Fat distribution and storage: how much, where, and how?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Journal of Endocrinology (2007) 157 S39–S45 ISSN 0804-4643
Fat distribution and storage: how much, where, and how?
Ram Weiss
The Diabetes Center and the Department of Pediatrics, Hadassah Hebrew University School of Medicine, PO Box 12000, Jerusalem 91120, Israel
(Correspondence should be addressed to R Weiss; Email: weissr@hadassah.org.il)
Abstract
Obesity does not necessarily imply disease and similarly obese individuals may manifest obesity-related
morbidity or seemingly be in reasonably good health. Recent studies have shown that patterns of lipid
partitioning are a major determinant of the metabolic profile and not just obesity per se. The underlying
mechanisms and clinical relevance of lipid deposition in the visceral compartment and in insulin-
sensitive tissues are described. Increased intramyocellular lipid deposition impairs the insulin signal
transduction pathway and is associated with insulin resistance. Increased hepatic lipid deposition is
similarly associated with the majority of the components of the insulin resistance syndrome. The roles
of increased circulating fatty acids in conditions of insulin resistance and the typical pro-inflammatory
milieu of specific obesity patterns are provided. Insights into the patterns of lipid storage within the cell
are provided along with their relation to changes in insulin sensitivity and weight loss.
European Journal of Endocrinology 157 S39–S45
The prevalence of obesity among adults as well as compartments such as the intra-abdominal (visceral)
children is on the rise and gaining epidemic proportions compartment, and in insulin-sensitive tissues that are
(1). There is an overall consensus based on numerous prone to deposition of lipid in specific clinical scenarios.
longitudinal studies that obesity poses a significant risk This may cause deposition of lipid within skeletal
factor for the development of cardiovascular disease, muscle and the liver, affecting their normal metabolic
alterations in glucose metabolism, certain cancers, pathways.
intellectual deterioration, and reduces life expectancy. This review focuses on the metabolic impact of overall
Despite these observations, a significant proportion of adiposity and specifically lipid partitioning in the s.c.
obese individuals can achieve longevity without devel- tissue, visceral compartment, muscle and liver on
oping any of the morbidities previously mentioned. One metabolic complications of obesity. The importance
hypothesis to explain this observation is that total body and clinical relevance of each compartment are high-
fat is not the sole source of the adverse health lighted with regards to the metabolic manifestations
complications of obesity; rather the fat distribution or associated with each partitioning profile. Insights into
the relative proportion of lipids in various potential lipid the dynamics of the morphology of lipid storage within
deposition compartments is what determines the muscle are described. The ‘sub-clinical’ inflammation
metabolic risk of the individual. characteristic of increased body fat is discussed. The
Lipid deposition is an evolutionary advantageous majority of examples are from studies performed in
process that allows efficient storage of maximal calories obese children and adolescents.
per unit volume of tissue. The classic compartment
intended for storage of excess calories is subcutaneous
fat tissue that potentially also serves as insulation in
Relation of obesity, lipid partitioning, and
the face of cold temperatures. The capacity to store
metabolic risk
lipid within the s.c. tissue is the key to facing famine The close association of type 2 diabetes mellitus with
and limited caloric supply on the one hand and to cardiovascular disease led to the hypothesis that the two
handling excess calories on the other. In cases where may arise from a common antecedent (2, 3). It was
s.c. fat reaches a threshold beyond which it can store Reaven et al. (4) who noticed that common risk factors
no more, lipids may be shunted to other depots. In that of cardiovascular disease and altered glucose metab-
scenario, lipids may be stored in less advantageous olism tend to cluster in specific individuals and thus
named this constellation of risk factors ‘the insulin
This paper was presented at the Ipsen symposium, ‘The evolving resistance syndrome’, highlighting the critical role of
biology of growth and metabolism’, Lisbon, Portugal, 16–18 March peripheral insulin resistance as a driving force of the
2007. Ipsen has supported the publication of these proceedings. underlying pathological process. This concept has been
q 2007 Society of the European Journal of Endocrinology DOI: 10.1530/EJE-07-0125
Online version via www.eje-online.orgS40 R Weiss EUROPEAN JOURNAL OF ENDOCRINOLOGY (2007) 157
defined by the World Health Organization as the as class 2 obesity, and BMIR40 kg/m2 as class 3 obesity
‘metabolic syndrome’ (MS). According to the National (7). No similar classifications for the degree of obesity
Cholesterol Education Program and Adult Treatment exist for children and adolescents, except for the
Panel III, individuals meeting at least three of the definition of those whose BMI is between the 85th and
following five criteria qualify as having the MS: elevated 95th percentiles as ‘at risk for overweight’ and those at
blood pressure, a high triglyceride level, low HDL- greater than the 95th percentile as ‘overweight’. Several
cholesterol level, high fasting glucose, and central studies have shown that the degree of obesity has an
obesity (5). Because of its wide prevalence, the MS has adverse impact on the metabolic profile of obese youth,
enormous clinical and public health importance, even although no sub-categorization of the degrees of obesity
at its earliest stages, as it promotes atherosclerosis and within the upper 5 percentiles, as described in adults,
sets the stage for the development of diabetes (6). exists for children. When obese children were divided to
