Effect of a fortified maize-meal porridge on anemia, micronutrient status, and motor development of infants1-3
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Effect of a fortified maize-meal porridge on anemia, micronutrient
status, and motor development of infants1–3
Mieke Faber, Jane D Kvalsvig, Carl J Lombard, and AJ Spinnler Benadé
ABSTRACT most: 48% of the children aged 6 –11 mo were anemic (3). No
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
Background: Maize-meal porridge is used for infant feeding in national prevalence data for zinc deficiency are available, but
many African countries, including South Africa. A low-cost, finely 46.8% of infants aged 6 –12 mo who participated in a supple-
milled, maize-meal porridge was fortified with -carotene, iron, and mentation study of multiple micronutrients had baseline serum
zinc (100% of recommended dietary allowance), as well as ascorbic zinc concentrations 쏝 10.7 mol/L (4).
acid, copper, selenium, riboflavin, vitamin B-6, vitamin B-12, and Several strategies can be used to improve the micronutrient
vitamin E. status of infants. The administration of high-dose vitamin A
Objective: We assessed whether the fortified porridge could reduce capsules can reduce vitamin A deficiency (5), but the sustain-
anemia and improve the micronutrient status and motor develop- ability of national programs for vitamin A supplementation has
ment of infants.
been questioned (6). Whereas the use of iron-fortified formula
Design: Infants aged 6 –12 mo (n ҃ 361) were randomly assigned to
milk prevents iron deficiency anemia (7), bacterial contamina-
receive either the fortified or unfortified porridge for 6 mo. Primary
tion of bottle feeds is a concern (8). Iron drops and fortified
outcomes were hemoglobin and serum retinol, zinc, and ferritin
concentrations and motor development. Growth was assessed as a
sprinkles are effective in addressing anemia (9), but distribution
secondary outcome. Primary and secondary outcomes were assessed may be a problem.
at baseline and 6 mo. Fortification of plant-based complementary foods can be an
Results: Two hundred ninety-two infants completed the study. The effective strategy for addressing childhood malnutrition in de-
fortified-porridge group had an intervention effect of 9.4 g/L (95% veloping countries (10), provided that it is affordable for most of
CI: 3.6, 15.1 g/L) for serum ferritin and 9 g/L (95% CI: 6, 12 g/L) the population. The use of fortified foods does not guarantee
for hemoglobin concentrations. The proportion of infants with ane- good nutritional status of infants, especially if inadequate
mia decreased from 45% to 17% in the fortified-porridge group, amounts are consumed. For example, a cross-sectional survey in
whereas it remained 쏜40% in the control group. The fortified- an urban area in South Africa where 쏜80% of the infants usually
porridge group achieved on average 15.5 of the 25 motor develop- consumed fortified infant cereals showed that many of these
ment score items, whereas the control group achieved 14.4 items infants were anemic (83%) or deficient in vitamin A (23%) or
(P ҃ 0.007). Serum retinol concentration showed an inconsistent zinc (32%). Dietary data showed that the fortified products were
effect, and no intervention effect was observed for serum zinc con- used in such a diluted form that they could not meet the infants’
centrations. nutrient requirements (11). The intake of inadequate quantities of
Conclusions: This low-cost fortified porridge can potentially have infant cereals was also shown for infants in rural South Africa,
a significant effect in reducing anemia and improving iron status and and it was argued that the high cost of these products prohibited
motor development of infants in poor settings. The formulation an adequate intake (12).
needs some adjustment in terms of zinc fortification. Am J Clin Maize porridge, which is a bulky food low in nutrient density,
Nutr 2005;82:1032–9. is used as complementary food in many African countries (10,
13, 14), including South Africa (15). A newly developed por-
KEY WORDS Fortified porridge, infants, micronutrients,
ridge made with finely milled maize meal that cooks in 3 min
anemia, motor development
1
From the Nutritional Intervention Research Unit (MF and AJSB) and
INTRODUCTION Biostatistics Unit (CJL), Medical Research Council, Tygerberg, South Af-
The critical period for developing childhood malnutrition co- rica, and the Child, Youth, and Family Development, Human Sciences Re-
incides with the introduction of complementary foods, which are search Council, Dalbridge, South Africa (JDK).
2
nutritionally inadequate in many developing countries (1). Iron, Supported by the Thrasher Research Fund and the Community-based
Health Programme of The Valley Trust. Tiger Food Brands Limited donated
zinc, and vitamin A are viewed as problem nutrients because of
the fortified-porridge product.
their low density in plant-based complementary foods (2). In 3
Reprints not available. Address correspondence to M Faber, Nutritional
South Africa, a national survey showed that, of children aged Intervention Research Unit, Medical Research Council, PO Box 19070,
6 –71 mo, 33% were vitamin A deficient (serum retinol concen- Tygerberg 7505, South Africa. E-mail: mieke.faber@mrc.ac.za.
tration 쏝 0.7 mol/L) and 21% were anemic (hemoglobin con- Received March 10, 2005.
centration 쏝 110 g/L). Children aged 6 –23 mo were affected the Accepted for publication July 26, 2005.
1032 Am J Clin Nutr 2005;82:1032–9. Printed in USA. © 2005 American Society for NutritionFORTIFIED MAIZE-MEAL PORRIDGE AND INFANTS 1033
(compared with 20 –30 min for standard maize meal) was forti- Subjects
fied to supply 100% of the recommended dietary allowance Infants were recruited through the community-based health
(RDA) (16) for zinc, iron, and vitamin A for infants aged 6 –12 program. All eligible infants who were aged 6 –12 mo at baseline
mo (Tiger Food Brands Ltd, n’Dabeni, South Africa). At the time were asked to participate, by invitation to their mothers. Infants
of the study, a prototype of the product was commercially avail- were excluded from the study if their parent or legal guardian did
able in 1 of the 9 provinces at a retail price 25–50% of that of other
not sign the consent form, their birth weight was 쏝2500 g, a
baby cereals, depending on the formulation of the baby cereal.
baseline blood sample was not obtained, or the hemoglobin con-
We assessed the effect of this fortified porridge in reducing
centration was 쏝80 g/L. Infants with the latter exclusion crite-
anemia and in improving iron, zinc, and vitamin A status and
rion were referred to the clinic for appropriate treatment.
motor development of the infant.
