aCKD presence determined by chart diagnosis during medical record abstraction. A breakdown of CKD stages follows: stage 1, n51; stage 2, n59; stage 3a/b, n511;
stage 4, n59; stage 5/ESKD, n55.
coefficient50.08, R25 0.006), indicating that viral load in were still alive at time of cutoff (Figure 3A). Figure 3B dis-
patients with AKI is not artificially high due to increased plays the cumulative incidence of inpatient mortality in those
cell shedding. To rule out additional possible confounding patients below and above the average of the highest recorded
factors, we further determined that the method of urine col- U-viral load (5141 copies/ng RNA) across all patients. At
lection (spontaneous voiding versus catheterization), the 60 days, those above and below this threshold had cumulative
presence of blood in urine, or requirement of mechanical mortality rates of 62% and 9%, respectively, with a
ventilation were not associated with higher U-viral loads corresponding HR of 11.5 (95% CI, 3.27 to 40.30;
(Supplemental Figure 3). P,0.001). Table 2 puts some clinical perspective on the sub-
Altogether, these results indicate higher levels of SARS- group of patients who died. A large majority had developed
CoV-2 genetic material in urine sediments from patients AKI (83.3%), and only two were in the non-AKI group. As
with COVID-19 who develop AKI. expected, the predominant cause of death was respiratory
and systemic complications from COVID-19. The only
U-Viral Load and COVID-19 Severity non-COVID-19–related death on record was one case of
U-viral load was associated with COVID-19 inpatient mor- metastatic cancer. This patient was in the non-AKI group
tality (P,0.001), with each increase of 10,000 viral copies/ and had low measurable U-viral load (539 copies/ng RNA),
ng RNA being associated with a 2.87-fold (95% CI, 1.76 to suggesting that the poor outcome was not related to
4.68) increased risk of death, and this increase in risk was COVID-19. Besides the higher U-viral load associated with
largely unchanged after adjustment for age, sex, and Black subsequent risk of death, we did not observe any correlation
race/ethnicity (HR, 3.28; 95% CI, 1.77 to 6.06; P,0.001). between mortality and duration of COVID-19, need of ven-
Among subjects who died, the U-viral load reached a high tilation, sepsis, or changes in BP (Table 2). However, because
of 11,07362816 copies/ng RNA at an average of 9 days before the number of patients who died (n512) was relatively small,
death. This viral load was three times higher than the average the statistical power was low. Similarly, we did not observe
33776860 copies/ng RNA (P50.03) recorded in subjects that any strong evidence of risk factors associated with patients
JASN 32: 2517–2528, 2021 Urine SARS-CoV-2 and Kidney Injury 2521BASIC RESEARCH www.jasn.org
A presenting with the highest U-viral loads .5141 copies/ng
35000 #
RNA in our cohort (Supplemental Table 1).
30000 In subjects with a urine ACR .30 mg/g, the average
U-viral load tended to be higher, but not significantly dif-
Viral copies / ng RNA
25000
ferent (383961330 viral copies/ng RNA for ACR,30 mg/
20000 g versus 564961329 viral copies/ng RNA for ACR$30
15000
mg/g; P50.50; Figure 3C). We did not find significant asso-
ciations of U-viral load with serum creatinine, blood in
10000 urine, C-reactive protein (Supplemental Figure 3), BUN,
5000 stage of AKI, or need for RRT (Figure 3D, 3E). This weak
correlation with renal parameters and markers of injury
0
Background Non-AKI AKI may be reflective of transient effects related to the time of
collection.
COVID-19 (-) COVID-19 (+)
B Presence of SARS-CoV-2 Proteins in Kidney Tissue
35000 #*
To provide additional evidence of SARS-CoV-2 infection in
30000 the kidney, we performed immunolabeling for the SARS-
CoV-2 spike and nucleocapsid proteins in kidney biopsy
Viral copies / ng RNA
25000
specimens from patients positive and negative for COVID-
20000
19 (Figure 4). Positive labeling for viral proteins was detected
15000 in different kidney cell types, including proximal tubules
(Figure 4, A, C, and D), parietal cells (Figure 4B), and distal
10000
tubules (with the appearance and size of collecting ducts;
5000 Supplemental Figure 4). Relatively low immunoreactivity
0
was observed in glomerular cells (Figure 4B). Only back-
Background Non-AKI 2 weeks 2+ weeks ground signal was observed in biopsy specimens from
patients negative for COVID-19 (Figure 4, E–G). ACE2,
weeks after AKI diagnosis
the receptor for viral entry, was abundant in proximal tubules
COVID-19 (-) COVID-19 (+)
and, to a lesser extent, parietal cells, and colocalized with
C Urine SARS-Cov-2 (+) intracellular SARS-CoV-2 in some proximal tubule cells (Fig-
Urine SARS-Cov-2 (-) ure 4, A and B, and Supplemental Figure 4B). We also con-
Percentage distribution (%)
100 ducted immunolabeling in fresh urine sediments embedded
80
in matrigel. The SARS-CoV-2 spike protein was detected in
single cells from a patient with positive urine RT-PCR (Fig-
60
ure 5A), but was absent in patients negative for COVID-19
40
(Figure 5B). ACE2 expression was detected in the same cells
20
(Figure 5), but not all cells in urine sediment expressed
0
Non-AKI AKI ACE2. Coexpression of ACE2 and the viral nucleocapsid pro-
tein was also observed in urine sediments from three addi-
tional patients with urine-positive RT-PCR (Supplemental
Figure 2. Higher presence of SARS-CoV-2 genetic material was Figure 5). The origin or identity of these cells was not
measured in urine sediments of patients with COVID-19 who determined.