According to the paradigm presented herein, the impact moderately (BMI z score of 2–2.5, corresponding to the
of obesity is determined by the pattern of lipid 97–99.5 percentiles) and severely (BMI z scoreO2.5,
partitioning, i.e. the specific depots in which excess fat corresponding to the 99.5 percentile) obese and
is stored. The pattern of lipid storage has an impact on compared with overweight and non-obese children in
the adipocytokine secretion profile, on circulating regards to components of the MS (8), the impact of the
concentrations of inflammatory cytokines and on the degree of obesity was demonstrated. In that study,
free fatty acid (FFA) flux. The combined effect of these increasing obesity categories in children and adolescents
factors determines the sensitivity of insulin target were associated with worsening of all components of the
organs (such as muscle and liver) to insulin and impacts MS, specifically with an increase in fasting glucose,
the vascular system by affecting endothelial function. fasting insulin, triglycerides and systolic blood pressure,
Peripheral insulin resistance and endothelial dysfunc- and the prevalence of impaired glucose tolerance (IGT)
tion are the early promoters of future pathology, mainly and a decrease of HDL cholesterol were observed with
of cardiovascular disease and altered glucose metab- increasing adiposity. The prevalence of the MS, using a
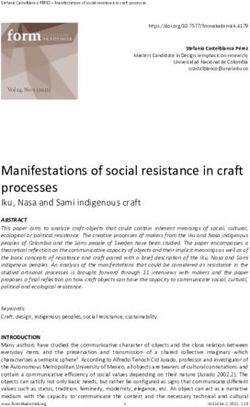
olism, eventually manifesting as type 2 diabetes (Fig. 1). modified conservative definition adjusted for the pedi-
atric age group, was w30% in the moderately obese and
nearly 50% in severely obese participants. When the
Degree of obesity and metabolic risk Bogalusa cohort participants (9) were stratified accor-
ding to discrete percentiles above the 90th for BMI, those
Classification of the degree of obesity in adults defines a in the 99th percentile for age and gender had a
BMIO30 kg/m2 as class 1 obesity, BMI 35–39.9 kg/m2 significantly greater prevalence of biochemical
Obesity
Altered lipid partitioning
Adipocytokines Cytokines FFAs
Insulin resistance Endothelial dysfunction
Metabolic syndrome
T2DM CVD
Figure 1 The metabolic effects of obesity are determined by patterns of lipid partitioning. A less favorable lipid partitioning pattern induces a
typical profile of circulating adipocytokines, inflammatory cytokines and free fatty acids (FFAs) that promotes peripheral insulin resistance
and endothelial dysfunction. The latter two are the mechanistic elements that drive the development of type 2 diabetes and accelerated
atherosclerosis.
www.eje-online.orgEUROPEAN JOURNAL OF ENDOCRINOLOGY (2007) 157 Fat distribution and storage S41
components of the MS and being above the 99th accumulate lipids in skeletal muscle may be differences
percentile for age and gender during childhood had a in quantity and functionality of the mitochondria within
very high predictive value for adult BMI of O35 kg/m2. the myocyte. Indeed, when elderly lean insulin-resistant
The implication of these studies is that among obese individuals were compared with younger body habitus
children and adolescents, those at the 99th percentile and activity-matched men using 13C and 31P magnetic
and above – in other words, the ‘severely obese’ – are an resonance spectroscopy, they were found to have a
extremely high-risk group for the presence of com- w40% reduction in oxidative phosphorylation (17).
ponents of the MS and for future class 2–3 obesity in When offspring of diabetics were compared with age- and
adulthood. Importantly, the prevalence of the MS, activity-matched insulin-sensitive controls, it was
regardless of the definition used, is significant even demonstrated that they had a w30% reduction rate of
among overweight and mildly obese children and ATP production in mitochondria of skeletal muscle (18).
adolescents (10, 11), and not limited to those with Lean offspring of diabetic parents have also been shown
severe obesity. to have lower mitochondrial content in skeletal muscle
and this is postulated to predispose them to increased
lipid accumulation within the myocyte (19). A second
Impact of lipid partitioning factor leading to IMCL accumulation may be fat
constituents of the diet. High-fat diets of varying
Obesity does not necessarily implicate pathology in durations have been shown to increase IMCL content
childhood or adulthood. Although obesity is the most by 36–90%, depending on their duration and baseline
common cause of insulin resistance in children and IMCL levels (20, 21). In physically inactive obese
adolescents, some obese youth may be very insulin individuals, a continuous increased supply of fatty
sensitive and thus be at reduced risk of the development acids by way of excess energy intake alongside a reduced
of the adverse cardiovascular and metabolic outcomes capacity to oxidize fat may lead overall fat storage,
driven by insulin resistance. In a study aimed at specifically in skeletal muscle. An obvious third source of
discovering the underlying pathophysiology of altered increased IMCL is an increase in circulating FFA
glucose metabolism in obese children and adolescents, it concentration, characteristic of obese insulin-resistant
was clearly demonstrated that those with IGT are individuals. These observations indicate that the
significantly more insulin resistant than those with
tendency to accumulate intramyocellular lipid may be
normal glucose tolerance, despite having an overall
genetically determined as well as influenced by diet and
equal degree of adiposity (12). The difference in insulin
activity and result from reduced quantity and altered
sensitivity was attributed to different patterns of lipid
functionality of myocellular mitochondria. A tendency
partitioning, where those with severe insulin resistance
were characterized by increased deposition of lipid in for increased IMCL deposition, which is partially
the visceral and intramyocellular compartments. genetically determined, predisposes individuals to
greater insulin resistance while obesity with low IMCL
deposition seems to be more ‘metabolically benign’.
