Guidance on the Monitoring of Salt Iodization Programmes and Determination of Population Iodine Status - Unicef
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Guidance on
the Monitoring
of Salt Iodization
Programmes and
Determination of
Population Iodine
Status
Guidance on
the Monitoring of Salt Iodization
Programmes and Determination
of Population Iodine Status
Photograph Credits:
On the cover:
©UNICEF/UNI12403/Holmes
©UNICEF/UNI161903/Holt
©UNICEF India/Pirozzi
©UNICEF/UNI190087/Quarmyne
Contents
©UNICEF/UNI42383/Tkhostova Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
©UNICEF/UNI189127/Quarmyne Summary of key recommendations . . . . . . . . . . . . . . . . . . . . . 5
Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Design of iodine nutrition surveys . . . . . . . . . . . . . . . . . . . . 9
Assessment of household coverage of iodized salt and
measurement of salt iodine content . . . . . . . . . . . . . . . . . . 11
Assessment of iodine status in population-based surveys . . . . . . 15
Technical Annex . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Analysis and presentation of household iodized salt
coverage data from surveys . . . . . . . . . . . . . . . . . . . . . . . 21
Analysis and presentation of data on iodine status . . . . . . . . . . 23
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
©UNICEF India/Pirozzi
©UNICEF/Marco Dormino
©UNICEF/UNI189119/Quarmyne
Acknowledgements
This document builds on the results obtained during a Technical Working
Group Meeting on Research Priorities for the Monitoring of Salt Iodization
Programmes and Determination of Population Iodine Status, which took
place in New York on 17–18 December, 2015.
UNICEF thanks the following experts for providing comments on the
document: Maria Andersson (Swiss Federal Institute of Technology),
Atmarita (Indonesia Nutrition Foundation for Food Fortification), Jessica
Blankenship (Independent Consultant), Omar Dary (United States Agency
for International Development), Aashima Garg (United Nations Children’s
Fund), Greg Garrett (GAIN), Robin Houston (Iodine Global Network), Noor
Khan (Nutrition International), Jacky Knowles (Independent Consultant),
Roland Kupka (United Nations Children’s Fund), Zivai Murira (United Nations
Children’s Fund), Banda Ndiaye (Nutrition International), Chandrakant Pandav
(All India Institute of Medical Sciences), Elizabeth Pearce (Boston University),
Lisa Rogers (World Health Organization), Fabian Rohner (GroundWork), Ruth
Situma (United Nations Children’s Fund), Arnold Timmer (Global Alliance for
Improved Nutrition), Frits van der Haar (Emory University), Bradley Woodruff
(GroundWork), Kapil Yadav (All India Institute of Medical Sciences), and
Michael Zimmermann (Swiss Federal Institute of Technology).
UNICEF also thanks the United States Agency for International Development
for providing financial support for this work.
iv 1
©UNICEF/UNI12390/Holmes
Introduction Changing context of salt
iodization and iodine
nutrition programmes
There has been remarkable progress towards The concept of universal salt iodization
eliminating iodine deficiency disorders (IDD) over entails the iodization of all food-grade
the past two decades. Since 1990, the number of salt (i.e. salt used in both households and
countries classified with iodine deficiency has declined during food processing) (4). However,
from 113 to 20 (1). This progress is due, primarily, programme efforts in many countries
to the scale up of salt iodization programmes. have been limited to ensuring that only
Current methods and practices have supported this household salt is adequately iodized.
remarkable progress. However, important lessons Given that the consumption of salt
have emerged in recent years on how to better track through processed foods1 is increasing in
and refine salt iodization programmes. many settings, the salt contained in such
foods is an important potential source
This document presents such lessons, as identified of dietary iodine and should therefore
during a Technical Consultation on the Monitoring be monitored by programme managers
of Salt Iodization Programmes held at UNICEF (5–7). At the same time, programme
Headquarters in December 2015 (2). The purpose of managers should consider the growing
this document is to guide programme managers in importance of reducing salt intake to
avoiding common mistakes made in the interpretation prevent non-communicable diseases. This
of data and implementation of national IDD control changing context highlights the need for
programmes. Some of the lessons discussed in this alignment between the implementation
document reinforce key recommendations made in and monitoring of salt iodization strategies
the 2007 WHO/UNICEF/ICCIDD Guide for Programme and salt reduction strategies (4). Salt
Managers: Assessment of iodine deficiency disorders iodization remains the main strategy for
and monitoring their elimination (3rd Edition), which achieving sustained IDD control, and global
remains a valuable resource for programme managers experience has demonstrated that the
(3). In addition, the current document presents new iodization of food grade salt is the most
information and updates not contained in the 2007 equitable, effective and sustainable strategy
WHO/UNICEF/ICCIDD Guide; this information may be to ensure optimal iodine nutrition for all
considered in future versions of the Guide. population groups.
