Guide 7: Cumulative harm - RESILIENCE PRACTICE FRAMEWORK - PRACTICE RESOURCES - The Benevolent Society
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

PRACTICE RESOURCES RESILIENCE PRACTICE FRAMEWORK Guide 7: Cumulative harm A framework to promote resilience in children and families www.benevolent.org.au

We are The Benevolent Society We help people change their lives through support and education, and we speak out for a just society where everyone thrives. We’re Australia’s first charity. We’re a not-for-profit and non-religious organisation and we’ve helped people, families and communities achieve positive change for 200 years. Authors Dr Leah Bromfield Manager of the National Child Protection Clearinghouse and Communities and Families Clearinghouse at the Australian Institute of Family Studies. Dr Bromfield is now Associate Professor and Deputy Director of the Australian Centre for Child Protection at the University of South Australia. Alister Lamont Research Officer for the National Child Protection Clearinghouse at the Australian Institute of Family Studies. Greg Antcliff At the time of writing was Senior Manager, Research to Practice, Benevolent Society. Greg is now Director, Professional Practice, Benevolent Society. Robyn Parker Senior Research Officer for the Australian Family Relationships Clearinghouse and Communities and Families Clearinghouse at the Australian Institute of Family Studies. Acknowledgements This Practice Guide is an adaptation of the Cumulative Harm Specialist Practice Guide written by Leah Bromfield and Robyn Miller for the Victorian Government Department of Human Services (2007). The adaptation of the guide was dependent upon generous feedback and valuable input from Benevolent Society practitioners. The Authors also acknowledge the Benevolent Society’s National Staff Network for Aboriginal and Torres Strait Islanders for their cultural consultation. January 2014 The Benevolent Society Level 1, 188 Oxford Street Paddington NSW 2021 T 02 8262 3400 F 02 9360 2319 research.policy@benevolent.org.au www.benevolent.org.au ©The Benevolent Society, 2013 All rights reserved. This work is copyright. Except under the conditions described in the Copyright Act 1968 of Australia and subsequent amendments, no part of this publication may be stored in a retrieval system, communicated or transmitted in any form or by any means without prior written permission. The Practice Resource Guides master materials may be produced by individuals in quantities sufficient for non-commercial use. Requests and enquiries concerning reproduction rights should be directed in writing to The Benevolent Society.

Practice Resource Guide
Table of Contents
Overview 4
Resilience 6
ractice Tool: Working with children and families with
P
no previously identified concerns 10
ractice Tool: Working with children and families with
P
identified concerns 13
Phase 1: Assessment 13
Phase 2: Planning 22
Phase 3: Intervention 23
Phase 4: Reviewing Outcomes 28
Closure 30
References 31
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 3
Practice Resource Guide
Overview
In this Practice Guide we take a resilience-led approach to assessment and
intervention in cases involving cumulative harm. The Resilience Practice
Framework provides an overarching model for working with children and
families. Practice Guides are designed to provide additional guidance in
cases where specific complex problems exist or with specific vulnerable
sub-groups.
What is cumulative harm? What causes cumulative Chronic child maltreatment
Cumulative harm refers to the effects harm? Bromfield and Higgins (2005) defined
of multiple adverse circumstances and Cumulative harm may be conceptualised chronic child maltreatment as recurrent
events in a child’s life. The unremitting very broadly to include the adverse incidents of maltreatment over a
daily impact of these experiences on the circumstances associated with poverty or prolonged period of time (i.e. multiple
child can be profound and exponential, the impact of adverse life events such as adverse circumstances and events) and
and diminish a child’s sense of safety, disability or chronic illness. However, as argued that chronic child maltreatment
stability and wellbeing. this Guide is designed to assist practice caused children to experience cumulative
in child and family services, the focus harm. Critically, they found that the
will be on cumulative harm caused as a majority of children who are abused or
consequence of repeated incidents of neglected experience multiple incidents
abuse, neglect, witnessing family violence and multiple types of child maltreatment.
and unrelenting low level care (i.e.
cumulative harm caused by chronic child
maltreatment).
4 RESILIENCE PRACTICE FRAMEWORK The Benevolent Society
Practice Resource Guide
How does cumulative harm Trauma Attachment
impact children? The term ‘complex trauma’ has been Human attachment relationships aim to
The main research and theories that used by many researchers to describe ensure that the ‘attached’ or dependent
have helped us to understand the way in the experience of multiple, chronic and child feels a secure bond with their
which cumulative harm impacts children prolonged traumatic events in childhood caregiver in order to learn and explore
are on early brain development, trauma, (Bromfield et al., 2007). Whereas single the social and physical world (Bacon &
attachment and resilience. Early brain traumatic incidents tend to produce Richardson, 2001). Babies and young
development, trauma and attachment isolated behavioural responses to infants exposed to cumulative harm are
theories provide different perspectives reminders of trauma, chronic trauma more likely to experience insecure or
on the processes and impacts adverse can have long-term pervasive effects disorganised attachment problems with
events have on children. Although each on a child’s development (Van der Kolk, their primary caregiver. For children with
theory focuses on separate aspects 2003). Exposure to chronic trauma an insecure attachment, the parent/
of child development, key themes are may lead to serious developmental caregiver (who should be the primary
inter-related. Acknowledging the three and psychological problems for source of safety and protection) becomes
perspectives provides a well-rounded children. Van der Kolk identified several a source of danger or harm, leaving the
theoretical grounding that further assists developmental effects of childhood child in irresolvable conflict. Attachment
in understanding the developmental trauma including: difficulties are likely to increase when
effects of adverse childhood experiences • complex disruptions of affect maltreatment is prolonged. Children’s
and why children may be behaving or regulation responses will largely mimic their parents’
reacting in particular ways. • disturbed attachment patterns and therefore the more disorganised
and inconsistent the parent, the more
• rapid behavioural regressions disorganised the child (Streeck-Fischer &
Early brain development and shifts in emotional states Van der Kolk, 2000). Without the security
Disruptions to normal brain development • loss of autonomous strivings and support from a primary caregiver,
in early life may alter later development • aggressive behaviour against self babies and infants may find it difficult to
of other areas of the brain. Researchers and others trust others when in distress, which may
investigating brain development • anticipatory behaviour and traumatic lead to persistent experiences of anxiety
have used the term ‘toxic stress’ to expectations and anger (Streeck-Fischer & Van der
describe prolonged activation of stress Kolk, 2000).
