Experimental validation for the Achilles tendon reinforced with new techniques
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Article
Genij Ortopedii. 2022. Vol. 28, no. 1. P. 76-82.
Original article
https://doi.org/10.18019/1028-4427-2022-22-1-76-82
Experimental validation for the Achilles tendon reinforced with new techniques
G.P. Kotelnikov, Yu.D. Kim, D.S. Shitikov, N.A. Knyazev, N.E. Likholatov
Samara State Medical University, Samara, Russian Federation
Corresponding author: Yuriy D. Kim, drkim@mail.ru
Abstract
An Achilles tendon injury is most common among subcutaneous tendon ruptures and accounts for 47 %. The purpose was to
experimentally evaluate the effectiveness of new methods of the Achilles tendon reinforcement. Material and methods The
experimental part of the work was performed in 3 stages using 60 biomannikins with intact Achilles tendon. A Krakow suture was
used at stage 1 for a group of 20 tendons and a force that would result in rupture of the tendon was measured. Reinforcement was
performed using the plantaris tendon (technical innovation offered at the Samara State Medical University) at the 2nd stage and the
force required for the appearance of signs of rupture was subsequently measured. A portion of the peroneus longus tendon (RF patent
No. 2616767) was used for reinforcement at the 3rd stage and the force measurement produced. Results The mean force required to
rupture the Krakow suture applied to the tendon at the first stage was 11.5 kg., The force required to rupture the suture reinforced with
the plantaris tendon at the second stage measured 33.4 kg. The force required to rupture the suture reinforced with a portion of the
peroneus longus tendon at the third stage was 37.3 kg. Conclusion The new techniques offered to reinforce the Achilles tendon with
the plantaris tendon and a portion of the peroneus longus tendon at the distal base facilitated increase in the strength of the injury site
by 195.6 % and 214.4 %, respectively.
Keywords: Achilles tendon, experiment, reinforcement
For citation: Kotelnikov G.P., Kim Yu.D., Shitikov D.S., Knyazev N.A., Likholatov N.E. Experimental validation for the Achilles tendon
reinforced with new techniques. Genij Ortopedii, 2022, vol. 28, no 1, pp. 76-82. https://doi.org/10.18019/1028-4427-2022-28-1-76-82
INTRODUCTION
Achilles tendon injuries are the most frequent and according to indications allows increase of the strength
account for up to 47 % among subcutaneous ruptures [1–3]. of the Achilles tendon suture. Some authors suggest
Rerupture is one of common complications of Achilles strengthening the rupture zone with synthetic materials
tendon surgery along with infection and requires increasing the risk of infectious complications [12],
repeated interventions [4, 5]. There is controversy on others do not find primary reinforcement of the Achilles
prevention strategy [6–9]. Consequences of prolonged tendon necessary with the established methods.
ankle immobilization leading to severe hypotrophy The purpose was to experimentally evaluate the
of the triceps are reported with a long rehabilitation effectiveness of new methods of the Achilles tendon
period [10, 11]. Early activation of the ankle joint is reinforcement.
important avoiding elongation of the Achilles tendon Research objectives:
that would result in decreased plantar flexion of the 1) evaluate the strength of the Achilles tendon using
foot. The strength of the Achilles tendon suture can be the Krakow whipstitches, new reinforcement methods
increased with modern suture material minimizing the for the Achilles tendon in the experiment and compare
risks of infectious complications due to the subcutaneous the results obtained;
location of the tendon avoiding ligature fistulas, deep 2) identify indications for primary reinforcement
and superficial necrosis and preserving the sliding of the Achilles tendon in clinical practice using new
apparatus at the site. Reinforcement of the rupture site techniques.
