GLOBAL HEALTH 2022 - ENT UK JOURNAL OF GLOBAL HEALTH
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

GLOBAL HEALTH
2022
E N T U K J O U R N A L O F G L O B A L H E A LT H
Scan the QR code
to learn more about
the VITOM® 3D at
our Virtual Booth
ENT 106 2.1 05/2021/A-E
VITOM® 3D –
The 3rgonomic Dimension
3D visualization for Otorhinolaryngology
KARL STORZ SE & Co. KG, Dr.-Karl-Storz-Straße 34, 78532 Tuttlingen/Germany
KARL STORZ Endoscopy (UK) Limited, 415 Perth Avenue, Slough, Berkshire SL1 4TQ/United Kingdom
www.karlstorz.com
GLOBAL HEALTH
2022
E N T U K J O U R N A L O F G L O B A L H E A LT H
Published in 2022 for ENT UK Global Health
Compiled by: Vijay Pothula
For information please contact:
Vijay Pothula vijaybabu@aol.com 01942 773546
Designed and Printed by: www.beamreachuk.co.uk

contents
ENT UK Journal of Global Health
Foreword (Prof. Nirmal Kumar) 7
Profiles (ENT UK Global Health Committee) 9
Global hearing health: progressing the goal of hearing care for all 17
ENT training and services in a tertiary care hospital of Northern
Province, Sri Lanka 21
Cost-effective innovations in airway surgery amidst the finite resources
in Nepal: An endeavor on balancing the economic constraints with the
surgical care 25
Making a difference, practical involvement in ENT Global Health 30
Deafness Screening & Cochlear Implantation in the Indian
Subcontinent - “The Hub & Spoke Model of Tamil Nadu” 38
The role of Social Media in Global Health 43
Hearing care by community health workers using
digital technologies 48
ENT UK GLOBAL HEALTH 2022 5
foreword
“No person is safe until all – everyone, everywhere – are safe, and
no country is safe until all countries are safe”
Amina Mohammed, Deputy Secretary General, UN
This quote relates to the pandemic and chairmanship of the group and with the
the roll out of vaccines, but I think this help of the able committee members
applies to all that the Global Health take the important work forwards. As
Committee is doing and “by working President of ENT UK, I am pleased that
together we can build a better world our international collaborations and
where everyone thrives in dignity and friendships are cemented by doing this
equality on a healthy planet”. work together and we can all learn from
each other in providing high quality
I wish to thank Vijay Pothula who has led care.
the global health group in all their worthy
endeavours following on the work of
Robin Youngs. I am delighted to see that
Nick Eynon-Lewis will be taking on the
Professor B Nirmal Kumar,
President, ENT UK
ENT UK GLOBAL HEALTH 2022 7
profiles ENT UK Global Health Committee Vijay Pothula – Chairman I was appointed as a consultant ENT and Head and Neck Surgeon in 2001 and work at WWL and Manchester Foundation Trust sites. I have a keen interest in humanitarian work and have conceived, designed and started the Shravana project in Hyderabad, India in 2006. I have assumed the chairmanship of ENTUK Global Health in 2018. It is our endeavour, in collaboration with British Society of Audiolgy, British Charities, Professionals and Industry, would like to help countries where people have no recourse to any help when affected with deafness or any ENT disorders. We intend to help create services and train their ENT, audiology professionals and make them self-sufficient. Nicholas Eynon-Lewis – Vice Chairman Nick is a Consultant ENT surgeon at Bart's Healthcare NHS Trust. He has had a longstanding interest in overseas medicine. He spent a year in Cape Town on a TWJ fellowship and has been involved in various ENT projects in Africa. He is the lead for undergraduate education at Bart's and organises and lectures on various postgraduate courses. He is the Vice Chair of the Global Health Committee ENT UK GLOBAL HEALTH 2022 9

profiles
Mr Matthew Clark Consultant Otologist,
Gloucestershire Royal Hospital and Education
& Training lead for ENT UKs Global Health
Committee
Matthew was a trainee in Oxford before undertaking
a fellowship in Otology & Neurotology in Vancouver,
Canada. He was appointed as an Otologist in
Gloucester in 2009 where he is a lead in training
and education. This role now extends to ENT UKs
Global Health Committee. He has worked in Nepal
and Uganda on ear camps and courses, whilst also
helping to establish and mentor a post-CCT fellowship
programme in Cambodia. Research includes the development of an ear surgery
simulator designed for low-resource settings and he is currently co-authoring a
guide on delivering and developing Otology in remote or resource-poor countries.
Mr. Sanjiv Kumar MS, DM, FRCSI, FRCS (Glasg),
FRCS(ORL-HNS)
I have been a consultant at University Hospital of
North Midlands NHS trust since 2012, where I
specialise in adult and paediatric otology and have
been active role in education and training. I am
interested in global health and equality of access
to medical care and training across the world. I
have been involved in humanitarian care doing ear
camps in Uganda. I have been active in setting up
and teaching primary care ENT to clinical officers
in Uganda. As a member of the ENT UK’s Global
committee, I am keen on co-ordinating and helping global charity work undertaken
by UK surgeons abroad.
Cheka Spencer
Cheka is a Consultant ENT Surgeon with a
special interest in Rhinology, Facial Plastics
and Paediatric ENT. He is the Clinical Lead for
ENT and Audiology at the Royal Free London
NHS Foundation Trust. He is the Global Health
editor for the international magazine ENT
and Audiology News. He is committed to
humanitarianism and has developed many links
around the world.
10 ENT UK GLOBAL HEALTH 2022Mr Misha Verkerk MA (Cantab.) FRCS (ORL-HNS)
Misha is a senior ENT Registrar in South London and since
2016 has been the UK Director of Global ENT Outreach,
a charity that aims to improve the lives of people with
hearing loss and ear disease through surgical training and
education. His main global health activities have been
focussed in Ukraine and Ethiopia. Since 2017, he has led
biannual Otology training camps to Mekelle, Ethiopia and
established the first temporal bone lab in the region to
train local ENT surgeons and prevent the so-called “brain
drain” of African-trained surgeons to the West.
Misha is a member of the WHO’s World Hearing Forum and the recipient of grants
and awards from the Royal College of Surgeons, Association of Surgeons in Training
and the British Medical Association to support his global health work. Misha was the
inaugural recipient of the Rising Star Award at the British Academic Conference in
Otolaryngology (BACO 2020) and in 2021 he was awarded the Gold Medal for top
performance in the FRCS (ORL-HNS) exam. He is proud to represent trainees on the
ENT-UK Global Health committee.
Emma Stapleton
Emma has been a Consultant Otolaryngologist at
Manchester Royal Infirmary since 2018. She is Clinical
Lead for the Manchester Cochlear Implant Programme
and Undergraduate Lead in ENT. Her other roles include
President Elect of the North of England Otolaryngology
Society, Editor of ENT UK Newsletter, and Associate
Editor of ENT and Audiology News magazine where she
introduced a responsible policy for coverage of Global
Health initiatives.
