Haemophilus parainfluenzae endocarditis presenting with symptoms of COVID-19
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Case report
BMJ Case Rep: first published as 10.1136/bcr-2021-245210 on 25 August 2021. Downloaded from http://casereports.bmj.com/ on December 16, 2021 by guest. Protected by copyright.
Haemophilus parainfluenzae endocarditis presenting
with symptoms of COVID-19
Laurie C Finch ,1 Spiro Gerdzhikov,2 Robert Buttery3,4
1
Critical Care Centre, North SUMMARY this patient’s original symptoms, facilitated the H.
West Anglia NHS Foundation A young man presented early in the UK’s second parainfluenzae bacteraemia or biased clinical assess-
Trust, Huntingdon, UK COVID-19 pandemic surge with a twelve-day history ment and management.1 4
2
Department of Anaesthesia,
of fever, dry cough, breathlessness, myalgia and loss
North West Anglia NHS
of smell and taste. His chest X-ray showed bilateral
Foundation Trust, Huntingdon, CASE PRESENTATION
UK ground-glass opacities. He was treated for COVID-19
A young man was brought by ambulance to the
3
Department of Respiratory pneumonitis but covered for bacterial infection with
emergency department (ED) of a district general
Medicine, North West Anglia antibiotics. He developed shock and respiratory failure,
hospital early in the UK’s second COVID-19
NHS Foundation Trust, requiring vasopressors and continuous positive airway pandemic surge. He had a 12-day history of fever,
Huntingdon, UK pressure. He improved but experienced transient visual dry cough, exertional breathlessness, light headed-
4
Department of Respiratory disturbances and headache. Nasopharyngeal swabs
Medicine, Royal Papworth ness, myalgia, fatigue, reduced appetite and loss of
and antibody tests for COVID-19 were negative. Blood smell and taste. He described chest ‘tightness’, head-
Hospital NHS Foundation Trust,
cultures grew Haemophilus parainfluenzae. A new ache, photophobia, visual disturbances, vomiting
Cambridge, UK
murmur prompted an echocardiogram. This confirmed a and diarrhoea. He had no known COVID-19
Correspondence to large, mobile mitral valve vegetation. An MRI of the brain contacts but had visited a UK city 2 days prior to
Dr Laurie C Finch; showed bilateral embolic infarcts. He underwent urgent becoming unwell. A nasopharyngeal COVID-19
laurie.finch1@nhs.net mitral valve repair and made an excellent recovery. swab collected 5 days into his illness had returned
Whether COVID-19 caused his presenting symptoms ‘indeterminate’.
Accepted 10 August 2021 or facilitated the bacteraemia remains unclear. It seems He was deteriorating at home and called NHS
more likely that infective endocarditis masqueraded as 111, which triggered an ambulance call-out. Para-
COVID-19. Clinicians should be aware of how context of medics found him to be tachypnoeic, tachycardic,
the pandemic can bias diagnostic reasoning. hypotensive and febrile (respiratory rate: 20
breaths/min, SpO2: 96% on air, heart rate: 124
beats/min, blood pressure (BP): 101/62 mmHg,
BACKGROUND temperature: 39.2°C).
With a varied and often insidious clinical course, He had a history of seborrhoeic dermatitis and
infective endocarditis (IE) can be difficult to diag- multiple tooth extractions 13 years previously. He
nose but incidence is increasing globally, even in had never smoked or used intravenous drugs.
low-risk individuals.1–3 In ED he was persistently febrile and became
Streptococci, Staphylococci and Enterococci more hypotensive (BP: 71/40 mmHg) but main-
together comprise over 90% of culture- positive tained saturations of 95% on air. On examination
IE.1 8.5% is caused by organisms often found in the he had increased work of breathing and bilateral
blood, which rarely attack cardiac valves (eg. Pseu- lung crepitations. He was cyanotic and peripherally
domonas species).1 The remaining 1.5% is caused shut down with a capillary refill time of 4 seconds
by oral and respiratory tract commensal organisms and dry mucous membranes. Auscultation revealed
that rarely enter the circulation but are tropic to no heart murmur.
