Guide for Future Directions for the Addiction and OUD Treatment Ecosystem
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DISCUSSION PAPER
Guide for Future Directions for the Addiction and
OUD Treatment Ecosystem
R. Corey Waller, MD, MS, HMA Institute on Addiction; Kelly J. Clark, MD,
MBA, American Society of Addiction Medicine; Alex Woodruff, MPH, Partnered
Evidence-based Policy Resource Center; Jean Glossa, MD, MBA, Health
Management Associates; Andrey Ostrovsky, MD, Social Innovation Ventures;
and the Prevention, Treatment, and Recovery Working Group of the Action
Collaborative on Countering the U.S. Opioid Epidemic
April 5, 2021
DISCLAIMER: The views expressed in this paper are those of the authors and not necessarily of the authors’
organizations, the National Academy of Medicine (NAM), or the National Academies of Sciences, Engineer-
ing, and Medicine (the National Academies). The paper is intended to help inform and stimulate discussion.
It is not a report of the NAM or the National Academies.
Introduction and overdose continue to devastate people across the
United States—particularly Black, Latinx, Native Ameri-
The United States is in the midst of a multifactorial drug
can, LGBTQ+, and other traditionally marginalized
overdose and death epidemic. In 2020, over 80,000
communities. Models observing the course of the drug
deaths [15] in the U.S. were attributed to drug over-
overdose epidemic predict that without treatment ex-
dose, more than 50,000 of which were opioid-related.
pansion, another 400,000 people will die from over-
This is an increase of roughly 10 percent from 2018,
dose by 2025 [17]. The COVID-19 pandemic has further
when nearly twice the number of people died from a
exacerbated the opioid epidemic [52]. Many counties
drug overdose than died from HIV/AIDS at the peak of
across the U.S. have reported disruptions in public
that epidemic in 1995 [51]. According to recent esti-
health programs essential to people who use drugs,
mates, with nicotine included, over 35 million people
disruptions to transportation to treatment providers,
have a substance use disorder (SUD) (14 percent of the
and ongoing challenges in accessing evidence-based
U.S. population), and roughly 10.1 million people re-
care because of inadequate access to quality treat-
ported opioid misuse or any heroin use in the previous
ment providers [52]. Moreover, the SUD treatment sys-
year [14].
tem should be adapted to better engage and educate
The epidemic of drug, and especially opioid-related,
patient family members and support networks about
overdose deaths has been declared a national public
their loved ones’ treatment plans. There is a clear need
health emergency since 2017. What is needed to turn
for future-oriented strategies to build a robust addic-
the tide of this epidemic is a long-term, sustainable
tion treatment system that ensures widespread access
approach to preventing and managing addiction as
to treatment.
a chronic disease that will replace America’s current
Overcoming the drug overdose epidemic will require
approach of lurching from one crisis to the next. Co-
identifying and addressing critical gaps across the SUD
ordinated, compassionate, and science-based care is
treatment system. The majority of U.S. states, coun-
necessary. Despite research on the individual, soci-
ties, and municipalities do not strategically distribute
etal, carceral, and economic factors that created the
funding across the SUD treatment landscape. To ap-
epidemic, public policy and treatment resources have
propriately align funding to needs across the treat-
been unable to keep up with its trajectory [26]. The ef-
ment system and invest in training adequate numbers
fects of drug use, ill-informed drug policies, addiction,
of new providers of multiple disciplines, the following
Perspectives | Expert Voices in Health & Health Care
DISCUSSION PAPER
are needed: a technical assessment of the local SUD ment of opioid use disorder (OUD)—the major driver
treatment system and administrative time to contract of overdose related deaths.
with state vendors; development of data-release pro-
cesses; and organization of the reporting structures The 4 Cs: Capacity, Competency, Consistency,
associated with state, county, and municipality regu- and Compensation
lations. These burdens delay funding to organizations To best describe the needs of and solutions for the ad-
that would otherwise be poised to develop and exe- diction treatment ecosystem, the authors of this man-
cute programs for people with SUDs. uscript propose the guidance of the “4 Cs”: Capacity,
Individuals who encounter the justice system have Competency, Consistency, and Compensation.
significantly higher rates of opioid use than the gen- Capacity refers to whether the system is correctly
eral population and are at significantly higher risk of sized and nuanced enough to fill the needs of the com-
overdose upon leaving jail or prison than their peers munity it is serving. The American Society of Addiction
who have not encountered the justice system [53]. This Medicine (ASAM) levels of care (LOCs) provide a use-
connection is obvious—people who experience SUDs ful framework to understand types of treatment called
may perform illegal activities to acquire their desired upon to treat SUD in a community [5]. Competency re-
substance, and many of these substances are currently fers to the education, training, and evaluation of those
illegal [53]. This reality spotlights the failed history of who work within the treatment system, including but
America’s “war on drugs” and how the American crimi- not limited to physicians, psychotherapists, administra-
nal justice system currently operates. Any attempt to tors, and peer recovery specialists. Consistency refers
improve addiction care in the U.S. must include an to whether the system is delivering high quality care.
expansion of assessment, treatment, and support for The quality of a system’s care is often assessed based
justice-involved populations based upon scientific data on fidelity to best treatment practices and appropriate
about best practices while considering the historic and use of the system’s infrastructure. Compensation re-
systemic racism that has led to mass incarceration of fers to whether the treatment system financially aligns
Black individuals, particularly Black men [39,53]. reimbursement with best practices. Payment can be
Policymakers and health leaders have an opportuni- viewed through the lens of the payment amount, pay-
ty to make targeted investments dedicated to repairing ment type, including whether payment is being made
the damage done by the drug overdose epidemic and for evidence-based practice versus legacy treatment
preventing further harm. To create a more robust and practices, and inclusion of carved-out versus carved-in
equitable medical system that recognizes and treats behavioral health. While one could rightfully argue that
addiction, evidence-based interventions and programs a fifth “C” could be added for Community, that consid-
need to be adequately funded and resourced. There eration is outside of the scope of this publication. The
also needs to be an effort to construct and enact the sections below explore each of these 4 Cs in detail.