management systems in the absence • lack of awareness of danger and
of support (Bromfield, Gillingham & resulting self endangering behaviours
Higgins, 2007). Stress prompts a cascade • self-hatred and self blame and chronic
of neurochemical changes to equip us feelings of ineffectiveness (Van der
to survive the stressful circumstance Kolk, 2003).
or event. However, if prolonged (e.g. if
a child experienced multiple adverse
circumstances or events), stress can
disrupt the brain’s architecture and
stress management systems leading
to hypersensitivity and over activity.
Children who have experienced ‘toxic
stress’ or severe disruptions to early
brain development may find it difficult
to regulate their own behaviour or
emotional reactions. Toxic stress may
sensitise children to further stress,
lead to heightened activity levels and
affect future learning and concentration
(Shonkoff & Phillips, 2001).
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 5
Practice Resource Guide
Resilience
There are two ways of thinking about resilience: point in time resilience
and a life course approach to resilience.
Point in time resilience Process or life course Understanding resilience
Taking this perspective you might ask approach to resilience Infants are born with their own unique
“How resilient is this child now?” or Taking this perspective you might temperament – some are highly resilient
“How resilient or vulnerable was the observe that “This child has adapted while others are more fragile. Intrinsic
infant at birth?” This is reflected in this relatively well to trauma and adversity factors such as a child having an easy
definition by Gilligan: “Resilience can over the course of their development” temperament as a baby are highly
cushion an individual from the worst or ask “What risks or strengths have associated with resilience in infancy.
effects of adversity and help them to surrounded the child to increase or Other babies may have a more difficult
cope, survive and even thrive in the decrease their resilience?” or “What temperament and could therefore
face of great hurt and disadvantage” interventions can we provide to struggle to thrive without the optimal
(Gilligan, 1997). build resilience in this child who has environment. However, an individual’s
experienced adversity and trauma?” level of resilience is not static, rather
This perspective is reflected in this it is dynamic and evolves and changes
The Benevolent Society’s definition by Luthar: “Resilience is over time in relation to the individual’s
definition of Resilience: a phenomenon or process reflecting life experiences.
relatively positive adaptation despite
Strength in the face of experiences of adversity or trauma”
For example, all children have aspects
adversity. The capacity to of individual vulnerability and resilience.
(Luthar & Zelazo, 2003, p. 6).
Outside the child are external forces or
adapt and rebound life events comprising: (a) risk factors,
from stressful life events experiences of trauma and adverse
events; and (b) protective factors,
strengthened and more positive experiences and potential
resourceful. sources of strength. An individual’s
6 RESILIENCE PRACTICE FRAMEWORK The Benevolent Society
Practice Resource Guide
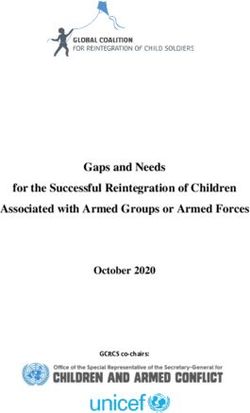
experiences of these external forces Figure 1: Domains of Resilience
can increase or decrease their levels of
vulnerability or resilience.
Resilience Practice
Framework
The Resilience Practice Framework
focuses your attention when making
assessments on gauging the child’s
vulnerability or resilience. Even the
most resilient child can struggle given
enough pressures in their environment.
Conversely, even the most fragile child
can thrive with the right care. The
Resilience Practice Framework focuses
your assessment on identifying the
strengths as well as the problems in
the child and family system (individual,
family, community) that may increase
or decrease the child’s resilience.
When working with children and their
families, use the Resilience Practice
Framework to guide your intervention
to increase the protective factors and
potential sources of strength as well as
addressing the problems and risk factors
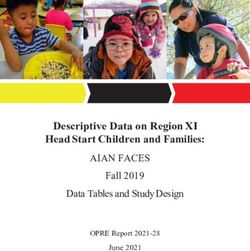
in the child and family system. The Figure 2: The Ecological Framework
underlying philosophy of a resilience-led
approach is that all children can survive
Wider Community
and thrive despite experiences of trauma
and adversity if they are given the right
care and nurturance.
A resilience model developed by Daniel Family Relationships
& Wassell (2002) highlights that there are
six domains of resilience (see Figure 1).
The Benevolent Society uses the
‘domains of resilience’ model as a means Child
for driving assessment and intervention.
The model is used in combination
with an ecological framework that
demonstrates the levels at which
resilience factors can be located.
In practice this means that practitioners
focus on all three levels (child, family
relationships and the wider community)
when considering how to assess
and boost resilience in a child’s life.