MATERIAL AND METHODS
The experimental part of the work was performed performed using the plantaris tendon (technical
using 60 tendons of biomanequins with intact Achilles innovation offered at the Samara State Medical
tendon. Three experimental groups were identified. A University) in addition to the Krakow suture in the
linear or Z-shaped access on the posterior aspect of the second group and the force required for the appearance
tibia was produced in the 3 groups and the Achilles of signs of rupture was subsequently measured.
tendon was intersected in the "classical" rupture zone A portion of the peroneus longus tendon (RF patent
(20–50 mm from the enthesis) and the Krakow suture No. 2616767) [13] was used for reinforcement in
applied. The strength of the experimental Achilles addition to the Krakow suture in the 3rd group and the
tendon repaired with the Krakow suture was measured force required for the appearance of signs of rupture
in the first group (20 tendons). Reinforcement was was measured. The weight required for the appearance
© Kotelnikov G.P., Kim Yu.D., Shitikov D.S., Knyazev N.A., Likholatov N.E., 2022
Genij ortopedii. 2022. Vol. 28, no. 1 76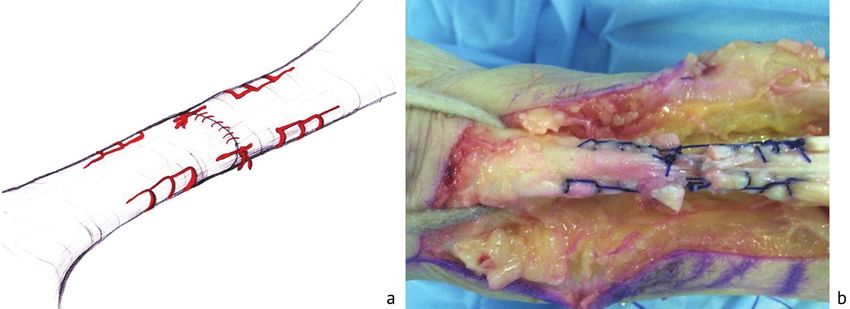
Original Article
of signs of rupture was measured in all study groups (Fig. 1b). The mean strength value in 20 experiments
(60 tendons) using the Garin electronic weighbeam was 11.5 kg (112.78 N).
(measuring accuracy of 10 grams). The second group (20 experiments) included the
The article was reviewed by the SamSMU Bioethics Achilles tendon reinforced with the plantaris tendon.
Committee for compliance with ethical standards. Based The reinforcement technique was patented as a technical
on evidence-based medicine statistical processing of the innovation at the SamSMU. A VICRIL 1 thread was
results was produced using the Statistica 6.0 program. used for the suture. Then the Krakow suture was applied
Testing of the null hypothesis about the absence of the to the distal and proximal ends of the Achilles tendon.
reinforcement effect was performed in three ways. The The threads were connected with each other, and
confidence intervals of the means calculated for the adaptive sutures used for the rupture. Then the plantaris
samples at each stage of the study did not overlap with tendon was distally exposed to preserve the nutrition
each other and were arranged in a strict sequence from of the latter. The average length of the plantaris tendon
the third stage to the first. was 340 mm and thickness measured 2 mm. The length
The first group included 20 experiments of the was sufficient to reinforce the rupture site. The plantaris
Achilles tendon stitched with the Krakow suture using tendon was U-shaped and X-shaped in the Achilles
VICRIL 1 thread. Then the Krakow suture was applied tendon with 5 cm off the rupture site and additionally
to the distal and proximal ends of the Achilles tendon. fixed in the Achilles tendon with nonskid sutures
The threads were connected with each other followed (Fig. 2a). Then the distal end of the Achilles tendon
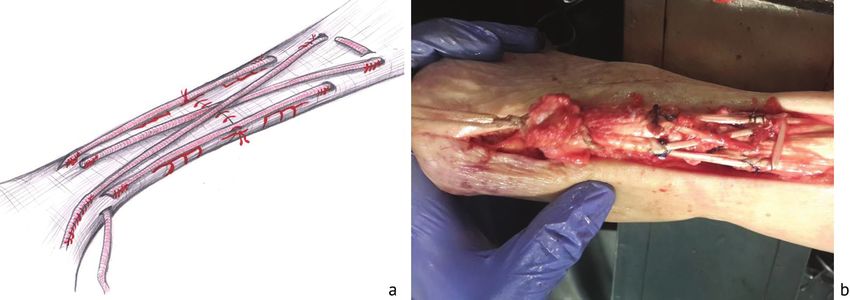
by adaptive sutures applied at the gap (Fig. 1a). Then was cut off with a portion of the calcaneus fixed with
the distal end of the Achilles tendon was cut off with a a 5 mm thread. The weight required for the appearance
portion of the calcaneus fixed with a 5 mm thread. The of signs of rupture of the Krakow suture was measured
weight required for the appearance of signs of rupture using the Garin electronic weighbeam (measurement
of the Krakow suture was measured using the Garin accuracy of 10 g) (Fig. 2b). The mean strength value in
electronic weighbeam (measurement accuracy 0.1 g) 20 experiments was 33.4 kg (327.54 N).