Sample size calculations were based on group differences of
0.1 mol/L for serum retinol and 4 g/L for serum ferritin. With
SUBJECTS AND METHODS a 5% significance level and a power of 80%, we needed 126
infants in each group. This sample size would allow us to detect
Product group differences of 10 g/L for hemoglobin, 4 mol/L for zinc,
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
The finely milled maize meal was fortified to supply 3 mg a 50% reduction in the prevalence of anemia (40 –20%), and a
-carotene, 11 mg iron (ferrous fumarate), and 3 mg zinc (zinc 1-point group difference for the motor development score. The
sulfate) per 40 g dry product. This supplied 100% of the RDA for required sample size of 126 infants for each treatment group was
iron, zinc, and vitamin A (using a 6:1 conversion factor for adjusted to allow for an expected dropout rate of 30%, which was
-carotene to retinol) for 6 –12-mo-old infants (16). Ascorbic observed in a previous study in the same area. Therefore, 180
acid (sodium ascorbate) was added (56 mg/40 g dry product) to infants per treatment group were recruited. To enable us to recruit
enhance iron absorption. The maize meal was further fortified enough children to meet the sample size requirement, the study
with certain nutrients that are limited in the diet of South African was done in 2 consecutive phases. During the first 6-mo phase,
children, so that it supplied 110 g copper, 10 g selenium, 0.4 from February to August 2002, 144 infants completed the study
mg riboflavin, 0.15 mg vitamin B-6, 0.25 g vitamin B-12, and (fortified-porridge group: n ҃ 71; control group: n ҃ 73). During
2.5 mg vitamin E per 40 g dry product. The vitamin and mineral the second 6-mo phase, September 2002 to March 2003, 145
premix was supplied by Roche Products (Isando, South Africa). infants completed the study (fortified-porridge group: n ҃ 73;
The dry product contained 617 kJ energy/40 g. The cooked prod- control group: n ҃ 72).
uct was analyzed for nutrient content by the South African Bu- Written informed consent was obtained from the mother or the
reau of Standards to ensure that the specified amounts of micro- guardian of each participating infant, after a detailed explanation
nutrient fortification were achieved after preparation. The of the purpose of the study was provided. The Ethics Committee
mothers helped to identify a suitable portion size, which was set of the South African Medical Research Council approved the
at 20 g dry product, mixed with 125 mL milk or water. The study, and permission was obtained from local community lead-
portion size was set at the intake of 6-mo-old infants to ensure ers.
that all participating infants could manage the recommended
amount. The dry product was packed in individual 25-g color-
Design and intervention
coded sachets; the additional 5 g/sachet allowed for spillage and
the mother’s tasting. An intake of 2 sachets/d was recommended, The study was a randomized controlled trial with an interven-
consumed as either 1 or 2 meals. A supply for 1 wk (14 sachets) tion period of 6 mo. Infants were randomly assigned to either the
was packed in color-coded zipper bags. The porridge was sup- fortified-porridge group or the control group. The allocation
plied for 6 consecutive months, free of charge. To avoid diver- schedule was generated in blocks of 8 by the drawing of a sticker
sion of the product to other children in the household, all children from a container that contained 4 yellow and 4 green stickers.
aged 울5 y in the household received 1.5 kg dry product (accord- Infants were randomly assigned in the order that they completed
ing to the treatment group of the participating infant) per month. the baseline survey. Infants in the control group received the
same porridge as did those in the fortified-porridge group, but
Study location, population, and structure without the added micronutrients. Color-coding was used to dis-
The study area was in The Valley of a Thousand Hills in tinguish between the 2 treatment groups. The project leader was
KwaZulu-Natal province, South Africa. This is a rural area of aware of which porridge each of the groups was receiving, be-
low socioeconomic status. The population density is low because cause the fortified porridge had a slight yellow color due to the
the families are scattered over a large mountainous area. The -carotene used as fortificant. The mothers and community
complementary diet of infants in this area supplies an adequate health workers were not aware of which porridge was fortified.
amount of energy but is inadequate in micronutrients (17). The All baseline and postintervention measurements were done in a
product used in this study was not commercially available in the blinded manner.
study area at the time of the study. The study was done through Each infant was issued a color-coded identification card that
the community-based health program of The Valley Trust, a contained the infant’s name and project code and included space
nongovernmental organization, that operates through 12 health for recording the amount of porridge issued and the date of the
posts and has 쏜100 community health workers. A project liaison next appointment; a 10-L color-coded bucket (to collect and store
officer was appointed for the duration of the study and was based the porridge); a porridge bowl with a tight-fitting lid; and a
at The Valley Trust. Five nutrition monitors who were experi- teaspoon. On the day of implementation, the nature and purpose
enced in community-based nutrition interventions acted as co- of the study were reinforced, and the preparation of the porridge
coordinators at the community level. was demonstrated.1034 FABER ET AL
The community health workers visited each infant weekly to A nonfasting blood sample (5 mL) was collected by antecu-
evaluate compliance. The amount of porridge that was left at each bital venipuncture while the child was in a supine position. Blood
infant’s home was observed and recorded. At each visit, the was collected mostly in the mornings, although some samples
community health worker reinforced the importance of daily were taken in the afternoon. Blood (1 mL) was transferred to a
consumption and correct preparation. Problems (if any) and pos- tube containing EDTA for measurement of hemoglobin concen-
sible solutions were discussed. The community health workers trations, and the remainder was transferred to a Gel and Clot
handled questions when possible; the nutrition monitors helped Activator tube (SST II Plus; Becton Dickinson Vacutainer Sys-
with problem cases. tems, Plymouth, United Kingdom). The latter was centrifuged
The mothers collected a supply of porridge monthly from the (750 ҂ g for 10 min at room temperature), and aliquots of serum
health post according to a fixed schedule. For these meetings, the were transferred to a series of Eppendorf tubes that were put in a
mothers were requested to bring the child with the identification cool box containing ice packs. The serum was frozen later the
card to the health post. During these meetings, porridge was same day at Ҁ20 °C. All tubes were free of trace elements to
issued, the child’s growth was recorded, a short questionnaire on avoid contamination with zinc. After completion of the baseline
compliance was completed, and the importance of daily con- and postintervention surveys, the serum samples were trans-
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
sumption and correct preparation was reinforced. The accept- ported to the Nutritional Intervention Research Unit in Cape
ability of the porridge and whether the mothers were giving the Town and stored at Ҁ80 °C until they were assayed.
