Factors Influencing Uptake of IPTp3+ Among Pregnant Women Attending ANC in Mawokota North Health Sub District, Mpigi District, Uganda
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
Factors Influencing Uptake of IPTp3+
Among Pregnant Women Attending
ANC in Mawokota North Health Sub
District, Mpigi District, Uganda
Kizito Omona [PhD]1*; Damali Mulungi1; Edson Twesigye1; Joram Tukamuhabwa1;
Medard Rukaari1; John Bosco Ninsiima1
Faculty of Health Sciences, Uganda Martyrs University, Uganda
Corresponding Author: Dr Omona Kizito, Lecturer. E-mail: komona@umu.ac.ug, Tel: +256706464873
DOI: 10.47760/cognizance.2021.v01i03.002
Abstract
Background: Annually, approximately 125 million pregnancies occur globally in malaria
endemic areas. 25 million pregnant women are at risk for malaria which accounts for over
10,000 maternal and 200,000 neonatal deaths annually. WHO recommends initiation of
IPT3+ in malaria endemic areas beginning with second trimester throughout pregnancy?
However, uptakes of IPT3+ remain low in many countries, for instance in Uganda, the
coverage of IPT3+ remains low at 66%.
Objectives: The study objectives were; to determine the socio-demographic factors of women
influencing uptake of IPTp3+, assess knowledge of women and facility related factors to offer
IPTp3+,
Materials and Methods: Analytical cross sectional study design was used employing mixed
methods. Quantitative data was collected using semi structured questionnaire among 150
women and qualitative data was collected from health workers as key informants.
Quantitative data was analysed using SPSS v20 while coding and themes were used for
qualitative data.
Results: Data was collected from 150 pregnant women. Study findings indicate that
knowledge about group at high risk of getting Malaria (χ2 = 4.113, df = 1, p = .043) and
knowing how to use the drug (χ2 = 6.590, df =2, p = .037) was significantly associated with
IPTP3+ Uptake of IPTp3+. The uptake of IPTp3+ was highest among pregnant women with
correct knowledge about group at high risk of getting Malaria (46.7%) and those who knew
about the drug dosage (26.7%).Findings further revealed that; the place Fansidar was picked
from (χ2= 15.318, df =4, p = .004) and staff availability to offer IPTP3+service (χ2 = 10.956,
df =2, p =.004) are the only facility related factors significantly associated with IPTP3+
Uptake. The uptake of IPTP3+ was highest amongst pregnant women who reported to have
picked Fansidar from health facility (45.3%) and reported availability of staff most of the
times (42.7%).
Conclusion: Knowledge about the group at risk of getting malaria, dosage of Fansidar,
Availability of the drug stocks at the facility and staff availability significantly affected uptake
of IPTP3+ by pregnant women in Mawokota North Health Sub District in Mpigi District.
Keywords: Intermittent Presumptive Treatment (IPT), Malaria, Pregnant Mothers, ANC
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 17cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
I. INTRODUCTION
Annually, approximately 125 million pregnancies occur globally in areas with Plasmodium
falciparum and Plasmodium vivax transmission (1). Malaria in pregnancy (MiP) contributes
to devastating maternal and neonatal outcomes, including maternal anaemia, maternal death,
stillbirth, spontaneous abortion, and low birth weight with an estimated 10,000 women and
100,000 infants dying as a result of malaria in pregnancy (1) and therefore Malaria is a
complex public health problem in African, where most cases and deaths are due to this
disease (2).
Twenty-five million pregnant women are currently at risk for malaria, and, according to the
World Health Organization. The impact is high in Sub Saharan Africa where women have
high chances of getting parasitemia (3). According to the World health organization(WHO),
In 2018, prevalence of exposure to malaria infection in pregnancy was highest in the West
African sub region and Central Africa (each with 35%), followed by East and Southern
Africa (20%). About 39% of these were in the Democratic Republic of the Congo and
Nigeria(4)
Uganda is ranked fourth among the highest malaria-burden countries in the world with some
of the highest transmission rates in the world; and pregnant women and children are
particularly vulnerable because of their reduced immunity (3) and it’s the leading cause of
Morbidity and mortality (5). Malaria is a febrile illness that predisposes mothers poor
pregnancy outcomes including severe or complicated malaria, abortion, premature labor,
maternal anaemia among others(4) and the benefits of using IPT3+ prevent this have been
documented (6).