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 7
Practice Resource Guide
For example, when thinking about a Cumulative harm and Working in a culturally
secure base (see Figure 1: Domains of
Resilience) one issue to consider for the
resilience sensitive way
Cumulative harm can overwhelm While many of the aspects of a
child might be “does the child appear
even the most resilient child and resilience-led approach are common
to feel secure?”. When considering
particular attention needs to be given across all cultures, it may be that
family relationships: “is the parent/
to understanding the complexity of the what is valued in one culture is not
caregiver able to make time for the
child’s experience. Families in which directly transferable to another and
child?”. When considering the wider
children are exposed to cumulative this should be taken into account when
community: “does the parent/caregiver
harm often lack strong protective working with families of different
have adequate emotional and material
factors and are characterised by a range ethnic and cultural backgrounds. For
resources to support him or her in the
of complex problems that can break example, research indicates that while
parenting of the child?”. Each of the six
down a child’s resilience. These may friendships are generally beneficial
individual domains of resilience should
include social isolation, family violence, for children across all cultures,
be considered in relation to the three
parental substance abuse, mental health the ways in which friendships are
levels of the ecological framework.
problems, disability and socio-economic conceptualised and levels of closeness
For more information about the disadvantage. Even the most resilient within friendships may vary depending
Domains of Resilience model see: Daniel child can struggle to grow in such on cultural expectations (French et
and Wassell, 2002. unrelenting conditions. al., 2005). Whilst there are certain
universal childhood needs, concepts
For this reason, we must be cautious
of attachment and understandings of
not to focus on resilience to the extent
who are the important people around
Cumulative harm can that we ignore the risks for the child.
children can vary across cultures.
overwhelm even the most Children who appear to be coping
Therefore it is important to respect
well, but who in fact have internalising
resilient child. symptoms (e.g. depression, lack of
different kin and non-kin structures
for caring for children, whilst retaining
self-worth), are vulnerable to being
a focus on the child. Culture has an
overlooked (Luthar & Zelazo, 2003). In
important effect on the significance and
cases where children have experienced
meaning of certain stressors, such as
cumulative harm the focus of an
disability, health difficulties and divorce
intervention must be on reducing the
(Luthar, 2003) as well as differing family
adversity in the child’s life, assisting
formations, aspirations and beliefs
their recovery and increasing their
(Schoon & Byner, 2003). Some ethnic
resilience to future adversity.
groups will be disproportionately
In gathering information, analysing, disadvantaged and have limited
intervening and reviewing our work access to good housing, resources and
with families where there is cumulative employment.
harm, we must be mindful of whether
there is improved safety and wellbeing
for children and adolescents. The short
and long term effects on them matter,
whether there is intent to harm or not.
In conjunction with your supervisors,
you will need to review the family
support plan and at times this may
mean involvement of child protection
services.
8 RESILIENCE PRACTICE FRAMEWORK The Benevolent SocietyPractice Resource Guide
Aboriginal and Torres Strait The Benevolent Society and The aim of this Practice Tool is to
provide specific guidance on what to
Islander children and families cumulative harm consider in responding to cumulative
and cumulative harm Practitioners working for the
harm for both:
Cultural competence, sensitivity Benevolent Society who work with
(a) children and families with no
and respect are essential in any children, parents or families need to:
previously identified concerns; and
intervention with families. The impact • be alert to signs that a child might be
of historical and ongoing dispossession, at risk of cumulative harm even if they (b) children and families with identified
marginalisation, racism, colonisation, have no previously identified concerns concerns.
poverty and the Stolen Generations has (e.g. child care worker)
led to high levels of unresolved trauma, • be able to make a “cumulative
depression and grief among Aboriginal harm assessment” for children with
and Torres Strait Islander families identified concerns (e.g. parenting
and communities (Human Rights and support)
Equal Opportunity Commission, 1997). • understand ways to intervene with
Some of the key individual, family and children and their families to decrease
community vulnerabilities associated the risk of cumulative harm and
with unresolved trauma have resulted enhance children’s resilience, and
in heightened rates of child abuse
and neglect in Aboriginal and Torres • review the effectiveness of their
Strait Islander communities (Berlyn & intervention.
Bromfield, 2010). It is not surprising The type of cumulative harm
that, without this crucial modelling and assessment you undertake and the
positive parenting experiences, the response you provide will differ
legacy for future generations is fraught for different roles and services and
with difficulties in their parenting may depend on how the child and
styles for many Aboriginal and Torres family came to be involved with the
Strait Islanders who were removed Benevolent Society.
from families and communities. In • If you are in a child care setting and
this context Aboriginal and Torres have identified signs that a child
Strait Islander children living in such might be at risk of cumulative harm,
communities are more vulnerable to the purpose of your assessment will
cumulative harm. be to identify if there is cause for
concern and determine what the
most appropriate service is to which
Culturally and linguistically
you can refer the family (e.g. child
diverse families and protection or a parenting program).
cumulative harm • If you are working in a family support
Refugee and migrant communities or therapeutic service (e.g. Child and
may be struggling with unresolved Family or Early Years Centre), you
trauma, grief and loss after fleeing might have accepted a referral from
from war, oppression, torture and child protection authorities and your
trauma. Adjusting to a new culture and cumulative harm assessment will be
way of life can also put further stress undertaken to inform your planning
on families and increase children’s and intervention with the child and
vulnerability. their family.
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 9Practice Resource Guide
Practice Tool: Working with children and families
with no previously identified concerns
Children experiencing multiple and ongoing low-severity adverse events
are more likely to be overlooked as we tend to think about our concerns
for children in terms of individual events. However, an ongoing pattern of
adversity can cause a child to experience cumulative harm. All professionals
working with children need to be aware of the impacts of cumulative harm
and alert to children who might be at risk of cumulative harm.