The intended users of this document are managers
1 In this document, the term ‘processed foods’ refers to
of national IDD control programmes. It is hoped large-scale, commercially produced and manufactured
that the information presented in this document will foods, including bread, instant noodles, bouillon and other
salty condiments.
enable those managers to improve the effectiveness
of the programmes they support.
2 3
©UNICEF/UNI189137/Quarmyne
Summary of key
recommendations
This document highlights the following key recommendations:
1. As resources allow, the adequacy of iodine intakes should
be examined among different subsets of the population,
especially among groups vulnerable to deficiency. National-
level median urinary iodine concentrations (mUIC) may hide
discrepancies in iodine intake among different sub-groups, such
as those defined by geographic region or residence, socio-
economic status, or programmatically relevant criteria (e.g.,
by sources of salt, packaged/unpackaged salt). Such stratified
analyses may help identify remaining challenges and inform
adjustments to salt iodization programmes.
2. Rapid test kits (RTKs) should only be used to differentiate
between non-iodized and iodized salt. RTKs can accurately
distinguish between iodized and non-iodized salt. However, the
ability of RTKs to measure the iodine content in quantitative
terms and to distinguish between iodine content in salt below
and above certain cutoff levels is questionable (even when the
RTK packaging suggests otherwise) (8–10). Given this limitation,
RTKs should only be used to measure the percentage of salt that
contains any iodine at all. More precise methods, such as titration
or other validated quantitative assessment tools are required to
measure the percentage of salt that is inadequately iodized or
adequately iodized (11).
3. The acceptable range of ‘adequate’ iodine intake among
school-age children can be widened from 100–199 µg/L to
100–299 µg/L. According to the 2007 WHO/UNICEF/ICCIDD
Guide for Programme Managers (3), a mUIC in the range 100–
199 µg/L indicates ‘adequate’ iodine intake and the range of
200–299 µg/L indicates ‘more than adequate’ iodine intake
4 5
among school-age children. The presence of a 4. With currently available methods, the mUIC
mUIC in the ‘more than adequate’ range has can only be used to define population iodine
raised concerns about the potentially adverse status and not to quantify the proportion Use of data to evaluate programme effectiveness
effects of high iodine intake on normal thyroid of the population with iodine deficiency or
function. However, a 2013 study assessing iodine excess. As an example, a mUIC of 122 National surveys provide important types of salt produced and processed
thyroid function and iodine status found that μg/L obtained from a survey among school- data on key indicators of salt iodization for different markets. This data serves to
the mUIC range of 100–299 µg/L was not age children identifies a population that has and iodine status. However, data from complement the information on brands,
associated with any thyroid dysfunction (12). no iodine deficiency. While a proportion of national surveys should be interpreted packaging and types of salt collected
As a result, the acceptable range of ‘adequate’ children in that survey would have UIC values in conjunction with complementary data through the survey and can help explain
iodine intake among school-age children can of < 100 μg/L, it would be incorrect to label that: (i) provides qualitative information survey results. For example, household
be widened to 100–299 µg/L. There is no data that percentage of children as ‘deficient’. on the programme; (ii) facilitates the coverage of iodized salt is often lower in
to indicate, however, that this widened range Likewise, those children in the population with interpretation of survey data; and (iii) areas of domestic salt farming, especially
can be applied to other groups such as women UIC scores of ≥300 µg/L cannot be labeled allows for triangulation or verification among poorer households, because these
of reproductive age. The interpretation of a as the proportion of children with ‘excessive’ of survey data. In addition, such families are more likely to access salt
mUIC of ≥ 300 µg/L as ‘excessive iodine intake’ iodine intakes. However, as recommended complementary data should be used in the directly from the point of production, prior
remains unchanged. in the 2007 WHO/UNICEF/ICCIDD Guide for design of the survey. Together, survey and to any iodization or packaging processes.
Programme Managers, not more than 20% of complementary data can identify the need In addition, small scale producers often
samples should be < 50 μg/L (3). for strategic changes and help address produce cheaper, lower-quality iodized (or
programmatic weaknesses. non-iodized) salt.
5. National salt iodization programmes should
As applicable for their contexts, • Processed foods: Data is needed
monitor the use of iodized salt in processed
programme managers may consider to identify which processed food
foods. Household- and school-based surveys
collecting complementary data from the manufacturers use iodized salt, and the
measuring iodine content in household salt
following areas: extent to which these manufacturers
have been an important monitoring tool for
verify the iodine content of the salt used
assessing the performance of salt iodization • Salt industry: This analysis requires
in the production of their foods.
programmes. While iodine in the diet was data from the following areas: (i) the
previously assumed to come predominantly percentage of salt (iodized and non- • Regulatory monitoring: Regulatory
from household iodized salt, recent evidence iodized) that is imported versus monitoring data from import, production
suggests that an increasing amount of domestically produced; (ii) the percentage and market levels are an important
iodized salt is consumed through processed of salt processed by large, medium and source of information for programme
foods (5–7, 13) in different settings. If the small enterprises; (iii) the percentage of managers. If there is a requirement to
salt contained in such foods is well iodized, food grade salt used for food processing; use iodized salt in the manufacturing
it can be an important source of iodine and (iv) the locations and brand names of processed foods, a system should
may help explain iodine sufficiency in settings of domestic salt farming/production be in place to assess the extent of that
where household iodized salt coverage is low and processing enterprises (including compliance.