To mitigate the consequences of Malaria in Pregnancy(MiP) in moderate to high malaria
transmission areas, the World Health Organization (WHO) recommends that pregnant
women receive intermittent preventive treatment during pregnancy (IPTp) with SP(7).SP is
the drug of choice for preventing malaria in pregnancy in Uganda (WHO, 2018). Intermittent
Preventive Treatment (IPT) decreases the incidence of low birth weight by 29%, severe
maternal anaemia by 38%, and neonatal mortality by 31%. (Roman et al 2019) IPTp is also
one of the major public health interventions.
In 2012, the WHO released a policy that promotes the initiation of IPT3+ in areas of
moderate to high malaria transmission, beginning as early as possible in the second trimester,
at each scheduled antenatal care (ANC) (9). Since 2016, 36 African countries had adopted a
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 18cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
policy of providing IPTp3 to pregnant women. In 2016, the WHO estimated that coverage of
IPTp1, 2, and 3 were 56%, 43%, and 19%, respectively. The gap between high ANC
attendance and the low proportion of eligible pregnant women receiving IPTp3 largely
reflects a failure of the health system to provide IPTp-SP at ANC facilities (1).
Uganda has scaled up IPTp to tackle the challenge of Malaria in pregnancy in line with
WHO recommendations. Sulfadoxine-pyrimethamine (SP) is the drug of choice for
prevention of malaria during pregnancy given by Directly Observed Therapy (DOTs)
system(10). There is slow uptake with 89 % of women receiving one or more doses of SP,
and this reduces to 45 % of those who received two or more doses and further down to 25 %
who received three or more doses. (6).The coverage in Uganda has remained low with slight
increase by only 4% to 66% from 63.2% in 2017/18 (11)
Despite of several interventions put in place to prevent malaria in pregnancy, up take of
IPTp3+ is still low hence the need for this study to establish factors affecting uptake of
IPTp3+. According to the Okethwangu et al., 2019 awareness of benefits for taking SP in
preventing malaria can influence it’s uptake. However side effects have not been documented
to affect it’s uptake(12).
In a study done by(10) about Knowledge and utilization of intermittent preventive treatment
for malaria among pregnant women about half 52.2% said that they have ever heard about
IPTp, 23% who had heard about IPTp were able to give a good definition of IPTp indicating
low knowledge. Education level correlate with knowledge about IPT as 77 % of pregnant
women knowledgeable about IPT3 had primary and secondary level educationChukwurah et
al., 2016,(14).
Facility staffing, availability of IPT 3 services affected IPT uptake. In Ghana 67% of facilities
lacked water for IPTp. Other factors reported like 56% stock outs at facilities and inadequate
supervision affected quality of service delivery. (2), (15) study revealed that there was lack of
safe water and sharing cups during taking of DOTs was also a challenge.
Health workers being knowledgeable, and this only benefits the women who attained ANC
(15). Findings from Ghana cost of services, distance to facility, Level of education, ANC
schedule (16),(17).Distance to the health facility, pregnancy disclosure is among factors that
affect ANC attendance and uptake of IPT3(9).
Elsewhere, in Malawi women reported obstacles were stock-outs of malaria test kits and
treatment at health facilities and the distance to treatment (15.9% and 15.0%, respectively).
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 19cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
Similarly, Availability and accessibility of malaria prevention and medication influenced
treatment uptake. This was mostly influenced by advice from healthcare staff and personal
experiences(12)
There is scanty information on factors hindering uptake of IPTp3+ in Mpigi District. This
study was done to asses factors affecting uptake of IPTp3+ Plus in in pregnant women with
special focus on; knowledge of pregnant mothers on use of IPT3+; determine facility
readiness to offer IPTp3+ and evaluate accessibility and availability of IPT3+ services in
Mawokota North Health Sub District in Mpigi District
This study is timely because understanding such factors is paramount for designing strategies
and programs for improving uptake and accessibility of IPT3+ services which will
consequently result in reduction of malaria in pregnancy and its associated factors.