developed AKI. (A) U-viral load was higher in patients with
COVID-19 and AKI, whereas it was not significantly different from
background in patients with COVID-19 without AKI. (B) U-viral Infectivity of SARS-CoV-2 Material from Urine
load was significantly higher in patients with COVID-19 and AKI It is unclear whether infective virions are shed in the urine, and
during the first 2 weeks after the AKI diagnosis. (C) A larger per- a previous study failed to detect this.18 We studied 32 fresh
centage of patients with COVID-19 and AKI had detectable urine sediments, 28 from patients positive for COVID-19
U-viral loads compared with patients with COVID-19 without AKI and four from negative controls, for cytopathic viral growth
(P,0.05, Fisher exact test). For patients with COVID-19, n551; in inoculated Vero E6 cells. Two out of 28 (7.1%) urine sedi-
for healthy controls, n514. Each dot represents an individual ment specimens generated cytopathic growth (both from
data point, average viral copies per nanogram RNA is indicated
patients diagnosed with AKI). However, subsequent RT-PCR
(dotted line) and SEM. Dark-colored dots represent the same indi-
failed to amplify any SARS-CoV-2 genetic material isolated
viduals in (A) and (B) with the highest viral loads. #P,0.05 versus
background; *P,0.05 versus non-AKI, Kruskal–Wallis test. from Vero E6 cells, suggesting the cytopathic effect observed
was secondary to a viral infection other than SARS-CoV-2.
2522 JASN JASN 32: 2517–2528, 2021www.jasn.org BASIC RESEARCH
C 35000
A 15000 B 30000
* 1.0 U-viral > 5140.7 counts/ng
U-viral ≤ 5140.7 counts/ng
13500
Cummulative Mortality Incidence
12000 0.8 25000
Viral copies /ng RNA
Viral copies /ng RNA
10500
0.6 20000
9000
7500 0.4 15000
6000
4500 0.2 10000
3000
0.0 5000
1500
0 10 20 30 40 50 60 70
0 Total Inpatient Days
Alive Deceased 0
< 30 ≥ 30
Albumin / Creatinin ratio (mg/g)
D 35000 E 35000
30000 30000
25000 25000
Viral copies /ng RNA
Viral copies /ng RNA
20000 20000
15000 15000
10000 10000
5000 5000
0 0
Non-AKI AKI-Stage 1 AKI-Stage 2 AKI-Stage 3 Non-AKI AKI-no RRT AKI-RRT
Figure 3. Higher SARS-CoV-2 U-viral load was associated with higher risk of mortality. (A) Increased U-viral load among patients who
died. (B) Cumulative incidence of inpatient mortality at above and below a viral load of 5141 copies/ng RNA. Sixty day HR, 11.50 (95%
CI, 3.27 to 40.30), P,0.001. The probabilities of nonsurvival (at risk) for the duration of the observation period were as follows: ,5141
copies/ng RNA, P50.09; .5141 copies/ng RNA, P50.62. (C) The average U-viral load was 1.5 times higher in patients with COVID-19
who had albuminuria at the time of sampling, but this was NS (P50.50, Kruskal–Wallis test). (D) Average U-viral load in patients with
COVID-19 at different stages of AKI (P50.12, Kruskal–Wallis test). (E) Average U-viral load in patients with COVID-19 and AKI who
needed RRT or not (P50.10, Kruskal–Wallis test). Each dot represents an individual data point, average viral copies per nanograms
RNA is indicated (dotted line) along with the SEM. n548. *P50.03, Kruskal–Wallis test.