valve tissue when they do. These are the HACEK
organisms (Haemophilus species, Aggregatibacter INVESTIGATIONS
species, Cardiobacterium hominis, Eikenella corro- An arterial blood gas (ABG) on air confirmed
dens and Kingella species). Haemophilus parain- type-one respiratory failure (pH: 7.45, partial pres-
fluenzae is the most common, causing one third sure of oxygen (pO2): 4.9 kPa, partial pressure of
of HACEK IE.4 In comparison to non-HACEK IE, carbon dioxide (pCO2): 4.0 kPa, SpO2: 93%, lactate:
HACEK organisms tend to affect younger people 1.6 mmol/L). An electrocardiogram (ECG) showed
(often with no cardiac history)1 and carry a higher sinus rhythm with right axis deviation (figure 1).
risk of haemorrhagic stroke but a better overall A chest X- ray (CXR) was reported as extensive,
prognosis.4 Diagnosing HACEK IE is notoriously bilateral ground-glass opacification with mid and
© BMJ Publishing Group
Limited 2021. No commercial
challenging, with only one third of cases confirmed lower zone predominance (figure 2), concerning for
re-use. See rights and within 4 days of hospital admission.1 COVID-19 pneumonitis but potentially suggestive
permissions. Published by BMJ. This case reminds us to consider IE in patients of pulmonary oedema.
with sepsis and signs of reduced cardiac output. It He had raised inflammatory markers (C-reactive
To cite: Finch LC,
Gerdzhikov S, Buttery R. BMJ highlights some classic features of HACEK IE and protein (CRP): 247 mg/L, white cell count (WCC):
Case Rep 2021;14:e245210. the value of blood cultures drawn prior to antibiotic 15.9×109/L, neutrophil count: 14.6×109/L) but
doi:10.1136/bcr-2021- administration. The clinical course also raises fasci- a lymphopenia (lymphocyte count: 0.4×109/L),
245210 nating questions as to whether COVID-19 caused normocytic anaemia (haemoglobin: 123 g/L, mean
Finch LC, et al. BMJ Case Rep 2021;14:e245210. doi:10.1136/bcr-2021-245210 1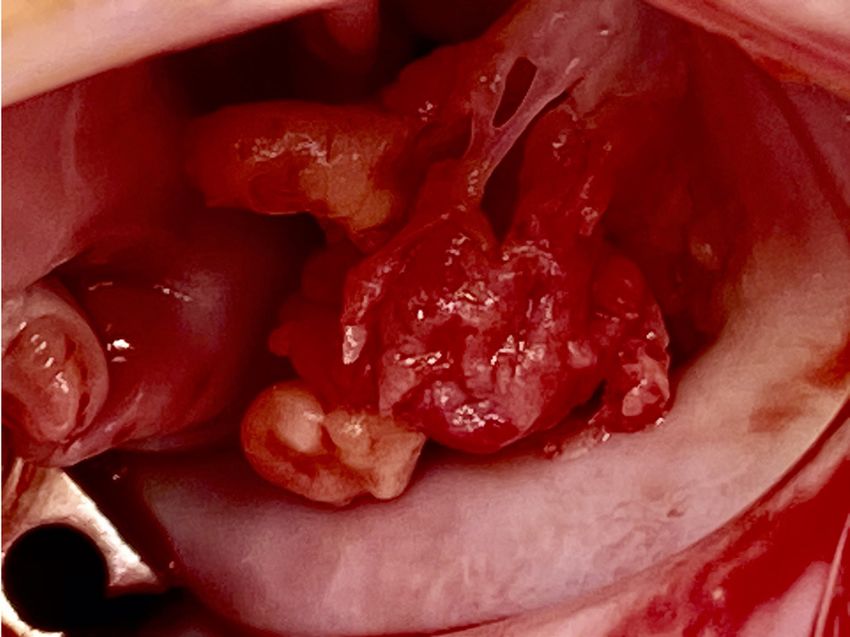
Case report
BMJ Case Rep: first published as 10.1136/bcr-2021-245210 on 25 August 2021. Downloaded from http://casereports.bmj.com/ on December 16, 2021 by guest. Protected by copyright.
Figure 1 Admission 12-lead ECG showing sinus rhythm with right
axis deviation.
cell volume: 82.3 fL) and thrombocytopenia (platelet count:
129×109/L). He was also hyponatraemic (Na: 127 mmol/L). Figure 3 Anterior–posterior chest X-ray from day 3 of admission
There were no prior baseline renal function tests for compar- showing worsening bilateral mid and lower zone patchy shadowing and
ison but creatinine and urea were probably raised given his slim upper lobe diversion.