II. OBJECTIVE
General Objective:
To assess Factors influencing uptake of IPT3 Plus among pregnant women in Mawokota
North Health Sub District, Mpigi District.
Specific Objectives:
1) To ascertain the level of uptake of IPTp3+ among pregnant mothers attending ANC in
Mawokota North Health Sub-district, Mpigi district
2) To determine the Socio-demographic factors influencing the uptake of IPTp3+ in
prevention of malaria in Mawokota North Health Sub District Mpigi District
3) To assess the knowledge of pregnant women on uptake of IPTp3+ in the prevention
of malaria
4) To determine the association between knowledge factors and IPTp3+uptake among
pregnant women attending ANC in Mawokota North Health Sub-District
5) To evaluate health facility related factors affecting uptake of IPTp3+ services in
Mawokota North Health Sub District in Mpigi District
III. MATERIALS AND METHODS
Analytical cross sectional study design was used employing mixed methods. A sample of 150
pregnant women attending ANC was used. Quantitative data was collected using semi
structured questionnaire. Qualitative data was collected from key informants using Key
informant guide. The study area was Mawokota North Health Subdistrict (HSD), in Mpigi
District. The district is in Central Uganda.
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 20cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
The study unit were Women attending ANC and eligible for IPTp3 and health workers
providing ANC care in selected facilities in Mawokota North HSD as key informants. The
sample size was calculated using Kish and Leslie formula (1965) and therefore, a total of 150
respondents were calculated.
The study used multi-stage random sampling to select the health sub district and facilities in
the health district and systematic random sampling of women to participate in the study.
Health workers were targeted as key informants at respective health facilities. The study used
semi structured questionnaire and Key informant guide. Data analysis was done using SPSS
v.20, and Qualitative data was analysed by Themes/content analysis. Cross Tabulation and
Pearson Chi-Square was performed to establish the Association between variables and
IPTp3+Uptake among pregnant Women. Data was analyzed descriptively, presented in tables
and figures as appropriate and Cross Tabulation and Pearson Chi-Square was performed to
establish the Association between Socio-Demographic Characteristics and IPTP3+ Uptake
among pregnant Women.
A letter of introduction from the university faculty of Health Sciences, Uganda Martyrs
University was taken to DHO, who endorsed it and introduced us to lower level facilities.
Verbal consent was sought before any data collected.
IV. RESULTS
Socio-Demographic characteristics
Majority of the respondents 41 (27.3%) were in the age bracket of 21-24 with the least group
9(6.0%) being in the age bracket of 37 and above. Adolescents and young women constituted
46.6%
Uptake of IPTp3+ Among Pregnant Mothers Attending ANC
IPTp3+Uptake among pregnant Mothers in Mawokota North Health Sub District, Mpigi
district is shown in figure 1 below
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 21cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
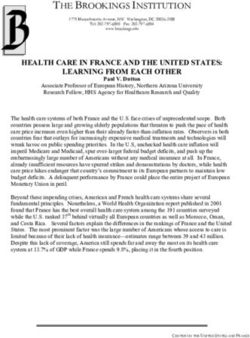
Figure 1: Uptake of IPTp3+ Among Pregnant Mothers
In the figure 1 above, the study found that among pregnant Mothers in Mawokota North
Health Sub District, Mpigi district most of them that 52.7% by proportion did not make use
of IPTp3+. The level of uptake of IPTp3+ was however as high as 47.5% among pregnant
Mothers in Mawokota North Health Sub District.