Emma has been a volunteer surgeon at the BRINOS
Hospital, Nepal, she is a Trustee of Helping Uganda Schools (HUGS) Charity and a
Trustee of the TWJ Foundation. She is married with two sons.
Baveena Heer
Baveena is currently a medical student at GKT School of
Medical Education, King’s College London, and an aspiring
ENT surgeon with an interest in Global Health. She leads a
multi-disciplinary research group at King’s College London
that is focused on developing sustainable technological
interventions for current ENT problems in low-resource
settings. She is a member of the Global OHNS Initiative,
where she works within the Racial Disparities and Gender
Disparities research groups. She is also the InciSioN UK
representative for King’s College London, where she works to promote safer access
to surgery for all through research, education and advocacy. She has previously
been a part of Global Brigades at King’s College London, during which she made
several brigades to Central America.
ENT UK GLOBAL HEALTH 2022 11profiles Ms Dulani Mendis, B.Sc. DO-HNS, MBA, FRCS
(ORL-HNS)
Dulani is a fellowship trained Otolaryngology
Consultant specialising in Laryngology, Rhinology
and Facial Plastics.
She has completed a Royal College interface
fellowship in Cosmetic and Reconstructive Surgery
and a Canadian fellowship in Benign Head and
Neck and Laryngology.
She has an interest in health policy, clinical leadership,
safety and governance having completed an MBA
at Keele University. She is currently completing a
Global Health Postgraduate certificate due to an
interest in Global Health and an inherent desire to tackle health inequality.
Dulani is also an ENT-UK Global Health committee member and treasurer.
Mahmood Bhutta DPhil FRCS (ORL-HNS)
Mr Mahmood Bhutta is academic lead in ENT Surgery
at Brighton & Sussex University Hospitals (UK) and
founder of the BMA Medical Fair and Ethical Trade
Group. He is a consultant ENT surgeon with diverse
interests, particularly relating to global inequity. He
was formally Phizackerley Senior scholar at Balliol
College Oxford where his DPhil was in genetic
susceptibility to otitis media. He works with national
and international partners on labour rights concerns
in healthcare supply chains. He also works on global
ear disease, and has delivered training to health
workers in Cambodia, Nepal and Uganda, and is a consultant to the WHO program
on prevention of deafness and hearing loss.
Mr Sanjay Verma MB, BCh, MA, FRCS(ORL-HNS),
PhD (Cantab)
Mr Sanjay Verma is an experienced Consultant ENT
surgeon at the Leeds Teaching Hospitals NHS Trust and
Nuffield Leeds Hospital, where he has a dedicated adult
and children’s ENT practise. He specialises in ear, nose
and sinus problems. Over the last decade he has been
instrumental in developing laser ear surgery, endoscopic
sinus surgery and coblation tonsillectomy techniques in
the region.
12 ENT UK GLOBAL HEALTH 2022Ms. Kate Stephenson FRCS ORL-HNS(Eng.),
FC ORL (SA), MMed Consultant Paediatric
Otorhinolaryngologist, Head and Neck
Surgeon Birmingham Children’s Hospital
Kate is a Paediatric Otorhinolaryngologist at Birmingham
Children’s Hospital. Her interests include paediatric head
and neck, airway and voice. She trained in both the UK
and South Africa and completed a fellowship at Great
Ormond Street Hospital.
Kate is the Networking Chairperson for the Young
Otolaryngologists of IFOS and has reviewed for a
number of ENT journals. She has also created Open Access educational materials
in collaboration with the University of Cape Town. Kate is currently developing a
global health section for the ENT UK e-lefENT website with Maha Khan.
Ms Maha Khan
Maha currently trains in Manchester. Her
clinical interests are neurotology and skull
base surgery, and translational and applied
research. She has raised funds for and
volunteered with ENT charities in both the UK
and abroad, and has an interest in the diagnosis
and management of paediatric hearing loss in
a Global Health setting. Maha is a member
of the ENT-INTEGRATE committee, and
President of the North West Trainee Research
Collaborative. She works to promote research and Global Health to students and
Foundation doctors through her work with the ENT-UK’s Student & Foundation
Doctors in Otolaryngology group. She lives in Cheshire with her husband and baby
boy, and when not working, is happiest outdoors.
Robin Youngs MD FRCS
Robin is an ENT Consultant Surgeon in Gloucestershire
who has an interest in the treatment of deafness. He has
been involved with deafness in developing countries for
25 years and is a Director of The Britain Nepal Otology
Service. In addition, he established the Mandalay School
for the Deaf Charity, which supports deaf children in
Myanmar. He has close connections with ENT surgeons
in Myanmar and Nepal, having organized numerous
educational activities.
He was the first Lead for Global Health for ENTUK and is a Past President of the
Otology Section of The Royal Society of Medicine. He is also Emeritus Editor of The
Journal of Laryngology and Otology, an international publication. His MD degree
from the University of London was awarded for research into chronic ear disease.
He has a Postgraduate Certificate in Global Health Policy from the London School
of Hygiene and Tropical Medicine.
ENT UK GLOBAL HEALTH 2022 13To advertise in
GLOBAL HEALTH
please contact:
Vijay Pothula vijaya.pothula@nhs.net 01942 773546
CON ADVANCE GAVISCON ADVANCE
ROVIDES PROVIDES GAV
EFFECTIVE RELIEF EFFECTIVE RELIEF FO
R PATIENTS WITH FOR PATIENTS WITH
R SYMPTOMS1 LPR SYMPTOMS1 S
opharyngeal Reflux (LPR) Laryngopharyngeal Reflux (LPR)
For a representative visit contact us For a representative visit co
at: Repvisit@rb.com
References
vour1.Oral
McGlashan JA, et
Suspension. al. Eur Arch
Summary Otorhinolaryngol.
of Product 2009;266:243–251.
Characteristics. 2. Gaviscon
Updated June 2021. nephrocalcinosis
Advance Peppermint Flavour
Accessed Oral Suspension.and recurrent
Summary calcium
of Product containing Updated
Characteristics. renal calculi. Contains
June 2021. methyl parahydr
Accessed
December
e Tablets. 2021.of
Summary https://www.medicines.org.uk/emc/product/6715/smpc. 3. Gaviscon
Product Characteristics. Updated February 2021. Accessed Advance Mint Chewablereactions
December (possibly
Tablets. Summary delayed).
of Product Fertility, Pregnancy
Characteristics. and Lactation:
Updated February ● Pregnancy:
2021. Accessed December Clinical s
2021.of
ummary https://www.medicines.org.uk/emc/product/73/smpc. 4. Gaviscon
Product Characteristics. Updated September 2019. Accessed Advance2021.