missing pieces of the currently fragmented system
for treating addiction in the U.S. These investments Capacity
and this new system all need to be developed and The disease of addiction, in all its forms, can affect and
deployed while considering the pervasive impact of is affected by issues such as:
structural racism on how those with addiction are both • early life trauma
viewed and treated (socially and medically). As such, it • behavioral health needs
is incumbent upon those building this new system to • biomedical needs
evaluate and repair any laws, regulations, or payment • psychiatric needs
structures that perpetuate this reality. • chronic pain
To ensure that funding is directed to aspects of the • withdrawal management needs
system that would most benefit from additional sup- • housing
port, the authors of this paper propose the following • food security
architecture and guidance. The authors of this manu- • transportation
script hope that this proposed guidance will help direct • communication access
funding and action toward a robust, well-functioning • cognitive capability
SUD treatment system, but also recognize that much of • cultural context
the proposed guidance is most applicable to the treat- • criminogenic history and behavior
Page 2 Published April 5, 2021
Guide for Future Directions for the Addiction and OUD Treatment Ecosystem
• structural racism patients will require adequate management of their
• a myriad of details for each named issue pain to facilitate improvement to their function and
quality of life [69].
This manuscript acknowledges the complexity of the In many counties across the U.S., there are no ad-
disease of addiction and attempts to discuss this dis- diction treatment facilities [22] even for those most
ease in totality, but all of the interventions proposed severely afflicted with SUD—let alone those with mild
in this paper will need to be rolled out with the whole to moderate SUD. In some counties, there may be an
patient, and all considerations outlined above, in mind. adequate number of addiction specialists, but health
The current state of the addiction treatment ecosys- plans do not provide equitable or accessible care, de-
tem is unable to manage and appropriately treat the spite the existence of the Mental Health Parity and Ad-
millions of people with substance misuse, SUD, and diction Equity Act (MHPAEA) [16]. This Act and other
addiction in the U.S. today. Because of the systemic parity-related legislation, such as the Affordable Care
barriers that make access to this care difficult, only a Act, have yet to be fully implemented and enforced.
minority of patients receive evidence-based care [26], Developing effective monitoring and enforcement of
including medications for opioid use disorder (MOUD) mental health and SUD laws is a national imperative.
and interventions for the social determinants of health- Despite multiple clear guidelines, the vast majority
related issues listed above. Sufficient consideration of of Americans with addiction do not receive treatment
patients with chronic pain who develop a physical de- inclusive of best practices, including MOUD. Many pro-
pendence to opioids or suffer from a SUD is also lack- grams rely on abstinence-based treatment, which re-
ing. In addition to behavioral health treatment, these quires patients to forgo evidence-based medications
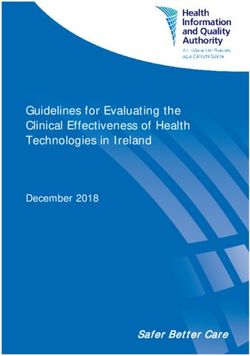
FIGURE 1 | The ASAM Criteria
SOURCE: American Society of Addiction Medicine. n.d. What is The ASAM Criteria? Available at: https://www.
asam.org/asam-criteria/about (reprinted with permission)
NAM.edu/Perspectives Page 3
DISCUSSION PAPER
that save lives [32]. This is particularly unfortunate ASAM Criteria, fits into the continuum of treatment
given the medical and policy understanding that using (see Figure 2).
these medications is consistent with both abstinence Basic concepts should be employed while following
and recovery [54]. Given the need to focus on cost-ef- the ASAM LOCs:
fective and rapid solutions, it is imperative that fund-
ing is allocated to the types and LOCs that are aligned 1. U.S. Food and Drug Administration (FDA)-ap-
with the needs of patients in individual communities. proved maintenance medications for addiction
For instance, the services unhoused patients need are treatment should be made available at every
different from those of people with stable housing, LOC.
and the system should be responsive to those differing 2. Access to all needs associated with addiction
needs. This section will discuss capacity as it relates to treatment should be available either at the loca-
the ASAM Continuum of Care, MOUD, workforce, tele- tion (if specified by LOC) or by referral.
health, naloxone, and harm reduction services. 3. These services (if not specified by otherwise) can
be delivered telemetrically, via group practice or
Capacity: ASAM Continuum of Care and the hub, and spoke methodology, via mobile units
Treatment Ecosystem or even electronic applications.
The single most important concept in the treatment of 4. Currently the ASAM Criteria is in the process of
patients with an OUD is the rapid and immediate initia- its fourth revision. The descriptions below are
tion of MOUD followed by patient-centered and stig- forward looking to this edition.
ma-free services at the appropriate LOC. This means
that while the medication is critical to rapidly stabilize Level 0.5
a patient, it must be matched with the correct inten- Level 0.5 is the most basic of interventions and con-
sity of interventions that address all components of sists of modalities such as screening, brief assessment,
care listed above, including the relevant social deter- brief intervention, and referral to treatment (SBIRT)
minants of health, to truly stabilize a patient in their or societal interventions, such as an impaired driving
recovery. For instance, consideration of patients’ ac- program for people who do not meet the diagnostic
cess to secure housing and reliable transportation as criteria for an SUD or addiction, but have high-risk driv-
well as their ability to afford care is critical in assessing ing behavior secondary to intoxication. This series of
the practical capacity of the treatment system. Without care tasks can, and should, occur in all areas of general
consistent access to care, availability of even the best medical care, including hospitals.
treatment options will be inadequate.