(14). Programme managers should therefore iodization and packaging/re-packing):
evaluate whether major processed foods are (v) salt distribution chains; and (vi) the
manufactured with iodized salt. In selected
cases, the iodine contained in water may also
©UNICEF/UNI189136/Quarmyne
need to be assessed.
6 7
©UNICEF/UNI189140/Quarmyne
Recommendations
Design of iodine nutrition surveys
The iodization of salt used in households and food processing is the
most effective and sustainable strategy for IDD control (4). The impact of
salt iodization programmes is best assessed through the measurement
of urinary iodine concentrations (UIC) in populations. According to global
recommendations, household-level data on salt iodine content and
population-based UIC data should be collected every five years (3). If
changes in iodine status are expected, such as due to changes in the
national salt iodization programme, a survey may be warranted even
before the five-year mark has passed. Household-level surveys may also
attempt to estimate the frequency of consumption of the most common
processed foods and condiments containing salt. If resources allow and
as dictated by local conditions, it may be programmatically useful to
design surveys such that geographic areas with suspected low iodized
salt coverage (such as those that are home to small-scale salt producers)
can be examined in separate strata. If feasible, surveys may separately
examine the iodine status of pregnant women, as there is evidence that
their iodine intakes may be insufficient, even in settings where iodine
intake is adequate among the general population (4). Table 1 presents
recommendations for addressing general issues encountered in the
design of iodine nutrition surveys.
8 9
Table 1. Recommendations for addressing common issues encountered in the design of Assessment of household coverage of iodized salt and
iodine nutrition surveys
measurement of salt iodine content
Problem Recommendation
The 2007 WHO/UNICEF/ICCIDD Guide for Programme Managers remains a valuable resource (3) for
Surveys designed to provide nationally • Examine household iodized salt coverage guiding the design of household-based surveys on iodized salt coverage and interpreting survey results.
representative estimates are not used to and/or population iodine status in subnational Table 2 emphasizes relevant points from that Guide and presents additional considerations to improve
detect areas of low household iodized salt strata or in other relevant groups, such as the assessment of household coverage of iodized salt and measurement of salt iodine content.
coverage and/or population groups with those defined by residence, socio-economic
non-optimal iodine status. The exclusive use status, or programmatically relevant criteria Table 2. Recommendations on the assessment of household coverage of iodized salt
of national-level data may hide discrepancies (e.g., by use of salt types). and measurement of salt iodine content
among different sub-groups, such as those
• Design the survey to provide representative
defined by geographic region or other Problem Recommendation
and precise estimates for desired strata and
criteria, and therefore fail to inform important
to allow for informative sub-group analyses.
programme adjustments. Rapid test kits (RTKs) are erroneously used • Do not use RTK as semi-quantitative tools
to assess whether salt is adequately iodized. given the limited ability of RTKs to measure
Data on household iodized salt coverage and • Seek opportunities to collect data on house- Several evaluations have shown that RTKs can the iodine content in quantitative terms and
iodine status are often not available due to a hold iodized salt coverage and iodine status in accurately distinguish between iodized and to distinguish between iodine content in salt
lack of funds to undertake dedicated iodine the context of other household surveys. non-iodized salt. However, the ability of RTKs below and above certain cutoff levels,
surveys. National stand-alone surveys may to measure the iodine content in quantitative
• Continue to consider stand-alone iodine • Use RTKs only to present the percentage of
be expensive and available resources may be terms and to distinguish between iodine content
surveys if opportunities to link to other surveys non-iodized versus iodized salt. To estimate
insufficient to support such surveys. in salt below and above certain cutoff levels is
are limited and if sufficient resources are the percentage of inadequately iodized,
available. questionable (even when the RTK packaging
adequately iodized, or excessively iodized
suggests otherwise) (8–10).
salt, titration or other validated quantitative
School-based surveys have specific design • Continue to use school-based surveys to track
assessment tools are required (11).
limitations. School-based surveys offer population iodine status in settings where
a valuable source of data on iodine status school-based surveys are the only feasible Surveys do not use an appropriate • Determine stratification requirements to
given the vulnerability of school-age children to data source. If resources allow, consider sample size to assess household iodized assess the sub-national effectiveness of the
deficiency and the easy access to schools for conducting household-based surveys as a salt coverage among sub-populations in programme and prioritize strategic approaches.
population-based surveys. However, such surveys means of addressing the design limitations stratified analyses. Sample sizes may be too
• Calculate necessary sample size for
also have limitations, including: i) the inability of school-based surveys. Household-based small or larger than necessary for accurate
household iodized salt coverage per stratum,
to reflect potential differences in iodine status surveys may enable better data collection on representation of the situation.