December Aniseed post-marketing
Oral Suspension. Summary
https:// experience
of Product indicate
Characteristics. no September
Updated malformative
2019.nor foeto/neonatal
Accessed toxicity
December 2021. of the a
https://
www.medicines.org.uk/emc/product/6187/smpc. ● Breast feeding: No known effect on breast fed infants. Gaviscon can be used during bre
Prescribing information reactions have been ranked under headings of frequency using the following convention:
(1/10,000 andTo advertise in
GLOBAL HEALTH
please contact:
Vijay Pothula vijaya.pothula@nhs.net 01942 773546
SCON ADVANCE PRESCRIBE
PROVIDES GAVISCON ADVANCE GA
EFFECTIVE RELIEF FOR THE TREATMENT F
R PATIENTS WITH OF LPR
PR SYMPTOMS1 SYMPTOMS2–4
ngopharyngeal Reflux (LPR) ADVANCE
ontact usFor
at:aRepvisit@rb.com
representative visit contact us at: Repvisit@rb.com
nephrocalcinosis and recurrent calcium containing renal calculi. Contains methyl parahydroxybenzoate (E218) and propyl parahydroxybenzoate (E216): May cause allergic
nephrocalcinosis and recurrent calcium containing renal calculi. Contains methyl para
nt Flavour Oral Suspension. Summary of Product Characteristics. Updated June 2021. Accessed
reactions (possibly delayed). Fertility, Pregnancy and Lactation: ● Pregnancy: Clinical studies
wable Tablets. Summary of Product Characteristics. Updated February 2021. Accessed December
in more(possibly
reactions than 500 pregnantFertility,
delayed). women Pregnancy
as well as aand
large amount of
Lactation: ● data from Clini
Pregnancy:
post-marketing
ion. Summary experience indicate
of Product Characteristics. Updatedno malformative
September nor foeto/neonatal
2019. Accessed December 2021.toxicity
https:// of the activepost-marketing
substances. Gaviscon can be
experience used during
indicate pregnancy,nor
no malformative if clinically needed.toxicity of t
foeto/neonatal
● Breast feeding: No known effect on breast fed infants. Gaviscon can be used during breast ● Breast●feeding:
feeding. Fertility:
NoNo known
known effect
effect onon human
breast infants.Side
fedfertility. effects:
Gaviscon canAdverse
be used durin
reactions have been ranked under headings of frequency using the following convention: veryreactions
commonhave(1/10),been
common (1/100
ranked underandGlobal Hearing Health:
Progressing the goal
of hearing care for all
Shelly Chadha
Technical lead, Ear and hearing care, World Health Organization
E ven as the world battles a prolonged
pandemic, hearing loss must be
included among and addressed as
It is possible to address hearing loss
Many cases of hearing loss can be
a public health priority.1 This is so prevented through effective and
because: available measures. For example,
hearing loss resulting from infections,
birth complications, ear diseases,
Hearing loss is rising exposure to noise or ototoxic medicines.
In children, nearly 60% of hearing loss is
It is anticipated that by 2050 there could preventable.4
be nearly 2.5 billion people with some
degree of hearing loss, at least 700
million of whom will need rehabilitation
services to ensure that they do not face
its adverse consequences.2
Inaction is expensive
The human cost of unaddressed hearing
loss is huge for those living with it and
their families. At the same time, a heavy
price is also levied on the society at large.
National economies are losing close to
one trillion dollars each year, due to our
collective failure to adequately address
hearing loss.3
ENT UK GLOBAL HEALTH 2022 17Innovative, cost-effective technological WHO’s public health framework for
and clinical solutions are available that ear and hearing care
can benefit nearly everyone who has
a hearing loss. Millions are already In it’s recently launched World report on
benefitting from these developments. hearing, WHO outlines the need and
However, nearly 80% of people with means for hearing across the life course.
hearing loss live in low- and middle- It acknowledges the challenges faced in
income countries where services and making ear and hearing care accessible
resources for ear and hearing care for all and proposes strategies to address
remain elusive.2,5 these. Examples of strategies elaborated
within the report include: task sharing
among highly trained professionals and
other health workers that have lesser
training requirements, use of digital
technologies, and telehealth solutions,
among others. Most importantly, the
World report on hearing provides a
public health framework for making ear
and hearing care accessible as part of
universal health coverage.
Ear and hearing care is a sound
investment
Combining the power of technology
with sound public health strategies can
ensure that its benefits can reach all
those in need. Moreover, investment in
hearing care is a financially viable option,
as governments can expect a return of
nearly $16 for every dollar invested in
ear and hearing care.6
18 ENT UK GLOBAL HEALTH 2022Integrated people-centered ear and • Workforce capacity development by
hearing care (IPC-EHC) scaling up education programmes
for relevant EHC workforce; task
IPC-EHC envisions all people having sharing with and training of non-
equal access to quality ear and hearing EHC cadres.
care as part of health services that meet • Health information and data that
their needs across their life course. helps determine population needs
Countries can deliver IPC-EHC by and priorities, identify gaps and
ensuring access to evidence-based tracking progress towards the
interventions that are delivered through targets set.
a strengthened health system.
• Equitable access to high-quality
hearing technologies, which could
Key public health interventions be furthered by their inclusion
in governments’ lists of essential
Provision of EHC services across the life devices.
course are summarized in the acronym • Access to safe and quality
‘H.E.A.R.I.N.G.’.1 This refers to: Hearing diagnostic and surgical equipment
screening and intervention; Ear disease as well as the medicines required
prevention and management; Access to for EHC.
technologies; Rehabilitation services;
• Relevant and impact-oriented
Improved communication; Noise
research that supports
reduction; and Greater community
implementation of integrated
engagement. Each country must
people centered EHC across the life
determine which of the H.E.A.R.I.N.G.
course.
interventions best suit its needs. This can
be achieved through an evidence-based
consultative prioritization exercise that
considers, among other things, cost–
effectiveness, equity and financial risk
protection.
Implementation of identified
interventions through the IPCEHC
approach requires actions at all levels of
the health system through:
• Policy guidance and planning with
a collaborative approach, including
the setting of realistic and time-
bound targets.
• Sustainable financing and health
protection to ensure that people
can access quality EHC services
without impoverishment.
ENT UK GLOBAL HEALTH 2022 19Given the importance and benefits 2 Haile LM, Kamenov K, Briant PS, Orji
of investing in a systematic scale-up AU, Steinmetz JD, Abdoli A, Abdollahi
of EHC services, the World report on M, Abu-Gharbieh E, Afshin A, Ahmed
H, Rashid TA. Hearing loss prevalence
hearing calls for countries to strive for
and years lived with disability, 1990–
a minimum of a 20% relative increase in 2019: findings from the Global Burden
the effective coverage of EHC services of Disease Study 2019. The Lancet.
from by 2030 and identifies three tracer 2021 Mar 13;397(10278):996-1009.
indicators to monitor progress towards 3 McDaid D, Park AL, Chadha S. Estimat-
this goal. ing the global costs of hearing loss.