build (creatinine: 82µmol/L, urea: 7.5 mmol/L). Liver function
tests were also mildly deranged (alanine transaminase: 57 IU/L,
Nasopharyngeal swabs for COVID-19 PCR on day 12 and
bilirubin: 21 µmol/L, alkaline phosphatase: 96 IU/L). A D-dimer
day 14 of symptoms were negative, as was COVID-19 antibody
was raised (845 ng/mL). A urine dip showed a trace of blood
serology on day 13.
but was negative for leucocytes and nitrites. Blood cultures were
A CXR on day 3 of admission showed worsening bilateral
taken.
mid and lower zone patchy shadowing and upper lobe diversion
His hypotension was refractory to fluid resuscitation. A
(figure 3).
bedside echocardiogram in ED showed no evidence of right
On day 5 of admission, blood cultures returned positive for H.
heart failure, although views were suboptimal. Valves were not
influenzae (sensitive to co-amoxiclav and tetracyclines). This was
assessed.
later amended to H. parainfluenzae.
A repeat ABG on oxygen at 15 L/min via non re-breathe mask
A loud pansystolic murmur prompted a formal echocardio-
showed severe type- one respiratory failure (pH: 7.43, pO2: gram. This revealed a large, friable, mobile mass (1.5×1.5 cm)
8.8 kPa, pCO2: 4.4 kPa). on the anterior mitral valve leaflet causing torrential mitral
regurgitation (figures 4 and 5).
A computed tomography (CT) scan of the chest, abdomen and
pelvis (figure 6) showed bilateral pleural effusions with atelec-
tasis and lower lobe ground-glass densities but no evidence of
distant emboli.
Magnetic resonance imaging (MRI) of the brain on day 9 of
admission was used to investigate recurrent episodes of right
frontal headache and visual disturbance (figure 7). This showed
Figure 2 Admission anterior–posterior chest X-ray reported as Figure 4 Echocardiogram four-chamber view showing the mitral valve
showing bilateral ground-glass opacities. vegetation.
2 Finch LC, et al. BMJ Case Rep 2021;14:e245210. doi:10.1136/bcr-2021-245210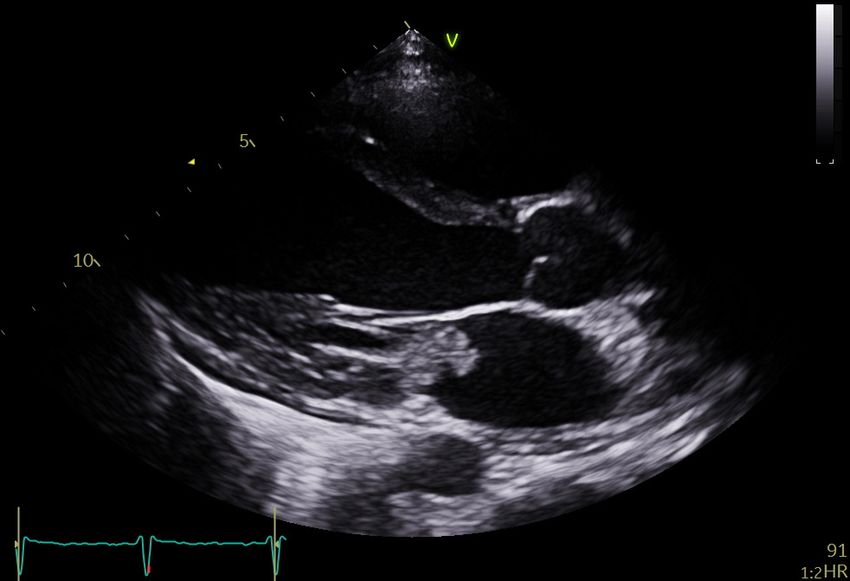
Case report
BMJ Case Rep: first published as 10.1136/bcr-2021-245210 on 25 August 2021. Downloaded from http://casereports.bmj.com/ on December 16, 2021 by guest. Protected by copyright.
Figure 5 Echocardiogram parasternal long-axis view showing the
mitral valve vegetation.
small foci of restricted diffusion in the supratentorial brain
parenchyma bilaterally, suggestive of embolic infarcts.
A repeat MRI of the brain for similar symptoms postopera-
tively showed resolution of these lesions but new microhaemor-
rhages in the left thalamus, right parietal lobe and possibly the
left superior frontal white matter. Figure 7 MRI of the brain showing small foci of restricted diffusion in
the supratentorial brain parenchyma bilaterally, suggestive of embolic
DIFFERENTIAL DIAGNOSIS infarcts.