which will be based on the expected
between school-age children and other vulnerable the coverage of household iodized salt and on
coverage, desired precision and expected
groups, such as pregnant women; ii) the fact the iodine status of population groups such as
design effect. Refer to established reference
that school-based surveys may not allow for the pregnant or non-pregnant women. They may
documents for more information (3, 15).
collection of data on socio-economic status and also allow for the collection of data required to
other relevant population characteristics; and conduct sub-group analyses and to examine
iii) the fact that school-based surveys may not other programmatically relevant factors.
provide a reliable reflection of the iodine status of
the general population, particularly in countries or
areas where school enrolment rates are low, or
where school-feeding programmes (using iodized
salt) operate on a large scale.
10 11
Problem Recommendation Problem Recommendation
Household surveys do not collect sufficient • Collect relevant information from each Households without salt at the time of • Consider excluding households without
data on the characteristics of household salt, household (if feasible) about the salt used data collection are treated differently in salt at the time of the survey from the
such as salt type, packaging, and grain type. and where the salt was purchased. Such the calculation of household iodized salt denominator in calculations to determine
Information on these parameters may help in information may include: type of salt coverage in different population-based household iodized salt coverage, as the most
the interpretation of salt iodine content. packaging; brand name; and source of surveys. As a result, the denominators useful programmatic coverage indicator is the
purchase (e.g., salt processor/farmer, wet and therefore the coverage estimates vary percentage of households using iodized salt
market, village retail shop or supermarket). across such surveys, thus complicating the among households with salt at the time of the
interpretation of household iodized salt coverage survey. However, the number of households
• Categorize the salt as processed (fine) versus
trends over time. without salt at the time of data collection
raw (coarse) or powder versus crystal vs rock.
should be noted in the survey results along
Categorization is best done by laboratory staff;
with a record of missing data (households
if this is not possible, trained field-level data
where salt was collected but not analyzed;
collectors may undertake this classification.
e.g., because there was an insufficient
Iodine in coarse salt may not be distributed • Mix the salt in the container or packet before amount, or it was lost during transfer to the
homogenously and small samples (≤10g) taking a sample, using a clean spoon. Use laboratory). Such households should be asked
may not yield accurate results on salt iodine sample weights of 50 grams if salt is coarse whether they have purchased salt in the
content. Variation in salt iodization practices, and if survey settings allow for the collection of last seven days. Results should be used to
suboptimal salt mixing, large crystal size, and such quantities (9). calculate the percentage of households not
high moisture content of the salt may lower the using iodized salt, as those households remain
homogeneity of iodine in salt samples. susceptible to iodine deficiency.
In surveys using titration or other validated • Interpret salt with < 5 ppm iodine as ‘salt Surveys do not consider that more than one • Include questions in the household
quantitative assessment tools, salt with without iodine’, and salt with ≥ 5 ppm iodine type of salt may be used in a household. questionnaire on whether more than one
iodine content of > 0mg/kg iodine is as ‘iodized salt’ (9). type of salt is used, what different types of
labeled as ‘iodized’. Such a definition likely salt are used, and what the different types
overestimates the percentage of iodized salt of salt are used for. The salt tested for iodine
given the variation in iodine measurements at content should be the salt used to prepare the
low iodine contents. previous evening’s meal. If no salt was used
to prepare last night’s meal, the surveyor may
The current classifications of salt into the • Provide the average salt iodine content (mg/ ask for a sample of the most commonly used
categories of non-iodized, inadequately kg) and an indication of variation (e.g., 95% cooking salt in the household. Responses to
iodized, adequately iodized, and excessively confidence interval (CI)) to better estimate the the additional questions about other types of
iodized do not allow for an estimation of the additional iodine supplied through salt. Salt salt should be taken into consideration when
contribution of iodized salt to dietary iodine samples without iodine should be excluded interpreting data on household coverage of
intakes. This is an issue, given that the goal of from this calculation. See Technical Annex for iodized salt and when looking at associations
salt iodization programmes is to address gaps in more information. between household coverage of iodized salt
dietary intake of iodine. and iodine status. In cases where considerable
proportions of other types of salt are used,
it may be necessary to collect samples and
information on more than one type of salt used
in the household.