porridge as required were explored during focus group discus- Hemoglobin concentrations were measured on the day of
sions during the fourth month of the intervention. Seven focus blood collection by using the cyanomethemoglobin method
group discussions were conducted across the 2 phases of the (Drabkin reagent) with the use of a portable photometer (Ames
study; 3 during phase 1 and 4 during phase 2 (8 –10 mothers per Minilab, Product No. 7316; Miles Inc, Elkhart, IN). Blood sam-
focus group). Additional data on the acceptability of the porridge ples of known hemoglobin concentration were used as the ref-
were collected at 6 mo by questionnaire. erence. The values measured for the reference samples were 113
g/L (known value 112 g/L) and 163 g/L (known value 161 g/L).
Measurements Serum ferritin was determined by immunoradiometric assay
The 6-mo intervention period was preceded by a baseline (Ferritin Mab Solid Phase Component System; ICN Pharmaceu-
survey and followed by a postintervention survey. The sociode- ticals, Hawthorne, NY) with the use of an Auto Gamma 500C
mographic data was collected during the baseline assessment counting system (United Technologies, Packard, IL) and an ex-
only; during the baseline and postintervention assessments, a ternal control sample (Ligand 1,2,3; Chiron Diagnostics Ltd,
questionnaire was administered to collect nutritional and health Halstead, United Kingdom). The control sample of high ferritin
data; anthropometric measurements were taken; and a blood concentration (294 g/L) was measured as 293.6 g/L, and the
sample was collected for each infant. control sample of low ferritin concentration (32 g/L) was mea-
Motor development of the infants was assessed by the moth- sured as 36.7 g/L. Serum retinol was determined by using a
ers’ reporting of gross motor milestones, a method known to be slightly modified version of the reversed-phased HPLC method
accurate and sensitive for identifying developmental delays (18, described by Catignani and Bieri (20). Serum zinc concentra-
19). Mothers were asked whether their infant could do each of 25 tions were determined by flame atomic absorption spectropho-
tasks related to motor development; 1 point was scored for each tometry (Pye Unicam SP9; Philips, Cambridge, United King-
item that the mother reported the infant could do. When the scales dom) with a commercial control serum (Seronorm Trace
were being constructed, the tasks listed underwent a series of Elements Serum; SERO AS, Billingstad, Norway) as a quality
piloting procedures before being finalized. The method whereby control. The control sample (4.04 mol/L) was measured as 4.16
development of motor skills of infants aged 6 –12 mo is assessed mol/L. The precautions that were taken to avoid contamination
by parental interview before and after treatment has been used in during blood sampling were similar to those recently recom-
an infant supplementation study of multiple micronutrients that mended by Hotz and Brown (21). The CV for hemoglobin, fer-
was done previously in the same study area, and it was shown that ritin (at high concentrations), and retinol assays was 쏝5%, and
the parents’ ratings correlated with the relevant Bayley II scores that for ferritin (at low concentrations) and zinc assays was
(JD Kvalsvig, written communication, 2004). 5– 6%.
Anthropometric measurements were all taken by the same Because serum ferritin, retinol, and zinc are acute phase reac-
fieldworker while the infant was wearing light clothing. Weight tants, C-reactive protein (CRP) was measured as a marker for
was measured on a calibrated, load cell– operated digital scale infection. CRP was measured by using an immunoturbidimetric
(UC-300 Precision Health Scale; Mascot, Tokyo, Japan) that is method (Technicon method no. SM4-0183G89, Technicon RA-
accurate to 50 g. Recumbent length was measured to the nearest 1000 auto-analyzer; Technicon Instruments, Tarrytown, NY)
0.1 cm with the use of a length board with a fixed wooden with the use of Bayer TESTpoint Serum Protein Controls (Bayer
headboard and a sliding footboard. Birth date was obtained from Diagnostics, Fernwald, Germany).
the child’s clinic card. The anthropometric data and age of the Anemia was defined as hemoglobin concentrations 쏝 110 g/L
child were used to yield 3 measures of nutritional status— (22). Iron deficiency was defined as serum ferritin concentrations
namely, length-for-age, weight-for-age, and weight-for- 쏝10 g/L (23), vitamin A deficiency as serum retinol concen-
length—which were expressed as z scores by using EPI INFO trations 쏝0.7 mol/L (24), and zinc deficiency as serum zinc
2000 software (version 2000; Centers for Disease Control and concentrations 쏝9.9 mol/L (21).
Prevention, Atlanta, GA). Children with length-for-age, weight-
for-age, and weight-for-length z scores 쏝 Ҁ2 SD of the median Statistical analysis
of the reference population were classified as stunted, under- Baseline characteristics were compared between the 2 groups
weight, and wasted, respectively. by using analysis of variance (ANOVA) with treatment group,FORTIFIED MAIZE-MEAL PORRIDGE AND INFANTS 1035
replication phase, and treatment group ҂ replication phase in-
teraction as main factors. Baseline characteristics did not show
any treatment group ҂ replication phase interaction and are,
therefore, given for the 2 treatment groups with the replication
phases combined. The chi-square test was used to compare cat-
egorical variables between groups at baseline. Individual-level
differences between preintervention and postintervention values
(calculated as postintervention value Ҁ baseline value) were
calculated and compared between groups by using ANOVA with
treatment group, replication phase, and treatment group ҂ rep-
lication phase interaction as main factors. Variables that showed
a significant treatment group ҂ replication phase interaction
(P 쏝 0.05) are reported for the 2 replication phases separately,
whereas variables that showed no treatment group ҂ replication
phase interaction (P 욷 0.05) are reported for the 2 replication
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
phases combined. The intervention effects and 95% CIs were
calculated from the pre- to postintervention differences. Data
were tested for equality of variances, and the appropriate value
for significance (P value) was applied. The t test for paired data
was used to compare preintervention and postintervention values
within each group. The intervention effect on the proportion of
infants with concentrations of hemoglobin and serum micronu-
trients below a certain cutoff was ascertained by logistic regres-
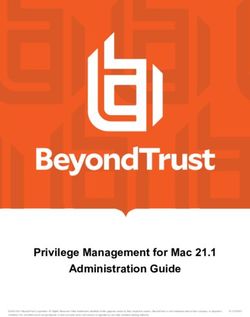
sion analysis with 2-way interaction (time ҂ treatment group). FIGURE 1. Study profile. CRP, C-reactive protein.