• Are there children you come into summarise the information according • Source of harm: To the best of your
contact with where you have noticed to the following dimensions: knowledge, who is responsible for the
ongoing, minor events that, while not • Type: Are there multiple types things that you are concerned about
optimal, are not cause for concern on of events causing you concern (e.g. mum, dad, both)?
their own? (e.g. child’s behaviour, parent’s • Severity: Does this seem to have
• If you are concerned about a child, presentation, parent–child affected the child’s development?
what is your primary concern? Are interactions)? What would be the likely
there other things that you have also • Frequency: Has the issue(s) that impact on the child if these
observed which may be indicative of you are concerned about occurred circumstances continued?
an underlying problem? repeatedly or was it a one-off event? On balance, do you believe this child
• Talk to your colleagues, have they • Duration: To the best of your might be at risk of cumulative harm?
noticed anything? (when considered knowledge, how long has the issue(s)
in isolation it may have seemed you are concerned about been Remember, cumulative harm refers
insignificant). present? Is it an ongoing pattern to the effects of multiple adverse
in the child’s life or is it associated circumstances and events in a child’s
Having gathered your own observations life, the unremitting daily impact of
and those of your colleagues, with a current stressful situation
or crisis for the family? which can be profound and exponential.
10 RESILIENCE PRACTICE FRAMEWORK The Benevolent SocietyPractice Resource Guide
If you believe a child to be at risk of need to reassess whether or not a
cumulative harm, it is important that report to child protection authorities
they are linked to appropriate services. is warranted. Remember to keep
Services to support the child and family children’s outcomes as central to your
might include parenting programs, family assessment of risk and wellbeing.
support, the Brighter Futures program,
the Helping Out Families program,
mental health services, drug and alcohol Mandatory Reporting Obligations
services, maternal and child health
nurses. Ensure that you discuss your Cumulative harm and the NSW mandatory reporters from taking action
concerns with your supervisor. If you Children and Young Persons in a way they believe is appropriate.
believe the child is at risk of significant (Care and Protection) Act 1998
Cumulative harm and the Queensland
harm, then you will need to make a The NSW Children and Young Persons Child Protection Act 1999
report to child protection authorities. (Care and Protection) Act 1998
Under the QLD Child Protection Act
specifically addresses the issue of
You will come into contact with children 1999 a matter must be reported to
cumulative harm. Under the Act a
who you are concerned about, but who child protection authorities if it is
matter must be reported to child
are not presently at risk of significant deemed that the child is at risk of
protection if the child is at risk of
harm. It is important that they are given harm. Harm to a child is defined as “any
‘significant harm’ S.23 (1). The Act states
the opportunity to access appropriate detrimental effect of a significant nature
that significant harm ‘may relate to
services. on the child’s physical, psychological
a single act or omission or to a series
• Talk to the parent. Let them know or emotional wellbeing” S. 9 (1).
of acts or omissions’ S.23 (2).
that you are concerned for them and
their child. Mandatory Reporting (QLD)
Mandatory Reporting (NSW)
• Engage them in a discussion about The QLD Child Protection Act 1999
The NSW Children and Young Persons
whether there are supports they requires that an authorised officer,
(Care and Protection) Act 1998 states
might find useful. You might provide employee of the department or a person
that a mandatory reporter is
them with information about other employed in a departmental care service
“(a) a person who, in the course of
services available through the or licensed care service is required to
his or her professional work or other
Benevolent Society (e.g. The Early report harm or suspected harm to a
paid employment delivers health care,
Years Centres, Partnerships in Early child in the care of a departmental care
welfare, education, children’s services,
Childhood program; supported service or a licensee S. 148. For further
residential services, or law enforcement,
playgroup); or provide them with the information regarding mandatory
wholly or partly, to children, and
contact details for a parent helpline reporting and how to make a report
(b) a person who holds a management
or a referral service. to child protection authorities visit:
position in an organisation the duties
www.communities.qld.gov
• Be careful when talking with parents of which include direct responsibility for,
not to sound accusatory, as this may or direct supervision of, the provision
alienate them and ultimately prevent of health care, welfare, education,
them seeking the help they need. children’s services, residential services,
• Parents may decide that they do not or law enforcement, wholly or partly,
wish to access support at that time, to children.” S.27.
let them know that ‘your door is Refer to the online Mandatory Reporter
always open’ if they want to discuss Guide http://sdm.community.nsw.gov.
anything with you. au/mrg/screen/docs/en-GB/summary to
• If parents choose not to access assist you to determine whether or not
available support services, you will to make a referral to child protection.
need to monitor the situation. If the Note: The Guide is not intended to
problems appear to escalate you will replace critical thinking or to stop
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 11Practice Resource Guide
Case Study: Daniel and Linda
You are a child care worker and are worried about four year old Daniel who has
been attending the centre for the last 12 months for one day a week. Daniel is
dropped off at the centre by his Mum Linda. Over the last few months you have
started to put together lots of little things about Daniel and Linda and you are
becoming concerned about Daniel’s wellbeing.
If you believe a child is at
risk of significant harm, you
need to make a report to
child protection authorities.