DISCUSSION the mortality rate observed among the AKI subset of patients
with COVID-19 is disproportionately high.12–14 To gain
During the time frame of our study, 1320 patients were insight into the effect of COVID-19 in kidney dysfunction,
admitted to our institution in Detroit, Michigan, with a clin- this study was targeted to a cohort of 52 patients with labo-
ical diagnosis of COVID-19. Retrospective review of our ratory RT-PCR diagnosis of COVID-19. Here, we report
medical records showed that 614 patients (46.5%) were also higher viral copy number detected in urine sediment from
diagnosed with AKI. AKI was present in 172 of 225 patients with COVID-19 who developed AKI, and a strong
(76.4%) patients who died. A high incidence of AKI (up to correlation between U-viral load and subsequent mortality.
49% in US minority groups)11 has been documented in Urine sediments represent a noninvasive diagnostic tool
COVID-19 epicenters around the world.6–10 Furthermore, with potential for assessing patients with COVID-19
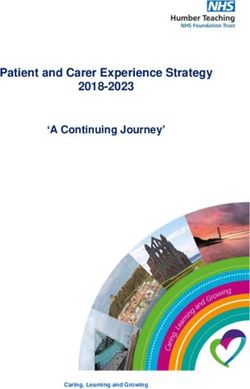
JASN 32: 2517–2528, 2021 Urine SARS-CoV-2 and Kidney Injury 2523BASIC RESEARCH www.jasn.org Table 2. Clinical characteristics of deceased COVID-19 patients Characteristics Alive Deceased P Value Total, n (%) 40 (76.9) 12 (23.1) AKI, n (%) 0.18 Yes 24 (60.0) 10 (83.3) No 16 (40.0) 2 (16.7) Cause of death, n (%) NA Acute respiratory failure — 7 (58.3) Multisystem organ failure — 1 (8.3) Arrythmia — 1 (8.3) Metastatic cancer — 1 (non-AKI) (8.3) Not on record — 1 (AKI) 1 1 (non-AKI) (16.7) Length of stay until death (d) — 23616 NA Duration of COVID-19 at sampling (d) 28619 20611 0.20 Required ventilation, n (%) 23 (57.5) 7 (58.3) .0.99 Developed sepsis, n (%) 12 (30.0) 2 (16.7) 0.48 Systolic BP (mm Hg), mean6SD 132621 124625 0.34 On BP medication, n (%) 31 (77.5) 8 (66.7) 0.47 Continuous variables are summarized as means6SDs. P values were calculated using the Kruskal–Wallis test (for continuous variables) or the Fisher exact test (for categoric variables). NA, not applicable. presenting with AKI.26 Previous, smaller-sized studies using COVID-19 shows evidence of tubular and glomerular whole urine detected no SARS-CoV-2–positive urine speci- damage, which is consistent with previous reports men,17,18 or only one such specimen.19,20 A recent, larger (Supplemental Figure 6). To our knowledge, there is no con- study in 81 patients showed a SARS-CoV-2 detection rate sensus in the literature on how kidney complications develop of 7% in whole urine.21 In an effort to maximize detection in patients hospitalized with COVID-19. AKI could arise in urine, in this study we collected urine sediments from from a systemic immune response, hemodynamic alterations, patients with COVID-19 and measured SARS-CoV-2 directly hypercoagulability, viral kidney tropism, or a combination of from cells contained in the sediment using a sensitive qRT- these factors. Although these mechanisms are not mutually PCR assay previously developed for respiratory samples.22 exclusive, the evidence for a localized immune response in We report a detection rate of 39% of tested urine sediment kidneys of patients with COVID-19 is inconsistent. Recent specimens, significantly higher than a 7.5% detection rate reports demonstrated autoimmune-like glomerular base- previously reported by a similar study in a cohort of 53 ment membrane disease,29 lymphocyte infiltration,4 arterio- patients with COVID-19.27 This increased sensitivity is prob- lar thrombosis, and collapsing glomerulopathy in the ably due to different RT-PCR methodologies, because this kidneys of patients with COVID-19. Other studies did not previous study using a probe-based RT-PCR assay for detec- find strong evidence of immune infiltration in kidney tissue tion of the SARS-CoV-2 N and Orf-1ab genes.27 In our during SARS-CoV-2 infection.26,30 These differences may hands, equivalent probe-based assays for the N and envelope be related to underlying conditions in populations from dif- (E) genes28 did not yield positive results. In comparison, the ferent ethnic backgrounds. Concerted actions and establish- SYBR Green–based assays we adopted for S and N genes22 ment of a national biopsy tissue repository should be showed higher sensitivity. Importantly, it has not been possi- generated to address these questions. ble, so far, to use U-viral load to establish a link between AKI An alternative cause of kidney damage as a consequence of and COVID-19,27 although this association has been widely COVID-19 is active SARS-CoV-2 tropism in the kidney. discussed in the medical literature, mostly on the basis of Recent studies reported detectable