When the interaction was significant, the change in proportion
within treatment groups was determined by using MacNemar’s Baseline characteristics for infants who completed the study
test. Serum ferritin concentrations were skewed, and therefore are given in Table 1. No differences were observed between the
they were log transformed before statistical analyses were per- 2 treatment groups in these baseline characteristics or in the other
formed. The level of significance for all tests was P 쏝 0.05. characteristics presented in Table 2 and Table 3, except for
Analyses were performed with the use of SPSS for WINDOWS serum retinol concentrations, which were higher in the control
software (version 10; SPSS Inc, Chicago, IL). group than in the fortified-porridge group during phase 2 (P ҃
The acute phase response was defined as serum CRP concen- 0.02). When infants with baseline CRP concentrations
trations 쏜 10 mg/L (25). Data analysis was repeated on a subset 쏜10 mg/L were excluded, serum retinol concentrations no
of data that excluded infants with CRP 쏜 10 mg/L at baseline or longer differed between the 2 groups during phase 2. At baseline,
postintervention assessment. Because the estimated intervention 83% of the infants were breastfeeding (fortified-porridge group:
effects for concentrations of hemoglobin and of serum ferritin, 87%; control group: 80%), and all were eating solid foods. At the
retinol, and zinc in the above-mentioned subanalysis did not postintervention assessment, 쏜70% of the infants, who were
differ significantly from the estimates of the complete data set, now aged 12–18 mo, were breastfeeding. In a recent study in rural
only the latter are reported. KwaZulu-Natal, the prevalence of breastfeeding was 83% for
infants aged 6 to 쏝12 mo and 64% for children aged 12 to 쏝18
mo (26). It is, therefore, clear that the porridge did not replace
breastfeeding in our study.
RESULTS Concentrations of serum ferritin and hemoglobin showed an
In total, 361 infants were enrolled in the study, of whom 292 intervention effect, and concentrations of serum retinol showed
completed the study. Reasons for dropping out of the study are an intervention effect during phase 1 but not phase 2, but con-
listed in Figure 1. Children who dropped out of the study centrations of serum zinc showed no intervention effect (Table
were older (9.4 앐 2.0 compared with 8.8 앐 1.9 mo; P ҃ 0.034), 2). Logistic regression analysis showed an intervention effect for
had lower length-for-age z scores (Ҁ1.2 앐 1.2 compared with the proportion of infants with hemoglobin concentrations
Ҁ0.84 앐 1.0; P ҃ 0.003), weight-for-age z scores (Ҁ0.17 앐 1.25 쏝110 g/L (P 쏝 0.001). The proportion of infants with hemoglo-
compared with 0.35 앐 1.3; P ҃ 0.003), serum retinol con- bin concentrations 쏝110 g/L decreased from 45% at baseline to
centrations (0.85 앐 0.23 compared with 0.98 앐 0.28 mol/L; 17% at the postintervention assessment in the fortified-porridge
P ҃ 0.0001), and hemoglobin concentrations (105 앐 13 com- group (P 쏝 0.001), whereas it remained 쏜40% in the control
pared with 111 앐 11 g/L; P ҃ 0.001), and had higher serum zinc group (P ҃ 0.735).
concentrations (10.9 앐 2.5 compared with 10.2 앐 2.1 mol/L; The motor development scores at baseline and at the postin-
P ҃ 0.011) at baseline than did children who completed the study. tervention assessment are given in Table 3. The postintervention
A blood sample could not be obtained for 3 children during the estimated mean motor development score of the fortified-
postintervention survey, and they are excluded from the data set. porridge group was approximately 1 point above that of the
The final data set consisted of 289 children (fortified-porridge control group (P ҃ 0.007).
group: n ҃ 144; control group: n ҃ 145). Adequate blood sam- The weight and length at baseline and postintervention assess-
ples to measure all the primary outcomes could not be obtained ments, as well as the z scores, are shown in Table 4. The length-
for all of the children (Figure 1). for-age and weight-for-age z scores decreased during the 6-mo1036 FABER ET AL
TABLE 1 collected at the postintervention assessment showed that approx-
Sociodemographic indicators and baseline characteristics of the infants imately 90% of the mothers across the 2 groups mixed the por-
who completed the study1 ridge with water. Most mothers asserted they followed the in-
Fortified-porridge Control structions of 125 mL liquid/sachet of dry product. When asked
group group whether they thought that the child benefited from participating
(n ҃ 144) (n ҃ 145) in the study, 93% in the fortified-porridge group and 91% in the
control group responded positively; the others were uncertain. In
Boys:girls (n) 73:71 74:71
Access to tap water (%)2 97 93 both groups, nutritional and health benefits were given as reason
Toilet facilities (%)3 92 91 for the positive response.
Electricity in the house (%) 82 75
Household food security (%)
Always enough food to eat 30 31 DISCUSSION
Sometimes not enough food to eat 58 55 This randomized controlled trial showed that the prevalence of
Often not enough food to eat 12 14 anemia decreased and iron status and motor development im-
Age (mo) 8.9 앐 1.94 8.9 앐 2.0
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
proved after infants aged 6 –12 mo consumed 40 g of a low-cost
Breastfeeding (%) 86 80
fortified maize-meal porridge daily for 6 mo. No consistent effect
Stunted (%)5 11 12
Underweight (%)6 3 5
on serum retinol concentrations was observed. The fortified por-
Wasted (%)7 1 — ridge failed to improve serum zinc concentrations.