Fig. 1 The diagram showing the Krakow suture of a tendon (a) and signs of rupture of the tendon suture in the experiment (b)
Fig. 2 Diagram showing the suture reinforced with the plantaris tendon (a) and appearance of rupture signs (b)
77 Genij ortopedii. 2022. Vol. 28, no. 1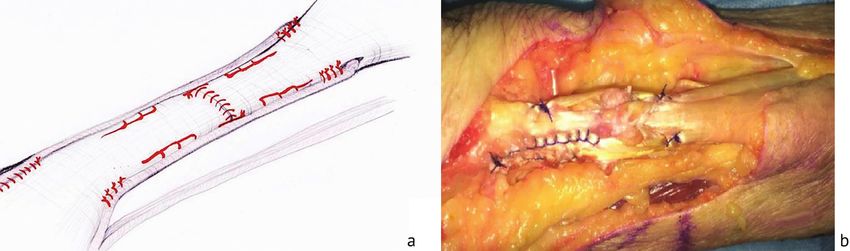
Original Article
The third group included 20 experiments of the fixed with a 5 mm thread. The weight required for the
Achilles tendon reinforced with a portion of the appearance of signs of rupture of the Krakow suture
peroneus longus tendon. The technique of the Achilles was measured using the Garin electronic weighbeam
tendon reinforcement was patented with invention (measurement accuracy of 10 g) (Fig. 3b).
No. 2616767 [13]. A VICRIL 1 thread was used for Null hypothesis testing of the reinforcement
the suture. Then the Krakow suture was applied to the effect was performed in three stages. Initial data and
distal and proximal ends of the Achilles tendon. The descriptive statistics were collected at the first stage.
threads were connected with each other, and adaptive The second stage aimed at checking homogeneity
sutures were used for the rupture site. A portion of of standard deviations. The third stage was meant to
the peroneus longus tendon was distally exposed verify the homogeneity of math expectations. The
to preserve nutrition. On average, the portion of the linear model constructed for correlations between the
peroneus longus tendon used was 190 mm long and tensile force and the reinforcement method had a high
5 mm thick. The length was suffecient to reinforce level of significance (coefficient of determination
the rupture site. The portion of the peroneus longus R2 = 0.99, Fisher criterion F = 3079, p » 0). Multiple
tendon was U-shaped in the Achilles tendon with 5 comparisons of the means in the groups performed by
cm off the rupture site, stitched at the medial side and randomization and using Bonferroni correction showed
additionally fixed in the Achilles tendon with nonskid a high significance of the reinforcement effect of the
sutures (Fig. 3a). Then the distal end of the Achilles plantar tendon (Student's criterion t =19.5, p » 0) and
tendon was cut off with a portion of the calcaneus the peroneus longus tendon (t = 23, p » 0).
Fig. 3 Diagram showing the suture reinforced with the portion of the peroneus longus tendon (a) and appearance of rupture signs (b)
RESULTS
The average strength value in 20 experiments of Table 1 (continued)
the first group was 11.5 kg (112.78 N) (Table 1). The Comparison of the forces required for the rupture
average operation time was 45 min. of the Krakow suture
The average strength value in 20 experiments of the Experiment No. Result, kg Force (N)
second group was 33.4 kg (327.54 N) (Table 2). The 7 12.50 122.58
average operation time was 55 min. 8 12.16 119.25
The average strength value in 20 experiments of 9 11.79 115.62
the third group was 37.3 kg (365.79 N) (Table 3). The 10 10.88 106.70
average operation time was 60 minutes.