SARS-CoV-2 proteins in case reports or autopsy findings.6–11,15 The quantitative postmortem kidneys,2–5 in addition to electron microscopy approach presented here, using a viral genome standard detection of virus-like particles.3,4,31,32 However, concerns curve, revealed a positive correlation between SARS-CoV-2 have been raised about the misinterpretation of electron copy number in urine sediment, a noninvasive sample, and microscopy evidence on the basis of morphologic features higher frequency of AKI and mortality. Because different and their similarity to normal intracellular structures.33,34 methodologies result in varying sensitivity, we emphasize This study provides additional immunodetection-based evi- the advantages of standard curve–based quantitative meth- dence of expression of two SARS-CoV-2 proteins, nucleocap- ods for better comparisons across different studies to help sid and spike, in kidney cells from COVID-19 biopsy identifying patients with COVID-19 who are at higher risk specimens (Figure 4 and Supplemental Figure 4). Sites with associated with AKI. positive SARS-CoV-2 immunolabeling were proximal Due to limited specimen availability, we did not thor- tubules, distal nephron, parietal cells, and—potentially— oughly investigate the cause of AKI in our cohort. A kidney inflammatory cells, along with the cells shed in the urine. biopsy specimen from one of our patients positive for Expression of ACE2 in kidney proximal tubule cells has 2524 JASN JASN 32: 2517–2528, 2021
www.jasn.org BASIC RESEARCH Figure 4. SARS-CoV-2 spike and nucleocapsid proteins (green) are expressed in kidney biopsies, often coexpressed with ACE2 (red) in the same cell. (A) Proximal tubule (PT) in kidney cortex of patient 1 (positive for COVID-19). ACE2 signal was apical, outlining the lumen of proximal tubules, and SARS-CoV-2 spike protein was observed in an intracellular location (arrows). (B) Glomerulus (G) in the same patient as in (A). Inset shows higher magnification of the area in outlined square, where SARS-CoV-2 spike expression was detected in parietal cells. (C) Spike expression in area of tubular necrosis in the kidney cortex of patient 2 (positive for COVID-19). Inset shows higher magnification of area in outlined square where spike expression was detected in cortical tubules (nephron segment outlined by dotted line). (D) SARS-CoV-2 nucleocapsid expression in cortical tubule of patient 2 (positive for COVID-19). Arrowheads indicate cells of the tubular segment expressing nucleocapsid at different intensities. Inset shows higher magnification of area in outlined square. (E) ACE2 expression and absence of spike expression in proximal tubules of patient negative for COVID-19. (F) Absent spike expression in glomerulus of patient negative for COVID-19. (G) Absent nucleocapsid expression in kidney cortex of a patient negative for COVID- 19. Blue label is 49 ,6-diamidino-2-phenylindole nuclear staining in all panels. been associated with the ability of SARS-CoV-2 to infect cul- consistent with proximal tubule injury in a group of patients tured proximal tubule cells.35,36 However, whether this with COVID-19.37 The strong ACE2 labeling we observed in results in cytotoxicity remains to be determined. A more the brush border of proximal tubules in COVID-19–positive recent study showed clinical and histologic manifestations (n52) and –negative (n52) kidney biopsy specimens is JASN 32: 2517–2528, 2021 Urine SARS-CoV-2 and Kidney Injury 2525
BASIC RESEARCH www.jasn.org Figure 5. SARS-CoV-2 spike protein and ACE2 are coexpressed in cells in urine sediment from patients with COVID-19. (A) ACE2 (red) and SARS-CoV-2 spike (green) coexpression in the same cell isolated from urine sediment of patient positive for COVID-19. (B) ACE2 expression and absence of spike in single cell from urine sediment of patient negative for COVID-19. Blue label is 49 ,6-diamidino-2-phe- nylindole nuclear staining. consistent with previous literature.38,39 We observed very low Limitations of the Study ACE2 immunolabeling in cells other than proximal tubules. Our cohort was selected to study patients with kidney involve- However, this does not preclude the expression of very low ment. Thus, the elevated rate of AKI is not representative of levels of ACE2, which has been detected in other kidney cells the overall population of patients with COVID-19. Our patient by RNA sequencing.40,41 population is largely Black (70%), with high prevalence of Despite finding SARS-CoV-2 genetic material and protein comorbidities like CKD, hypertension, diabetes, and high in urine sediments, viability assays for cytopathic viral mortality (Table 1). AKI and prior