Serum retinol 쏝 0.7 mol/L (%) 17 19 After the age of 6 mo, an infant must receive nearly all of his
Serum zinc 쏝 9.9 mol/L (%) 43 48 or her iron requirements via complementary foods because of the
Serum ferritin 쏝 10 g/L (%) 58 61 low iron concentration in breast milk. The required amount of
Hemoglobin 쏝 110 g/L (%) 46 42 iron intake is difficult to obtain, and the median iron intake of
Elevated acute phase protein infants aged 6 –12 mo in this community was shown to be 3 mg
CRP 쏜 10 mg/L (%) 15 13 (17), whereas the RDA is 11 mg (16). The fortified porridge
1
No significant difference was observed between the 2 groups supplied 11 mg iron/d, which is in line with a recent recommen-
(ANOVA for continuous variables, chi-square test for categorical variables). dation for fortified complementary foods (27). Although the use
2
From a tap outside the house, a tap inside the house, a public tap, or a of ferrous fumarate in complementary foods has been questioned
neighbor’s tap. (28), our study showed an improvement in concentrations of
3
Facilities were mostly pit latrines. hemoglobin and serum ferritin in infants after they consumed a
4
x 앐 SD (all such values). porridge that was fortified with ferrous fumarate. According to
5
Length-for-age z score below Ҁ2 SD of the median of the reference
Hurrell (29), studies in Bangladesh suggested that young chil-
population.
6
Weight-for-age z score below Ҁ2 SD of the median of the reference
dren may absorb ferrous fumarate only 25% as well as they
population. absorb ferrous sulfate. A disadvantage of the more soluble com-
7
Weight-for-length z score below Ҁ2 SD of the median of the reference pounds such as ferrous sulfate is that they are associated with
population. organoleptic changes of the fortified product. Ferrous fumarate
may cause unwanted color and flavor reactions but to a lesser
extent than does ferrous sulfate (29).
Porridge made with maize meal is an integral part of the diet of
intervention in both groups. No significant difference was ob- many infants in South Africa (15), as was the case in our study,
served between the 2 groups in the change in length and weight in which all but 2 of the infants had consumed porridge made with
or length-for-age, weight-for-age, and weight-for-length z scores maize meal on the day before the baseline interview (M Faber,
during the 6-mo intervention period. unpublished data, 2002). A disadvantage of using maize meal as
Information obtained during the focus group discussions a carrier for fortification is that its high phytate content inhibits
showed that the acceptability of the porridge was high. The the absorption of both iron (30) and zinc (31). Ascorbic acid was
mothers appreciated the smooth texture of the porridge and the added to the finely milled maize meal to overcome the inhibitory
short cooking time required. They acknowledged that infant ce- effect of phytate on iron absorption (32). The high phytate con-
reals are available that do not require any cooking, but they said tent of maize meal probably contributed to the absence of any
that those products are expensive. The fortified porridge had a effect on the concentration of serum zinc. The amount of zinc
slightly yellow color because of the -carotene used as fortificant fortification was too low; a recent recommendation for fortified
and was said to look like either custard or curry, taste like pump- complementary foods to be used in a cereal-based diet was set at
kin, and smell like medicine or some nutritious tablets for babies. 4 –5 mg zinc/d (27). The iron-to-zinc ratio in our study was 11:3.
The unfortified porridge had no similar associations. Data col- A high iron:zinc was shown to inhibit zinc absorption when given
lected by questionnaire showed that the porridge was acceptable as supplements but apparently not when given with food (33).
to 97% of the caregivers in both treatment groups, and the re- The poor sensitivity and specificity of serum zinc concentra-
maining 3% were indifferent. tions to changes in dietary zinc also could have contributed
From the focus group discussions, it was clear that compliance toward the lack of effect on serum zinc concentrations (34).
in terms of consumption and method of preparation was high. There is a diurnal variation, in which serum zinc concentrations
The frequency of consumption of the porridge, reported monthly are lower during the afternoon than in the morning (21). In our
and during the postintervention survey, showed that between study, not all blood samples were taken before 1200, and, unfor-
95% and 99% of the infants across the 2 treatment groups ate the tunately, the time of blood sampling was not recorded for the
recommended amount of porridge every day. Retrospective data individual children. It could be, therefore, that the baseline andFORTIFIED MAIZE-MEAL PORRIDGE AND INFANTS 1037
TABLE 2
Concentrations of hemoglobin and of serum retinol, ferritin, and zinc at baseline and postintervention assessment within-group changes, and intervention
effects in the fortified-porridge and control groups
Baseline Postintervention Change1 Intervention effect2 P3
Serum retinol (mol/L)4
Phase 1 0.14 [0.02, 0.27] 0.021
Fortified-porridge group (n ҃ 68) 1.02 앐 0.275 1.21 앐 0.356 0.19 [0.09, 0.29]
Control group (n ҃ 69) 1.05 앐 0.27 1.10 앐 0.30 0.05 [Ҁ0.03, 0.13]
Phase 27 Ҁ0.03 [Ҁ0.15, 0.08] 0.570
Fortified-porridge group (n ҃ 71) 0.88 앐 0.25 0.80 앐 0.28 Ҁ0.08 [Ҁ0.16, 0.00]
Control group (n ҃ 64) 1.00 앐 0.30 0.95 앐 0.26 Ҁ0.05 [Ҁ0.12, 0.03]
Serum ferritin (g/L) 9.4 [3.6, 15.1] 0.001
Fortified-porridge group (n ҃ 141) 8.7 (3.9, 18.2)8 15.8 (7.3, 26.3)9 6.9 [2.3, 11.5]
Control group (n ҃ 138) 6.8 (2.9, 13.1) 6.5 (2.7, 14.5) Ҁ2.4 [Ҁ5.8, 0.9]
Hemoglobin (g/L) 9 [6, 12] 0.001
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
Fortified-porridge group (n ҃ 144) 111 앐 115 119 앐 119 8 [6, 10]
Control group (n ҃ 142) 111 앐 11 110 앐 14 Ҁ1 [Ҁ7, 1]
Serum zinc (mol/L)10 0.0 [Ҁ0.4, 0.6] 0.832
Fortified-porridge group (n ҃ 140) 10.2 앐 2.0 10.6 앐 2.1 0.4 [0.1, 0.8]
Control group (n ҃ 132) 10.2 앐 2.1 10.6 앐 1.8 0.4 [0.0, 08]
1
Within-group change from baseline to postintervention assessment; x ; 95% CI in brackets.