12 13Assessment of iodine status
in population-based surveys
Historically, the mUIC has frequently been
assessed through school-based surveys to
estimate the iodine status of the general
population. However, the mUIC among school-
age children may not reflect the iodine status
among pregnant women, whose iodine
Interpretation of household iodized salt coverage requirements are greater (3). Household-based
against UIC surveys have been used to assess the iodine
status of other demographic groups, such as
The dramatic reduction in the number of iodized salt and adequate iodine status non-pregnant women of reproductive age.
iodine deficient countries over the last 25 among the general population remain This is important because the iodine status
years was brought about by the scale up strong, there are instances where of women of reproductive age is also the
of salt iodization programmes worldwide population iodine status is adequate status of women entering pregnancy, when
(1,4). To this day, the iodization of all food- despite suboptimal household iodized salt adequate maternal iodine status is vital for
grade salt used in households and food coverage. In those settings, programme fetal development. However, the iodine status
processing continues to be recognized as managers need to determine the feasibility, of non-pregnant women may not be a good
the most effective and sustainable strategy cost-effectiveness, risks and added value indication of the iodine status among pregnant
to prevent and control iodine deficiency of further increasing the use of adequately women. A review of data sets with survey
disorders in populations (4). Ensuring iodized salt within households. To illustrate, data on both non-pregnant and pregnant
universal access to adequately iodized salt in settings with a fragmented salt industry, women indicates that when the mUIC among
should therefore remain an important goal characterized by the presence of many non-pregnant women was adequate or above
of nutrition programmes, and the 2007 small-scale producers, it may not be requirements, approximately half of the studies
WHO/UNICEF/ICCIDD Guide for Programme programmatically feasible or cost-effective indicated inadequate iodine intake in pregnant
Managers recommends that > 90% of to expect sustainable increases in the women (16). As an additional limitation, there
households should be using adequately production of adequately iodized salt. In is a lack of consensus on the optimal mUIC
iodized salt (3).2 such settings, a more appropriate strategy range for non-pregnant women of reproductive
may be to consolidate gains made while age. The 2007 WHO/UNICEF/ICCIDD Guide for
However, the iodization of all food-grade ensuring adequate iodine status for all Programme Managers (3) proposes a range of
salt is not the ultimate goal of IDD control population groups. Specific subgroup 100–199 μg/L; however, the scientific basis for
programmes. Rather, the goal of IDD analyses comparing mUIC against this recommendation is weak (17). Research is
programmes is to sustainably achieve salt iodine content may also provide currently ongoing to better define the optimal
optimal iodine status among all population valuable additional insights on whether mUIC range for non-pregnant women of
groups. While in many settings, the links programmatic adjustments are needed. See reproductive age.
between high household coverage of Technical Annex for more information.
Programme managers should also note that it
2 The Guide defines adequately iodized salt as salt containing
between 15 and 40 ppm iodine at household levels. remains unclear how to best conduct sample
14 15
©UNICEF/UNI189140/Quarmynesize calculations for such surveys estimating methods using spot UIC measurements do not Drawing on the latest available information, Table 3 presents recommendations on the assessment of
population iodine status by measuring spot allow for the identification of the proportion of iodine status in population-based surveys.
UIC. The 2007 WHO/UNICEF/ICCIDD Guide for the population with iodine deficiency (or with
Table 3. Recommendations on the assessment of iodine status in population-based surveys
Programme Managers (3) presents considerations iodine excess) (Table 3; see Technical Annex for
on sample size calculations for surveys attempting more information). Given the uncertainty on how
Problem Recommendations
to estimate the proportion of households using to best construct statistical power calculations
iodized salt, while stating that ‘further sample size for surveys determining population iodine status According to the 2007 WHO/UNICEF/ICCIDD • Based on the latest scientific evidence (12),
calculations are needed if additional information using spot UIC measurements, programme Guide for Programme Managers, a mUIC in widen the acceptable range of ‘adequate’
is collected, such as urinary iodine […]’. However, managers may choose to take a conservative the range 100–199 µg/L indicates ‘adequate’ iodine intake among school-age children
the Guide does not provide any such additional approach and define the required survey sample intake and 200–299 µg/L indicates ‘more than from 100–199 µg/L to 100–299 µg/L. Note,
information. A UNICEF/Programme Against sizes with methods that may lead to sample sizes adequate’ intake among school-age children. however, that the interpretation of mUIC ≥
Micronutrient Malnutrition (PAMM) guide that may be higher than required. This would mUICs in the ‘more than adequate’ range have 300 µg/L as ‘excessive iodine intake’ among
published in 2000 on ‘Urinary Iodine Assessment: involve starting their deliberations on required raised concerns about potentially adverse effects school-age children remains unchanged. Also
A Manual on Survey and Laboratory Methods’ sample sizes by following the longstanding of high iodine intakes on normal thyroid function. note that this widened range must not be
provides detailed and valuable information for recommendation of conducting a 30-cluster However, a 2013 study assessing thyroid function applied to women of reproductive age. See
and iodine status found that the mUIC range of Technical Annex for more information.
programme managers involved in the planning survey with 30 urine specimens per cluster if
100–299 µg/L was not associated with any thyroid
and conduct of surveys determining population only a nationally representative survey estimate
dysfunction (12).