The ASAM Criteria, formerly known as the ASAM Level 1
Patient Placement Criteria, “is the most widely used Level 1 is designed to deliver services in a variety of
and comprehensive set of guidelines for [service set- locations and to a diverse subset of individuals. This
ting], continued stay, transfer, [and] discharge of pa- LOC can be delivered at school-based clinics, mental
tients with addiction and co-occurring conditions” [5]. health clinics, or primary care offices, and can be used
When used correctly, the criteria guide the treatment for patients who are experiencing mild or moderate
provider through a six-dimensional biopsychosocial levels of addiction and are ready for a change or need
assessment (see Figure 1) that informs a comprehen- ongoing addiction treatment. This could be an initial
sive treatment plan. Once the needs of the patient are LOC or a step-down LOC for someone who is invested
identified, an appropriate LOC can be chosen [4]. By in recovery but is leaving residential treatment, or step-
identifying the areas where a patient’s support system down treatment for someone who had intensive out-
is lacking or underdeveloped, addiction specialists can patient treatment. It can, and should, include referral
tailor interventions and service settings that would give for medications for addiction such as buprenorphine,
the patient the best chance for stabilization. naltrexone, or acamprosate, among many other choic-
After the multidimensional assessment, patients are es. While the prescribing of medication for addiction
then recommended an ASAM Criteria LOC based on treatment is of utmost importance, it is only part of the
the assessment outcome and the needs identified in treatment and should not be delivered without some
the treatment plan. Below, the authors of this manu- ability to address all needs in some fashion. There are
script briefly describe how each LOC, defined by the fewer than nine hours of structured clinical services
Page 4 Published April 5, 2021Guide for Future Directions for the Addiction and OUD Treatment Ecosystem
FIGURE 2 | ASAM Criteria Within the Continuum of Care
SOURCE: Figure created by authors using data from American Society of Addiction Medicine. n.d. What is The
ASAM Criteria? Available at: https://www.asam.org/asam-criteria/about.
delivered by peers or addiction counselors provided at use all forms of MOUD. OBOTs are outpatient offices
this LOC. that use only buprenorphine and naltrexone for OUD.
Example: A patient who meets criteria for level 1 However, buprenorphine is a controlled substance,
services for OUD could have their medication written highly regulated by the Drug Enforcement Administra-
by a primary care physician who, if needed, refers the tion (DEA). At the time of this publication, prescribers
patient to an SUD counseling location. must have a DEA waiver to prescribe buprenorphine
and meet the state’s requirements for prescribing this
Comprehensive Level 1 medication [20]. They need to either deliver on-site
This LOC encompasses opioid treatment programs behavioral therapy or have the ability to refer out to
(OTPs/methadone clinics) and comprehensive office- behavioral therapy. There should also be access to pri-
based opioid treatment providers (OBOT). OTPs are mary care services, either in-house or by referral, at
heavily regulated and provide both medication and this LOC.
behavioral health services on site or in close coor- Example: A patient who is being treated at a com-
dination. They can provide varying levels of intensity prehensive level 1 will need more substantial medica-
for clinical services on-site and have some grouping of tion monitoring (daily dosing or short-term prescrip-
counselors and licensed staff available for both indi- tions) and closer coordination with case management
vidual and group therapies. OTPs can and generally do and behavior services. The addition of peer support
NAM.edu/Perspectives Page 5DISCUSSION PAPER
and more comprehensive toxicological evaluations Level 3.5 Clinically Managed High-Intensity Residen-
should be the norm. tial Services
This LOC is designed for patients with relationships
Level 2.1 and 2.5 that are abusive, chaotic, or non-supportive; who have
not developed adequate coping skills for recovery; and
Level 2.1 Intensive Outpatient
who are in imminent danger, needing 24-hour stabili-
This LOC must support medical, psychiatric, psycho-
zation and treatment. This LOC is staffed with licensed
logical, laboratory, and toxicology services through
clinical staff, including social workers, licensed profes-
direct care, through telemedicine, or by referral. They
sional counselors, and addiction counselors. There are
should have emergency services available 24 hours per
daily programmed services that should include cogni-
day and have direct access to the other LOCs. This LOC
tive behavioral therapies, motivational enhancement
provides nine hours or more of programed clinical in-
therapies, and psychotherapies. This LOC should have
tervention per week. A patient would continue services
access to medications for addiction treatment and toxi-
here until they are ready to step down to a less inten-
cological studies for monitoring purposes. They do not
sive LOC or are moved to a more intensive LOC be-
have to be on-site. There should be ongoing interdisci-
cause of increasing severity of illness. The nine or more
plinary assessments and treatment directed at inhibi-
hours of programming should be tailored to the indi-
tors of recovery and linking to ongoing addiction treat-
vidual and not be the same for every patient. This LOC
ment.
should also have access to medications for addiction
and psychiatric illness via telemedicine or direct care. Level 3.7 Medically Monitored Intensive Inpatient Ser-
vices
Level 2.5 Partial Hospitalization
Level 3.7 includes physician monitoring and around-
This LOC can be done in the same setting as a level
the-clock nursing care. This LOC includes access to psy-
2.1 but will need to provide at least 20 hours of pro-
chiatric, toxicological, and lab services on-site, via refer-
grammed clinical intervention per week. This should
ral or through telemedicine. This LOC is designed for
be a mixture of individual, group, or self-help therapy.
patients with concerns in dimensions 1–3 (withdrawal,
A patient should be living in a sober-living facility, at
medical, and psychological) and the need for medical
home, or in a shelter to receive this care efficiently.
monitoring for these. There is direct delivery of clinical
Both levels 2.1 and 2.5 can be “co-occurring enhanced,”
services as in Level 3.5.
which means that they will handle all outpatient psychi-
While all of the levels described so far are considered
atric needs in-house.