2
Between-group difference in mean change from baseline to postintervention assessment; x ; 95% CI in brackets.
3
Between-group difference in change from baseline to postintervention assessment by t test.
4
Values for the two replication phases are given separately because a significant treatment group ҂ replication phase interaction was observed for the
change from baseline to postintervention assessment, P ҃ 0.037 (ANOVA).
5
x 앐 SD (all such values).
6,9
Significantly different from baseline within group (t test for paired data): 6P ҃ 0.001, 9P ҃ 0.0001.
7
Baseline values differed between groups, P ҃ 0.02 (ANOVA); when infants with C-reactive protein 쏜10 mg/L were excluded, the groups no longer
differed.
8
Median; 25th and 75th percentiles in parentheses (all such values); serum ferritin concentrations were transformed to natural log-transformed before
analysis.
10
Both groups increased significantly over time, P ҃ 0.001 for main effect of time (ANOVA); there was no significant difference between groups.
postintervention blood samples for the same child were taken at retinol concentrations. Vitamin A supplementation increased se-
different times of the day. rum retinol concentrations, and supplementing the mother with
Serum retinol concentrations responded differently for the 2 capsules of high-dose vitamin A increased the vitamin A content
replication phases: only the first phase showed an intervention of the breast milk (35). We tried to obtain information on vitamin
effect. Pre- to postintervention changes in serum retinol concen- A supplementation from the children’s clinic cards, but these
trations showed a large variability. Measurements of serum ret- data were unreliable. The mothers also could not provide this
inol concentrations were repeated in all children for whom the information because vitamin A supplements had been adminis-
serum retinol concentration changed by 쏜0.35 mol/L; similar tered without informing the mothers what it was that they and
values were obtained, and that finding overruled the possibility their infants were receiving. The lack of reliable information on
that the large within-subject variation was caused by laboratory vitamin A supplementation prevented the drawing of any con-
errors. The introduction of a supplementation program with clusions about the different responses in the 2 replication phases.
high-dose vitamin A before the onset of the baseline survey and Although suboptimal storage and undesirable cooking processes
the variability within the supplementation program probably could have affected the -carotene content of the product, that is
contributed toward the large within-subject variation in serum unlikely because correct storage, giving the required amounts,
TABLE 3
Motor development scores at baseline and postintervention assessment, within-group changes, and intervention effects of the fortified-porridge and control
groups
Baseline Postintervention Change1 Intervention effect2 P3
Motor development score (25 items) 1.1 (0.3, 1.9) 0.007
Fortified-porridge group (n ҃ 128) 7.7 앐 2.94 15.5 앐 4.05 8.1 (7.5, 8.7)
Control group (n ҃ 138) 7.6 앐 2.9 14.4 앐 3.75 7.0 (6.5, 7.5)
1
Within-group change from baseline to postintervention assessment; x ; 95% CI in parentheses.
2
Between-group difference in mean change from baseline to postintervention assessment; x ; 95% CI in parentheses.
3
Between-group difference in change from baseline to postintervention assessment by t test.
4
x 앐 SD (all such values).
5
Significantly different from baseline within groups, P ҃ 0.0001 (t test for paired data).1038 FABER ET AL
TABLE 4
Anthropometric indexes at baseline and postintervention assessment, within-group changes, and intervention effects in the fortified-porridge and control
groups
Baseline Postintervention Change1 Intervention effect2 P3
Length (cm)4 0.1 (Ҁ0.2; 0.2) 0.400
Fortified-porridge group (n ҃ 143) 69.1 앐 3.45 76.1 앐 3.3 7.0 (6.7, 7.3)
Control group (n ҃ 145) 68.5 앐 3.8 75.7 앐 3.8 7.1 (6.9, 7.4)
Weight (cm)4 0 (Ҁ0.2; 0.2) 0.902
Fortified-porridge group (n ҃ 143) 9.0 앐 1.3 10.7 앐 1.4 1.6 (1.4, 1.7)
Control group (n ҃ 145) 9.1 앐 1.4 10.7 앐 1.6 1.6 (1.4, 1.7)
Length-for-age z score Ҁ0.01 (Ҁ0.14; 0.13) 0.962
Fortified-porridge group (n ҃ 143) Ҁ0.79 앐 0.97 Ҁ0.94 앐 1.05 Ҁ0.15 (Ҁ0.25, Ҁ0.04)
Control group (n ҃ 145) Ҁ0.92 앐 1.09 Ҁ1.06 앐 1.15 Ҁ0.14 (Ҁ0.24, Ҁ0.05)
Weight-for-age z score6 0.04 (Ҁ0.15; 0.22) 0.725
Fortified-porridge group (n ҃ 143) 0.28 앐 1.25 0.05 앐 1.25 Ҁ0.23 (Ҁ0.36, Ҁ0.11)
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
Control group (n ҃ 145) 0.37 앐 1.37 0.09 앐 1.37 Ҁ0.27 (Ҁ0.40, Ҁ0.13)
Weight-for-length z score7 0.05 (Ҁ0.19; 0.29) 0.661
Fortified-porridge group (n ҃ 143) 1.12 앐 1.16 0.82 앐 1.15 Ҁ0.30 (Ҁ0.46, Ҁ0.13)
Control group (n ҃ 145) 1.34 앐 1.29 0.99 앐 1.23 Ҁ0.35 (Ҁ0.53, Ҁ0.17)
1
Within-group change from baseline to postintervention assessment; x ; 95% CI in parentheses.
2
Between-group difference in mean change from baseline to postintervention assessment; x ; 95% CI in parentheses.
3
Between-group difference in change from baseline to postintervention assessment by t test.
4,6,7
Both groups increased over time, with no significant difference between groups (time effect, ANOVA); 4P 쏝 0.0001, 6P 쏝 0.05, 7P 쏝 0.001.