11 12.24 120.03
Table 1
12 10.73 105.23
Comparison of the forces required for the rupture
of the Krakow suture 13 11.62 113.95
14 12.07 118.37
Experiment No. Result, kg Force (N)
15 9.85 96.60
1 12.36 121.21
16 11.71 114.84
2 11.58 113.56
17 10.56 103.56
3 9.74 95.52
4 11.87 116.40 18 13.02 127.68
5 10.42 102.19 19 9.91 97.18
6 13.06 128.07 20 12.47 122.29
Genij ortopedii. 2022. Vol. 28, no. 1 78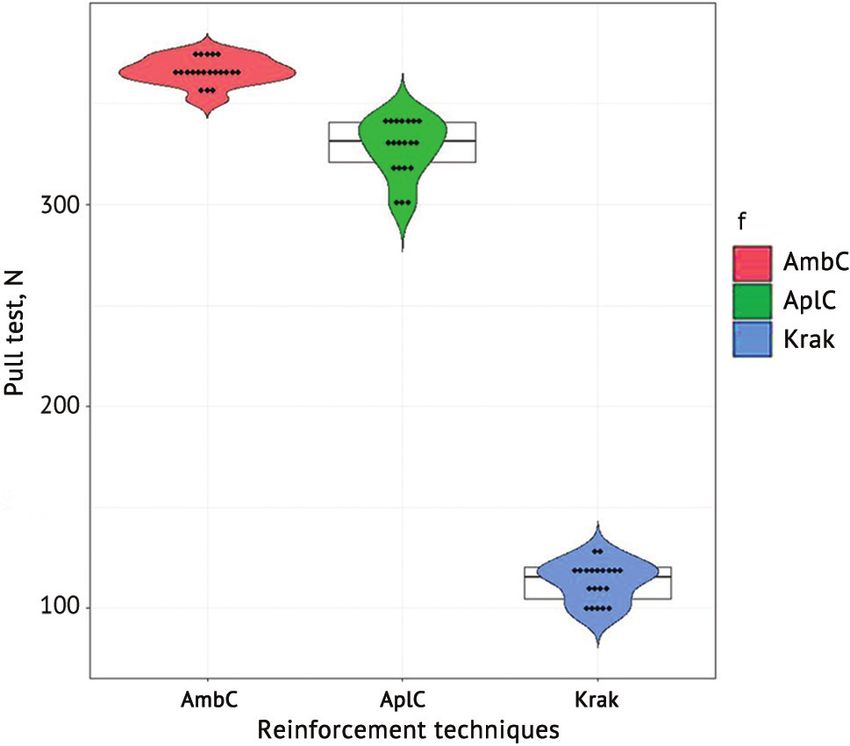
Original Article
Table 2 With numerical values received statistical data
Comparison of the forces required for the rupture processing was produced in 3 stages.