“residential”, they vary based on the level of clinician
Example: A patient with OUD, who meets the in-
oversite (the managing clinician may be an LCSW or a
tensive outpatient or partial hospitalization LOC, will
psychologist, etc.). Level 3.1 has the lowest need for
need highly structured behavioral interventions de-
clinical intervention and is generally not staffed with
livered by qualified personnel. Someone could simul-
licensed clinicians and thus does not deliver psycho-
taneously qualify for comprehensive level 1 care (an
therapy. Level 3.5 provides the safety of a therapeutic
opioid treatment program) and still need level 2.1 or
environment and delivers behavioral therapies from li-
2.5. The reason for this is that they would need both
censed clinicians. The need for a patient to enter treat-
enhanced medical and medication monitoring as well
ment in a specific level of care in a residential environ-
as increased behavioral services.
ment to go to residential can vary based on the stability
Levels 3.1, 3.5, and 3.7 (Residential) of their living environment, their readiness to change,
and their risk of relapse. For those with medical condi-
Level 3.1 Clinically Managed Low-Intensity Residential tion that need medical monitoring, level 3.7 provides
Services for 24 hour nursing care and access to an on-call physi-
Level 3.1 is the first residential LOC and is designed for cian.
people who have little or no community connection,
a high-risk living environment, or very low recovery Level 4.0 Medically Managed Intensive Inpatient
skills. It is generally staffed by allied health profession- Services (Hospital-Based Services)
als, peers, and group living workers. This is the least Level 4.0 is a hospital LOC that includes addiction treat-
intensive level of residential treatment when it comes ment. The care is managed by a physician who is re-
to direct services delivered. sponsible for diagnosis, treatment planning, and treat-
Page 6 Published April 5, 2021Guide for Future Directions for the Addiction and OUD Treatment Ecosystem
ment. This care generally focuses on the withdrawal pain and their expectations of living with pain, which
syndrome, stabilization of medical issues, or acute psy- may require supplementary psychosocial supports.
chosis, but does not include direct addiction treatment
by addiction counselors or clinicians. Capacity: Where Most Patients Fall on the
A critical component to successful management of Continuum of Care
the chronic disease of addiction is that the LOCs should Because addiction is a chronic relapsing and remitting
not live in isolated silos. Patients should be able to flow disease, the needs of patients may fluctuate, mean-
from one LOC to the other as their condition improves ing they may need higher and lower LOCs over time.
or worsens. This focus on patient response to treat- Therefore, the entire continuum of care must be con-
ment can be accomplished by community coordination sidered for a patient’s course of treatment. It should
of services through a central assessment and coordi- be anticipated that patients could require higher LOCs
nation location, contracted step-down pathways, and as their disease worsens. A process that is more re-
knowledge of the array of services delivered at each sponsive to the needs of patients could consider the
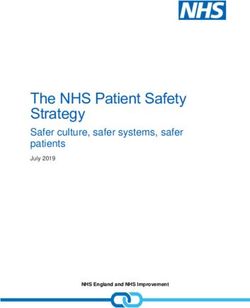
location. While this integrated system may seem like case of patients who begin care according to Table 1.
the idealized state, addiction medicine physicians and For example, patients who suffer from mild OUD may
allied professionals have understood this need for over begin and stay at level 1 outpatient, while others may
30 years—now is the time to build the right compo- need initial placement in level 4 treatment. Once stable
nents to deliver the right service at the right time. Im- in level 4, they will progress down the intensity cascade
portantly, patients with chronic pain may require spe- until in recovery. However, most patients do not prog-
cial consideration throughout this continuum of care. ress in a linear fashion and will need restabilization
In addition to treating SUDs, clinicians will need to work after relapse. Experts and data from the ASAM Con-
with these patients to adequately manage their chronic tinuum evaluation tool estimate that 40-50 percent of
ASAM Levels of Care
% of patients 0.5 1 2.1 - 2.5 3.1 - 3.7 4
Dependent and Early
50% misuse intervention/
prevention
(secondary and
tertiary)
40% of OUD and Early Outpatient
50% misuse intervention/
prevention
(secondary and
tertiary)
20% of OUD Early Outpatient Intensive
intervention/ outpatient
prevention
(secondary and
tertiary)
20% of OUD Early Outpatient Intensive Residential
intervention/ outpatient
prevention
(secondary and
tertiary)
20% of OUD Early Outpatient Intensive Residential Hospital
intervention/ outpatient
prevention
(secondary and
tertiary)
TABLE 1 | ASAM Levels of Care and Patient Care Trajectories
SOURCE: Created by authors.
NAM.edu/Perspectives Page 7DISCUSSION PAPER
OUD patients will start in level 1, while approximately However, for some patients who do not need this over-
20 percent will need level 4 treatment. sight, it is burdensome, expensive, and unnecessary.
The SUD treatment system in the U.S. does not In contrast, oral buprenorphine has the ability to be
conform to this ideal state, and treatment availability dispensed frequently and flexibly at a pharmacy; how-
across the care continuum varies across the country. ever, currently, only practitioners who obtain a special-
Data from internal ASAM surveys reveal that some ex- ized DEA waiver can prescribe this medication [20], and
perts feel that capacity is lacking in certain LOCs (e.g., they can only prescribe to a limited number of patients.
intensive inpatient and outpatient) and have excess Only 4 percent of doctors nationwide are waivered to
capacity for others (e.g., inpatient rehabilitation pro- prescribe buprenorphine and only half of those are ac-
grams in level 3.5). However, this perception may be tive prescribers [21]. Given the limited availability and
due to differing access to insurance, the array of servic- increased flexibility of oral buprenorphine treatment
es available, and the heterogeneity of quality through- options in comparison to those of methadone, it is par-
out the continuum. Accessibility to all LOCs throughout ticularly concerning that Black patients are less likely
the continuum is required for both clinical and cost- than white patients to be prescribed buprenorphine.
effective care to occur. This disparity persists across income level, with wealth-
It is important for the ASAM Criteria to be used re- ier individuals being more likely than lower-income
gardless of the actual substance(s) a person has been individuals to have access to buprenorphine, and ur-
misusing. If a community or health plan does not have gently needs to be addressed [70].
a full continuum of care available to treat people ad- Naltrexone injections (extended-release Naltrexone)
dicted to opioids, they most likely do not have the ap- are administered monthly at a doctor’s office or clinic.
propriate resources to treat people addicted to alcohol As the least-regulated medication, extended-release
or methamphetamine. This leads to mismatched care Naltrexone requires abstinence (i.e., free from short-
and patients who feel lack trust in their care and pro- or long-acting opioids for 6 or 7–10 days, respectively,
viders and the system as a whole. based on ASAM’s National Practice Guideline [6]) upon
injection. The current rigid and asynchronous regula-
Capacity: Medication for Opioid Use Disorder tions for MOUD are not conducive to a well-functioning
(MOUD) treatment system and frustrate an already complex
The use of MOUD is a core component of the man- problem. Having these medications fragmented across
agement of OUD. Medical science shows that ongo- providers is antithetical to confronting OUD with per-
ing medication management saves lives, and the use sonalized treatment options.