The effects of intramyocellular lipid accumulation on
Intramyocellular lipid deposition the response of the myocyte to insulin stimulation are
not caused by the stored triglyceride per se. Rather, fatty
Increased intramyocellular lipid (IMCL) deposition has
acid derivates of the accumulated IMCL cause a
been shown to occur early in childhood obesity and be
directly associated with peripheral insulin sensitivity disturbance of the insulin signal transduction pathway,
(13). Importantly, not all obese children have increased eventually leading to reduced glucose uptake (22).
IMCL levels and those who do not are much more insulin The insulin signal transduction pathway culminates in
sensitive (14). Why intramyocellular lipid deposition the trafficking of glucose transporter 4 (GLUT-4) to the
differs between individuals who are seemingly equally cellular membrane, allowing transport of glucose into
obese and share common lifestyle and dietary habits is a the myocyte. In brief, insulin stimulation causes
matter of intensive research. An excellent model to study phosphorylation of insulin receptor substrate 1 (IRS-1)
this issue is lean offspring of patients with type 2 diabetes, leading to its binding and activation of phosphatidyl-
as they lack the confounding factors of obesity and inositol-3 (PI3) kinase. Activation of PI3 kinase leads to
hyperglycemia seen in obese patients with diabetes. GLUT-4 trafficking to the cell membrane, allowing
These individuals have been shown to have impaired glucose transport into the myocyte. Fatty acid derivates
insulin-stimulated non-oxidative muscle glucose dispo- within the cell have been shown to inhibit this signal
sal, i.e. to possess significant skeletal muscle insulin transduction pathway through activation of protein
resistance earlier than the development of any clinical kinase C–q which in turn blunts IRS-1 tyrosine
manifestation of altered glucose metabolism (15). The phosphorylation via a serine–threonine kinase cascade.
best correlate of insulin resistance in these lean Reduction of IRS-1 tyrosine phosphorylation leads to
individuals was indeed intramyocellular lipid content reduced PI3 kinase activation and reduced GLUT-4
(16). A putative explanation for the tendency to trafficking to the cellular membrane (23).
www.eje-online.orgS42 R Weiss EUROPEAN JOURNAL OF ENDOCRINOLOGY (2007) 157
Abdominal lipid deposition increased s.c. fat (33). The contribution of visceral fat to the
typical sub-clinical chronic inflammation seen in some
Upper body obesity, manifested clinically by increased waist obese individuals may thus be the causal link between
circumference, is known to be associated with cardiovas- visceral adiposity and the MS and its related morbidity.
cular disease and type 2 diabetes. The adverse impact of Indeed, adults with visceral adiposity tend to manifest
upper body obesity is implicated on accumulation of intra- insulin resistance, hypertension, a hypercoagulable state
abdominal (visceral) fat yet the adverse effects of abdominal and dyslipidemia in comparison with those who are equally
s.c. tissue should not be overlooked. The major source of obese with lower levels of visceral fat (34, 35). Increased
circulating FFAs is fat tissue and one can assume that with visceral adiposity has also been shown to be related to a
greater adiposity there is an increase in FFA flux. When FFA greater atherogenic metabolic profile in childhood (36).
flux is expressed per units of fat mass (from where FFAs are Visceral fat has been shown to be related to greater insulin
released), thus enabling a comparison of lean and obese resistance and lower insulin secretory response in obese
individuals, FFA turnover is w50% lower in obese children and adolescents (37), thus potentially promoting
compared to lean individuals (24). This may be attributed deteriorating glucose metabolism. Adiponectin levels are
to greater circulating insulin concentrations that may thus lower in obese children with increased visceral fat
prevent an overflow of FFAs released from the increased deposition (38), even when the comparison is made
lipid stores of obese persons. When FFA turnover is between those with similar overall adipositiy (10).