of the Achilles tendon suture reinforced 1. Baseline data and descriptive statistics
with the plantaris tendon Dependent variable: pull test, N
Experiment No. Result, kg Force (N) Independent factor: reinforcement techniques
1 30.41 298.22 Total number of measurements: 60
Number of factor ranking: 3
2 32.76 321.27
Equal group proportions: there are
3 33.58 329.31
4 33.91 332.54 1.1 Statistics for different factor ranking
5 35.01 343.33 Factor
6 34.89 342.15 АmbС АplС Krak
7 34.82 341.47 Mean 366.1 327.9 113.0
8 34.61 339.41
Median 366.625 331.465 115.230
9 34.75 340.78
Standard deviation 6.833 14.590 10.150
10 35.00 343.23
Ni 20 20 20
11 32.84 322.05
12 30.67 300.77 Standard error 1.528 3.262 2.271
13 33.21 325.68 Min 351.96 298.22 95.52
14 34.14 334.79 Max 375.59 343.33 128.07
15 33.78 331.27
1.2 Diagram of observations distributed by groups
16 30.93 303.32
17 31.97 313.52
18 32.69 320.58
19 33.82 331.66
20 34.96 342.84
Таблица 3
Comparison of the forces required for the rupture
of the Achilles tendon suture reinforced with a portion
of the peroneus longus tendon
Experiment No. Result, kg Force (N)
1 37.53 368.04
2 38.30 375.59
3 35.89 351.96
4 36.90 361.86
5 37.61 368.83
6 38.02 372.85
7 36.85 361.37 This "violin diagram" shows a smoothed density
8 37.22 365.00 function of the data distribution in each group. The
9 3827 375.30 borders of the boxes are the first and third quartiles (25th
10 37.12 к 364.02 and 75th percentiles, respectively), the line in the middle
11 35.92 352.25 of the box is the median (50th percentile). Bonferroni
12 36.78 360.69 correction was applied for multiple comparisons. The
13 38.19 374.52 significance level of 0.05 was adopted for the null
14 37.36 366.38 hypothesis when all pairs of treatment methods did not
differ from each other. The significance level of 0.017
15 37.41 366.87
was used for comparisons of each particular pair of
16 36.89 361.77
methods.
17 37.57 368.44
18 38.17 374.32 1.3 Values of critical and confidence probabilities
19 36.93 362.16 alpha alphaM
20 37.65 369.22 0.05 0.017
79 Genij ortopedii. 2022. Vol. 28, no. 1Original Article
2. Checking uniformity of standard deviations 3.2 Diagram of confidence intervals of
2.1 Confidence intervals of standard deviations at mathematical expectations
alpha = 0.017
Factor
АmbС АplС Krak
Standard deviation 6.833 14.590 10.150
Ni 20 20 20
CI_low 4.912 10.490 7.297
CI_upper 10.92 23.32 16.22
2.2 Diagram of confidence intervals of standard
deviations
3.3 Tests of paired comparisons of group means
3.3.1 Parametric Student's t-test
АmbС АplС Krak
Factor
Student's t-test
АmbС 3.4700 23.0000
АplС 0.0076 19.5000
To compare different methods with t-test you need to Krak < 0.001 < 0.001
first make sure that the spread (variance) in each group
Parametric p-value
is approximately the same. Confidence intervals were
employed to verify the assumption. The diagram above Note: the Bonferroni adjusted p-value was used
showed the confidence intervals for standard deviations
overlapping each other and one can assume that the 3.3.2 Permutation test Student's t-test
variances were homogeneous. The Bonferroni adjusted
АmbС АplС
p-value was used. The hypothesis of equal population
means could be tested. АplС 0.006
3. Checking the uniformity of mathematical Krak 0.006 0.006
expectations
Note: the Bonferroni adjusted p-value was used
3.1 Confidence intervals of group means at
alpha = 0.017 The test of paired comparisons was produced using
Factor the usual parametric method and the permutation
АmbС АplС Krak algorithm unrelated to the nature of the data
Mean 366.1 327.9 113.0 distribution. Both tests showed that the null hypothesis
Ni 20 20 20 of the hypothesis of equal population means should be
CI_low 361.8 323.6 108.7 rejected for all pairs of methods.