CKD diagnosis are report- growth were negative, consistent with a previous report.18 edly higher in Black individuals with a COVID-19 diagno- The reasons behind these observations are not clear and sis.42,43 It is possible that our patient population is highly invite further investigation designed for this purpose. Some susceptible to developing AKI and this may not be representa- possibilities may include the inability of kidney cells to tive of other populations. That said, we relied on adjudicated assemble or release infective virions, or subsequent destruc- AKI diagnoses/outcomes for analyses rather than medical tion by extracellular proteases in the urine. However, lack record diagnoses, increasing the accuracy of our kidney out- of infective material in urine does not preclude from the comes. A larger cohort should be studied to determine the fact that SARS-CoV-2 may be able to reach and infect kidney influence of ethnic background or prior CKD diagnosis. In cells, as demonstrated by the detection of viral proteins in addition, a larger cohort can also better address the predictive kidney biopsy specimens in this report and previous studies value of SARS-CoV-2 RT-PCR detection in urine sediments to in postmortem kidney.2,3,5 Absence of infectious SARS- determine risk of AKI and severity of COVID-19. This predic- CoV-2 particles in urine is independent of whether viral pres- tive potential is also, most likely, tied to parallel monitoring of ence in urine material is associated with AKI and risk of poor viral loads in urine and blood. In this regard, a previous study COVID-19 outcome. This fact allowed us to present evidence in the related SARS coronavirus found that viral detection in in support of our hypothesis of direct kidney tropism, and blood seems to peak transiently during the first week of infec- detectable and quantifiable SARS-CoV-2 genetic material in tion, followed by a peak in urine and stool afterward.44 Deter- urine sediment, providing an accessible specimen with diag- mining whether SARS-CoV-2 follows a similar dynamic and nostic and predictive potential in terms of incidence of AKI its relationship to development of AKI could provide a power- and COVID-19–related mortality. Our study was not ful diagnostic tool. These considerations, together with addi- designed to determine whether SARS-CoV-2 kidney tropism tional variables like sex and age, should be addressed to directly causes AKI. This is a standing question requiring inform revised guidelines for care of patients with COVID- mechanistic studies in animal models or organoids directly 19 who have kidney involvement, in efforts to identify patients addressing this possibility. at higher risk and to better allocate scarce resources. 2526 JASN JASN 32: 2517–2528, 2021
www.jasn.org BASIC RESEARCH
DISCLOSURES Supplemental Figure 2. Starting amount of RNA purified from urine sedi-
ments for qRT-PCR.
P.A. Ortiz reports receiving research funding from the American Heart Supplemental Figure 3. U-viral load in relation with method of sampling,
Association (AHA), National Institute of Diabetes and Digestive and Kidney ventilation and parameters of kidney injury.
Diseases (DK105818A1), and the NIH; and serving as the past chair on the Supplemental Figure 4. SARS-CoV-2 immunofluorescence in kidney biopsy.
AHA Kidney in Cardiovascular Diseases Council, on the editorial board of Supplemental Figure 5. Expression of nucleocapsid and ACE2 in cells shed
the American Journal of Physiology-Renal Physiology, as a scientific advisor in urine sediment from SARS-CoV-2 urine-positive patients.
Supplemental Figure 6. Kidney histopathology of COVID-19 patient with
for—or member of—Hypertension, and as a permanent member
AKI.
(2013–2019) of the NIH Study Section (HM). K. Umanath reports receiving
research funding from AstraZeneca, GlaxoSmithKline, ReCor Medical, and
Sentien; having consultancy agreements with AstraZeneca and ICON/Novo REFERENCES
Nordisk; Honoraria from Ardelyx; serving on the editorial board of Kidney
Medicine, Frontiers in Physiology – Renal and Epithelial Physiology, Journal 1. World Health Organization: W.H.O. Coronavirus disease 2019
of the American Association of Physicians of Indian Origin; and serving as (COVID-19): Situation report, 51, Geneva, Switzerland, World Health
vice president and on the board of directors of The Collaborative Study Organization, 2020
Group. J. Yee reports Consultancy Agreements with AstraZeneca, GLG; 2. Puelles VG, L€ utgehetmann M, Lindenmeyer MT, Sperhake JP, Wong
Ardelyx, EBSCO/Dynamed, Bayer; Ownership Interest in Vasc-Alert(TM); MN, Allweiss L, et al.: Multiorgan and renal tropism of SARS-CoV-2.