International Journal of Audiology.
2021 Mar 1;60(3):162-70.
Achieving this target requires 4 World Health Organization. Childhood
concerted action by all stakeholders Hearing Loss: Strategies for prevention
in the field of ear and hearing care and care. Geneva: WHO; 2016 . Avail-
including governments, international able at: https://apps.who.int/iris/han-
organizations, EHC professionals, civil dle/10665/204632
society and private sector entities. 5 Orji A, Kamenov K, Dirac M, Davis A,
Chadha S, Vos T. Global and regional
needs, unmet needs and access to
hearing aids. International journal of
References: audiology. 2020 Mar 3;59(3):166-72.
6 Tordrup D, Smith R, Kamenov K, Ber-
1 World Health Organization. World tram MY, Green N, Chadha S. Global
report on hearing. Geneva: WHO; 2021. return on investment and cost-effec-
Available at: https://www.who.int/pub- tiveness of WHO’s HEAR interventions
lications/i/item/world-report-on-hear- for hearing loss: a modelling study.
ing The Lancet Global Health. 2022 Jan
1;10(1):e52-62.
20 ENT UK GLOBAL HEALTH 2022ENT training and
services in a tertiary
care hospital of
Northern Province,
Sri Lanka
Abarnna Balasubramaniam1 and Balakrishnan Thirumaran2
1
Senior Registrar in Otorhinolaryngology & Head and Neck
surgery Teaching Hospital Jaffna Sri Lanka
2
Consultant ENT Surgeon, Teaching Hospital Jaffna Sri Lanka.
Introduction:
G overnment health care system of
Sri Lanka is broadly classified into
curative and preventive side. Curative
side is further divided into primary,
secondary and tertiary care (Table 1)
depending on the availability of the
facilities and the strength of the staff.
ENT surgeons are appointed from
secondary care onwards1.
The population of Northern Province
(NP) is around 1050000. NP has one
Teaching hospital (Teaching Hospital
Jaffna- THJ) with 2 consultant ENT
Surgeons, 4 District general hospitals
(DGH) and 2 type A Base hospitals for
Sri Lanka
ENT UK GLOBAL HEALTH 2022 21Table 1
secondary care services. Besides the Following procedures such as
TH, 2 DGH have acting ENT Surgeons, examination under microscope,
they are covering around 1:100000 Fiberoptic laryngoscope/
populations during weekdays. Therefore bronchoscope, Stroboscope,
ENT Surgeons in THJ cover 1:425000 Rigid nasal endoscope and
during weekdays and 1:525000 Functional endoscopic evaluation of
populations during weekends. swallowing are conducted whenever
the patient needs it.
ENT service in primary care setup • Inward patient care – Two ENT
is limited. They manage acute ENT wards are available, They have to
infections such as ear wax ENT foreign share with Orthopaedic unit. Each
bodies (if they are visible or large), ward has 10 beds for ENT patients
vertigo and allergic rhinitis depending with trained nursing officers.
on their ENT training. Rest, they either Here they manage the patients
transfer or refer the patients to the with infections, epistaxis, airway
hospital with ENT surgeon, depending problems and surgical patients.
on the severity of the disease3. Trauma patients are admitted
separately in the Accident and
Following services related to ENT are Trauma unit.
available in TH Jaffna2. • Investigations – Biochemical,
imaging, endoscopic and
• Clinic – Patients are referred histopathological facilities are
from outpatient department, available. Usual waiting list for
referred from other clinics, other routine imaging is less than a
wards of THJ and other hospitals. month except MRI. It goes upto 6
22 ENT UK GLOBAL HEALTH 2022to 7 months. ENT unit has one day should actively be involved to all
endoscopic session per week. But if the components of ENT services
any emergency can do procedures during their training period.
in other days also after get the • Audiology services –Screening
permission from relevant unit. and diagnostic test battery for
Histopathology reports are usually hearing are conducted to the
available in 2 weeks from the date patients from neonates to elderly
of procedure. including universal newborn
• Multidisciplinary team discussion hearing screening. Health advice
both local and virtual is available for and counselling to the patients
problematic cases. regarding hearing loss and its
• Surgeries – Wide range from prevention are given. Provide
minor to highly skilled surgeries hearing aids freely to the patients
and combined surgeries are done. with hearing loss.
During surgeries microscope, rigid • Speech and language therapy –
endoscopes, laser and coblator are These are provided to the patient
used whenever they are needed. with either speech or swallowing
• Training – To undergraduate problems.
medical students, postgraduate • Rehabilitation services - Eg:
trainees, nursing students and also Vestibular rehabilitation therapy for
conduct workshops to medical patients with chronic vertigo.
officers. Postgraduate ENT trainees
ENT UK GLOBAL HEALTH 2022 23Challenges to the ENT Units to provide • ENT casualty procedures for Covid
services are, 19 positive patients are done in
a separate theatre with full PPE.
• Long waiting list for surgery Therefore the ENT team needs to
especially ear surgeries (Eg: arrange the theatre time for them.
myringoplasty) as large population Transfer of patients also takes time.
is covered by THJ • Difficult to conduct telemedicine
due to lack of staff and
communication problems to the
Challenges after Covid-19 pandemic patients.
are,
• Most ENT examinations are aerosol References:
producing procedures- so need
to delay them until the RAT for 1 http://www.health.gov.lk/moh_fi-
Covid-19 were done. nal/english/hospital_government.
php?spid=24
• When the number of infected
2 Monthly Audit, Department of ENT
patients’ increases, routine theatre TH/Jaffna.
sessions are stopped. Only casualty 3 Personal communication with Primary
cases, emergency cases and care unit
malignant cases are done.