CI_upper 370.4 332.2 117.3
DISCUSSION
Repair of the torn Achilles tendon using the plantaris to reinforce the injury site with the plantaris tendon
tendon as a reinforcing membrane was first described in Z-shaped manner. Randomized trials comparing
by T.A. Lynn in 1966. In 2004, E.M. Bluman offered primary reinforcement (Lindholm method employed
Genij ortopedii. 2022. Vol. 28, no. 1 80Original Article
lateral flaps for the Achilles reconstruction; Lynn use of autologous tissues on a distal feeding base was
performed reinforcement with a flattened plantar tendon) expected to reduce the rate of infectious complications in
included those performed by S. Aktas and T. Nyyssonen comparison with synthetic materials. The disadvantage
who used end-to-end suture. The cohorts of patients of the plantaris tendon reinforcement is the variable distal
described did not differ in rerupture rate and functional location of the plantararis tendon [17], and harvesting
results. N. Maffulli and co-authors recommended the autograft for reinforcement can be difficult. The
primary reinforcement for long-term neglected and new method of Achilles tendon reinforcement aimed at
repeat ruptures [14, 15]. Among Russian authors increased strength of the Achilles tendon reinforcement
A.A. Panov et al. offered to use a titanium nickelide with predictable harvesting of the autotendon on the
mesh implant for the Achilles tendon reinforcement and distal base.
reported a significant reduction in the recovery time of We intended to identify accurate indications for
working capacity in comparison with primary end-to- the Achilles tendon reinforcement. For example, no
end tendon suture [16]. reinforcement procedure would be practical for open
Publications reporting comparison of the strength traumatic injury to the severed Achilles tendon due to
of tendon sutures are difficult to summarize. The same the normal morphological structure of the tendon at the
suture in the hands of different users can show different injury site [18–21]. And a pronounced dystrophy of the
results and would be dependent more on the condition Achilles tendon in association with corticosteroid use
of the tendon tissue and the strength of the thread. We in the treatment of achillobursitis with dissociated ends
chose to use the VICRIL 1 thread due to its technical of more than 3 cm can be addressed with reinforcement
characteristics (a half-life period of 30 days and of the Achilles tendon suture. Another indication for
complete resorption after 56–70 days) that was optimal reinforcement is long-term Achilles tendinitis that is
for a tendon suture. Our suture application relied on the unresponsive to conservative treatment. Patients are
findings rerported by Russian researchers A.A. Gritsyuk concerned with Achilles tendon pain that increases
and A.P. Sereda who experimentally established the after physical activity [22–25]. Examination reveals a
maximum strength of the Krakow suture [14]. We thickening in the middle third of the Achilles tendon and
analyzed the literature on Achilles tendon reinforcement soreness during palpation in this area. The purpose of
and made efforts to understand the effectiveness of surgical treatment of the pathology is the removal of the
reinforcement of the site using autologous tissues involved parathenone and resection of involved tendon
through the experiments. at the site of aseptic inflammation. Reinforcement
Reinforcement of the Achilles tendon with autologous at the site can be considered according to indications
tissues including the plantaris tendon and a portion of preventing a rupture at the site of Achilles excision.
the peroneus longus tendon on the distal base allowed Clinical details of the reinforcement procedure will be
for a 3-fold increase in the strength of the suture. The presented in the next article.
CONCLUSION
1. Methods offered to reinforce the Achilles 2. There is a greater risk of rerupture with pronounced
tendon with the plantaris tendon and a portion of the dissociated fibers at the ends of the rupture site and
peroneus longus tendon on the distal base facilitated Achilles tendinitis as evidenced by the literature.
the strength increased at the injury site by 195.6 and Reinforcement of the Achilles tendon using techniques
214.4 %, respectively, in comparison with Krakow offered can help to minimize the risks of rerupture that
whipstitches. will be explored in the clinical chapter of the work.
References
1. Mironov S.P., Kotelnikov G.P. editors. Ortopediia: natsionalnoe rukovodstvo [Orthopedics: a national guide]. M., GEOTAR-Media. 2013. 944 p.
(in Russian)
2. Ahmad J., Jones K., Raikin S.M. Treatment of Chronic Achilles Tendon Ruptures with Large Defects. Foot Ankle Spec., 2016, vol. 9, no. 5, pp. 400-
408. DOI: 10.1177/1938640016640895.
3. Suchak A.A., Bostick G.P., Beaupré L.A., Durand D.C., Jomha N.M. The influence of early weight-bearing compared with non-weight-bearing after
surgical repair of the Achilles tendon. J. Bone Joint Surg. Am., 2008, vol. 90, no. 9, pp. 1876-1883. DOI: 10.2106/JBJS.G.01242.