expressed per lean body (fat free) mass (where FFAs are
mainly consumed), FFA lipolysis is greater in obese
compared to lean individuals by w50% (25) and those
with upper body obesity have greater FFA lipolysis rates in
Hepatic lipid deposition
comparison to those with lower body obesity (26). These Non-alcoholic fatty liver disease (NAFLD) represents fatty
observations suggest that there are differences in the infiltration of the liver without excessive alcohol con-
regulation of lipolysis in adipose tissue in individuals with sumption (39). The spectrum of NAFLD ranges from
different obesity phenotypes. isolated fatty infiltration (steatosis) to inflammation
Visceral fat has been suggested to cause insulin (steatohepatitis, also known as NASH), to fibrosis and
resistance (27). Whether this relation is due to the relative even cirrhosis (40). Lipid accumulation in the liver is
resistance of visceral fat to insulin resulting in increased characterized as macrovesicular hepatic steatosis and is
FFA release is unclear. Elegant studies by Jensen et al. (28) the result of an imbalance between production and
revealed that increased visceral fat is indeed associated with utilization of triglycerides. There are three sources that
increased delivery of FFAs to the liver, yet that this visceral may increase the hepatic fatty acid pool: circulating FFAs
FFA flux is responsible for only about 20–30% and that from various adipose compartments discussed earlier,
splanchnic bed contributes up to 15% of FFAs reaching the de novo lipogenesis within the liver, and dietary factors that
liver. This implies that visceral fat is probably not the source promote lipogenesis. De novo lipogenesis, shown to be
of the majority of systemic circulating FFAs and its increased in NAFLD (41), is dependent on acetyl Co-
postulated effects on insulin resistance of tissues other enzyme A, an intermediate that enables proteins and
than the liver cannot be attributed to increased discharge of carbohydrates to be driven towards lipogenic pathways.
FFAs. Thus, the abdominal s.c. fat is probably the source of The two main effectors that drive hepatic de novo
increased circulating FFAs of lean and obese individuals. lipogenesis are acetyl-CoA carboxylase and fatty acid
Indeed, upper body fat (mainly from the s.c. abdominal synthase. Dietary factors that may promote hepatic
tissue) is lipolytically more active than lower body fat and lipogenesis include exogenous fatty acids as well as
contributes the majority of circulating FFAs in the post- carbohydrates which can drive triglyceride formation by
absorptive state (29, 30). This observation may explain the way of triose phosphate as a basis for glycerol formation
adverse metabolic implications of ‘male pattern obesity’, and by way of fatty acid formation by acetyl-CoA. A
characterized by greater upper body fat, in comparison specific dietary factor that promotes hepatic lipogenesis is
with ‘female pattern obesity’ which typically involves fructose which is an unregulated substrate for liver
greater lower body fat. Thus, the contribution of visceral fat triglyceride synthesis. Factors that decrease the hepatic
to insulin resistance may be related to elements other than fatty acid pool are either synthesis of triglycerides and
FFA discharge and its presence may be only a surrogate of phospholipids or fatty acid oxidation. Very low density
relatively increased upper body fat depots. A proposed lipoprotein and chylomicron remnants have also been
mechanism by which visceral fat may cause its adverse shown to contribute to hepatic triglyceride synthesis and
effects is related to secretion of inflammatory cytokines. storage (42). The rate-limiting step of mitochondrial
When examined in vitro, visceral fat has been shown to b-oxidation is the transfer of fatty acids into the
secrete increased amounts of inflammatory mediators, mitochondria, regulated by carnitine palmitoyl acyltran-
including CRP, IL-6, TNF-a, and PAI-1, compared to s.c. fat ferase-1 which is inhibited by insulin. The balance
(31, 32). Similarly, obese individuals with increased between lipogenesis and lipolysis in the liver is mainly
visceral adiposity have increased markers of systemic affected by the ratio of insulin and glucagon. In the case of
inflammation compared to equally obese subjects with insulin resistance, fatty acid flux to the liver is increased
www.eje-online.orgEUROPEAN JOURNAL OF ENDOCRINOLOGY (2007) 157 Fat distribution and storage S43
from increased lipolysis in adipose tissue leading to pattern that is advantageous and that enables efficient
increased fatty acid uptake. This in turn increases hepatic fatty acid utilization at times of exertion. Another
glucose output and triggers increased insulin secretion in observation that supports the importance of patterns of
order to maintain euglycemia. Increased concentrations lipid storage and not only lipid quantity comes from weight
of insulin in the liver induce de novo lipogenesis thus loss studies performed by Kelley et al. (51). A 4-month diet
creating a vicious cycle. The dietary factors such as and exercise weight loss program in obese adults resulted
increased consumption of carbohydrates (specifically in a weight loss of w10% body weight and a w45%
fructose) and saturated fats, typically seen in obese increase in insulin sensitivity. Intramyocellular lipid
subjects, may further contribute to hepatic lipogenesis. content did not significantly change, however lipid droplet
NAFLD is not confined to adults and is now the most size decreased significantly alongside an increase in
common liver disease among obese children and adoles- mitochondrial labeling and oxidative capacity. These
cents in North America (43, 44) with similar reports observations suggest that muscle lipid content per se is
coming from other countries (45, 46). The NHANES III not the major factor that determines insulin sensitivity,
survey found NAFLD to be more prevalent in obese African rather the way lipid is stored and packaged within the cell.