24 ENT UK GLOBAL HEALTH 2022Cost-effective innovations
in airway surgery amidst the
finite resources in Nepal:
An endeavor on balancing
the economic constraints
with the surgical care
Bigyan Raj Gyawali, MRCS-ENT (UK), MS,
FICS, FACS
Assistant Professor
Department of ENT-HNS, Maharajgunj
Medical Campus, Institute of Medicine,
T.U.Teaching Hospital, Kathmandu, Nepal
S urgical care in today’s world has
been tightly linked with engineering
and surgical outcomes have drastically
struggling with the basic health facilities
in the far-flung areas of the country. A
small market on one hand and exorbitant
improved with the advent of new cost of the modern surgical equipment
technologies. Researches, inventions, and appliances incommensurate with
and innovations have always been the economic standards of the patient on
foundation of patient care with the the other makes it difficult to deliver
majority of them being done from the quality surgical care especially amidst
developed part of the world. With a good the scenario where the concept of health
economy, developed countries have insurance is just emerging.
easy access to modern technologies,
surgical equipment, and appliances and While the country's economy and
this has a huge impact on treatment flaws from the concerned authorities
outcomes. Developing countries like to prioritize health sector has led to
Nepal, on the other hand, are yet this backlog, need-based researches
ENT UK GLOBAL HEALTH 2022 25and innovations should now be our the generous support of experts from
priority to improve patient care with the USA, the country’s central referral
utmost utilization of local resources and hospital, Tribhuvan University Teaching
manpower to deliver safe, results-driven, Hospital has been able to start pediatric
cost-effective care. Here, we share airway surgery services for the last couple
some of our cost-effective innovations of years.1 The surgery on one hand
in airway surgery to uplift the level of demands a good surgical finesse and on
airway surgical care in Nepal. the other requires costly equipment if
good outcomes are to be achieved. The
Airway surgery in Nepal is an emerging paucity of the cases and the surgeries
subspecialty in otolaryngology. With demanding good dexterity made us
Figure 1: 3D Designing and printing
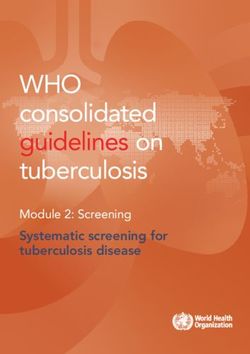
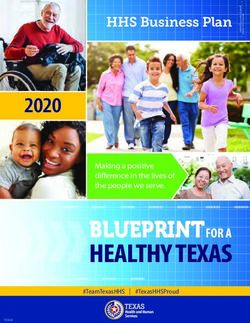
26 ENT UK GLOBAL HEALTH 2022feel a dire need of a simulation surgical airway. We used ITK-SNAP software for lab with airway specimens that could reconstruction purposes.2 The printed be practiced upon. Earlier, cadaveric airway specimens before surgery can goat larynx for simulation were used, be used not only for surgical simulation, however, they do not have a lot to offer practicing incisions and stitches, but also when it comes to dealing with airway to explain to patients the pathology and pathologies. This led us to incorporate the interventions being done as well as 3D reconstruction and printing into our to design prosthesis, laryngeal stents, practice. Three-dimensional printing in etc. The process of reconstruction and medicine is relatively a new dimension in printing is depicted in figure 1. Also, Nepal. Very few institutions in the country for simulation surgery, we designed an have 3D printers. We were supported airway surgery laboratory along with by an organization named SAMA a laryngeal stand that can hold the Nepal, which generates 3D printed specimen with an adjustable distance implants for orthopedic rehabilitation between the laryngoscope and the of disabled children. Three-dimensional specimen. A range of endoscopic and printing requires 3D reconstruction open surgeries can be practiced in this and generation of a printable format laboratory. Figure 2 shows our airway from the DICOM (digital imaging and surgery laboratory model along with the communication in medicine) computed laryngeal stand that we designed. tomography files of the patients’ Figure 2: Airway surgery laboratory model ENT UK GLOBAL HEALTH 2022 27
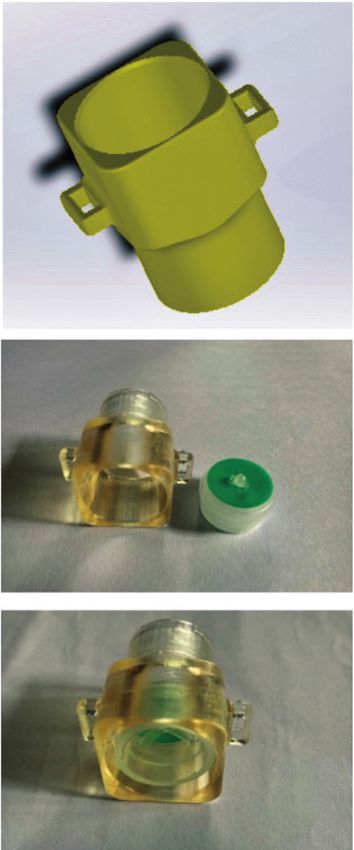
As of today, pediatric airway surgery is only being practiced in Tribhuvan University Teaching Hospital in Nepal. Despite the tireless efforts, surgical expertise yet remains to be enhanced when it comes to dealing with complex airway reconstruction and we have to rely most of the time on the experts from abroad to come and perform surgery in those cases. Supraglottic airway stenosis is one such problem that is very hard to deal with and often the patients are left with tracheostomy tubes for a considerable period. While managing a child with supraglottic stenosis, we felt a need for a speaking valve that could let the child speak while on a tracheostomy tube until the reconstructive surgery was done. However, speaking valves are not available in Nepal due to a very small market and very few consumers. Getting it from the neighboring countries is possible however, the cost would be very high which generally is unaffordable to the majority of our patients. This made us innovate a prototype of a speaking valve based on the design of the Passy-Muir speaking valve. We collaborated with engineers of the National Innovation Center, an organization that helps researchers to promote local innovations in Nepal. We designed a 3D model of an outer case and printed it with surgical guide Figure 3: Prototype of speaking valve resin that could harbor the valve. We used valves used in conduits of the mechanical ventilator for one-way flow speaking time was around 8 seconds, as the diaphragm. Figure 3 shows the with a median pitch of 108.04 Hz, end product, a prototype of a speaking Jitter: 2.21%, Shimmer: 18.53%, and valve. It was designed in such a way intensity of 63.9 dB. This prototype, that the air will flow through the valve however, needs approval from the DDA during inspiration and on expiration, (Department of Drug Administration) the valve would close to allow airflow of Nepal and currently is in the process through vocal cords and thus generate of procurement of the approval. Once the sound. On trial, the patient had a approved the valve will cost around 20 good speech with slight discomfort GBP which can be easily afforded by on expiration. With each expiration, our patients. 28 ENT UK GLOBAL HEALTH 2022
Surgical care should be tailored on a
need basis and there should always be
room for need-directed innovations.
Every effort should be made to deliver
the utmost patient care with the available
resources. Our innovations, although
being very small, could be a new start in
achieving the best surgical outcomes for
developing countries like Nepal.
Acknowledgments References
I would like to acknowledge Prof. 1 Guragain R, Gyawali BR, Dutta H,
Rajendra Guragain, Dr. Heempali Dutta, Neupane Y. Establishment of Paediatric
Airway Surgery Services in Tribhuvan
Dr. Yogesh Neupane, Mrs. Prabha
University Teaching Hospital: A Leap
Dawade from Institute of Medicine, in Otorhinolaryngology in Nepal.
Mr. Dhruba Raj Gyawali and Mr. Shyam Indian J Otolaryngol Head Neck Surg.