You will come into contact
with children who you are
concerned about, but who
are not presently at risk of
Daniel Linda
• Daniel has always been shy and • Linda often drops Daniel off or picks
significant harm. Ensure that
withdrawn. He doesn’t tend to play him up significantly later than the you discuss your concerns
with other children. times she had booked. Sometimes with your supervisor. It is
• He can be aggressive towards staff she fails to bring him in at all. Linda
and other children when disciplined generally has explained that this important that the family
and/or asked why he does not want is because “they have had a bit of is given the opportunity to
to play. trouble getting ready”, “lost track of
time” or “slept in”. access appropriate services.
• You’ve noticed that Daniel doesn’t
tend to ‘try new things’ and that his • Linda has always been difficult to
language skills are not as developed engage and has often appeared
as most of the other kids his age. distracted as if she has had other
things on her mind—she doesn’t
• At times Daniel has been
tend to ask about how Daniel’s day
inappropriately clothed for the
was.
weather conditions.
• Another member of staff
• On some occasions you have
mentioned to you that she heard
noticed that he appears quite
Linda telling Daniel in the car park
hungry, having multiple serves at
that he was “bad” and that she
lunch and snack times.
would “send him away to the home
for naughty boys”.
12 RESILIENCE PRACTICE FRAMEWORK The Benevolent SocietyPractice Resource Guide Practice Tool: Working with children and families with identified concerns The aim of this tool is to provide some additional guidance to Benevolent Society practitioners about specific things you might consider when a child might be at risk of cumulative harm. The tool consists of four sections representing each phase of casework: assessment (including information gathering and analysis), planning, intervention and reviewing outcomes. Phase 1: Assessment In this part of the tool, we provide should be individualised and respectful single recurring adverse circumstances specific tips and guidance for the of families’ unique strengths and needs. or events, or by multiple different assessment phase of your work with There are two steps involved in circumstances and events, cumulative children, parents or families where assessment: harm may be a factor for any child there is suspected cumulative harm. (1) information gathering; and who has experienced, or is at risk Comprehensive assessment is an (2) analysis. of experiencing, abuse or neglect. ongoing process of gathering, analysing, However, it is unlikely that a child will comparing and synthesising information be referred for services explicitly due from various sources in order to come INFORMATION GATHERING to concerns about ‘cumulative harm’. to an understanding of family strengths Families who self-refer or who are This means that practitioners need to and needs relating to the child’s safety referred to the Benevolent Society be alert to the possibility of multiple and wellbeing (U.S Department of for parenting or family support or for adverse circumstances and events Human Services, 2008). As all families therapeutic services are vulnerable and impacting children in all vulnerable have their own unique strengths and will often be experiencing multiple and families with whom they interact. needs, there is no ‘one size fits all’ complex problems. As cumulative harm model for assessment. Assessment may be caused by an accumulation of The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 13
Practice Resource Guide
Practitioners who engage effectively Gather information from
Practitioners need to be with families:
multiple sources
• treat family members with respect
alert to the possibility of and courtesy
Practitioners need to gather information
from multiple sources to form an accurate
cumulative harm in all • focus on building on the picture of the child and their family.
vulnerable families with family’s strengths
Case files and referral information can
whom they interact. • promote positive relationships among provide a rich source of information
parents and children about the child and their family, their
• develop trust through sensitive previous involvement with support
Engaging families and inclusive enquiry about their services and provide a good starting
circumstances point for information gathering. The case
While your role may be to gain an
• take an active, caring, whole-of-family history and referral will often provide
understanding of parenting constraints
approach to their situation the initial alert that a cumulative harm
and how these are impacting children,
• link up with other relevant services assessment is required.
starting a conversation by asking
about or raising parenting problems and work together to avoid conflicting Speak to other professionals and
is unlikely to create an emotionally requirements and processes services involved with the family:
safe environment for parents. This • focus on the children’s needs, and • Ask other professionals specifically
may adversely affect your capacity to • maintain a continuous relationship about the potential or actual impact
gather information effectively; at worst with the family (McArthur, Thompson, of family problems on children and
it may damage your ability to build a Winkworth & Butler, 2009). the potential for cumulative harm.
relationship with the parent over time • How have other service systems
and reduce the efficacy of your practice. intervened in the life of the family?
Parents’ and children’s openness to First impressions last, so • Have you consulted with other
engaging with services may also be cultural services if appropriate?
affected by their past experiences
think carefully about how
• Keep in mind that any professional
with formal services and supports. For you are going to engage opinion is of itself limited by the time,
example, in a recent study McArthur the family to make your role and focus of the practitioner (e.g.
and colleagues (2009) found that some impression positive. Effective maternal and child health nurses who
of the barriers and disincentives to
parents accessing services were:
engagement will require you only see the infant for brief periods
once a fortnight, or the drug and
• past experiences of feeling to build a trusting relationship alcohol practitioner who is focused
discriminated against or treated with all family members. on the adults’ recovery not their
unequally due to their situation parenting capacity).
• feeling humiliated and embarrassed
Professional knowledge is just one type
by their circumstances and fearful
of knowledge:
their children would be removed
• Parents are experts about their family
• being judged as not needy enough or and their children and it is important
not meeting set criteria to talk to them about their views of
• feeling it was up to them to make what are the strengths and stressors
contact with the right person the first for their family.
time. • Think broadly about extended family
and other key people in the child’s life.
• Last, but by no means least, it is
critical that the child’s subjective
experience be central to your
information gathering to identify the
impact of cumulative harm.
14 RESILIENCE PRACTICE FRAMEWORK The Benevolent SocietyPractice Resource Guide
Talk with and observe Refer to the following resources to aid What are the family strengths
your observations of child development,
the child trauma and attachment:
and stressors?