American and Hispanic males, with T2DM, hypertension An increase in insulin sensitivity, in this case caused by
and hyperlipidemia (47). These associations have led to the lifestyle modifications, induces storage of fat in smaller
hypothesis that NAFLD may precede the onset of type 2 droplets without affecting overall fat content and this
diabetes in some individuals. The natural history of NAFLD probably is coupled to the increased oxidative capacity that
in children is unknown yet it may progress to cirrhosis and is related to greater insulin sensitivity. Further studies are
related complications (48). The gold standard for the needed to investigate what determines storage patterns of
assessment of fatty liver is a liver biopsy yet recently several lipid droplets within cells and the effects of their proximity
non-invasive quantitative methods, such as specific to cellular structures such as mitochondria as
magnetic resonance imaging protocols and NMR spec- determinants of their potential ‘lipotoxic’ effect.
troscopy, have been developed to evaluate patients
suspected to have NAFLD. A surrogate typically used in
the clinical setting is screening of alanine amino
transferase (ALT) levels. In a study of 392 obese children
Lipid deposition and ‘sub-clinical
and adolescents (49), elevated ALT (O35 U/l) was found inflammation’
in 14% of participants, with a predominance of male Recent accumulating evidence indicates that obesity and
gender and white/Hispanic race/ethnicity. After adjusting insulin resistance are associated with sub-clinical
for potential confounders, rising ALT was associated with chronic inflammation (52). The immune and metabolic
reduced insulin sensitivity and glucose tolerance, as well as responses are tightly linked as both evolved from
increasing concentrations of FFAs and triglycerides. common structures, still present in primitive organisms
Worsening of glucose and lipid metabolism was already such as the Drosophila fat body which shares the
evident as ALT levels rose into the upper half of the normal functions of the liver and the hemetopoietic/immune
range (18–35 U/l). When hepatic fat fraction was assessed system (53). It is thus reasonable to assume that
using fast magnetic resonance imaging, 32% of subjects regulatory signal transduction pathways are shared by
had an increased hepatic fat fraction, which was the metabolic and immunological systems and respond
associated with decreased insulin sensitivity and adipo- to similar stimuli (54). The adipose tissue is not merely a
nectin, and with increased triglycerides and visceral fat. simple reservoir of energy stored as triglycerides, but
The prevalence of the MS was significantly greater in those serves as an active secretory organ releasing many
with fatty liver. These results implicate that fatty peptides and cytokines into the circulation (55). In the
infiltration of the liver is a common finding among obese presence of obesity, the balance between these numerous
children and adolescents and is associated with the molecules is altered, such that enlarged adipocytes
adverse components of the MS, namely insulin resistance, produce more pro-inflammatory cytokines (i.e. TNF-a,
dyslipidemia, and altered glucose metabolism. IL-6) and fewer anti-inflammatory peptides such as
adiponectin (56). The relation of elevated circulating
pro-inflammatory molecules and peripheral insulin
Patterns of intracellular lipid storage resistance is mediated by the common interface of
these signals and the insulin signal transduction
IMCL accumulation, as shown previously in this review, is pathway at the level of insulin receptor substrates
associated with peripheral insulin resistance. This obser- through activation of several serine kinases (57).
vation is generally true yet has a paradoxical exception – The dysregulated production of adipocytokines has
trained athletes have similar IMCL levels to obese diabetic been found to participate in the development of
insulin-resistant patients yet possess a much greater metabolic and vascular diseases related to obesity (58).
oxidative capacity (50). As trained athletes are very Evidence indicates that as the degree of obesity increases,
insulin sensitive and have low percent of body fat, they the adipose tissue is infiltrated by macrophages (59).
must therefore store the lipid within the myocyte in a Such macrophages may be the major source of
www.eje-online.orgS44 R Weiss EUROPEAN JOURNAL OF ENDOCRINOLOGY (2007) 157
pro-inflammatory cytokines initiating a pro-inflam- 7 Kuczmarski RJ & Flegal KM. Criteria for definition of overweight in
matory status that predates the development of insulin transition: background and recommendations for the United
States. American Journal of Clinical Nutrition 2000 72 1074–1081.
resistance and endothelial dysfunction (60). Indeed, 8 Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE,
inflammation may be the missing link between obesity Yeckel CW, Allen K, Lopes M, Savoye M, Morrison J, Sherwin RS &
and insulin resistance. In obese children and adoles- Caprio S. Obesity and the metabolic syndrome in children
cents, C-reactive protein, a marker of systemic inflam- and adolescents. New England Journal of Medicine 2004 350
2362–2374.
mation (61), and interleukin-6 levels are related to the 9 Freedman DS, Mei Z, Srinivasan SR, Berenson GS & Dietz WH.
degree and severity of obesity (8, 62). In contrast, levels Cardiovascular risk factors and excess adiposity among overweight
of adiponectin, an anti-inflammatory biomarker, children and adolescents: the Bogalusa Heart Study. Journal of
decreased with increasing levels of obesity and insulin Pediatrics 2007 150 12–17.
resistance. 10 Druet C, Dabbas M, Baltakse V, Payen C, Jouret B, Baud C,
Chevenne D, Ricour C, Tauber M, Polak M, Alberti C & Levy-
Marchal C. Insulin resistance and the metabolic syndrome in
obese French children. Clinical Endocrinology 2006 64 672–678.