Shrestha from AnD Health Services and 2019;71(3):285-288. doi:10.1007/
ENT Care Center, Mr. Suresh Kaphle s12070-019-01706-x
and Mr. Rabin Dhamala from SAMA 2 Yushkevich PA, Piven J, Hazlett HC,
Nepal, Mr. Mahabir Pun and Mr. Samir et al. User-guided 3D active contour
segmentation of anatomical struc-
Aryal from National Innovation Center
tures: significantly improved effi-
for providing their immense support in ciency and reliability. Neuroimage.
this endeavor. 2006;31(3):1116-1128. doi:10.1016/j.
neuroimage.2006.01.015
ENT UK GLOBAL HEALTH 2022 29Making a difference,
practical involvement
in ENT Global Health
Mike Smith
From presentation at the ENT UK Global
Health Virtual Conference October 2021
Introduction So, what did I learn, and would I do it
all again?
H aving spent time in several LMIC,
particularly some years of full-time
work in Nepal, working in government Why go?
hospitals, charity hospitals, mission
hospitals, teaching hospitals, primary Motives vary and are often mixed. Many
health centres and remote communities, people simply want to help and know
I have experienced some of the issues they have been lucky enough to have
associated with cross cultural work. been given the skills to enable them to
Including running ear camps and do so. Some want to develop their own
building and staffing a specialist ear skills and learn in a different environment
hospital. Apart from Nepal I have trained and work with patients having more
and worked for short periods in North advanced or unusual conditions, and
and South India, Ethiopia, Uganda, and this is fine when checked by suitable
Thailand. This led me to think over the supervision. Some, for ethical, moral,
benefits and disbenefits of such work or political reasons feel called to go to
and discuss these with many people. people they perceive to be in need,
30 ENT UK GLOBAL HEALTH 2022whether to serve, or to teach or both. highly sceptical. Don’t be put off!
Many just want to travel and have It may well require some pushing,
an adventure. It could be a desire to but you are very unlikely to regret
teach, combine with a holiday, to see the move and will learn a lot,
family, or even perhaps dubiously as an not just medically but also in life
enhancement to a CV. Think about your experiences.
audience and what is most useful for • As a specialist, perhaps as a
them. Be aware that circumstances will senior trainee, consultant or GP.
probably not be exactly as you expect. Manoeuvering to get time out
Can you accept that, and are you able may be difficult, you may need
to adapt? to use study leave, annual leave,
unpaid leave, sabbatical, and
There are many personal benefits. You negotiate with family. Depending
will almost certainly make new friends on the length of time needed,
and relationships. Remember it is a a combination of these may be
partnership, working as a team and required.
respecting colleagues. • Retired. This may be an ideal time,
you have built up wide experience,
You will have new experiences, and hopefully are not too stuck
challenges, comical moments, and in your ways! You trained at a
incredible memories, and these may be time when equipment was more
some of the best of your life. limited, and you may find the same
equipment available in a LMIC. Or,
Timing, when and how long should you may have been at the forefront
you go for? of some technique or training
programme that you are asked to
There are different phases in our careers demonstrate in that LMIC.
when we may consider volunteering
e.g.: You may be thinking of a short visit of a
few days to a few weeks or much longer.
• As a trainee, between posts or Each has its benefits, depending on
as time out of training. Often circumstances.
the opportunity will depend on
the attitudes of colleagues and • Brief visits, such as a week or two,
bosses. Some will see great value useful to do some specific teaching
in such work and others will be or as a sampler with the intention
Opportunities to meet incredible people. Beautiful places and challenging travel.
ENT UK GLOBAL HEALTH 2022 31of going back when you know more • Ideally, work with local individual(s)
about the situation and can be with strong motivation. You need
more useful. This is probably what these for a lasting effect and
most people want to do and is most to make your visit worthwhile.
practical. Preferably team up with someone,
• Regular visits, with ongoing contact or an organisation, who has
and commitment are very valuable. influence and diplomatic skills in
• Longer term: months, or years. Not their medical establishment.
for everyone, but there are some • Situations and people change.
who commit for longer periods Don’t be disappointed, it is not
even in some cases for life. always easy to make cross cultural
relationships, foster change or see
development. You may find good
Challenges people that you work well with
move on, or even behave badly.
• Identify opportunities to work That does not make the work
overseas, this is often by word of ineffective, there will have been
mouth, perhaps something you benefit, but perhaps not exactly
heard in a conference, or may what you hoped for.
be part of a recognised regular • Accept limitations, failure,
programme. frustrations. If you are committed,
• Alone or team? If you go as part of you will find this hard. If you are a
a team, you will have back up and short-term visitor, do what you can
camaraderie, but may be insulated in a short time, and hope it has
from the daily difficulties faced by been a fruitful experience for all
your hosts. concerned, and if possible, keep in
• Covering costs. there are grants touch and continue to encourage
available, but the costs are unlikely and learn.
to be high. The major outgoing will
be for travel. You may well spend
more if you stay at home. Language and Culture
• Visa, medical registration. You
need to know the local regulations, • Do you speak a useful language
there may be a need to obtain a for that country? If so, that could
work permit, even as an unpaid be invaluable. The medical staff
volunteer. You should follow local may speak good English, but many
medical regulations, as we would patients will not. Try to learn and
expect of someone coming to speak a few phrases. It shows you
our home country. This will also are keen to communicate and can
protect you. This can take time and be fun.
paperwork such as copying your • The culture will be different,
certificates of qualification and and there may be many cultures
higher trainings and providing a CV. and languages even within one
It is straightforward to request the community. It is fascinating, not
GMC to send notification of your just for nice photos but to listen
UK medical registration directly to and appreciate different world
the medical council of the country views. You may be surprised how
involved, if needed. even simple assumptions and
32 ENT UK GLOBAL HEALTH 2022Climate
There may be better seasons to go, for
example in the dry season, when travel
may be easier and safer. Be prepared
with the right clothing.
Attitudes and expectations
• Don’t take on patients that are
beyond your experience, especially
for surgery. Even when you think
no one else local can help, be very
cautious. If things don’t go well,
apart from the harm to the patient,
you may not be supported.
• Expectations of you may be too
high (from staff and patients).
• Consider alternatives to your first-
choice treatment plan in your home
country, there may be more suitable
Try to learn some basic language terms or phrases. options in the circumstances.
Don’t drive people into more
poverty with expensive treatments.
attitudes in one culture can be Remember that patients may not
quite different in another. That return for follow up or comply
applies between international with medication. They have more
volunteers as much as with hosts. immediate problems in their lives.
Don’t jump to judgement when They may have different views
something appears wrong to of illness, including traditional
you. Mistakes can lead to offence beliefs or have no choice but to
or misunderstanding. Brush up follow advice from their family or
on things like dress code, table community leaders.
manners and gestures. • Use appropriate treatment, tailored
The Ear hospital in June, downpours are often daily during the
monsoon.