of MOUD treatment is the gold standard of care [32]. Another barrier to receiving MOUD is the administra-
Short-term medication use for withdrawal manage- tive restrictions often faced by patients and physicians,
ment is applied extensively in medically managed or including restrictive formularies, prior authorization,
medically supervised withdrawal management pro- and step therapy or “fail first” protocols. If a patient is
grams (ASAM levels 4 and 3.7). MOUD as a long-term stable on a specific medication or formulation of the
maintenance treatment is most often associated with MOUD, but the medication is not on a health plan,
level 1 outpatient care. In an ideal state, MOUD with all Medicaid, or pharmacy benefit management company
three FDA-approved medications for OUD (methadone, formulary, the patient may be forced to discontinue or
buprenorphine, and extended-release naltrexone) delay therapy until a prior authorization can be com-
would be a core treatment component throughout the pleted. Sometimes, the prior authorization may be
entire residential and outpatient continuum of care [4]. further delayed or denied altogether, forcing the pa-
If applied properly, the use of MOUD negates the need tient into withdrawal or subjecting the patient to un-
for inpatient withdrawal management. affordable costs for out-of-pocket payments to remain
The regulations surrounding each of these medica- in compliance. According to a 2018 Substance Abuse
tions create different barriers for people seeking treat- and Mental Health Services (SAMHSA) report, only 42
ment. Methadone, the longest standing MOUD, is ini- state Medicaid programs reimburse for methadone
tially dispensed daily at an independent OTP. This daily for the treatment of OUD [45]. Patients may also face
dosing can be helpful for those needing a stabilizing these hurdles if they switch insurance plans—in that
pattern of enhanced medication monitoring while mini- one company might cover a particular formulation, but
mizing disruptions to the responsibilities of daily life. if that is not the formulation being used by the patient,
Page 8 Published April 5, 2021Guide for Future Directions for the Addiction and OUD Treatment Ecosystem
the only way to obtain coverage may be for the patient all geographic areas, and rarely in rural areas.
to fail on the covered medication first. These policies • Despite having the best outcomes for some pa-
are not evidence-based and can have deadly conse- tients, methadone still possesses the highest
quences. These issues are complicated even further by level of stigma of the MOUD treatment medica-
the fact that these policies differ from state to state, tions.
making education surrounding prescribing complex at • Lack of insurance coverage contributes to ac-
best and near impossible at worst. cess barriers for this treatment.
For patients and providers who are able to navigate
the fragmented medication system and a myriad of Capacity: Workforce Needed
administrative barriers, patient outcomes have consis- The implementation of MOUD has not kept up with the
tently proven that MOUD saves lives, prevents infec- growth of the opioid overdose epidemic in the U.S. The
tious disease, and provides economic benefits to pa- number of OTP clinics increased by only 36 percent
tients and their communities. Methadone treatment from 2003 to 2016, and those offering buprenorphine
is the most studied of the three of the FDA-approved treatment increased from 11 percent to 58 percent
medications and shows consistent retention in treat- [3]. In the same timeframe, opioid-related overdose
ment—from 60 percent to as high as 80 percent over increased by approximately 230 percent [33]. In 2018,
six months [23]. It is difficult to differentiate whether 20 percent of people with OUD received specialty ad-
this is specifically a medication effect or the effect of diction treatment [27]. To close this treatment gap,
being in a highly observed and consistent environment clinics need to be properly funded and administrated.
with daily interaction with treatment staff. However, the most beautiful building and the best ad-
Studies show limited public support for the use of ministration cannot treat addiction without the appro-
federal dollars for any form of addiction treatment priate workforce. The compensation structures that
[10], and only 19 percent of Americans endorse the make this investment overly complicated are explored
use of methadone [31]—one of the most commonly in detail below. The staffing numbers listed below take
used forms of MOUD [28]. As a result, many people do into account current limitations placed on providers by
not seek treatment out of fear of being marginalized, state and federal licensing. They are not endorsed by
especially by their coworkers and neighbors. Further- these authors, as they lack nuance and have little to no
more, one in seven rural providers will not prescribe data to support them. However, they do represent the
buprenorphine because of issues with DEA intrusion current state of the addiction medicine workforce.
into their practice [8]. Multiple barriers restrict the availability of top-of-the-
While the results are very positive for a certain seg- line OUD treatment, including stigmatizing attitudes
ment of patients, methadone maintenance can have toward MOUD, cost of treatment for the individual, and
limitations: restrictive regulations for prescribing [46]. One factor
• The administration of methadone medication is blocking access to appropriate treatment is the severe
highly regulated, limiting the number of treat- shortage of trained professionals available to meet the
ment centers qualified to administer this form dramatically expanded treatment need dictated by the
of treatment (special licenses and intense over- opioid overdose epidemic.