You can get a good sense of what the At the beginning of your involvement,
family environment is like for the child • Infant/Toddler Learning Foundations it will be important to put together a
by watching and interacting with them, Book and DVD, California Department comprehensive and detailed picture
keeping in mind whether and how their of Education of the family—its history and current
demeanour and presentation may • Department of Human Services, circumstances, strengths and needs
reflect the impact of cumulative harm. Victoria Child Development and and the impacts of those circumstances
• How does the child present? Watch Trauma Guides on the safety and wellbeing of the
for developmentally-appropriate • Circle of Security Maps children. As the case progresses existing
play, communication, and emotional • Marte Meo child elements checklist information will need to be updated and
responses; comfort-seeking behaviour new information will need to be sought,
• The Benevolent Society’s Resilience and both assimilated into the family
when distressed; parent-child
Assessment Tool. support plan.
interactions; and the child’s responses
to strangers. If you observe signs that the child is not Research has shown that families in
• Which toys are used in play and how developmentally on track or is showing which children experience cumulative
are they used? How does the child signs of trauma you may consider harm are frequently characterised
interact and play with other children? referring the child to a specialist for a by multiple and complex problems
formal assessment. (Bromfield, 2005). Where families have
• Ask the children about their day. What
are their routines? What happens multiple, chronic and inter-related
after school? Talk to parents about problems, this can result in children’s
needs being unmet (Cleaver, Nicholson,
• Ask about their home and family life. their child Tarr & Cleaver, 2007; Cleaver, Unell &
Who lives in their house? Who comes Parents’ love for their children and
to visit? Who looks after them? What Aldgate, 1999). Families with multiple
motivation for them to be safe and well
makes them happy? What makes and complex problems are frequently
will be the primary reason parents come
them sad? What is the child saying/ socially isolated and lack strengths or
to the Benevolent Society for support.
not saying? What does this tell us? protective factors (Bromfield, 2005).
Give parents space to talk about their
Make your observations and hopes and dreams, worries and fears
interactions with children purposeful. for their children. You will get rich
What do your observations and information about the child and start
interactions tell you about child to build a relationship with the parent
development, trauma, attachment and around your shared aim of achieving the
resilience? Keep in mind that parents best outcomes for their child.
and children may behave differently • Parents are experts about their
in the contrived and often stressful children and will be an important
situation of an assessment. Avoid source of information about whether
making definitive assessments about children are developmentally
parent–child relationships too early. ‘on track’ and able to relate, play,
It might be important to make multiple concentrate, participate and belong.
observations in different settings/ • Are there any characteristics of
environments. the child making it hard for the
• Is the child meeting developmental parent to meet their child’s needs
milestones? (e.g. disability, medically fragile,
• Is he or she displaying any signs behavioural problems)?
of trauma? • Ask parents, are there any
• Are there any indications that the characteristics of this child that
child has attachment difficulties? may strengthen or undermine
their resilience?
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 15Practice Resource Guide
What problems are being Context of the problem(s) Responses within families are diverse
experienced? Ask the parent about other aspects and some are able to create supportive
Which are the primary problems of their life. Is this family living and nurturing environments despite
contributing to the parent’s current within a broader context of poverty, parental problems. What are the
circumstances? Identify the events or disadvantage and social isolation? strengths that families can build upon?
behaviours that have brought the family Consider how a context of disadvantage You might need to start small, such as
to the notice of your service — what and exclusion might be compounding recognising the parent’s love for their
happens and when, how often, who the effects of other problems or creating child and desire for them to be happy
is involved? What are the impacts on barriers to the parent’s ability to deal and well, even when parents themselves
the parent as an individual? How does with their problems. Also explore what cannot meet their child’s needs.
this situation impact their capacity to steps or actions are being, or have • How willing are the parents to seek
parent? been, taken by the parent (alone or with support services?
• What have the parent’s experiences the aid of another service provider) • Is there a strong parent–child
been? to address or manage their problems. attachment?
• What is the repeating and/or current Have these been effective? • How has the family tried to manage
pattern around the concerning • Does the family have adequate the problems before coming to the
behaviours? housing? Benevolent Society?
• How is the parent’s mental, emotional • Are the parent’s in employment?
For further information on gathering
and physical wellbeing? • Are the parent’s struggling with information to form your assessment
• Do they have ongoing issues that may money problems? Can they pay their refer to the Benevolent Society’s
affect their parenting capacity (e.g. bills and buy groceries? Resilience Assessment Tool and User
disability or mental illness)? • Does the family have access to Guide.
• How have the parent’s circumstances transport? Is this affecting their
or problems impacted on their capacity to meet their child’s needs?
relationship with their child? • Do they feel safe and supported in
• With appropriate support, is the their neighbourhood?
parent likely to be able to provide an • Does the family have supportive
adequate level of care to their child? networks within their community (e.g.
access to local services)?
• Are the family support networks,
or lack thereof, a source of stress or
support?
• What kind of relationship does
the parent have with friends and
extended family? Are the parent’s
social networks making it hard for the
parent to change (e.g. their friends
also have substance addictions)? Is
the parent isolated? Are the parent’s
family or friends a potential source of
support?
• What strengths can the parent/family
build upon?