Socio-demographic factors influencing the uptake of IPTp3+ in the prevention of
malaria in Mawokota North Health Sub District District
Analysis of a number of socio-demographic factors was made. Cross Tabulation and Pearson
Chi-Square results for association between Socio-demographic factors and IPTp3+ Uptake
among Women was determined. See table 1 below
Table 1: Socio-demographic factors influencing the uptake of IPTp3+
Socio-demographic Variables IPTp3+Uptake Total Test Statistics
(n =150)
Yes No
Age in years
cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
Divorced 4(2.7%) 2(1.3%) 6 p = .779
Widowed 1(0.7%) 1(0.7) 2
Monthly Income
No Response 5(3.3%) 1(0.7%) 6 χ2 = 6.569
5000-cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
Association Between Knowledge Factors and IPTp3+Uptake Among Women
Cross Tabulation and Pearson Chi-Square for association between knowledge factors and
IPTp3+Uptake among Women was determined. See results in table 3 below
Table 3: Association Between Knowledge Factors and IPTp3+Uptake Among Women
Knowledge Variables IPTp3+ Uptake Total Test Statistics
Yes No (N = 150)
Knowledge about group at high Risk of getting
Malaria
Correct 70(46.7%) 72(48.0%) 142 χ2 = 4.113
Incorrect 1(0.7%) 7(4.7%) 8 df = 1
13 p = .043**
Aware of signs of Malaria
Fully Aware 52(34.7%) 65(43.3%) 117 χ2 = 1.890
Partially aware 17(11.3%) 13(8.7%) 30 df = 2
Not aware 2(1.3%) 1(0.7%) 3 p = .389
Knowledge of Fansidar in Preventing Malaria
Knowledgeable 59(39.3%) 60(40.0%) 119 χ2 = 1.166
Not Knowledgeable 12(8.0%) 19(12.7%) 31 df = 1
p = .280
Knows how to use the drug
Aware of drug dosage 40(26.7%) 30(20.0%) 70 χ2 = 6.590
Not aware of drug Dosage 30(20.0%) 49(32.7%) 79 df =2
No Response 1(0.7%) 0(0.0%) 1 p = .037**
Knowledge on effects of Malaria
Aware of All 37(24.7%) 41(27.3%) 41 χ2 = .060
Can Explain Some 31(20.7%) 34(22.7%) 34 df =2
Not aware 3(2.0%) 4(2.7%) 4 p = .970
Χ2 =Pearson Chi Square, df = Degree of Freedom, p=Probability Value
The findings in relation to knowledge shows that aware of signs of malaria (χ 2 = 1.890, df = 2,
p = .389), knowledge of fansidar in preventing malaria (χ 2 = 1.166, df = 1, p = .280) and
knowledge on effects of malaria (χ2 = .060, df =2, p = .970) had no significant association
with IPTp3+ Uptake among pregnant women in Mawokota North Health Sub District.
The study results, however, show that knowledge about group at high risk of getting Malaria
(χ2 = 4.113, df = 1, p = .043) and knowing how to use the drug (χ2= 6.590, df =2, p = .037)
was significantly associated with IPTp3+ Uptake among pregnant women in Mawokota
North Health Sub District. The uptake of IPTp3+ was highest among pregnant women with
correct knowledge about group at high risk of getting Malaria (46.7%) and those who knew
about the drug dosage (26.7%).
Facility Related Factors Affecting Uptake of IPTp3+ Services
Most of the pregnant women 125 (83.3%) received Fansidar from the facility, 12(5.3%)
received it from Private sector Clinics and only 1 (0.7%) got it from the drug shop. However,
8.0% of the women did not receive fansidar since they were not eligible to start on IPTp.
Majority of the respondents 57 (38.0%) stay within a distance of 0-5km and the least 25
(16.7%) stay in a distance of 16 km and above.
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 24cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
The facilities had an average of 5 staffs to offer the services, on average 4 staff had been
trained, 2 of the facilities had guidelines to offer the services, 1 of the facilities had received a
support supervision from the supervisory authorities and 1 facility had the required materials.