sight required). The schematics on the following page are examples
• Methadone treatment is typically delivered in of provider staffing needs at each ASAM LOC. The num-
an OTP daily, with each dose delivered to the bers in the schematic are derived from limits set forth
patient under observed conditions, thus limit- by a combination of the DEA, state licensing boards,
ing this form of treatment for patients for which and current payment support mechanisms. Advanced
daily treatment is not a viable option. Only after practice clinicians, such as physician assistants and
a patient has been stable for six weeks will some nurse practitioners, can only prescribe buprenorphine
states even allow patients to have take-home to 100 patients. Physicians can likewise only prescribe
doses. For some, achieving “stability” can take for 100 patients, increasing to 275 only if they are spe-
years. cialists or working within specific qualified practice
• Methadone treatment is associated with signifi- settings. The numbers attributed to a therapist and
cant stigma. case manager (CM) are restricted by scheduling ca-
• Methadone treatment clinics are not available in pacity and, in some states, licensing limits. Peer limits
NAM.edu/Perspectives Page 9DISCUSSION PAPER
are practical limitations as described by multiple peer- • 3 addiction specialists (covering an OTP, level 3.7
based interventions and presumes that peer support and level 4)
specialists are supportive of maintenance medications. • 10 prescribers seeing 100 patients, or 50 pre-
It is possible to extrapolate the appropriately sized scribers seeing 20 patients
workforce needed for a town of 100,000 residents • 100 therapists
using the numbers outlined above. This scenario will • 70 case managers
build on the assumption that 10 percent of the popula- • 100 peers
tion either has an SUD or suffers from misuse and re-
quires an intervention. This estimation is much higher For comparison, the current national average of psy-
in communities that are hit hardest by the opioid crisis. chiatrists per 100,000 is 12.9; the average number of
This extrapolation yields approximately 10,000 peo- addiction psychiatrists and addiction medicine phy-
ple needing care. To make this value more realistic, for sician specialists is 0.3 per 100,000 [56]. While this
the sake of this thought exercise, assume only 70 per- thought exercise is oversimplified, this example illus-
cent of those want help. This results in 7,000 people trates we only have a fraction of the staffing needs
needing care, including differing levels of need and required for quality care. . This thought exercise also
medications for OUD and SUD. Using the numbers in does not include those tasked with community sup-
the schematic, this town of 100,000 would need ap- ports for the myriad of social determinants of health or
proximately: reentry needs. Given the need for multiple LOCs in the
Level 1: Outpatient
ASAM Level of # Patients per # Patients per # Patients per # Patients per
Care Prescriber Therapist RN-CM Peer Coach
Level 1 Primary 100 100 300 N/A
Care
Comprehensive 275 [44] 90 200 50
Level 1 or Addiction
Specialist
OTP 300 65 150 50
Level 2: Intensive Outpatient
ASAM Level of # Patients per # Patients per # Patients per # Patients per
Care Prescriber Therapist RN-CM Peer Coach
Level 2.1 100 - 275* 50 100 50
Level 2.5: Partial 100 - 275* 45 100 50
Hospitalization
*If the prescriber is a qualified addiction specialist or working in a qualified practice setting, the
higher numbers apply [55].
Level 3: Residential
ASAM Level of # Patients per # Patients per # Patients per # Patients per
Care Prescriber Therapist RN-CM Peer Coach
Level 3.7 30 30 30 N/A
Level 4: Intensive Inpatient
ASAM Level of # Patients per # Patients per # Patients per # Patients per
Care Prescriber Therapist RN-CM Peer Coach
Level 4 20 20 20 N/A
Page 10 Published April 5, 2021Guide for Future Directions for the Addiction and OUD Treatment Ecosystem
setting of a limited number of specialists, the addiction and transformative to health care. The lessons learned
specialists we do have, are often stretched relatively from the EHR transition are applicable to help build the
thin compared to their specialty provider counterparts. capacity to treat complex conditions like addiction in a
Remember, in this example we are only talking about a virtual setting. For most providers, virtual care was not
city the size of San Angelo, TX—imagine the workforce a choice but a necessity as COVID-19 spread across the
needed in a city with over one million people. There is country. Similar to the experience during the rapid ex-
clearly a massive national effort needed to build an ap- pansion of EHRs, health teams are working to optimize
propriately sized workforce, while leveraging the use of telehealth as they are being forced to use it, and there
available technology to make the relatively small size of are no clear best practices for virtual care in many set-
the current workforce operate more efficiently. tings. Making the transition to telehealth for addiction
care as effective as possible will require a focus on:
Capacity: Telehealth
Telehealth has been shown to be an effective modal- • clinician skill building and competency,
ity to provide care for many medical and behavioral • development of accepted criteria on when to use
health conditions [2]. Despite the evidence for the virtual versus in-person modalities, and
appropriate and effective use of telehealth in certain • payment parity for virtual and in-person care.
conditions, telehealth uptake has generally been slow,
largely because of the limitations in payment models Many providers and health systems have undergone
and other regulatory barriers. With the onset of the meaningful practice transformation to a model of ro-
COVID-19 pandemic and subsequent rollout of stay-at- bust team-based care leading to improved engage-
home orders, telehealth rapidly emerged as the solu- ment across the care team and optimization of each
tion to provide care while avoiding potential COVID-19 staff member’s unique role. As care teams move into
transmission. Most notable has been the rapid expan- the virtual clinical model, practices need to continue
sion of telehealth by Medicare members. For example, focusing on the role of each team member and their
in a six-week period, there was an 11,617 percent in- interaction with the patient. This can be challenging
crease in Medicare member visits alone [36]. This in- in a virtual environment when care is asynchronous
crease was the result of a massive expansion of tele- and spread across locations. Practices need to resist
health flexibilities at the federal level. Concurrently, returning to the provider/prescriber-centric model, a
one by one, states adopted their own flexibilities and common occurrence when practices transitioned from
updated regulations for the use of virtual platforms to paper to EHR. This is another opportunity to learn from
deliver care. Along with the new payment allowances, past experiences as practices move through this para-
additional flexibilities were announced that allowed the digm shift.
prescription of controlled substances via telehealth for Using telehealth to treat addiction and behavioral
both new and established patients, as well as the abil- health conditions has several distinctly different ap-
ity to use a broader array of technology platforms to proaches compared to addressing other physical or
communicate with patients. Finally, the DEA and SAM- medical conditions. Most of these differences are relat-
HSA put in place numerous flexibilities specifically for ed to the need to build an empathetic and responsive
patients being treated with MOUD, including the abil- connection with the patient. Building such a connec-
ity to prescribe buprenorphine based on an audio-only tion is already difficult in the office setting, and physi-
telephone visit with a patient [74]. cal separation only makes this more difficult. Although
The change from in-person to virtual care is a para- there may be less reliance on the “hands-on” physical
digm shift in health care on the scale of the transition examination (PE), there is a greater need to connect
from paper charts to electronic health records (EHRs). on a personal level that may be challenging in a virtual
In the case of EHRs, when federal funding was allocat- world. The clinician must be cognizant of addressing
ed to support this transition, there was rapid uptake issues like unanticipated interruptions in connectivity
by health systems. However, providers received little and having distracting sounds in the background. Hav-
to no training to prepare and develop best practices. ing standard tools and protocols to support this activity
As a result of this lack of preparation and despite the is a must. A broad set of skills are needed to treat a
potential benefits of EHRs, providers and patients alike patient with addiction that requires mastery in a virtual
have expressed widespread dissatisfaction with the environment including but not limited to:
system. Transitioning to virtual care is equally rapid
NAM.edu/Perspectives Page 11DISCUSSION PAPER
• assessing the medical and behavioral condition Rapid and substantial expansion of naloxone distri-
of the patient and associated comorbidities; bution programs, including standing orders in pharma-
• assessing other patient needs such as living situ- cies, has proven to save lives and reduce hospitaliza-
ation, housing, family dynamics, and relation- tions related to opioid overdose. The FDA has issued
ships; and guidance to accelerate the development of over-the-
• assessing patient safety in real time. counter naloxone, which could substantially expand
access to this life-saving medication [41].