5
x 앐 SD (all such values).
and preparing the porridge as required were reinforced during group (37). Prenatal factors, maternal stature (38), poor socio-
each encounter with the mothers during the weekly home visits economic conditions (39), frequent infections (40), and micro-
and monthly sessions at the health posts. Because -carotene was nutrient deficiencies, such as those of zinc, iron, and possibly
used as fortificant, the fortified porridge had a slightly yellow vitamin A (41), can contribute to poor growth. The study was not
color, and the mothers reported a distinct taste and smell. None- powered to measure an intervention effect on growth. For non-
theless, the product was highly acceptable within the study pop- stunted children, a between-group difference of 1 cm for linear
ulation. The consistent encouragement and motivation through- growth could be expected on the basis of a zinc supplementation
out the duration of the study could have contributed toward the trial reported by Umeta et al (42). We would have needed a
mothers’ acceptance of the fortified porridge. Acceptability to sample size of 욷252 children per group. Even if the sample size
the consumer in terms of color, taste, and smell must be deter- were adequate, we most probably would not have seen any effect
mined more extensively before marketing the product nationally on growth because we failed to show a positive biochemical
with -carotene as a fortificant. response to zinc fortification.
The reduction in anemia during the 6-mo intervention period In conclusion, our study showed that a low-cost fortified
is a favorable outcome, because children with low hemoglobin maize-meal porridge can potentially have a significant effect on
concentrations during infancy are at risk of being adversely af- reducing iron deficiency and improving motor development of
fected in terms of developmental outcomes (36). At the postin- infants in a low socioeconomic setting. No conclusions can be
tervention assessment, children in the fortified-porridge group drawn about the effect of the fortified porridge on vitamin A
had on average a 1-point higher motor development score than status because of the implementation of a supplementation pro-
did children in the control group. The advantage of using the gram with high-dose vitamin A in the area just before the onset
parent rating method is that it is quick to administer and allows of the current study. The formulation needs some adjustment in
the parents to participate in a way that is meaningful to them. To terms of zinc fortification.
forestall any tendency by mothers to overrate or underrate their
child’s ability, care was taken to secure parental cooperation in We thank the staffs of Tiger Brands and The Valley Trust; the nutrition
providing accurate responses, and the child was asked to dem- monitors; community health workers and their facilitators; the phlebotomist;
onstrate the ability to perform some of the items. It is unlikely that the team from the Human Sciences Research Council, who conducted the
the mothers’ responses were influenced by the slight color dif- focus group discussions and completed the child development questionnaire;
staff members from the Medical Research Council, who assisted during the
ference between the fortified and unfortified product, because
fieldwork and provided technical support; and the mothers and children who
most of the mothers in both groups were of the opinion that their
participated in the study.
children benefited from the study through the health and nutri- MF was the project leader, contributed toward the study design, organized
tional benefits of the porridge. and managed the data collection, conducted the statistical analysis, inter-
Just 쏜10% of the infants were stunted and 3–5% were under- preted the results, and drafted the manuscript. JDK obtained, analyzed, and
weight at baseline. The decrease in mean length-for-age and interpreted the data on the motor development of the infants and on the
weight-for-age z scores that was observed across the 2 groups acceptability of the porridge as determined by focus group discussions. CJL
during the 6-mo intervention period is commonly seen in this age guided the study design, the statistical analysis, and the interpretation ofFORTIFIED MAIZE-MEAL PORRIDGE AND INFANTS 1039
results. AJSB conceptualized the study and participated in the study design ␣-tocopherol in serum or plasma by liquid chromatography. Clin Chem
and interpretation of the results. All authors revised the manuscript and 1983;29:708 –12.
approved the final version. None of the authors had any personal or financial 21. Hotz C, Brown KH. International Zinc Nutrition Consultative Group
conflict of interest. (IZiNCG) technical document no. 1: assessment of the risk of zinc
deficiency in populations and options for its control. Food Nutr Bull
2004;25:S94 –204.
22. Stoltzfus RJ, Dreyfuss ML. Guidelines for the use of iron supplements to
REFERENCES prevent and treat iron deficiency anemia. Washington, DC: International
1. Gibson RS, Ferguson EL, Lehrfeld J. Complementary foods for infant Nutritional Anemia Consultative Group, 1998.
feeding in developing countries: their nutrient adequacy and improve- 23. Pilch SM, Senti FR. Assessment of the iron nutritional status of the US
ment. Eur J Clin Nutr 1998;52:764 –70. population based on data collected in the second National Health and
2. Brown K, Dewey K, Allen L. Complementary feeding of young children Nutrition examination Survey, 1976-1980.Bethesda, MD: Life Services
in developing countries: a review of current scientific knowledge. Ge- Research Office, Federation of the American Societies for Experimental
neva, Switzerland: World Health Organization, 1998. Biology, 1980.
3. South African Vitamin A Consultative Group (SAVACG). Children 24. WHO/NUT/96.10. Indicators for assessing vitamin A deficiency and
aged 6 to 71 months in South Africa, 1994: their anthropometric, vitamin their application in monitoring and evaluating intervention programmes.
A, iron and immunisation coverage status. Johannesburg, South Africa: Geneva, Switzerland: World Health Organization, 1996.
25. Paracha PI, Jamil A, Northrop-Clewes CA, Thurnham DI. Interpretation
Downloaded from https://academic.oup.com/ajcn/article/82/5/1032/4607463 by guest on 03 January 2021
South African Vitamin A Consultative Group, 1995.
4. Smuts CM, Dhansay MA, Faber M, et al. Efficacy of multiple micronu- of vitamin A status in apparently healthy Pakistani children by using
trient supplementation for improving anemia, micronutrient status, and markers of subclinical infection. Am J Clin Nutr 2000;72:1164 –9.
growth in South African infants. J Nutr 2005;135:653–9S. 26. Smuts CM, Faber M, Schoeman SE, et al. Integrated Nutrition Pro-
gramme: baseline survey. KwaZulu-Natal and Eastern Cape. Part 1.
5. Mason J, Deitchler M, Mathys E, Winichagoon P, Tuazon MA. Lessons
Community based survey. Tygerberg, South Africa: Medical Research
from successful micronutrient programs. Part III: program impact. Food
Council, 2004.
Nutr Bull 2004;25:53–78.