Table 4: Cross Tabulation and Pearson Chi-Square Results for Association between facility related factors
and IPTp3+Uptake among pregnant Women
Facility Related Variables IPTp3+Uptake Total Test Statistic
Yes No (n =150)
Place Fansidar was picked from
Health Facility 68(45.3%) 57(38.0%) 125
χ2 = 15.318
Clinic 2(1.3%) 10(6.7%) 12
df =4
Drug shop 0(0.0%) 1(0.7%) 1
p = .004**
First Time not Applicable 1(0.7%) 9(6.0%) 10
No Response 0(0.0%) 2(1.3%) 2
Distance from Home to health Facility
0-5km 25(16.7%) 29(19.3%) 54
6-10km 20(13.3%) 17(11.3%) 37 χ2 = 3.515
11-15km 15(10.0%) 16(10.7%) 31 df =4
16km and above 11(7.3%) 14(9.3%) 25 p = .476
No Response 0(0.0%) 3(2.0%) 3
Waiting time at the facility
Over Delayed 18(12.0%) 20(13.3%) 38
χ2 = .907
Slightly Delayed 12(8.0%) 13(8.7%) 25
df =3
It was appropriate 41(27.3%) 45(30.0%) 86
p = 0.824
No Response 0(0.0%) 1(0.7%) 1
Staff availability to offer IPTp3+service
Most of the times present 64(42.7%) 68(45.3%) 132 χ2 = 10.956
At times not there 2(1.3%) 11(7.3%) 13 df =2
Present but come late 5(3.3%) 0(0.0%) 5 p =.004**
Χ2 =Pearson Chi Square, df = Degree of Freedom, p=Probability Value
Findings regarding facility related factors indicates that the distance from home to health
facility (χ2= 3.515, df =4, p = .476) and waiting time at the facility (χ 2= .907, df =3, p = 0.824)
were not significantly associated with IPTp3+ Uptake among pregnant women in Mawokota
North Health Sub District.
The results, however, show that the place Fansidar was picked from (χ2= 15.318, df =4, p
= .004) and staff availability to offer IPTp3+service (χ2 = 10.956, df =2, p =.004) are the only
facility related factors significantly associated with IPTp3+ Uptake among pregnant women
in Mawokota North Health Sub District. The uptake of IPTp3+ was highest amongst pregnant
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 25cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
women who reported to have picked Fansidar from health facility (45.3%) and reported
availability of staff most of the times (42.7%).
V. DISCUSSION
Socio demographic factors affecting uptake of IPTp3+
The current study found that none of the demographic characteristics that’s age in years (χ2 =
1.292, df = 2, p = 0.524), education Level(χ2 = 4.670; df = 5, p = 0.457), marital Status (χ2 =
1.091, df = 3, p = .779), monthly Income (χ2 = 6.569, df = 4, p = .160), religion(χ2 = 4.906,
df = 5, p =0 .427), number of Pregnancies Carried(χ2 = 3.809, df = 2, p = .149) and number
of Children ever born (χ2 = 2.380, df = 2, p = .304) were influential in the uptake of IPTP3+
Uptake. Such a result is quite different from what was found Tanzania by Boateng and Anto
(2017) that poverty among mothers greatly hinders the use of ANC services. The
discrepancy in the current result could be attributed to variations of measurement as only
monthly income was the only aspect considered in this study, yet poverty levels encompass
several including assets.
Knowledge factors and uptake of IPTp3+
In this study it was established that knowledge in terms of awareness of signs of malaria (χ 2 =
1.890, df = 2, p = .389), knowledge of fansidar in preventing malaria (χ 2 = 1.166, df = 1, p
= .280) and knowledge on effects of malaria (χ2 = .060, df =2, p = .970) did not significantly
influence IPTp3+ Uptake among pregnant mothers. This result is different from those in a
study which was done in Tanzania by (Mchwampaka et al., 2019) that mothers did not like
taking Fansidar because of its associated side effects such as nausea. Such contradictions
could be perhaps attributed to the fact that benefits of IPTp3+ exceed the side effects if well
known by the pregnant mothers themselves.
This study however showed that knowledge about group at high risk of getting malaria (χ2 =
4.113, df = 1, p = .043) and knowing how to use the drug (χ 2 = 6.590, df =2, p = .037) had a
significant influence on IPTp3+ Uptake among pregnant mothers. It was found that uptake
was highest among pregnant mothers with correct knowledge about group at high risk of
getting Malaria (46.7%) and those who knew about the drug dosage (26.7%). This result is
consistent with what was found by Akinleye, Falade and Ajayi (2009) that little knowledge
on the dosage of Fansidar was still a challenge and this greatly affects its usage. The result is
also consistent with what was earlier established by Chukwurah et al. (2016) that knowledge
enabled institution of possible preventive measures such the use of long lasting Insecticide
treated nets (which found out that pregnant women were at high risk of acquiring the malaria.