This previously healthy, young man presented in shock. Deter-
mining the type of shock was the initial priority. The presenting
symptoms, including the cardinal symptoms of COVID-19, and CRP trended steeply down with initial therapy, but the leuco-
bilateral CXR changes were considered consistent with a respi- cytosis and lymphopenia persisted. CRP began climbing again
ratory viral syndrome. This prompted a working diagnosis of from day 8 of admission, which could have suggested an ongoing
septic shock with COVID-19 pneumonitis. source of infection, although he remained afebrile on antibiotics
However, the examination findings could suggest a state of and his overall clinical state improved.
reduced cardiac output such as distributive or cardiogenic shock. His transient right frontal headache and visual disturbances,
When his blood pressure failed to improve, a bedside echo including a black shadow over the right visual field, continued,
helped rule out cardiac decompensation from tamponade or a although there was no focal deficit at the time of neurological
large pulmonary embolism. examination.
On day 8 of admission, he complained of intermittent left
lateral chest discomfort. This, alongside the unusual blood
culture result, rising inflammatory markers and transient neuro-
logical symptoms prompted a repeat examination. This revealed
a loud pansystolic murmur and a splinter haemorrhage. A formal
echocardiogram confirmed the diagnosis of mitral valve IE.
Reassessment of the blood culture samples confirmed H. parain-
fluenzae. The same organism was later identified on intraopera-
tive tissue samples sent for 16S PCR.
TREATMENT
Initial treatment included oxygen via a non re-breathe mask,
liberal intravenous fluid resuscitation and antibiotics. COVID-19
pneumonitis was treated with dexamethasone, remdesivir and
intermediate-dose dalteparin thromboprophylaxis. Intravenous
co-amoxiclav and clarithromycin were soon escalated to pipera-
cillin and tazobactam.
Over the first 3 days he required continuous positive airway
pressure and intermittent vasopressor support with peripheral
metaraminol on ICU. He improved and, by day 7, was weaned
off oxygen and mobilising well.
Once H. parainfluenzae was confirmed, antibiotics were
Figure 6 CT image of the chest showing atelectasis and lower lobe changed to ceftriaxone (2g twice daily) and the isolate reported
ground-glass densities. to Public Health England.
Finch LC, et al. BMJ Case Rep 2021;14:e245210. doi:10.1136/bcr-2021-245210 3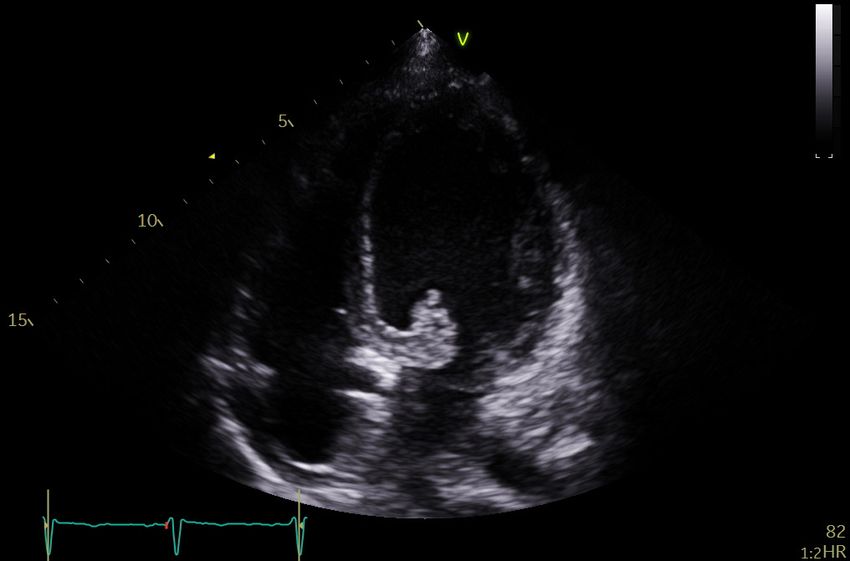
Case report
BMJ Case Rep: first published as 10.1136/bcr-2021-245210 on 25 August 2021. Downloaded from http://casereports.bmj.com/ on December 16, 2021 by guest. Protected by copyright.
Figure 10 Echocardiogram image showing the repaired mitral valve
and annular ring in a parasternal short-axis view (3 weeks post surgery).