Conclusion 11 de Ferranti SD, Gauvreau K, Ludwig DS, Neufeld EJ, Newburger JW &
Rifai N. Prevalence of the metabolic syndrome in American
Obesity is the major cause of insulin resistance in adolescents: findings from the Third National Health and Nutrition
childhood and insulin resistance probably drives the Examination Survey. Circulation 2004 110 2494–2497.
12 Weiss R, Dufour S, Taksali SE, Tamborlane WV, Petersen KF,
majority of obesity-related comorbidity. In general, as the Bonadonna RC, Boselli L, Barbetta G, Allen K, Rife F, Savoye M,
degree of obesity increases, so does the risk for disease, yet Dziura J, Sherwin R, Shulman GI & Caprio S. Prediabetes in obese
among equally obese individuals the pattern of lipid youth: a syndrome of impaired glucose tolerance, severe insulin
partitioning is what determines the metabolic profile. resistance, and altered myocellular and abdominal fat partition-
Increased deposition of fat in the visceral compartment, ing. Lancet 2003 362 951–957.
13 Sinha R, Dufour S, Petersen KF, LeBon V, Enoksson S, Ma YZ,
in muscle, and in liver, is associated with reduced insulin Savoye M, Rothman DL, Shulman GI & Caprio S. Assessment of
sensitivity and an adverse metabolic profile. The skeletal muscle triglyceride content by (1)H nuclear magnetic
tendency to accumulate fat in less favorable depots is resonance spectroscopy in lean and obese adolescents: relation-
genetically as well as environmentally determined. ships to insulin sensitivity, total body fat, and central adiposity.
‘Lipotoxic’ effects of intracellular lipids may be related Diabetes 2002 51 1022–1027.
14 Weiss R, Taksali SE, Dufour S, Yeckel CW, Papademetris X, Cline G,
to their pattern of storage. Insights into patterns of lipid Tamborlane WV, Dziura J, Shulman GI & Caprio S. The ‘obese
storage within insulin-sensitive tissues may shed new insulin-sensitive’ adolescent: importance of adiponectin and lipid
light on the sophistication of fatty acid utilization in partitioning. Journal of Clinical Endocrinology and Metabolism 2005
conditions of excess and of need. 90 3731–3737.
15 Rothman DL, Magnusson I, Cline G, Gerard D, Kahn CR,
Shulman RG & Shulman GI. Decreased muscle glucose trans-
port/phosphorylation is an early defect in the pathogenesis of
Disclosure non-insulin-dependent diabetes mellitus. PNAS 1995 92
983–987.
This paper forms part of a European Journal of 16 Krssak M, Falk Petersen K, Dresner A, DiPietro L, Vogel SM,
Endocrinology supplement, supported by Ipsen. The Rothman DL, Roden M & Shulman GI. Intramyocellular lipid
author discloses: concentrations are correlated with insulin sensitivity in humans:
a 1H NMR spectroscopy study. Diabetologia 1999 42 113–116.
Ram Weiss: no relation and no conflict of interest. 17 Petersen KF, Befroy D, Dufour S, Dziura J, Ariyan C, Rothman DL,
This article was subject to rigorous peer review before DiPietro L, Cline GW & Shulman GI. Mitochondrial dysfunction in
acceptance and publication. the elderly: possible role in insulin resistance. Science 2003 300
1140–1142.
18 Petersen KF, Dufour S, Befroy D, Garcia R & Shulman GI. Impaired
mitochondrial activity in the insulin-resistant offspring of patients
References with type 2 diabetes. New England Journal of Medicine 2004 350
664–671.
1 Haslam DW & James WP. Obesity. Lancet 2005 366 1197–1209. 19 Morino K, Petersen KF, Dufour S, Befroy D, Frattini J, Shatzkes N,
2 Hu FB, Stampfer JM, Haffner SM, Solomon CG, Willett WC & Neschen S, White MF, Bilz S, Sono S, Pypaert M & Shulman GI.
Manson JE. Elevated risk of cardiovascular disease prior to clinical Reduced mitochondrial density and increased IRS-1 serine phos-
diagnosis of type 2 diabetes. Diabetes Care 2002 25 1129–1134. phorylation in muscle of insulin-resistant offspring of type 2 diabetic
3 Haffner SM. Epidemiology of insulin resistance and its relation to parents. Journal of Clinical Investigation 2005 115 3587–3593.
coronary artery disease. American Journal of Cardiology 1999 84 20 Zderic TW, Davidson CJ, Schenk S, Byerley LO & Coyle EF. High-fat
11J–14J. diet elevates resting intramuscular triglyceride concentration and
4 Reaven GM. Banting lecture 1988. Role of insulin resistance in whole-body lipolysis during exercise. American Journal of Physi-
human disease. Diabetes 1988 37 1595–1607. ology. Endocrinology and Metabolism 2003 286 E217–E225.