Honoraria from AstraZeneca, Fresenius Medical Corporation, North Amer- N Engl J Med 383: 590–592, 2020
ica, Cara Therapeutics, Bayer, Gerson Lehman Group, AlphaSights, Ardelyx; 3. Su H, Yang M, Wan C, Yi LX, Tang F, Zhu HY, et al.: Renal histopath-
Patents and Inventions with Vasc-Alert(TM); Scientific Advisor or Member- ological analysis of 26 postmortem findings of patients with COVID-19
ship AstraZeneca, Ardelyx, Bayer; and Other Interests/Relationships with in China. Kidney Int 98: 219–227, 2020
National Kidney Foundation, Editorial Board for Am J Kidney Dis, 4. Diao B, Wang C, Wang R, Feng Z, Tan Y, Wang H, et al.: Human kidney
EBSCO/DynaMed Editorial Board, Elsevier Clinical Key Author, Elsevier is a target for novel severe acute respiratory syndrome coronavirus 2
Section Editor, Ferri’s Clinical Advisor 2022, BMC Nephrology Editorial (SARS-CoV-2) infection. Nat Commun 12: 2506, 2021
Board, Springer Heart Failure Reviews Editorial Board, Am J Nephrol 5. Bradley BT, Maioli H, Johnston R, Chaudhry I, Fink SL, Xu H, et al.: His-
Nephrology Editorial Board, and Journal of Onco-Nephrology Editorial topathology and ultrastructural findings of fatal COVID-19 infections
Board. All remaining authors have nothing to disclose. in Washington State: a case series. Lancet 396: 320–332, 2020
6. Shao M, Li X, Liu F, Tian T, Luo J, Yang Y: Acute kidney injury is asso-
ciated with severe infection and fatality in patients with COVID-19: A
FUNDING systematic review and meta-analysis of 40 studies and 24,527
patients. Pharmacol Res 161: 105107, 2020
P.A. Ortiz is supported, in part, by NIH grant RO1 DK105818A1. This 7. Palmieri L, Vanacore N, Donfrancesco C, Lo Noce C, Canevelli M,
study was supported, in part, by Henry Ford Health System grant A30960. Punzo O, et al.; Italian National Institute of Health COVID-19 Mortality
Group: Clinical characteristics of hospitalized individuals dying with
COVID-19 by age group in Italy. J Gerontol A Biol Sci Med Sci 75:
1796–1800, 2020
ACKNOWLEDGMENTS 8. Mohamed MM, Lukitsch I, Torres-Ortiz AE, Walker JB, Varghese V,
Hernandez-Arroyo CF, et al.: Acute kidney injury associated with coro-
The following reagent was deposited by the CDC and obtained through BEI navirus disease 2019 in urban New Orleans. Kidney360 1: 614–622,
Resources, NIAID, NIH: Quantitative PCR (qPCR) ControlA from Heat- 2020
Inactivated SARS-Related Coronavirus 2, Isolate USA-WA1/2020, NR 52347. 9. Arentz M, Yim E, Klaff L, Lokhandwala S, Riedo FX, Chong M, et al.:
P.A. Ortiz formulated the hypothesis; P.S. Caceres and P.A. Ortiz Characteristics and outcomes of 21 critically ill patients with COVID-
designed the experiments and wrote the manuscript; P.S. Caceres analyzed 19 in Washington State. JAMA 323: 1612–1614, 2020
the data and prepared figures; G. Savickas, S.L. Murray, M.N. Khan and S. 10. Cummings MJ, Baldwin MR, Abrams D, Jacobson SD, Meyer BJ,
Sarkar recruited patients, reviewed medical records, and compiled Table 1; Balough EM, et al.: Epidemiology, clinical course, and outcomes of
P.S. Caceres, D. Maskey, and J. Fitzgerald performed RT-PCRs; S. Sarkar critically ill adults with COVID-19 in New York City: A prospective
analyzed ACRs; K. Umanath, J. Uduman, J. Yee, and Y. Sharma performed cohort study. Lancet 395: 1763–1770, 2020
the AKI adjudications, established the patient selection criteria, and contrib- 11. Pelayo J, Lo KB, Bhargav R, Gul F, Peterson E, DeJoy Iii R, et al.: Clin-
uted to the outline of the manuscript; T.-D. Liao and P.A. Ortiz performed ical characteristics and outcomes of community- and hospital-
immunofluorescences; A.M. Levin performed statistical analysis and pre- acquired acute kidney injury with COVID-19 in a US inner city hospital
pared the inpatient mortality figure; S. Bolin performed virus infectivity system. Cardiorenal Med 10: 223–231, 2020
assays; A.H. Ormsby processed the kidney biopsy specimens; and all authors 12. Ali H, Daoud A, Mohamed MM, Salim SA, Yessayan L, Baharani J, et