4. Maffulli N., Oliva F., Maffulli G.D., Giai Via A., Gougoulias N. Minimally Invasive Achilles Tendon Stripping for the Management of Tendinopathy
of the Main Body of the Achilles Tendon. J. Foot Ankle Surg., 2017, vol. 56, no. 5, pp. 938-942. DOI: 10.1053/j.jfas.2017.05.019.
5. Brauner T., Pourcelot P., Crevier-Denoix N., Horstmann T., Wearing S.C. Achilles Tendon Load is Progressively Increased with Reductions in
Walking Speed. Med. Sci. Sports Exerc., 2017, vol. 49, no. 10, pp. 2001-2008. DOI:10.1249/MSS.0000000000001322.
6. Chan J.Y., Elliott A.J., Ellis S.J. Reconstruction of Achilles rerupture with peroneus longus tendon transfer. Foot Ankle Int., 2013, vol. 34, no. 6,
pp. 898–903. DOI: 10.1177/1071100712473273.
7. Lohrer H., Nauck T. Results of operative treatment for recalcitrant retrocalcaneal bursitis and midportion Achilles tendinopathy in athletes.
Arch. Orthop. Trauma Surg., 2014, vol. 134, no. 8, pp. 1073-1081. DOI: 10.1007/s00402-014-2030-8.
8. Kearney R.S., Parsons N., Underwood M., Costa M.L. Achilles tendon rupture rehabilitation: a mixed methods investigation of current practice
among orthopaedic surgeons in the United Kingdom. Bone Joint Res., 2015, vol. 4, no. 4, pp. 65-69. DOI: 10.1302/2046-3758.44.2000400.
9. McCormack R., Bovard J. Early functional rehabilitation or cast immobilisation for the postoperative management of acute Achilles tendon rupture?
81 Genij ortopedii. 2022. Vol. 28, no. 1Original Article
A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med., 2015, vol. 49, no. 20, pp. 1329-1335. DOI: 10.1136/
bjsports-2015-094935.
10. Olewnik Ł., Wysiadecki G., Polguj M., Topol M. Anatomic study suggests that the morphology of the plantaris tendon may be related to Achilles
tendonitis. Surg. Radiol. Anat., 2017, vol. 39, no. 1, pp. 69-75. DOI: 10.1007/s00276-016-1682-1.
11. Hansen M.S., Nilsson Helander K., Karlsson J., Barfod K.W. Performance of the Achilles Tendon Total Rupture Score Over Time in a
Large National Database: Development of an Instruction Manual for Accurate Use. Am. J. Sports Med., 2020, vol. 48, no. 6, pp. 1423-1429.
DOI:10.1177/0363546520912222.
12. Fell D., Enocson A., Lapidus L.J. Surgical repair of acute Achilles tendon ruptures: a follow-up of 639 consecutive cases. Eur. J. Orthop. Surg.
Traumatol., 2020, vol. 30, no. 5, pp. 895-899. DOI: 10.1007/s00590-020-02650-1.
13. Kotelnikov G.P., Chernov A.P., Losev I.I., Kim Yu.D., Shitikov D.S., Zimin D.V., Kniazev N.A. Sposob armirovaniia Akhillova sukhozhiliia [The
way of Achilles tendon reinforcement]. Patent RF 2616767, A 61 B 17/00, 2016. (in Russian)
14. Gritsiuk A.A., Sereda A.P. Akhillovo sukhozhilie [Achilles tendon]. M., RAEN, 2010, 313 p. (in Russian)
15. Costa M.L., Achten J., Wagland S., Marian I.R., Maredza M., Schlüssel M.M., Liew A.S., Parsons N.R., Dutton S.J., Kearney R.S., Lamb S.E.,
Ollivere B., Petrou S. Plaster cast versus functional bracing for Achilles tendon rupture: the UKSTAR RCT. Health Technol. Assess., 2020, vol. 24,
no. 8, pp. 1-86. DOI: 10.3310/hta24080.