The INF Ear Centre at Green Pastures Hospital,
Pokhara, Nepal, in November, dry season
ENT UK GLOBAL HEALTH 2022 33to the patient’s social situation,
the equipment, and investigations
available, and other facilities, such
as nursing care.
• The local staff are used to this and
experienced, listen to their wise
counsel
• Do not criticize. In any culture,
but particularly in honour-shame
cultures, this will be offensive
and very hard to repair damaged
relationships.
• Local hierarchy and seniority are
important, even if you can see Urban development at the foot of the Himalayas, where many
obvious inequity, poor care or even still live by subsistence farming.
corruption, be very careful what you
say and to whom. significant risks, such as malaria,
• Centres such as teaching hospitals typhoid, hepatitis, HIV, dengue,
in major cities need sub-specialists Japanese encephalitis, rabies.
and complex expensive equipment Ensure you are vaccinated up to
and interaction with experts in the date and aware of local risk factors
field. However, regional medical and preventative strategies. Make
facilities need generalists and safe sure team members or hosts are
techniques that are appropriate, aware of your pre-existing medical
with teaching about the basics and conditions and take adequate
red flags for referral. (permitted) medication with you.
• Do whatever you can to support • Natural disasters, such as floods
those dedicated to work in their and landslides pose risks.
own country, despite the difficulties • Travel, especially road travel at
they encounter night, can be very hazardous. take
all reasonable precautions. Don’t
drive yourself if there is any choice.
Development and change • Crime, terrorism, kidnap, in some
areas these are real risks, and you
Low and middle income countries (LMIC) should avoid situations that could
are developing, often very fast. increase this.
• Politics; as a visitor keep clear of
Disparities in health care are growing demonstrations, media comments
between cities, deprived urban areas, and anything that could be
remote areas, rich and poor, and private perceived as offensive.
and government health care. Try to • Include time for travel delays in your
support those who are most in need. itinerary.
Consider risks Encourage research and audit
These will differ by country e.g.: It will usually be welcome if you offer
• Sickness, some areas have to be a mentor or share authorship to
34 ENT UK GLOBAL HEALTH 2022help colleagues get published. Help • Webinars, host one yourself or
the local team to critically analyse share links and participate together
their own research proposals and then discuss afterwards.
how to write clearly and reach the • WhatsApp and social media groups,
standards required by peer reviewed can offer good opportunities to
journals. Run a journal club meeting. discuss difficult cases (but consider
LMIC countries often lack data specific patient confidentiality).
to their situation or about medical • Facilitate international research
conditions rarely seen elsewhere. Much collaborations
of the research conducted in-country will • Help publicize global health issues,
be poor quality, for many reasons. Assist e.g.: Improve the ‘Audibility/
in building up information to better Visibility’ of the problem of hearing
inform public health and the evidence loss and ear diseases to those with
base. You may be able to assist in setting the power to make changes and
up research into low-cost solutions, through personal and professional
especially for the underprivileged. contacts.
Promote reflective practice audit,
to better understand personal and Equipment donation
institutional results. Sharing you own
audits and complications honestly may There are many pitfalls but done well
help. Ethics, and transparency in medical this can be an invaluable support.
practice are often lacking, possibly for
financial reasons, tread carefully, but try • Consider what can be improvised,
to demonstrate best practice. or bought locally, this may be
cheaper and more sustainable. It
may also be possible for others to
replicate effectively.
Auditing patient flow.
Make online connections
You may be able to help develop
connections, such as:
• Telemedicine, with access to
experts. A donated anaesthetic machine arrives with
• Seminars and case conferences. broken glass and missing parts.
ENT UK GLOBAL HEALTH 2022 35• Seminars for ENT surgeons and
general physicians, ask what
subjects they would like you to
teach, and offer some examples.
• Share your personal experience.
• Pre-prepare some suitable teaching
materials/presentations, case
studies, ready to deliver at short
notice if needed.
Donors and Fund raising
Fortunately in this case, with the help of a visiting • Can you raise donations (or useful
colleague and the local maintenance man, it was
equipment) before you go, or after
possible to replace or repair the broken parts
returning?
• Think of creative fundraising ideas,
events, presentations, etc.
• Think whether a donated item can
• Consider who to pass any donations
be affordably maintained.
to and how to ensure they reach the
• If you have the chance to beg or
right place.
buy suitable equipment that you
• Feedback to supporters.
can take with you, do so, but do not
add to a mountain of junk that lacks
parts or is past its useful life.
Set up or support a charity
(Take care with customs rules and
do not take items that are past their
Involve yourself in fund raising, whether
use by date).
you are a runner or a socialite everyone
• Only bring expensive equipment
has some way to help their chosen
at your peril! If parts such as spare
charities.
bulbs will be needed, then take a
Most charities desperately need
good supply.
manpower, for admin, website
development, social media and a host
of other tasks. Ask and see what they
Repair and maintenance
need.
Learn how to fix simple problems
yourself and show others.
When there is no local repair mechanism,
items are often discarded.
Training courses
Some examples of courses you could
offer or assist with would be:
• ENT red flag teaching to health
workers
Traveling to remote and unusual places.
36 ENT UK GLOBAL HEALTH 2022Gratitude and reward
Yes, it is possible to make a difference
and to enjoy the experience. OK,
so there are some challenges and
preparations to consider, but you will be
forgiven a lot as a foreigner and you will
make many new friends and memories,
and hopefully leave something useful
behind, and yes, I would do it all again.
Teamwork, making lifelong friends and colleagues.
Contact details
www.earaidnepal.org
mike.smith@earaidnepal.org
Periodical surveillance meetings to monitor the success of the hub & spoke model
ENT UK GLOBAL HEALTH 2022 37Deafness Screening &
Cochlear Implantation in
the Indian Subcontinent -
“The Hub & Spoke Model
of Tamil Nadu”
Prof. Mohan Kameswaran - MS, FRCSEd, FICS, FAMS, DSc,
DLO
Prof. Raghu Nandhan - MS, DNB, FRCS (ORL-HNS), MCh,
PhD
Consultant ENT Surgeons, Dept of Neurotology & Auditory
Implants,
Madras ENT Research foundation, Chennai, TN, India
Mail to: merfmk30@yahoo.com
Introduction
A s per a recent WHO report, there
are at present 360 million people
worldwide who have disabling hearing
the estimate of childhood deafness
at about 23 million. A nation-wide
survey by the National Program for
loss, out of which children constitute Prevention and Control of Deafness
nearly 35%. In the Indian subcontinent (NPPCD), has concluded that deafness
the national statistics report nearly 65 is the commonest congenital anomaly to
million people to suffer from severe to affect the huge 1.30 billion strong Indian
profound hearing disability, which puts population, with the incidence being
38 ENT UK GLOBAL HEALTH 20223:1000 live births. The presence of such a were implemented in India beginning
high incidence of hearing loss in children in the early 1970s and later, several
has been causing significant losses to hospitals established their own hearing
physical and economic productivity, screening programs. Presently, despite
since these children lose their skill to the lack of a universal newborn hearing
develop speech and language to grow screening program, several hospital-
up as disabled persons. based programs and some community-
based programs have evolved. In 2006,
Certain parts of India, especially the India launched the National Program
southernmost state of Tamil Nadu for Prevention and Control of Deafness
is heralded as the 'deafness state of (NPPCD), through which Institution-
India', and reports nearly double the based screening began to screen every
incidence of congenital deafness when baby born in a hospital or admitted
compared to the rest of the country. there soon after birth using OAE.