This could be attributed to fear of being infected as propelled by knowledge of the riskier
groups. Besides knowing how to use integrates efforts easing uptake.
Facility Related Factors and uptake of IPTp3+ among pregnant women.
This study found the distance from home to health facility (χ2 = 3.515, df =4, p = .476) and
waiting time at the facility (χ2 = .907, df =3, p = 0.824) were not significantly associated with
IPTP3+ Uptake among pregnant mothers in Mawokota North Health Sub District. This
finding is not similar to what was found in Malawi by Azizi, 2020) that distance to treatment
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 26cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
centers was a major obstacle for women is accessing health care and highlighted difficulties
encountered when trying to access finances to be used to travel to the health care facilities.
The current study in addition found that public health facilities having the Fansidar (χ 2 =
15.318, df =4, p = .004) and staff being readily available to offer IPTp3+service (χ2 = 10.956,
df =2, p =.004) significantly influenced with IPTp3+ Uptake among pregnant mothers. Such
results are much similar to what was earlier found in a similar study done in Ghana which
established that facilities were always stocked with IPT supplies and only experienced a stock
out only ounce and that’s even when the National medical Stores had caught fire. It was also
revealed that staff availability and IPTp supplies helped pregnant women to receive all the
prescribed drugs from the health facilities. In the same study staff confirmed that that they
were always supplied in time with IPTp supplies (18).
VI. CONCLUSION AND RECOMMENDATIONS
Study findings revealed that women’s socio-Demographic characteristic was not significantly
associated with uptake of IPTp3+. However, it revealed that Knowledge about the group at
risk of getting malaria, dosage of Fansidar drug, Availability of the drug stocks at the facility
ready to be dispensed to pregnant women and staff availability significantly affected uptake
of IPTp3+.
Recommendations:
1. We recommend frequent health education sessions for all pregnant women on the
importance of attending ANC and taking IPT during pregnancy with emphasis that
pregnant women are at a risk of Malaria.
2. The health workers, community leaders should intensify mobilization and
sensitization about the need for early ANC attendance, and the benefits of taking a
complete SP dosage during pregnancy.
3. The government should increase the staffing levels at all health care facilities as a
measure to improve uptake of IPT services.
4. Government and health Facilities should always maintain drug stocks and ensure that
all pregnant women receive the prescribed drugs from the facility.
VII. ACKNOWLEDGEMENT
The authors appreciate and acknowledge the support rendered by management Mpigi district
health office towards the success of this study. We are indebted to our respondents without
whom this study would not be possible
VIII. DECLARATION
The authors declare not conflict of interest. No external fund was got for this study
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 27cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
REFERENCES
1. Roman E, Andrejko K, Wolf K, Henry M, Youll S, Florey L, et al. Determinants of
uptake of intermittent preventive treatment during pregnancy : a review. Malar J
[Internet]. 2019;1–9. Available from: https://doi.org/10.1186/s12936-019-3004-7.
2. Doku DT, Zankawah MM, Boateng A, Gyamfi A. Factors influencing dropout rate of
intermittent preventive treatment of malaria during pregnancy. BMC Res Notes.
2016;1–7.
3. Okethwangu D, Opigo J, Atugonza S, Kizza CT, Nabatanzi M, Biribawa C, et al.
Factors associated with uptake of optimal doses of intermittent preventive treatment
for malaria among pregnant women in Uganda : analysis of data from the Uganda
Demographic and Health Survey , 2016. Malar J [Internet]. 2019;1–8. Available from:
https://doi.org/10.1186/s12936-019-2883-y.
4. Global Malaria Programme: WHO Global. World malaria report 2019 [Internet].
WHO Regional Office for Africa. 2019. Available from: https://www.who.int/news-
room/fact-sheets/detail/malaria.
5. Mbonye AK, Buregyeya E, Rutebemberwa E, Clarke SE, Lal S, Hansen KS, et al.
Treatment and prevention of malaria in pregnancy in the private health sector in
Uganda : implications for patient safety. Malar J. 2016;1–7.