5 Third Report of the National Cholesterol Education Program 21 Helge JW, Watt PW, Richter EA, Rennie MJ & Kiens B. Fat utilization
Expert Panel on Detection, Evaluation and Treatment of High during exercise: adaptation to a fat-rich diet increases utilization of
Blood Cholesterol in Adults (Adult Treatment Panel III): Executive plasma fatty acids and very low density lipoprotein-triacylglycerol in
Summary. NIH Publication N0 01-3670. Bethesda, MD: National humans. Journal of Physiology 2001 537 1009–1020.
Institutes of Health, 2001. 22 Shulman GI. Cellular mechanisms of insulin resistance. Journal of
6 Cersosimo E & DeFronzo RA. Insulin resistance and endothelial Clinical Investigation 2000 106 171–176.
dysfunction: the road map to cardiovascular diseases. Diabetes/ 23 Griffin ME, Marcucci MJ, Cline GW, Bell K, Barucci N, Lee D,
Metabolism Research and Reviews 2006 22 423–436. Goodyear LJ, Kraegen EW, White MF & Shulman GI. Free fatty
www.eje-online.orgEUROPEAN JOURNAL OF ENDOCRINOLOGY (2007) 157 Fat distribution and storage S45
acid–induced insulin resistance is associated with activation of 43 Roberts E. Nonalcoholic steatohepatitis in children. Current
protein kinase C theta and alterations in the insulin signaling Gastroenterology Reports 2003 5 253–259.
cascade. Diabetes 1999 48 1270–1274. 44 Lavine JE & Schwimmer JB. Nonalcoholic fatty liver disease in the
24 Horowitz JF, Coppack SW, Paramore D, Cryer PE, Zhao G & Klein S. pediatric population. Clinics in Liver Disease 2004 8 549–558.
Effect of short-term fasting on lipid kinetics in lean and obese 45 Tominaga K, Kurata JH, Chen YK, Fujimoto E, Miyagawa S, Abe I
women. American Journal of Physiology 1999 276 E278–E284. & Kusano Y. Prevalence of fatty liver in Japanese children and
25 Jensen MD, Haymond MW, Rizza RA, Cryer PE & Miles JM. relationship to obesity. An epidemiological ultrasonographic
Influence of body fat distribution on free fatty acid metabolism in survey. Digestive Diseases and Sciences 1995 40 2002–2009.
obesity. Journal of Clinical Investigation 1989 83 1168–1173. 46 Franzese A, Vajro P, Argenziano A, Puzziello A, Iannucci MP,
26 Koutsari C & Jensen MD. Thematic review series: patient-oriented Saviano MC, Brunetti F & Rubino A. Liver involvement in obese
research. Free fatty acid metabolism in human obesity. Journal of children. Ultrasonography and liver enzyme levels at diagnosis
Lipid Research 2006 47 1643–1650. and during follow-up in an Italian population. Digestive Diseases
27 Lebovitz HE & Banerji MA. Point: visceral adiposity is causally and Sciences 1997 42 1428–1432.
related to insulin resistance. Diabetes Care 2005 28 2322–2325. 47 Meltzer AA & Everhart JE. Association between diabetes and
28 Nielsen S, Guo Z, Johnson CM, Hensrud DD & Jensen MD. elevated serum alanine aminotransferase activity among Mexican
Splanchnic lipolysis in human obesity. Journal of Clinical Americans. American Journal of Epidemiology 1997 146 565–571.
Investigation 2004 113 1582–1588. 48 Feldstein AE, Canbay A, Angulo P, Taniai M, Burgart LJ, Lindor KD
29 Tan GD, Goossens GH, Humphreys SM, Vidal H & Karpe F. Upper & Gores GJ. Hepatocyte apoptosis and fas expression are prominent
and lower body adipose tissue function: a direct comparison of fat features of human nonalcoholic steatohepatitis. Gastroenterology
mobilization in humans. Obesity Research 2004 12 114–118. 2003 125 437–443.
30 Guo Z, Hensrud DD, Johnson CM & Jensen MD. Regional 49 Burgert TS, Taksali SE, Dziura J, Goodman TR, Yeckel CW,
postprandial fatty acid metabolism in different obesity phenotypes. Papademetris X, Constable RT, Weiss R, Tamborlane WV,
Diabetes 1999 48 1586–1592. Savoye M, Seyal AA & Caprio S. Alanine aminotransferase levels
31 Fain JN, Madan AK, Hiler ML, Cheema P & Bahouth SW. and fatty liver in childhood obesity: associations with insulin
Comparison of the release of adipokines by adipose tissue, adipose resistance, adiponectin, and visceral fat. Journal of Clinical
tissue matrix, and adipocytes from visceral and subcutaneous Endocrinology and Metabolism 2006 91 4287–4294.
abdominal adipose tissues of obese humans. Endocrinology 2004 50 Goodpaster BH, He J, Watkins S & Kelley DE. Skeletal muscle lipid
145 2273–2282. content and insulin resistance: evidence for a paradox in
32 Shimomura I, Funahashi T, Takahashi M, Maeda K, Kotani K, endurance-trained athletes. Journal of Clinical Endocrinology and
Nakamura T, Yamashita S, Miura M, Fukuda Y, Takemura K, Metabolism 2001 86 5755–5761.