One possible reason for such high Community-based screening also was
incidence in Tamil Nadu (6/1000 live done simultaneously to screen babies
births) is the traditional custom of who are not born in hospitals, using
consanguineous marriages, which leads a brief questionnaire with behavioral
to propagation of the defective genes testing done by healthcare workers at
amongst members of the family across the time of their first immunization. By
generations. Multi-centric research work this effort, several children received
is presently ongoing to identify the Cochlear implants and hearing aids
unknown genetic factor responsible for in a timely manner to achieve good
the high deafness rates. outcomes.
Deafness Screening Programs Government Cochlear Implant
Schemes
Implementing universal newborn
screening in a vast country like India In India, establishing cochlear
has been a challenging task because of implantation as a treatment modality
a high birth rate (25 babies per 1000), for profound hearing loss has been a
diverse socio-economic and cultural daunting task. India was late to wake up
backgrounds, limited resources and to the reality of cochlear implantation.
a large rural population. Newborn In the late 90's there was skepticism
hearing screening (NHS) programs amongst the medical professionals and
the public alike regarding the usefulness
of this procedure. Prohibitive costs,
multilingual society and deep-rooted
cultural prejudices were other reasons for
non-acceptance of this technology. The
dilemma was to balance an advanced
and expensive technology with the
requirements of a developing country
with economic pressures. Gradually, the
situation began to change and in the
Deafness screening program at a peripheral centre last two decades, cochlear implantation
in Tamil Nadu has been established with universal
ENT UK GLOBAL HEALTH 2022 39and language development to join
mainstream schools. More recently, the
Government of India under its Ministry of
Social Welfare’s Assistance to Disabled
Persons scheme (ADIP) has launched
a Cochlear Implant Program that has
more than 130 empanelled centers for
performing implant surgeries. There
Reaching the doorstep: CI Habilitation in are nearly 10 states in the country that
progress at a satellite centre have successfully launched government
supported CI programs in the past few
acceptance as the standard of care, ably years.
aided by a rapidly growing economy
and expanding literacy rates.
The Successful Tamil Nadu State 'Hub
India has now crossed more than two & Spoke' Model
decades since CI technology reached
its shores. Today there are around 200 The Tamil Nadu Chief Minister’s
state-of-the-art cochlear implant centers Comprehensive Cochlear Implant
across India, in each major city with Scheme, stands as one of the pioneering
talented professionals and well equipped programs of India, with more than 4000
habilitation units for comprehensive cochlear implantations having been
management of deaf individuals. The done free of cost for poor and needy
“Cochlear Implant Group of India” children below the age of 6 years, which
which was conceptualized 15 years covers nearly 40 million population
ago based on the British Cochlear of rural Tamil Nadu. However, it soon
Implant Group, has successfully created became clear that the biggest challenge
awareness regarding CI and has for this scheme was auditory habilitation
provided the guidelines and support for as the habilitation centers were few
its propagation across the country. and located only in the major cities.
This necessitated that the child and
Even though more than 40,000 cochlear parents would have to be in the vicinity
implantations has thus far been done of such centers for at least an year –
across India, we still face an uphill task
with potentially one million children
awaiting implantation, for many of
whom cost of implant is a deterrent.
Hence, many State Governments have
now taken the initiative for fully funding
Cochlear Implants through their “Chief
Ministers Comprehensive Health
Insurance Schemes”. This innovative
program has been a resounding success
with a large number of congenitally
deaf children aged below 6 years that
have received free of cost implants
and with meticulous habilitation have The success story: Two pre-lingually deaf siblings implanted
now progressed to gain normal speech under the Government Scheme sharing a secret!
40 ENT UK GLOBAL HEALTH 2022project’ will be useful for expanding the
scheme to the whole state with the goal
to have a ‘deafness free Tamil Nadu’ by
2025. Similar success has been achieved
by neighboring southern states and the
rest of India.
The focus has now shifted to propagate
this technology further to the grass-
root level and reach all the remote
rural villages across this vast country.
Creating Public Awareness: Out-reach counseling program for The highly successful Indian IT industry,
parents which provides 24x7 services to the
Global citizens, has facilitated setting up
an economic impossibility for many a network of Telemedicine centers with
families. To overcome this obstacle, the broadband connectivity to offer remote
'Hub & Spoke' model was developed in programming and habilitation services
2006. It helped to deliver habilitation via at the door-step for cochlear implantees
quality assured satellite centers in rural hundreds of miles away from the parent
areas at the doorstep of the patient CI centre. The implant companies have
and helped to overcome the need for also extended their network of support
families to relocate many miles to the services to reach up to these implantees
state capital for the sake of their child. at their hometowns.
As a result, the percentage of children
attending habilitation increased from 60
to nearly 90%. The main center acted as Take Home Message
the main hub and peripheral ‘centers of
hearing‘ were created in 5 corners of TN The Indian hearing screening & habilitation
state with full facilities for diagnosing model's huge success has helped
hearing loss & habilitating children with start similar programs in neighboring
hearing loss who have received Hearing countries such as Nepal, Srilanka, and
aids or Cochlear Implants. Bangladesh. Indian surgeons have also
been mentoring similar CI programs in the
A recent cross-sectional study assessing African countries of Kenya, Tanzania and
the quality of outcomes in peripheral Nigeria. With the success of this national
centers showed no statistical difference program for eradication of deafness,
to those recorded in the state capital the distant dream of a 'deafness free
Chennai and found to correlate well India' now remains a possibility in the
with the duration of habilitation. The near future. The need of the hour today
implications of this unique model have is for the Indian government to enforce
a definite impact for clinical practice compulsory newborn hearing screening
and has provided the pedestal for and for hearing verification at the time
comparative multi-centric research work. of school admissions. Efforts to integrate
As the next step, currently 2 districts newborn hearing screening into the
have been identified for implementing immensely popular national vaccination
a pilot scheme for making the districts program has now been initiated, with the
deafness free. At the end of 2 years, hope of making it more effective than
the experience garnered from this ‘pilot before.
ENT UK GLOBAL HEALTH 2022 41You can also read