16 RESILIENCE PRACTICE FRAMEWORK The Benevolent SocietyPractice Resource Guide
Tips for engaging parents
Parents may be struggling to meet Ask parents: • What would you like for your family
their children’s needs, but this does • What does a good day look like? down the track? Do you have any
not mean that they do not love their What does a bad day look like? particular goals for your family?
children, want to be good parents • In parenting your children, what things • Who else in your family/kinship group
or that they do not have hopes and do you think you do pretty well? is involved in the care and upbringing
aspirations for their family. Experienced of your children?
practitioners suggest: • What do you see are the main issues
of concern for your family? Practitioners should demonstrate
• asking parents about their hopes,
dreams and aspirations for • What things would you like assistance warmth and acceptance and avoid the
their children with at the moment? ‘expert role’ by presenting ideas and
• What might be barriers to you strategies as choices or options the
• being honest with parents about family can choose to help them care
your concerns. getting this help? E.g transport
or child care issues. for their children.
Tips for engaging children
Remember that the child may be • Don’t ask too many questions as it can drawing) — they can choose when to
scared and confused about what is shut a conversation down. make eye contact, and can take a bit
happening, but also aware of some of • Ask specific questions “can you tell of time to think about their answer.
the consequences of disclosure. Talking me exactly what happened?”. Their • If the child is engaged in play, name
with you may raise concerns for them responses will suggest follow up what they are doing. For example:
about being loyal to their parent — even questions. “Oh, I see you have the blue truck”,
an abusive parent. then wait for their next initiative. This
• Ask the child about events, feelings
• Meet the child at their level — kneel and routines rather than themselves. lets the child know that someone is
on the ground with them, join them with them in their play and that they
• Ask the child what they would like to
on the swings. have good play ideas, which is very
happen — what would they like to
• Make eye contact. important for social development.
change?
• Ask open ended questions that invite • Offer simple, direct responses to their
• Avoid asking the very difficult
a conversation not a quick response. questions.
questions too early in the
Sources: Noble-Carr (2006); the Raising Children
• After asking a question of a child conversation.
Network (raisingchildren.net.au)
ensure that you leave enough time for • Let them know you are taking them Aarts, M. (2008). Marte Meo Basic Manual (2nd
the child to consider the question and seriously — don’t interrupt. Ed.) Arts Productions, Eindhoven, Netherlands
make a response (active waiting).
• Younger children in particular may
• Tell children why you are there and feel more at ease if you talk with them
working with the family. while taking part in an activity (e.g.
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 17Practice Resource Guide
Case study: James and Diane
James and Diane self-referred to • Diane’s addiction to prescription • Diane seems to have a good
the family support program at the drugs has meant that at times she relationship with one of the Centre
Benevolent Society’s Browns Plains has been unable to get out of bed to workers who initially suggested
Early Years Centre (BPEYC) as Diane wash, feed and dress James in the she might access support from a
was having difficulty staying on top morning. She says that she finds this family support worker. From her
of daily routines and managing a ‘chore’. observations working with James
James’s behaviour. You have been • Her parenting style is unpredictable. in child care, the centre worker has
working with them over the past few When on a ‘particular high’ she says informed you of the concerns she
weeks, assessing information to inform she often plays with James and gives has with James’s development.
your planning and intervention with him gifts. At other times she says she • Although James has been a little
the family. ‘can be off in her own little world and more withdrawn in the last few
Over the course of two one-hour forget that James is there’. On one weeks, no further concerns have
sessions with Diane at the BPEYC while occasion she left James in a shopping arisen since Diane sought further
James is in child care, Diane has openly centre. support.
discussed the parenting difficulties • Diane says she has difficulty
she is having and has revealed managing James’s behaviour and has
several personal problems that have sometimes lost control and smacked
been affecting her ability to provide him harder than she intended.
adequate care to James. From your • Diane also revealed having a history
sessions you have ascertained that: of abuse and neglect in her own
• Diane and James live in a public childhood, culminating in her and
housing unit in a neighbourhood her sister being cared for by her
they experience as unfriendly and, grandparents when she was 15 after
at times, scary. her mother overdosed for a second
• Diane supports herself and James by time. Her mother is deceased and
receiving welfare support benefits, she does not have any contact with
however she is behind on the rent. her father.
• James has never met his father. • Diane knows that the drugs are
His father lives interstate and not helping her, particularly her
wanted nothing to do with Diane or ability to cope with James, however,
James once he found out Diane was she says that when she is not on
pregnant. drugs she feels alone and worthless.
• You suspect Diane suffers from Sometimes she has felt like killing
depression, the symptoms of which herself.
have intensified since James’s birth. • Diane says she loves James with
• Diane has been self-medicating with all her heart and wants the best for
prescription drugs by consistently him. However, she is worried that
changing doctors and often uses if she does not get back on track
marijuana to ‘numb the pain’. and get support ‘that the same
thing might happen to James that
• The drugs she takes to ‘help her happened to her’.
through’ include Duromine and
Xanax.
18 RESILIENCE PRACTICE FRAMEWORK The Benevolent SocietyPractice Resource Guide Practice Resource Guide
ANALYSIS • Do children have a regular routine? Talents and Interests
In analysing the above information, you Having a routine is important • What things do you really like to do
need to be a critical thinker and juggle for children as it provides them (in or out of school) – things you are
multiple competing needs prioritising with consistency, and makes the interested in (e.g. hobbies, sports,
the child’s safety and development. world more predictable for them. games, music/dance, art, craft)?
Careful attention needs to be given However, having a routine is not the • Where do you do it? How often?
to the balance of risk and protective same as having a rigid or inflexible Who do you do those things with?
factors, strengths and difficulties in daily schedule.
• What things are you pretty good at?
the family. Synthesise the information • Are parents spending time with
you have gathered about the current children providing them with the
context and the pattern and history nurturance, attention, love and Social Competencies
and weigh the risk of harm against the affection they need for positive • Do you spend as much time
protective factors. emotional development? as you would like with other
children your age?