In response to physical distancing guidelines imple- Naloxone distribution is most effective when strate-
mented during the COVID-19 pandemic, the DEA gically and equitably distributed to at-risk groups. This
waived the requirement for an in-person visit prior to equates with free and low barrier availability at many
beginning buprenorphine treatment [37]. Many payers locations. There are key distribution points that must
expanded their telehealth reimbursement to include be included in a naloxone allocation system for maxi-
additional services and increased payment to equal in- mum harm reduction. These locations include:
person visits. Each state has its own telehealth statutes • syringe exchange programs
and regulations that add to the variability in capacity • correctional departments, prisons, and jails
for treatment. • housing shelters
One aspect of addiction treatment that is often • hospitals
overlooked are disparities associated with socioeco- • emergency departments
nomic status. This equates to some patients having • community-based pharmacies
decreased broadband access, no data plans for their • community-based naloxone distribution pro-
smartphone, and unreliable Wi-Fi connections. There grams
is also a digital literacy divide that will need to be ad- • health departments
dressed for this population. While data is still being de- • mobile health clinics
veloped in how to effectively address these issues, the • safety net providers
digital and literacy divide will continue to persist and • first responders, including law enforcement
cause gaps in care and treatment if not addressed in
an expedited manner. However, some of these issues The workforce capacity to distribute naloxone is often
may be partially offset by the deceased need for travel, inadequate at the local level and often based on the
childcare, and absence from work that an in-person opioid overdose rate in a community. Typically, full-
visit requires. time employees are required to run a publicly funded
overdose education and naloxone distribution pro-
Capacity: Naloxone Education and Distribution gram, with support from other state agencies including
Naloxone is a medication that will reverse an opioid the department of public health.
overdose. Naloxone is made available in the commu-
nity for use in emergencies by multiple distribution Capacity: Other Harm Reduction Services
methods, including co-prescription with opioids, stand- Another key capacity-based strategy for addressing the
ing state orders by public health physicians, and distri- opioid overdose epidemic is harm reduction programs
bution through treatment programs and harm reduc- like syringe services programs (SSPs). Harm reduction
tion programs such as syringe service locations (needle refers to any program that provides services to protect
exchanges). Naloxone is also available in many areas people who use drugs from disease or harm without
as part of emergency medical kits and carried by first demanding people to stop using substances. SSPs are
responders. These prescriptions can be provided for community-based programs that provide access to
patients with a known OUD or those who take opioids free sterile needles and syringes and safely destroy
for pain. Some states have expanded access to nalox- used needles and syringes. These locations can also
one by allowing pharmacies to have a standing order act as entry points for treatment, education, and care
for the medication, permitting anyone to receive the coordination. High-risk injection behaviors are strongly
medication over the counter [57]. Forms of naloxone associated with several communicable diseases such
include intramuscular injection, nasal spray, and in- as HIV and Hepatitis C. These and similar programs
travenous administration. Naloxone has saved tens of reduce the spread of disease while teaching safe in-
thousands of individuals from death due to an opioid- jection practices and training individuals on overdose
related overdose. rescue [9]. Harm reduction strategies are highly stig-
Page 12 Published April 5, 2021Guide for Future Directions for the Addiction and OUD Treatment Ecosystem
matized and often mischaracterized as enabling drug lationship between a patient and a provider. Without
use. There is no proven association between the use of clear practice guidelines, various forms of traditional
SSPs and increased drug use. and experimental treatments have been able to thrive
Besides the humanitarian argument to protect peo- without scientific evidence on their safety or efficiency.
ple in all stages of use and recovery from devastating Without a baseline quality metric, the addiction treat-
infection, SSPs are economically advantageous. Pre- ment system does not have adequate means to stan-
venting the contraction and spread of communicable dardize and improve its quality. Some medical provid-
diseases costs significantly less than the downstream ers are working to integrate addiction treatment into
costs of infection and death [53]. Return on investment established primary care and psychiatric practices and
(ROI) for these efforts is as high as $7 for every dollar publish guidelines based on this work. Addiction medi-
spent [19], demonstrating very efficient use of funding cine has recently become a recognized field within the
to protect health. This ROI, specifically, accounts for National Board of Medical Specialties, which will not
only the cost of avoiding having to pay for HIV treat- only provide a scalable specialized clinical and research
ment alone—the addition of other avoided costs in- workforce, but also build emphasis on addictive dis-
cluding hepatitis C and other related issues will further eases into the medical school curriculum, into hospital
increase the ROI of these programs. staff training, and throughout the medical care system.