27. Lutter CK, Dewey KG. Proposed nutrient composition for fortified com-
6. Deitchler M, Mathys E, Mason J, Winichagoon P, Tuazon MA. Lessons
plementary foods. J Nutr 2003;133:3011S–20S.
from successful micronutrient programs. Part II: program implementa-
28. Lynch SR, Stoltzfus RJ. Iron and ascorbic acid: proposed fortification
tion. Food Nutr Bull 2004;25:30 –52.
levels and recommended iron compounds. J Nutr 2003;133:2978S– 84S.
7. Williams J, Wolff A, Daly A, MacDonald A, Aukett A, Booth IW. Iron
29. Hurrell RF. Fortification: overcoming technical and practical barriers. J
supplemented formula milk related to reduction in psychomotor decline
Nutr 2002;132:806S–12S.
in infants from inner city areas: randomised study. BMJ 1999;318:
30. Davidson L. Iron bioavailability from weaning foods: the effect of phytic
693– 8.
acid. In: Micronutrient interactions. Impact on child health and nutrition.
8. Bergström E. Bacterial contamination and nutrition concentration of Washington, DC: International Life Sciences Institute, 1996:21–7.
infant milk in South Africa: a sub-study of the national PMTCT study. 31. Gibson RS, Ferguson EL. Food processing methods for improving the
Uppsala, Sweden: Uppsala University, 2003. zinc content and bioavailability of home-based and commercially avail-
9. Zlotkin S, Arthur P, Antwi KY, Yeung G. Treatment of anemia with able complementary foods. In: Micronutrient interactions. Impact on
microencapsulated ferrous fumarate plus ascorbic acid supplied as sprin- child health and nutrition. Washington, DC: International Life Sciences
kles to complementary (weaning) foods. Am J Clin Nutr 2001;74:791–5. Institute, 1996:50 –7.
10. Lartey A, Manu A, Brown KH, Peerson JM, Dewey KG. A randomized, 32. Siegenberg D, Baynes RD, Bothwell TH, et al. Ascorbic acid prevents
community-based trial of the effects of improved, centrally processed the dose-dependent inhibitory effects of polyphenols and phytates on
complementary foods on growth and micro-nutrient status of Ghanian nonheme-iron absorption. Am J Clin Nutr 1991;53:537– 41.
infants from 6 to 12 mo of age. Am J Clin Nutr 1999;70:391– 404. 33. Lönnerdal B. Iron-zinc-copper interactions. In: Micronutrient interac-
11. Oelofse A, van Raaij JMA, Benadé AJS, Dhansay MA, Tolboom JJM, tions. Impact on child health and nutrition. Washington, DC: Interna-
Hautvast JGAL. Disadvantaged black and coloured infants in two urban tional Life Sciences Institute, 1996:3–10.
communities in the Western Cape, South Africa differ in micronutrient 34. Brown KH. Effect of infections on plasma zinc concentration and im-
status. Public Health Nutr 2002;5:289 –94. plications for zinc status assessment in low-income countries. Am J Clin
12. Faber M, Benadé AJS. Perceptions of infant cereals and dietary intakes Nutr 1998;68(suppl):425S–9S.
of children aged 4 –24 months in a rural South African community. Int J 35. Bahl R, Bhandari N, Wahed MA, Kumar GT, Bhan MK and the WHO/
Food Sci Nutr 2001;52:359 – 65. CHD Immunization-Linked Vitamin A Group. Vitamin A supplemen-
13. Bentley ME, Dickin KL, Mebrahtu S, et al. Development of a nutrition- tation of women postpartum and of their infants at immunization alters
ally adequate and culturally appropriate weaning food in Kwara State, breast milk retinol and infant vitamin A status. J Nutr 2002;132:3243– 8.
Nigeria: an interdisciplinary approach. Soc Sci Med 1991;33:1103–11. 36. Sheriff A, Emond A, Bell JC, Golding J, and the ALSPAC Study Team.
14. Huffman SL, Oniang’o R, Quinn V. Improving young child feeding with Should infants be screened for anemia? A prospective study investigat-
processed complementary cereals and behavioural change in urban Ken- ing the relation between haemoglobin at 8, 12, and 18 months and
ya. Food Nutr Bull 2000;21:75– 81. development at 18 months. Arch Dis Child 2001;84:480 –5.
15. Faber M, Oelofse A, Kriek JA, Benadé AJS. Breastfeeding and comple- 37. Allen LH. Nutritional influences on linear growth: a general review. Eur
mentary feeding practices in a low socio-economic urban and a low J Clin Nutr 1994;48:S75– 89.
socio-economic rural area. S Afr J Food Sci Nutr 1997;9:43–51. 38. Dewey KG. Cross-cultural patterns of growth and nutritional status of
16. Food and Nutrition Board, Institute of Medicine. Dietary Reference breast-fed infants. Am J Clin Nutr 1998;67:10 –7.
Intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, 39. Gorstein J, Sullivan K, Yip R, et al. Issues in the assessment of nutritional
iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and status using anthropometry. Bull World Health Organ 1994;72:273– 83.
zinc. Washington, DC: National Academy Press, 2001. 40. Guerrant RL, Schorling JB, McAuliffe JF, de Souza MA. Diarrhea as a
17. Faber M. Complementary foods consumed by 6 –12-month-old rural cause and an effect of malnutrition: diarrhea prevents catch-up growth
infants in South Africa are inadequate in micronutrients. Public Health and malnutrition increases diarrhea frequency and duration. Am J Trop
Nutr 2005;8:373– 81. Med Hyg 1992;47:28 –35.
18. Ireton H, Glascoe FP. Assessing children’s development using parents’ 41. WHO/CHS/CAH/99.3. A critical link. Interventions for physical growth
reports. The Child Development Inventory. Clin Pediatr (Phila) 1995; and psychological development. Geneva, Switzerland: World Health
34:248 –55. Organization, 1999.
19. Knobloch H, Stevens F, Malone A, Ellison P, Risemberg H. The validity 42. Umeta M, West CE, Haidar J, Deurenberg P, Hautvast JGAJ. Zinc
of parental reporting of infant development. Pediatrics 1979;63:872– 8. supplementation and stunted infants in Ethiopia: a randomised con-
20. Catignani GL, Bieri JG. Simultaneous determination of retinol and trolled trial. Lancet 2000;355:2021– 6.You can also read