The signs that a child was experiencing • What do you think the child might
name as the good and bad things • Do you usually get on OK with
cumulative harm are frequently
about their daily lived experience? other children?
evident with hindsight. A cumulative
harm assessment does not require • Do you find that you fall out with
practitioners to collect different or friends easily?
Resilience-based analysis
additional information. Rather, it To further assist in your analysis, For further details see Brigid Daniel
requires careful analysis and re-analysis practitioners can use a resilience-based & Sally Wassell, 2002 and The
of the information you routinely collect, analysis method to guide your Benevolent Society’s Resilience
and the continuous re-assessment assessment. Examples of questions Assessment Tool – Child Resilience.
of information you gather over time used for school-aged children in
through the course of your involvement
with children and families. Discuss the
the Benevolent Society’s Resilience Be alert to chronic neglect
Assessment Tool include: It is particularly relevant to be alert
information and your analysis with
to the possibility of cumulative harm
your supervisor.
Secure Base in cases of chronic neglect that are
• Who is the person who most cares characterised by an unremitting
Put together a picture of about you and loves you? low-level of care. The cumulative effects
what’s happening in the • Who are the people you really of chronic low-level neglect are easily
care about? missed as the term ‘abuse’ connotes a
child’s daily life ring of urgency that ‘neglect’ does not
Put the pieces of your information • Who do you see?
and the effects of neglect are usually
together to create a picture of the
not as obvious. Frederico, Jackson
child’s daily life. Imagine the situation Education
and Jones (2006) caution “It is critical
through the child’s eyes, what are • How are you going with school work?
that neglect is not considered a
the characteristics of their daily • Who (adults) takes an interest in how lesser problem than other forms
lived experience? well you do at school? of maltreatment” (p. 18).
• Are the child’s basic daily needs being • Does (caregiver/s) come to stuff at
met: sleeping, eating, hygiene? school much? What?
• How are children spending their time?
Are they playing and interacting? Friends
Going to school or child care? • If you hear the word ‘friend’, what
Spending extended periods without does it mean to you?
interaction in their pram or in front
of TV? • What things about you would make
people want to be your friend?
• How many friends do you have?
The Benevolent Society RESILIENCE PRACTICE FRAMEWORK 19Practice Resource Guide
Assessing parenting capacity It is critical that you do not assume • Duration: Over what period of time
culture is a risk factor — culture can be has the child experienced these
in Aboriginal and Torres Strait protective for children. For example, adverse circumstances and events?
Islander and CALD families culture and the maintenance of Link this back to the child’s age and
Parenting practices are not universal culture are central to healthy infant developmental stage and whether
and practitioners must be careful not development and identity formation this makes them more or less at risk
to impose their own cultural practices, in Aboriginal and Torres Strait Islander of harm.
values and beliefs about parenting communities. An Aboriginal child knows • Severity: What has been the impact
onto families with whom they are who they are according to how they of the circumstances or events on the
working. Cultural consultations can relate to their family, community and child’s development and wellbeing?
play an important role in this part of land (Victorian Government Department What is the likely impact if the
the assessment — who can you call of Human Services, 2008). Practitioners adverse circumstances and events are
on for input in relation to this specific will need to assess whether, in the repeated over a prolonged period?
family? Your role is to assess whether present circumstances, traditional,
children are safe from harm and are • Source of harm: Who is responsible
cultural parenting practices are
receiving the physical care, affection for the child experiencing these
contributing positively to the child’s
and emotional security they need. Be adverse circumstances and events
safety and wellbeing, or putting them
cautious that you are not imposing (one person or multiple people)?
at greater risk of harm and neglect.
upon families how they must parent to Does the situation make the child
Be aware that culture and parenting
meet these needs. For example, in some vulnerable to other perpetrators of
practices are not homogenous and
cultures the mother may not be the abuse or neglect (e.g. extra-familial
can vary across families, communities
primary attachment figure for an infant. perpetrators)?
and geographic areas. Practitioners
If there are multiple caregivers your role will need to determine which practices To explore these dimensions you might
is to observe the infant and “to assess are applied in the family they are ask yourself questions such as:
whether the infant seems confident of working with (Neckoway, Brownlee • Have you been aware of similar issues
who to turn to when in need, whether & Castellan, 2007). in the past? If so, have the problems
there is a central person who holds the escalated?
infant and their needs in mind, and to
ensure that the infant does not have to Make a cumulative harm • Are there indicators that the child has
experienced other types of adversity
attempt to get care from many people assessment in addition to those you are aware of?
to get their physical and emotional Draw together all of the information you
needs met” (Jordan & Sketchley, 2009). have collected. To identify whether a • Have the alleged circumstances
child is at significant risk of experiencing caused, or are they likely to cause,
cumulative harm it is important to significant harm if they are repeated
summarise the information along the over a prolonged period?
Practitioners need to be
following dimensions: Put the child at the centre of your
aware of their own values • Type: What are the range of adverse assessment:
and how these might circumstances and events that • How long have the problems in the
influence the way they work the child has experienced? Make family been present?
with families from culturally particular note of any types of • How are parental problems and family
abuse or neglect that the child may
and linguistically diverse have experienced or be at risk of
circumstances impacting the child?
backgrounds. experiencing. • Does the child’s development present
as being socially and physically
• Frequency: From your knowledge of on track?
the child’s history, is there a pattern
of these circumstances or events
being repeated?
20 RESILIENCE PRACTICE FRAMEWORK The Benevolent SocietyYou can also read