Such programs often use counselors and peer sup- While these efforts are critical to opening new av-
port staff who help patients navigate their way into a enues for care, the deeper issue lies with how health
treatment program. Research consistently demon- practitioners and the broader public understand ad-
strates the effectiveness of unused syringe access in diction as an illness. In the U.S., two ends of a spec-
preventing infectious disease transmission and soft trum often emerge as to how addiction develops and
tissue infections while also supporting the overall is maintained: as a chronic relapsing and remitting dis-
“health and well-being of drug users through linkages ease as understood by the medical and scientific com-
to drug treatment, medical care, housing, [overdose munities, or as a hedonistic failure of people who just
prevention, insurance coverage,] and other vital social “can’t say no.”
services.” [75] SSPs also “respect, value, and prioritize Too often, addiction has been treated as a behav-
the human rights and dignity of people who use drugs” ioral and moral failure rather than a medical condition
[75] while challenging drug-related stigma. with behavioral symptoms [34]. For decades, the U.S.
has relied on behavioral interventions such as detoxi-
Competency fication, incarceration, and other legal penalties—all
The Institute of Medicine (now the National Academy of of which fail to address the underlying causes of ad-
Medicine) defined the core competencies of medicine diction. While these interventions may make sense
in 2002, which include patient-centered care, inter- if addiction were an issue of poor choices and moral
disciplinary practice, evidence-based practice, quality failings, the lack of effectiveness of these methods is
improvement, and informatics [24]. These competen- consistent with what is now known about the brain
cies have not fully penetrated into addiction medicine science of addiction as a chronic disease. As with any
at scale. Integrating research and providing evidence- disease, health providers need to address the needs
based care has proven challenging in the addiction of each patient for biological, psychological, and social
treatment and recovery system, as many (if not most) interventions.
addiction treatment centers do not offer evidence- Framing addiction as a behavioral problem has al-
based medical treatment [71]. It is also evident that the lowed for the expansion of short-term treatment mod-
core competencies in all of medicine are lacking an un- els such as withdrawal management and residential
derstanding of how structural racism and discrimina- treatment. These facilities provide a space to “break”
tion impact every level of treatment. physical dependence on opioids and introduce behav-
The main reason for the lack of evidence-based care ioral changes but are not effective for long-term recov-
is that addiction treatment has historically been siloed ery [43]. After one year, the failure rate of withdrawal
from traditional office-based medical and psychiatric management alone is 80 percent, and withdrawal
practice. When this separation is coupled with stigma, management alone may actually increase the risk of
structural racism, and discrimination, it becomes a po- future overdose [43]. While residential treatment is
tent mix that permeates the very core of a trusting re- part of the care continuum, different facilities offer a
NAM.edu/Perspectives Page 13DISCUSSION PAPER
huge variation in the treatment, and therefore results from traditional medicine, and that health care provid-
are variable [38]. For example, some residential treat- ers are not immune to the deep stigma of addictive
ment programs may or may not offer individual coun- disease, those who do not work explicitly in addiction
seling or MOUD. Some even require patients who are have increasingly felt that the extent of their ability to
stable on MOUD to discontinue use, putting the patient help is to order a referral for the patient to speak to a
at even further risk of overdose and death. Therefore, psychologist or social worker [59]. Now that overdose
every residential treatment facility must be analyzed is the number one cause of injury-related death in the
individually, and persons in crisis do not often have U.S. and the number one cause of death for people un-
the time or the mental capacity to do so. Recovery resi- der 50 [18], the medical system must reorient toward
dences also face their own stigma from neighborhood appropriate and adequate care for those with addic-
and community organizations, often as a result of the tion.
perception that people with OUD will attract poverty The latest estimates show that very few primary care
and crime to the community [25]. and OB/GYN offices in the U.S. actively screen for ad-
Because of structural racism, incarceration affects diction on a regular basis [47]. To address this gap,
racial minorities at significantly higher rates than their medical practices need to add the education and EHR
white peers and has been used as a tool to control cer- capability to consistently and predictably apply validat-
tain types of substance use for decades [40]. The “war ed verbal screening and early intervention, in order to
on drugs” created a pervasive mindset that aligned meet new United States Preventive Services Task Force
certain types of drug use and criminality [35]. Although recommendations [60]. One method to reach this goal
many people with OUD interact with the criminal jus- would be for the top five EHR systems to build out ap-
tice system, few receive any form of evidence-based propriate screening tools, toolkits, and order-sets for
treatment while incarcerated or otherwise justice- primary care develop online learning modules to pro-
involved [13]. This method of controlling certain sub- mote a high degree of fidelity and precision.
stances and the people who use them does not work The provision of addiction medicine via telehealth
and is both catastrophic and costly to those within the has become the reality for many providers since the
criminal justice system as well as their families and so- COVID-19 outbreak. As previously discussed, this meth-
cial groups. The mass incarceration of people with SUD od of health care delivery was not carefully contem-
has devastating effects on family structures, most no- plated or optimized before its widespread use became
tably children [53]. a necessity. Technological competency, in the various
Overdose is the most common cause of death among modalities of telehealth, is going to be its own require-
the formerly incarcerated, with the month after release ment in the future of addiction medicine. By definition,
being the most dangerous [11]. Initiating and continu- telehealth encompasses several modalities including
ing MOUD in jails and prisons is a common-sense way live or asynchronous video visits, audio phone only, e-
to reduce mortality but is rarely done. Removing a consult (peer-to-peer interprofessional consultations),
patient’s medication for a chronic illness as they en- e-visits, and virtual check ins. Depending on the needs
counter the justice system is cruel and unbefitting of of the individual patient, the treatment plan could in-
their right to health care [12]. Providing methadone or clude care provided over any of these platforms—a
buprenorphine treatment, per a patient-centered de- decision the provider should base on the individual.
cision-making model, has been shown to significantly The provider, rather than regulatory agencies, should
lower overdose deaths in the months post-incarcera- decide on whether it’s possible, appropriate, or in the
tion [58]. patient’s best interest to provide care in these ways.
Addiction medicine has traditionally been viewed As the use of telehealth becomes more universally
as being outside of mainstream medicine and rarely accepted, the provider needs to develop the compe-
taught in medical school or residency, as well as in all tency of understanding the appropriate use of these
health professions. Due in part to the criminalization virtual care platforms. Whether to offer telehealth or
and stigma of addiction, this separation has even been to require an in-person visit should be at the discre-
codified in the Code of Federal Regulations (42CFR Part tion of the treating provider, who remains ultimately
2) by segregating the addiction-related medical records responsible for the quality and appropriateness of
of those in treatment from the rest of their medical care. Whether to engage in telehealth care remains the
records. Given that addiction medicine is so separate choice of the patient, and the totality of the treatment
Page 14 Published April 5, 2021You can also read