16. Panov A.A., Podoluzhnyi V.I., Lanshakov V.A., Giunter V.E., Bakhovudinov A.Kh. Issledovanie rezultatov primeneniia sverkhelastichnykh
implantatov iz nikelida titana v lechenii razryvov Akhillova sukhozhiliia [Studying the results of using superelastic titanium nickelide implants in
the treatment of Achilles tendon ruptures]. Sibirskii Meditsinskii Zhurnal, 2009, vol. 24, no. 3-1, pp. 42-44. (in Russian)
17. Winnicki K., Ochała-Kłos A., Rutowicz B., Pękala P.A., Tomaszewski K.A. Functional anatomy, histology and biomechanics of the human Achilles
tendon – A comprehensive review. Ann. Anat., 2020, vol. 229, 151461. DOI: 10.1016/j.aanat.2020.151461.
18. Maffulli N., Via A.G., Oliva F. Chronic Achilles tendon rupture. Open Orthop. J., 2017, vol. 11, pp. 660-669. DOI: 10.2174/1874325001711010660.
19. Yasui Y., Tonogai I., Rosenbaum A.J., Shimozono Y., Kawano H., Kennedy J.G. The risk of Achilles tendon rupture in the patients with Achilles
Tendinopathy: Healthcare Database analisis in the United States. Biomed. Res. Int., 2017, vol. 2017, ID 7021862. DOI: 10.1155/2017/7021862.
20. Yang B., Liu Y., Kan S., Zhang D., Xu H., Liu F., Ning G., Feng S. Outcomes and complications of percutaneous versus open repair of acute
Achilles tendon rupture: A meta-analysis. Int. J. Surg., 2017, vol. 40, pp. 178-186. DOI: 10.1016/j.ijsu.2017.03.021.
21. Alcelik I., Saeed Z.M., Haughton B.A., Shahid R., Alcelik J.C., Brogden C., Budgen A. Achillon versus open surgery in acute Achilles tendon repair.
Foot Ankle Surg., 2018, vol. 24, no. 5, pp. 427-434. DOI: 10.1016/j.fas.2017.04.016.
22. Patel M.S., Kadakia A.R. Minimally Invasive Treatments of Acute Achilles Tendon Ruptures. Foot Ankle Clin., 2019, vol. 24, no. 3, pp. 399-424.
DOI: 10.1016/j.fcl.2019.05.002.
23. Krueger H., David S. The Effectiveness of Open Repair versus Percutaneous Repair for an Acute Achilles Tendon Rupture. J. Sport Rehabil., 2016,
vol. 25, no. 4, pp. 404-410. DOI: 10.1123/jsr.2015-0024.
24. De la Fuente C., Carreño G., Soto M., Marambio H., Henríquez H. Clinical failure after Dresden repair of mid-substance Achilles tendon rupture:
human cadaveric testing. Knee Surg. Sports Traumatol. Arthrosc., 2017, vol. 25, no. 6, pp. 1849-1856. DOI: 10.1007/s00167-016-4182-2.
25. Deng S., Sun Z., Zhang C., Chen G., Li J. Surgical Treatment versus Conservative Management for Acute Achilles Tendon Rupture: A
Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Foot Ankle Surg., 2017, vol. 56, no. 6, pp. 1236-1243. DOI: 10.1053/j.
jfas.2017.05.036.
The article was submitted 16.07.2021; approved after reviewing 16.09.2021; accepted for publication 23.12.2021.
Information about the authors:
1. Gennadii P. Kotelnikov – Doctor of Medical Sciences, Professor, Academician of RAS;
2. Yuriy D. Kim – Candidate of Medical Sciences, drkim@mail.ru;
3. Dmitriy S. Shitikov – Candidate of Medical Sciences;
4. Nikita A. Knyazev – M.D.;
6. Nikita E. Likholatov – M.D.
Genij ortopedii. 2022. Vol. 28, no. 1 82You can also read

















