iodine status (18). Similar to other previous (without subnational stratification) is required.3 For
expert guidance (15), the Manual presents subnational estimates, managers should consider Goiter is not a sensitive indicator of the • Stop assessing goiter as part of routine
power calculations using the proportion of the using 30 clusters with 20 urine specimens per impact of salt iodization on the population, surveys on iodine status. If goiter is
population with iodine deficiency as a key input. cluster for each subnational estimate as a starting yet continues to be widely used. Goiter was assessed, provide clear justification,
This is a severe limitation, as currently available point,4 as recommended in the aforementioned measured in the past when the condition was still including how the data will be interpreted
UNICEF/PAMM guide. Managers may furthermore widespread before iodized salt programs were in compared to UIC data, which is the best
choose to slightly increase the sample size per place. However, thyroid size and goiter prevalence marker of dietary iodine intake.
cluster to account for potential non-response. The are not responsive to recent changes in iodine
intake. There is also significant subjectivity in
sample size needs for each subnational estimate
the measurement of small goiters, even when
should then be totalled to obtain the final survey
ultrasound is used (21).
sample size. Where resources are limited, and/
or if stratification will be programmatically useful, National-level mUIC in the adequate range • Examine the mUIC in relevant sub-
it should be noted that smaller sample sizes can is incorrectly interpreted as an indication of populations if survey design and sample size
still provide programmatically useful information, effective control of iodine status in all parts allow.5 Consider the following stratification
however. Research indicates that around 400 of a given country. However, national-level variables: residence (urban/rural),
urine samples per population group are required estimates may mask subnational disparities in geographical region, socio-economic status,
to measure the mUIC with 5% precision and 100 iodine status. or level of salt iodization. Local conditions
urine samples to measure the mUIC with 10% may require stratification by other variables.
precision (19, 20).
3 In large countries, more than 30 clusters may be required.
4 Based on the assumption of 50 per cent prevalence of iodine
©UNICEF/UNI189141/Quarmyne deficiency, 95% confidence level, a design effect of 1.5 and a 5 Relevant sub-populations should be identified at the time of planning for and designing the survey and adequate sample sizes for each
precision value of ±5 per cent relevant sub-population calculated.
16 17Problem Recommendations Problem Recommendations Surveys measuring UIC are inappropriately • Do not interpret the proportion of the The mUIC is often presented by itself without • Calculate the 95% CI using ‘bootstrapping’ or used to determine the proportion of the population with UIC
©UNICEF/UNI189147/Quarmyne
Technical Annex
Analysis and presentation of
household iodized salt coverage
data from surveys
The coverage of iodized salt at the household level is one
of the most important indicators of the performance of salt
iodization programmes. A suggested table shell is provided
below for the presentation of survey data using quantitative
tests (Table A1). These table shells should be further adapted
to allow for the best representation of local survey data.
If only RTK data is available, then the columns should be
modified to indicate the percentage of households with ‘no
iodine (RTK negative)’ and ‘any iodine (RTK positive)’.
20 21Table A1. Household iodized salt coverage by relevant strata: results of quantitative salt
iodine testing1
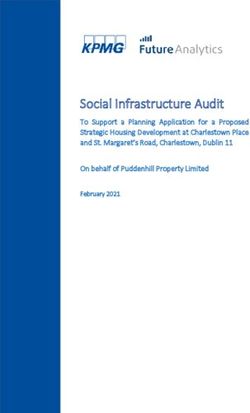
Total no of Among all households, Among households with tested salt, the percentage with 2 Analysis and presentation of the population and the proportion of UIC values <
households the percentage with 50 μg/L. It should be noted that currently there are
in survey Salt No salt No iodine Inadequate Adequate Excess Median data on iodine status no suitable measures to define the proportion of
tested in the (< 5 iodine Iodine iodine iodine
iodine deficiency in the population, but efforts are
household mg/kg) (5–14.9 (15–40 (> 40 content The mUIC is a good indicator of population iodine
mg/kg) mg/kg) mg/kg) (mg/kg) 3 underway to develop such methodologies (23).
status. In school-age children, a mUIC of between
National
100 μg/L and 299 μg/L defines a population with Figure A1 provides an example of a common, but
no iodine deficiency. A common mistake is to incorrect, interpretation of UIC data. In this setting,
Residence
assume that all individuals with a spot UIC < 100 the mUIC value is 122 µg/L, which suggests
Urban
μg/L are iodine deficient. Since dietary iodine optimal iodine status. However, the presentation
Rural
intake and therefore UIC are highly variable implies that 40% of individuals in the population
from day to day, even among individuals whose have inadequate iodine intakes, which is not
Region
average iodine intake is sufficient to maintain correct. Likewise, it is incorrect to state that 10%
Region 1
normal thyroid function, there will be individual of the population has excessive iodine intakes.