Tokunaga K & Matsuzawa Y. Enhanced expression of PAI-1 in 51 He J, Goodpaster BH & Kelley DE. Effects of weight loss and physical
visceral fat: possible contributor to vascular disease in obesity. activity on muscle lipid content and droplet size. Obesity Research
Nature Medicine 1996 2 800–803. 2004 12 761–769.
33 Tsigos C, Kyrou I, Chala E, Tsapogas P, Stavridis JC, Raptis SA & 52 Wellen KE & Hotamisligil GS. Inflammation, stress, and diabetes.
Katsilambros N. Circulating tumor necrosis factor alpha concen- Journal of Clinical Investigation 2005 115 1111–1119.
trations are higher in abdominal versus peripheral obesity. 53 Leclerc V & Reichhart JM. The immune response of Drosophila
Metabolism 1999 48 1332–1335. melanogaster. Immunological Reviews 2004 198 59–71.
34 Yudkin JS, Juhan-Vague I, Hawe E, Humphries SE, di Minno G, 54 Beutler B. Innate immunity: an overview. Molecular Immunology
Margaglione M, Tremoli E, Kooistra T, Morange PE, Lundman P, 2004 40 845–859.
Mohamed-Ali V & Hamsten A; the HIFMECH Study Group. Low- 55 Rajala MW & Scherer PE. The adipocyte at the crossroads of
grade inflammation may play a role in the etiology of the energy homeostasis, inflammation and atherosclerosis. Endo-
metabolic syndrome in patients with coronary heart disease: the crinology 2003 144 3765–3773.
HIFMECH study. Metabolism 2004 53 852–857. 56 Matsuzawa Y, Funahashi T & Nakamura T. Molecular mechanism
35 Ridker PM & Cook N. Clinical usefulness of very high and very low of metabolic syndrome X: contribution of adipocytokines:
levels of C-reactive protein across the full range of framingham risk adipocyte-derived bioactive substances. Annals of the New York
scores. Circulation 2004 109 1955–1959. Academy of Sciences 1999 892 146–154.
36 Bacha F, Saad R, Gungor N, Janosky J & Arslanian SA. Obesity, 57 Taniguchi CM, Emanuelli B & Kahn CR. Critical nodes in
regional fat distribution, and syndrome X in obese black versus signalling pathways: insights into insulin action. Nature Reviews.
white adolescents: race differential in diabetogenic and athero- Molecular Cell Biology 2006 7 85–96.
genic risk factors. Journal of Clinical Endocrinology and Metabolism 58 Yudkin JS, Kumari M, Humphries SE & Mohamed-Ali V.
2003 88 2534–2540. Inflammation, obesity, stress and coronary heart disease: is
37 Cruz ML, Bergman RN & Goran MI. Unique effect of visceral fat on interleukin-6 the link? Atherosclerosis 2000 148 209–214.
insulin sensitivity in obese Hispanic children with a family history 59 Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL &
of type 2 diabetes. Diabetes Care 2002 25 1631–1636. Ferrante AW Jr. Obesity is associated with macrophage accumu-
38 Lee S, Bacha F, Gungor N & Arslanian SA. Racial differences in lation in adipose tissue. Journal of Clinical Investigation 2003 112
adiponectin in youth: relationship to visceral fat and insulin 1796–1808.
sensitivity. Diabetes Care 2006 29 51–56. 60 Pickup JC & Crook MA. Is type 2 diabetes mellitus a disease of the
39 Angulo P. Nonalcoholic fatty liver disease. New England Journal of innate immune system? Diabetologia 1998 41 1241–1248.
Medicine 2002 16 1221–1231. 61 Blake GJ & Ridker PM. Inflammatory biomarkers and cardio-
40 Ludwig J, Viggiano TR, McGill DB & Ott BJ. Nonalcoholic vascular risk prediction. Journal of Internal Medicine 2002 252
steatohepatitis: mayo clinic experience with a hitherto unnamed 283–294.
disease. Mayo Cinic Proceedings 1980 55 434–438. 62 Ford ES & National Health and Nutrition Examination Survey.
41 Diraison F, Moulin P & Beylot M. Contribution of hepatic de novo C-reactive protein concentration and cardiovascular disease risk
lipogenesis and reesterification of plasma non esterified fatty acids factors in children: findings from the National Health and
to plasma triglyceride synthesis during non-alcoholic fatty liver Nutrition Examination Survey 1999–2000. Circulation 2003
disease. Diabetes and Metabolism 2003 29 478–485. 108 1053–1058.
42 Parks EJ & Hellerstein MK. Thematic review series: patient-
oriented research. Recent advances in liver triacylglycerol and
fatty acid metabolism using stable isotope labeling techniques. Received 28 February 2007
Journal of Lipid Research 2006 47 1651–1660. Accepted 2 May 2007
www.eje-online.orgYou can also read