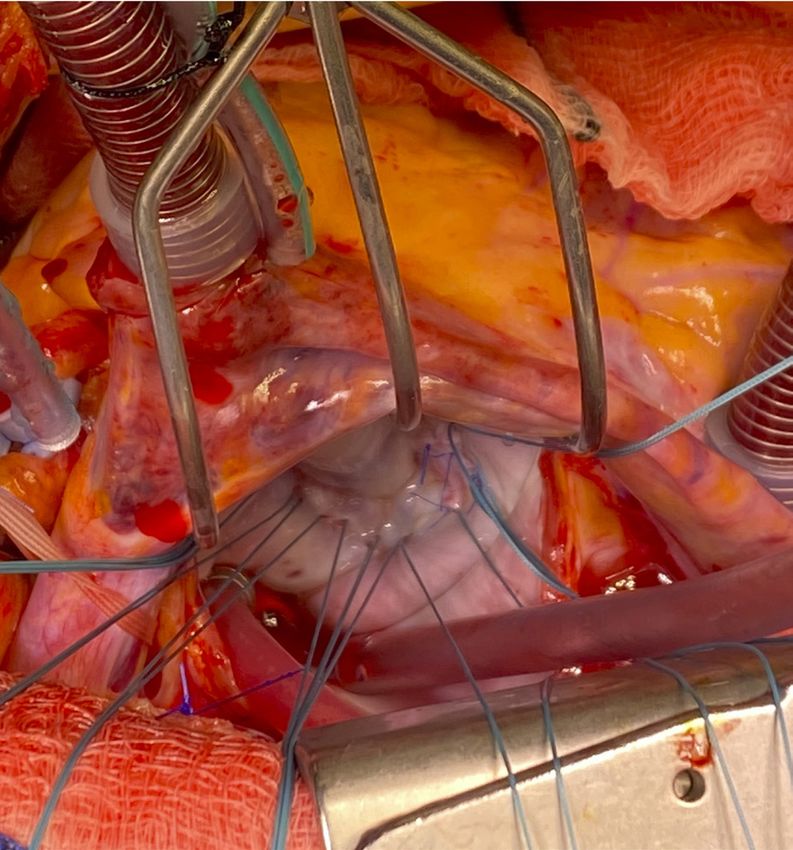
Figure 8 Intraoperative photo showing the large vegetation on the
anterior mitral valve leaflet.
embolic cause. He awaits a neurology opinion as to whether
these could represent migrainous auras. He returned to work.
The echocardiogram findings, recurrent neurological symp-
An echocardiogram 3 weeks post-operatively confirmed a well-
toms and MRI evidence of cerebral emboli prompted an urgent
functioning mitral valve (figures 10 and 11). He was followed-up
interhospital transfer for cardiac surgery. He underwent mitral
6 weeks post discharge in cardiology and cardiac surgical clinics.
valve repair on day 12 of admission (figures 8 and 9). Postoper-
ative blood cultures were negative.
An echocardiogram 5 days post-operatively confirmed good
DISCUSSION
Most septic patients are intravascularly depleted and require
placement of the annuloplasty ring, no mitral regurgitation and
fluid resuscitation. However, this case highlights pulmonary
mildly impaired left and right ventricular systolic function.
oedema and cardiogenic shock as important differential diag-
He completed a further 6 weeks of postoperative intrave-
noses in patients who remain hypotensive or become increas-
nous ceftriaxone on advice of the microbiology team. He
ingly hypoxic following fluid resuscitation. The combination
was also commenced on aspirin, omeprazole and low-dose
of sepsis and cardiogenic shock should raise suspicion of IE.
bisoprolol.
This case demonstrates some key features of HACEK IE. In
comparison to non-HACEK IE, it takes longer to diagnose,1
OUTCOME AND FOLLOW-UP
affects younger people and those with no history of cardiac
He made an excellent recovery, suffering no persisting neuro-
disease,1 and carries a higher risk of stroke and intracranial
logical deficit. He continues to experience self-resolving visual
haemorrhage.4 Mitral valve HACEK IE is particularly associated
disturbances (floaters and shadows) for which neither ophthal-
with stroke.4 The course of HACEK IE is classically considered
mologists or stroke physicians are convinced of a vascular or
insidious. However, this case mirrors other reports5 6 of H. para-
influenzae acting aggressively in previously healthy people.
This patient’s dental history was his only risk factor for IE.
However, this detail came to light only after the diagnosis
was made. Physicians rarely delve into dental histories and
community dental work rarely appears on general practitioner
Figure 11 Echocardiogram image showing the repaired mitral valve
Figure 9 Intraoperative photo showing the repaired mitral valve. and annular ring in a parasternal long-axis view (3 weeks post surgery).