Region 2
days when UIC is < 100 μg/L. As a result, in
Region 3
populations whose average dietary iodine intake In addition to the overall mUIC of the population,
is sufficient, there will always be values < 100 stakeholders may choose to conduct stratified
Socioeconomic
status μg/L; however, these values do not describe the analyses to identify potential variations in iodine
Quintile 1 prevalence of iodine deficiency in the population. status across subgroups. This cross-tabulation by
Quintile 2 The only available guidance with regard to low different sub-groups helps to identify where there
Quintile 3 UIC values is that not more than 20% of samples are disparities and where programme efforts may
Quintile 4 should be < 50 μg/L. In summary, the two key need to be focused and resources targeted (see
Quintile 5 survey statistics to report are the mUIC value of Table A2 and Figure A2).
Salt type4 Figure A1. Inappropriate interpretation of UIC data as a measure of population
Processed (fine) iodine status
Raw (coarse)
60
Packaging
Sealed branded
Proportion of population (%)
50
package
Sealed
40
unbranded
package
30
No package/
loose
20
10
1 Strata (e.g. urban/rural; quintiles; salt type) are illustrative and should be modified and adapted as required and as programmatically relevant.
2 While it is recommended that the definition of ‘no iodine’ be maintained in different settings, the definitions of inadequate, adequate, and excess 0
iodine should be modified based on national standards. 5mg/kg of iodine.
Urinary Iodine Concentration (μg/L)
4 Categories of salt type and packaging should be set based on an understanding of how the salt industry operates in a given country.
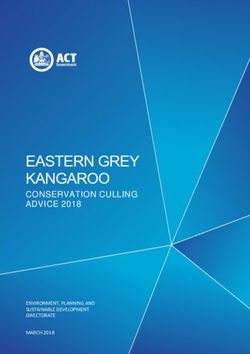
22 23Table A2. Suggested sub-group analysis for household-based surveys on population Figure A2. Sample figure to display the association between household salt iodine
iodine status5 content and iodine status (measured as median UIC) among school-age children7
Variable Purpose 350
By household iodine To clarify whether there is an association between iodine status and
content6: the level of iodine in household salt. 300
• Non-iodized (40mg/kg). information about the consumption of salt in processed foods and the
use of iodized salt in those foods in future monitoring.
100
By residence or To examine the association between iodine status and residence/
geographic locations: location in order to identify geographic locations with poor iodine 50
• Urban vs. rural status.
• Regions or provinces 0
Non-iodized Inadequately Adequately Over-iodized
By socio economic To examine a potential link between iodine status and socio- (40mg/kg)
status: (5-14.9mg/kg) (15-40mg/kg)
economic status.
• Richest quintile Poorer populations may have lower iodine status because they are
• Fourth quintile likely to have access to salt with lower or no iodine content and/or
may be more dependent on household salt as the major dietary salt
• Middle quintile
source (as opposed to processed foods). Such a finding should lead
• Second quintile to further investigation of dietary salt sources and factors inhibiting
• Lowest quintile their adequate iodization.
By other programmatically To consider additional variables that may explain differences in iodine
relevant criteria such as in status and may help in targeting programme efforts and resources.
salt producing versus non-
salt producing areas
5 To test whether mUIC vary across subgroup, non-parametric tests should be employed. See Figure 2 for a suggested presentation of mUIC
with 95% CIs from subgroup analyses. 7 A mUIC between 100 and 200 µg/L indicates adequate iodine status. mUICs are presented with 95% CIs. While it is recommended that the
6 While it is recommended that the definition of ‘no iodine’ be maintained in different settings, the definitions of inadequate, adequate, and definition of ‘no iodine’ be maintained in different settings, the definitions of inadequate, adequate, and excess iodine should be modified
excess iodine should be modified based on national standards. based on national standards.
24 25References
effects on thyroid function in the UIC range 19. Dold S, Zimmermann MB, Jukic T, Kusic Z, Jia
of 100–299 mug/L: a UNICEF/ICCIDD study Q, Sang Z, Quirino A, San Luis TOL, Fingerhut
group report. J Clin Endocrinol Metab R, Kupka R, Timmer A, Garrett GS, Andersson
2013;98(3):1271–80. M. Universal Salt Iodization Provides Sufficient
Dietary Iodine to Achieve Adequate Iodine
13. Knowles J, Van der Haar F, Shehata M,
Nutrition during the First 1000 Days: A
Gerasimov G, Bimo B, Cavenagh B, Maramag
Cross-Sectional Multicenter Study. J Nutr
CC, Otico E, Izwardy D, Spohrer R, Garrett GS.
1. Iodine Global Network. Global Scorecard of used as ingredients in the food industry and 2018;148(4):587-98.
Iodine Intake through processed food: Case
Iodine Nutrition 2017. Zuerich: IGN; 2017. implications for large-scale food fortification
studies from Egypt, Indonesia, the Philippines, 20. Karmisholt J, Laurberg P, Andersen S.
programs in Southeast Asia. Food Nutr Bull
2. UNICEF. Meeting Report. Technical Working the Russian Federation and Ukraine, 2010– Recommended number of participants in
2013;34(2 Suppl):S50–61.