6. Wanzira H, Katamba H, Okullo AE, Rubahika D. The challenge of using intermittent
preventive therapy with sulfadoxine / pyrimethamine among pregnant women in
Uganda. Malar J. 2016;1–7.
7. WHO. WHO policy brief for the Implementation of Intermittent Preventive Treatment
of Malaria in Pregnancy Using Sulfadoxine-Pyrimethamine (IPTp-SP). WHO Press
[Internet]. 2014;(October 2012):1–13. Available from:
http://www.who.int/malaria/publications/atoz/iptp-sp-updated-policy-brief-
24jan2014.pdf?ua=1.
8. Experience P. Implementing Malaria in Pregnancy Programs in the Context of World
Health Organization Recommendations on Antenatal Care for a Positive Pregnancy
Experience. 2018;64(January):1–7.
9. Bajaria S, Festo C, Mrema S, Shabani J, Hertzmark E, Abdul R. Assessment of the
impact of availability and readiness of malaria services on uptake of intermittent
preventive treatment in pregnancy (IPTp) provided during ANC visits in Tanzania.
Malar J [Internet]. 2019;18(1):1–10. Available from: https://doi.org/10.1186/s12936-
019-2862-3.
10. Akinleye SO, Falade CO, Ajayi IO. BMC Pregnancy and Childbirth Knowledge and
utilization of intermittent preventive treatment for malaria among pregnant women
attending antenatal clinics in primary health care centers in rural southwest , Nigeria : a
cross-sectional study. 2009;9:1–9.
11. MOH Uganda. The Republic of Uganda Ministry of Health Annual Health Sector
Performace Report 2016/17. Minist Heal Annu Heal Sect Perform Rep. 2019;1–147.
12. Pell C, Meñaca A, Afrah NA, Manda-Taylor L, Chatio S, Were F, et al. Prevention and
management of malaria during pregnancy: Findings from a comparative qualitative
study in Ghana, Kenya and Malawi. Malar J. 2013;12(1):1–13.
13. Chukwurah JN, Idowu ET, Adeneye AK, Aina OO, Agomo PU, Otubanjo AO.
Knowledge , attitude and practice on malaria prevention and sulfadoxine -
pyrimethamine utilisation among pregnant women in Badagry , Lagos State , Nigeria.
2016;7(3):1–6.
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 28cognizancejournal.com
Kizito Omona et al, Cognizance Journal of Multidisciplinary Studies, Vol.1, Issue.3, March 2021, pg. 17-29
14. Sabin L, Hecht EMS, Brooks MI, Singh MP, Antwi KY, Rizal A, et al. Prevention and
treatment of malaria in pregnancy : what do pregnant women and health care workers
in East India know and do about it ? Malar J [Internet]. 2018;1–13. Available from:
https://doi.org/10.1186/s12936-018-2339-9.
15. Mchwampaka WM, Tarimo D, Chacky F, Mohamed A, Kishimba R, Samwel A.
Factors affecting uptake of ≥ 3 doses of Sulfadoxine-Pyrimethamine for malaria
prevention in pregnancy in selected health facilities , Arusha region , Tanzania.
2019;0:1–8.
16. Boateng IO, Anto F. Intermittent preventive treatment of malaria in pregnancy : a cross
‑ sectional survey to assess uptake of the new sulfadoxine – pyrimethamine five dose
policy in Ghana. Malar J. 2017;1–9.
17. Portugaliza HP, Galatas B, Nhantumbo H, Djive H, Murato I, Saúte F, et al.
Examining community perceptions of malaria to inform elimination efforts in Southern
Mozambique: A qualitative study. Malar J [Internet]. 2019;18(1):1–14. Available from:
https://doi.org/10.1186/s12936-019-2867-y.
18. Amankwah S, Anto F. Factors Associated with Uptake of Intermittent Preventive
Treatment of Malaria in Pregnancy : A Cross-Sectional Study in Private Health
Facilities in Tema Metropolis , Ghana. 2019;2019.
©2021, Cognizance Journal, cognizancejournal.com, All Rights Reserved 29You can also read