4 Finch LC, et al. BMJ Case Rep 2021;14:e245210. doi:10.1136/bcr-2021-245210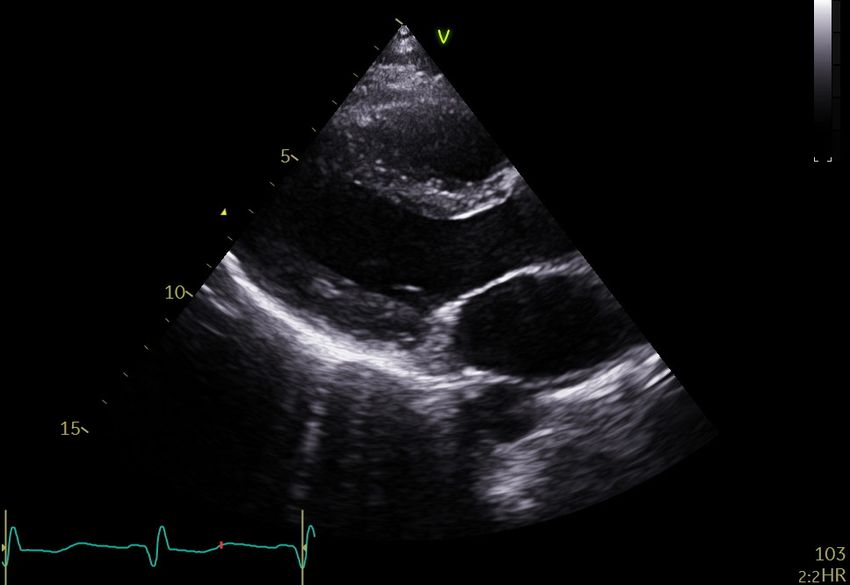
Case report
BMJ Case Rep: first published as 10.1136/bcr-2021-245210 on 25 August 2021. Downloaded from http://casereports.bmj.com/ on December 16, 2021 by guest. Protected by copyright.
summaries. Asking patients with sepsis of unknown origin about COVID-19 prevalence should affect how diagnostic tests
dental work could help raise suspicion of IE. are interpreted, although this is a challenge in practice when
HACEK organisms pose a challenge in the laboratory. This prevalence is changing rapidly. Tests for diseases with a high
patient’s blood culture was initially reported positive for H. prevalence carry a lower negative predictive value and, there-
influenzae (the most common of the Haemophilus species) fore, a higher chance of false negatives. COVID-19 preva-
rather than H. parainfluenzae. It is possible that a request lence was relatively low when this patient presented (only
form suggesting the sample was part of a work-up for pneu- one COVID-19positive patient was admitted in our hospital
monia contributed to this. The presence of cytochrome oxidase at the time). In this context, a negative swab result is more
confirms Haemophilus species growing on chocolate agar.7 reliable; so stronger clinical suspicion is needed to continue
However, it is not possible to differentiate Haemophilus species to treat for COVID-19.
on gram stain appearance or colonial morphology.8 9 Classically,
porphyrin synthesis testing has been used to exploit the ability Learning points
of certain Haemophilus species (including H. parainfluenzae)
to produce porphyrins using the enzyme porphobilinogen ►► Infective endocarditis is a rare but important differential
synthase.8 9 However, newer but expensive 16S rRNA PCR diagnosis in patients with infection and signs of reduced
testing and mass spectrometry can now rapidly and reliably cardiac output or cardiogenic shock.
differentiate Haemophilus species and other HACEK organisms ►► Neurological symptoms in the context of infection can
without the need for culture.9 suggest an embolic process.
Confirmed H. parainfluenzae bacteraemia is strongly associ- ►► Haemophilus parainfluenzae is the most common HACEK
ated with endocarditis. The positive predictive values of HACEK organism to cause endocarditis and can form large mitral
and H. parainfluenzae bacteraemias for endocarditis are 60% valve vegetations.
and 55%, respectively.10 ►► H. parainfluenzae can act in an aggressive manner to cause
This patient presented with symptoms of COVID-19 in the shock in young, healthy people.
early stages of the second pandemic ‘surge’ in the UK. However, ►► Clinicians should be astute to diagnostic framing bias and
COVID-19 antigen and antibody tests were negative. Whether base rate neglect as the pretest probability of COVID-19
COVID-19 facilitates translocation of H. parainfluenzae from infection changes with pandemic surges.
the nasopharynx into the circulation is unknown, although H.