Group Meeting on Research Priorities for the 2015. Nutrients 2017;9(8):797. iodine nutrition studies is similar before and
Monitoring of Salt Iodization Programs and 8. Gorstein J, van der Haar F, Codling K, Houston after an iodine fortification programme. Eur J
14. Abizari AR, Dold S, Kupka R, Zimmermann
Determination of Population Iodine Status 17–18 R, Knowles J, Timmer A. Performance Nutr 2014;53(2):487-92.
MB. More than two-thirds of dietary iodine in
December 2015. New York: UNICEF; 2016. of rapid test kits to assess household
children in northern Ghana is obtained from 21. Gorstein J. Goiter assessment: help or
coverage of iodized salt. Public Health Nutr
3. World Health Organization. Assessment of bouillon cubes containing iodized salt. Public hindrance in tracking progress in iodine
2016;19(15):2712–24.
iodine deficiency disorders and monitoring Health Nutr 2017;20(6):1107–1113. deficiency disorders control program? Thyroid
their elimination : a guide for programme 9. Jooste PL, Strydom E. Methods for 2001;11(12):1201–2.
15. Gorstein J SK, Parvanta I, Begin F. Indicators
managers. Geneva: WHO; 2007. determination of iodine in urine and salt. Best
and Methods for Cross-Sectional Surveys of 22. Cogswell ME, Wang CY, Chen TC, Pfeiffer
practice & research. Clinical Endocrinology &
4. World Health Organization. Guideline: Vitamin and Mineral Status of Populations. CM, Elliott P, Gillespie CD, Carriquiry AL,
Metabolism 2010;24(1):77–88.
fortification of food-grade salt with iodine for Ottawa: The Micronutrient Initiative and Sempos CT, Liu K, Perrine CG, Swanson CA,
the prevention and control of iodine deficiency 10. Pandav CS, Arora NK, Krishnan A, Sankar R, Atlanta: The Centers for Disease Control and Caldwell KL, Loria CM. Validity of predictive
disorders. Geneva: World Health Organization; Pandav S, Karmarkar MG. Validation of spot- Prevention; 2007. equations for 24-h urinary sodium excretion
2014. testing kits to determine iodine content in salt. in adults aged 18–39 y. Am J Clin Nutr
16. Wong EM, Sullivan KM, Perrine CG, Rogers
Bull World Health Organ 2000;78(8):975–80. 2013;98(6):1502–13.
5. Brown IJ, Tzoulaki I, Candeias V, Elliott LM, Pena-Rosas JP. Comparison of median
P. (2009) Salt intakes around the world: 11. Rohner F, Kangambega MO, Khan N, urinary iodine concentration as an indicator of 23. Zimmermann MB, Hussein I, Al Ghannami
implications for public health. Int. J. Epidemiol. Kargougou R, Garnier D, Sanou I, Ouaro BD, iodine status among pregnant women, school- S, El Badawi S, Al Hamad NM, Abbas Hajj
38, 791–813. Petry N, Wirth JP, Jooste P. Comparative age children, and nonpregnant women. Food B, Al-Thani M, Al-Thani AA, Winichagoon P,
validation of five quantitative rapid test kits for and nutrition bulletin 2011;32(3):206–12. Pongcharoen T, van der Haar F, Qing-Zhen
6. Spohrer R, Garrett GS, Timmer A, Sankar R,
the analysis of salt iodine content: Laboratory J, Dold S, Andersson M, Carriquiry AL.
Kar B, Rasool F, Locatelli-Rossi L. Processed 17. Zimmermann MB, Andersson M.
performance, user- and field-friendliness. PLoS Estimation of the Prevalence of Inadequate
foods as an integral part of universal salt Assessment of iodine nutrition in populations:
One 2015;10(9):e0138530. and Excessive Iodine Intakes in School-Age
iodization programs: a review of global past, present, and future. Nutr Rev
experience and analyses of Bangladesh 12. Zimmermann MB, Aeberli I, Andersson M, Children from the Adjusted Distribution of
2012;70(10):553–70.
and Pakistan. Food Nutr Bull 2012;33(4 Assey V, Yorg JA, Jooste P, Jukic T, Kartono Urinary Iodine Concentrations from Population
18. UNICEF, PAMM. Urinary Iodine Assessment: Surveys. J Nutr 2016;146(6):1204–11.
Suppl):S272–80. D, Kusic Z, Pretell E, San Louis TO Jr, Untoro
A Manual on Survey and Laboratory Methods.
J, Timmer A. Thyroglobulin is a sensitive
7. Spohrer R, Larson M, Maurin C, Laillou PAMM: Washington, DC; 2000.
measure of both deficient and excess iodine
A, Capanzana M, Garrett GS. The growing
intakes in children and indicates no adverse
importance of staple foods and condiments
26 27Photograph Credits:
On the back cover:
©UNICEF/UNI189136/Quarmyne
©UNICEF/UN021384/Tesfaye
©UNICEF/UNI119116/Noorani
©UNICEF/UNI12425/Holmes·I
··
••·
•·You can also read