contributed to the final edited version of the manuscript. al.: Survival rate in acute kidney injury superimposed COVID-19
patients: A systematic review and meta-analysis. Ren Fail 42: 393–
397, 2020
13. Wang X, Fang X, Cai Z, Wu X, Gao X, Min J, et al.: Comorbid chronic
SUPPLEMENTAL MATERIAL diseases and acute organ injuries are strongly correlated with disease
severity and mortality among COVID-19 patients: A systemic review
This article contains the following supplemental material online at http:// and meta-analysis. Research (Wash D C) 2020: 2402961, 2020
jasn.asnjournals.org/lookup/suppl/doi:10.1681/ASN.2021010059/-/ 14. Lim JH, Park SH, Jeon Y, Cho JH, Jung HY, Choi JY, et al.: Fatal out-
DCSupplemental. comes of COVID-19 in patients with severe acute kidney injury. J Clin
Supplemental Table 1. Clinical risk factors for patients with U-viral load Med 9: 1718, 2020
higher than 5140 copies/ng RNA. 15. Braun F, L€ utgehetmann M, Pfefferle S, Wong MN, Carsten A, Linden-
Supplemental Figure 1. RT-PCR amplification in urine sediments and meyer MT, et al.: SARS-CoV-2 renal tropism associates with acute kid-
SARS-CoV-2 standard curve. ney injury. Lancet 396: 597–598, 2020
JASN 32: 2517–2528, 2021 Urine SARS-CoV-2 and Kidney Injury 2527BASIC RESEARCH www.jasn.org
16. Hanley B, Naresh KN, Roufosse C, Nicholson AG, Weir J, Cooke GS, et 31. Larsen CP, Bourne TD, Wilson JD, Saqqa O, Sharshir MA: Collapsing
al.: Histopathological findings and viral tropism in UK patients with glomerulopathy in a patient with coronavirus disease 2019 (COVID-
severe fatal COVID-19: A post-mortem study. Lancet Microbe 1: 19). Kidney Int Rep 5: 935–939, 2020
e245–e253, 2020 32. Farkash EA, Wilson AM, Jentzen JM: Ultrastructural evidence for direct
17. Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, et al.: Detection of SARS- renal infection with SARS-CoV-2. J Am Soc Neprhol 31: 1683–1687,
CoV-2 in different types of clinical specimens. JAMA 323: 1843–1844, 2020
2020 33. Miller SE, Brealey JK: Visualization of putative coronavirus in kidney.
18. W€ olfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, M€ uller Kidney Int 98: 231–232, 2020
MA, et al.: Virological assessment of hospitalized patients with 34. Roufosse C, Curtis E, Moran L, Hollinshead M, Cook T, Hanley B, et al.:
COVID-2019. Nature 581: 465–469, 2020 Electron microscopic investigations in COVID-19: Not all crowns are
19. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al.; China Medical coronas. Kidney Int 98: 505–506, 2020
Treatment Expert Group for Covid-19: Clinical characteristics of coro- 35. Xia S, Wu M, Chen S, Zhang T, Ye L, Liu J, et al.: Long term culture of
navirus disease 2019 in China. N Engl J Med 382: 1708–1720, 2020 human kidney proximal tubule epithelial cells maintains lineage func-
20. Peng L, Liu J, Xu W, Luo Q, Chen D, Lei Z, et al.: SARS-CoV-2 can be tions and serves as an ex vivo model for coronavirus associated kidney
detected in urine, blood, anal swabs, and oropharyngeal swabs speci- injury. Virol Sin 35: 311–320, 2020
mens. J Med Virol 92: 1676–1680, 2020 36. Monteil V, Kwon H, Prado P, Hagelkr€ uys A, Wimmer RA, Stahl M, et al.:
21. Frithiof R, Bergqvist A, J€ arhult JD, Lipcsey M, Hultstr€
om M: Presence Inhibition of SARS-CoV-2 infections in engineered human tissues
of SARS-CoV-2 in urine is rare and not associated with acute kidney using clinical-grade soluble human ACE2. Cell 181: 905–913.e7, 2020
injury in critically ill COVID-19 patients. Crit Care 24: 587, 2020 37. Werion A, Belkhir L, Perrot M, Schmit G, Aydin S, Chen Z, et al.; Clin-
22. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al.: A pneu- iques universitaires Saint-Luc (CUSL) COVID-19 Research Group:
monia outbreak associated with a new coronavirus of probable bat ori- SARS-CoV-2 causes a specific dysfunction of the kidney proximal
gin. Nature 579: 270–273, 2020 tubule. Kidney Int 98: 1296–1307, 2020