parainfluenzae IE has been associated with other coronaviruses.6
Whether the mitral valve vegetation was formed at presen- Acknowledgements Jagadeesan M (MJ) reviewed the microbiological details,
advising on the antimicrobial treatment of Haemophilus parainfluenzae infective
tation is unclear. The initial bedside echo was a brief assess-
endocarditis and the technicalities of identifying Haemophilus species in the
ment in the ED to rule out acute right heart decompensation
laboratory. Koshy G (GK) advised on the relevant clinical reasoning from a critical
and tamponade. The valves were not commented on and it care perspective. Our thanks to Wells F (FW) for kindly providing the intraoperative
has not been possible to retrieve these images for retrospec- photos. Many thanks to the patient for supporting this work. LCF, SG, RB, MJ, GK and
tive review. There may have been poor acoustic windows FW were all involved in the patient’s care.
on a tachycardic heart or perhaps the clinical concern of a
Contributors LCF drove the conception of the work, gathered the clinical details
massive pulmonary embolus (in the context of sepsis from and images, drafted the report and revised the manuscript. SG provided critical
COVID-19) distracted the team from alternatives. IE was not review and reviewed the final manuscript. RB provided critical review, advised on the
among the differential diagnoses at that stage, particularly as use of figures, edited the final manuscript and reviewed revisions.
no murmur had been identified. In hindsight, following up Funding The authors have not declared a specific grant for this research from any
sooner with a formal echo may have expedited the diagnosis. funding agency in the public, commercial or not-for-profit sectors.
However, the presentation and initial response to treatment Competing interests None declared.
was thought in keeping with sepsis from COVID-19 pneumo- Patient consent for publication Obtained.
nitis. It was only after de-escalation to oral antibiotics that
Provenance and peer review Not commissioned; externally peer reviewed.
clinical signs of ongoing systemic infection became apparent.
Interestingly, the CRP and WCC fell steeply over the first This article is made freely available for use in accordance with BMJ’s website
terms and conditions for the duration of the covid-19 pandemic or until otherwise
3 days of admission. The CRP continued to fall until day 9, determined by BMJ. You may use, download and print the article for any lawful,
approaching the upper limit of normal, whereas the leucocy- non-commercial purpose (including text and data mining) provided that all copyright
tosis plateaued from day 5 onwards. The CRP trend, in the notices and trade marks are retained.
context of an overall clinical improvement, may have given
ORCID iD
false reassurance. Laurie C Finch http://orcid.org/0000-0001-9196-1648
Whether or not this patient had COVID-19, we perceive the
potential for the pandemic to influence diagnostic reasoning.
Patients are understandably alert to symptoms of COVID-19 REFERENCES
and professionals rightly see case recognition as the key to 1 Limonta S, Cambau E, Erpelding M-L, et al. Infective endocarditis related to unusual
breaking chains of infection. As such, COVID-19 was the microorganisms: a prospective population-based study. Open Forum Infect Dis
main concern from this patient’s call to NHS 111 onwards. 2020;7:ofaa127.
2 Dayer MJ, Jones S, Prendergast B, et al. Incidence of infective endocarditis in England,
Framing biases (eg. in spoken handovers or on request forms 2000-13: a secular trend, interrupted time-series analysis. Lancet 2015;385:1219–28.
for investigations requiring subjective analysis such as CXRs) 3 Pant S, Patel NJ, Deshmukh A, et al. Trends in infective endocarditis incidence,
could have diverted attention from alternative diagnoses. microbiology, and valve replacement in the United States from 2000 to 2011. J Am
Base rate neglect11 could also have played a part, given that, Coll Cardiol 2015;65:2070–6.
from a statistical standpoint, the chance this man had COVID-19 4 Chambers ST, Murdoch D, Morris A, et al. Hacek infective endocarditis: characteristics
and outcomes from a large, multi-national cohort. PLoS One 2013;8:e63181.
pneumonitis requiring admission was small. A study of 20 000 5 McCann N, Barakat MF, Schafer F. An aggressive form of Haemophilus parainfluenzae
patients admitted with COVID-19 during the first pandemic infective endocarditis presenting with limb weakness. BMJ Case Rep 2018;2018.
surge in the UK captured only 85 men aged 25–29 years.12 doi:10.1136/bcr-2017-223775. [Epub ahead of print: 04 Jun 2018].
Finch LC, et al. BMJ Case Rep 2021;14:e245210. doi:10.1136/bcr-2021-245210 5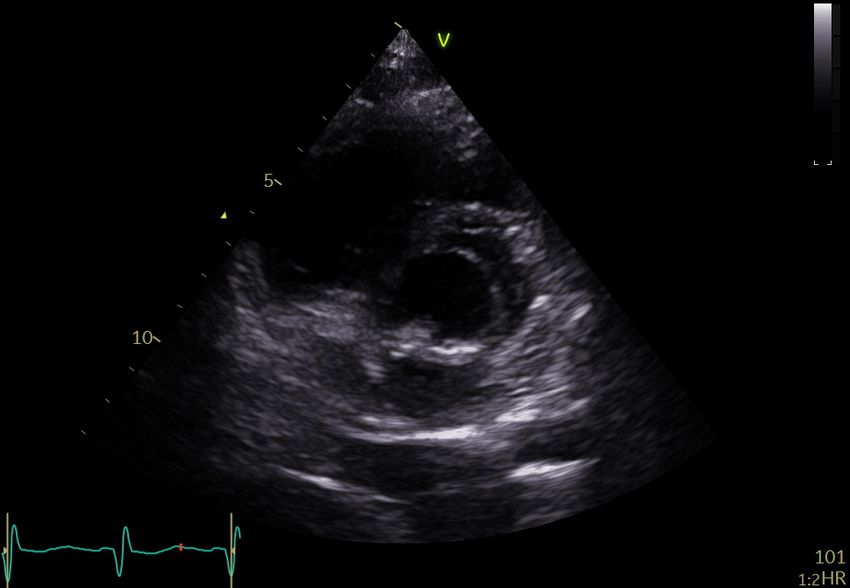
Case report
BMJ Case Rep: first published as 10.1136/bcr-2021-245210 on 25 August 2021. Downloaded from http://casereports.bmj.com/ on December 16, 2021 by guest. Protected by copyright.
6 De Castro A, Abu-Hishmeh M, El Husseini I, et al. Haemophilus parainfluenzae 9 Public Health England. Identification of Haemophilus species and the HACEK Group of
endocarditis with multiple cerebral emboli in a pregnant woman with coronavirus. Organisms. UK standards from microbiological investigations. Available: https://assets.
IDCases 2019;18:e00593. publishing.service.gov.uk/government/uploads/system/u ploads/attachment_data/file/
7 World Health Organization, Centers for Disease Control and Prevention (U.S.). 952488/UK_SMI_I D_12i4.pdf [Accessed Mar 2021].
Laboratory methods for the diagnosis of meningitis caused by Neisseria meningitidis, 10 Sen Yew H, Chambers ST, Roberts SA, et al. Association between HACEK bacteraemia
Streptococcus pneumoniae, and Haemophilus influenzae. 2nd Edn. Geneva, and endocarditis. J Med Microbiol 2014;63:892–5.
Switzerland: WHO Press, 2011: 87–98. https://apps.who.int/iris/handle/10665/70765 11 Watson J, Whiting PF, Brush JE. Interpreting a covid-19 test result. BMJ
8 Public Health England. Porphyrin synthesis (Ala) test. UK standards for microbiology 2020;369:1808. m.
investigations. Test procedures. Available: https://www.gov.uk/uk-standards-f or- 12 Docherty AB, Harrison EM, Green CA. Features of 20 133 UK patients in hospital
microbiology-investigations-smi-quality-and-consistency-in-clinical-laboratories with covid-19 using the ISARIC WHO clinical characterisation protocol: prospective
[Accessed Mar 2021]. observational cohort study. BMJ 2020;369:1985. m.
Copyright 2021 BMJ Publishing Group. All rights reserved. For permission to reuse any of this content visit
https://www.bmj.com/company/products-services/rights-and-licensing/permissions/
BMJ Case Report Fellows may re-use this article for personal use and teaching without any further permission.
Become a Fellow of BMJ Case Reports today and you can:
►► Submit as many cases as you like
►► Enjoy fast sympathetic peer review and rapid publication of accepted articles
►► Access all the published articles
►► Re-use any of the published material for personal use and teaching without further permission
Customer Service
If you have any further queries about your subscription, please contact our customer services team on +44 (0) 207111 1105 or via email at support@bmj.com.
Visit casereports.bmj.com for more articles like this and to become a Fellow
6 Finch LC, et al. BMJ Case Rep 2021;14:e245210. doi:10.1136/bcr-2021-245210You can also read

















