23. Bouhaddou M, Memon D, Meyer B, White KM, Rezelj VV, Correa Mar- 38. Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H: Tis-
rero M, et al.: The global phosphorylation landscape of SARS-CoV-2 sue distribution of ACE2 protein, the functional receptor for SARS
infection. Cell 182: 685–712.e19, 2020 coronavirus. A first step in understanding SARS pathogenesis. J Pathol
24. Hosier H, Farhadian SF, Morotti RA, Deshmukh U, Lu-Culligan A, 203: 631–637, 2004
Campbell KH, et al.: SARS-CoV-2 infection of the placenta. J Clin 39. Donoghue M, Hsieh F, Baronas E, Godbout K, Gosselin M, Stagliano
Invest 130: 4947–4953, 2020 N, et al.: A novel angiotensin-converting enzyme-related carboxypep-
25. Zhao B, Ni C, Gao R, Wang Y, Yang L, Wei J, et al.: Recapitulation of tidase (ACE2) converts angiotensin I to angiotensin 1-9. Circ Res 87:
SARS-CoV-2 infection and cholangiocyte damage with human liver E1–E9, 2000
ductal organoids. Protein Cell 11: 771–775, 2020 40. Wilson PC, Wu H, Kirita Y, Uchimura K, Ledru N, Rennke HG, et al.: The
26. Hernandez-Arroyo CF, Varghese V, Mohamed MMB, Velez JCQ: Uri- single-cell transcriptomic landscape of early human diabetic nephrop-
nary sediment microscopy in acute kidney injury associated with athy. Proc Natl Acad Sci U S A 116: 19619–19625, 2019
COVID-19. Kidney360 1: 819–823, 2020 41. Wu H, Uchimura K, Donnelly EL, Kirita Y, Morris SA, Humphreys BD:
27. Wang L, Li X, Chen H, Yan S, Li D, Li Y, et al.: Coronavirus disease 19 Comparative analysis and refinement of human PSC-derived kidney
infection does not result in acute kidney injury: An analysis of 116 hos- organoid differentiation with single-cell transcriptomics. Cell Stem
pitalized patients from Wuhan, China. Am J Nephrol 51: 343–348, Cell 23: 869–881.e8, 2018
2020 42. Price-Haywood EG, Burton J, Fort D, Seoane L: Hospitalization and
28. Corman VM, Landt O, Kaiser M, Molenkamp R, Meijer A, Chu DK, et mortality among black patients and white patients with Covid-19. N
al.: Detection of 2019 novel coronavirus (2019-nCoV) by real-time Engl J Med 382: 2534–2543, 2020
RT-PCR. Euro Surveill 25: 2000045, 2020 43. Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL, et al.;
29. Prendecki M, Clarke C, Cairns T, Cook T, Roufosse C, Thomas D, et al.: Northwell COVID-19 Research Consortium; Northwell Nephrology
Anti-glomerular basement membrane disease during the COVID-19 COVID-19 Research Consortium: Acute kidney injury in patients hos-
pandemic. Kidney Int 98: 780–781, 2020 pitalized with COVID-19. Kidney Int 98: 209–218, 2020
30. Dorward DA, Russell CD, Um IH, Elshani M, Armstrong SD, Penrice- 44. Xu D, Zhang Z, Jin L, Chu F, Mao Y, Wang H, et al.: Persistent shedding
Randal R, et al.: Tissue-specific tolerance in fatal Covid-19. Am J of viable SARS-CoV in urine and stool of SARS patients during the con-
Respir Crit Care Med 203: 192–201, 2021 valescent phase. Eur J Clin Microbiol Infect Dis 24: 165–171, 2005
AFFILIATIONS
1
Hypertension and Vascular Research Division, Department of Internal Medicine, Henry Ford Hospital, Detroit, Michigan
2
Department of Physiology, Wayne State University, Detroit, Michigan
3
Translational and Clinical Research Center, Henry Ford Hospital, Detroit, Michigan
4
Division of Nephrology and Hypertension, Department of Internal Medicine, Henry Ford Hospital, Detroit, Michigan
5
Division of Nephrology and Hypertension, Wayne State University, Detroit, Michigan
6
Veterinary Diagnostic Laboratory, Michigan State University, Lansing, Michigan
7
Division of Biostatistics, Department of Public Health Sciences, Henry Ford Hospital, Detroit, Michigan
8
Center for Bioinformatics, Henry Ford Hospital, Detroit, Michigan
9
Department of Orthopedic Surgery, Bone and Joint Center, Henry Ford Hospital, Detroit, Michigan
10
Department of Pathology and Laboratory Medicine, Henry Ford Hospital, Detroit, Michigan
2528 JASN JASN 32: 2517–2528, 2021You can also read