Domestic Violence Fatality Review Commission 2018 Report
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

State of Vermont
Domestic
Violence
Fatality
Review
Commission
2018 Report
Vermont Attorney General’s Office
http://www.ago.vermont.govTABLE OF CONTENTS
Part One: Case Review Findings and Recommendations............................................... 5
Part Two: Domestic Violence 2017 Homicide Data ....................................................... 16
Historical Data (1994 - 2017) ........................................................................................ 23
Part Four: Updates ........................................................................................................ 27
Domestic Violence & Suicide Prevention Resources .................................................... 29
This project was supported by grant number: 2014-WF-AX-0043, awarded by the
Office on Violence Against Women, Office of Justice Programs, U.S. Department
of Justice.
Points of view in this document are those of the author(s) and do not necessarily
represent the official position or policies of the U.S. Department of Justice.
iDEDICATION
The Vermont Domestic Violence Fatality Review Commission dedicates this year’s
report to the families that share their stories with us. We admire your courage and hope
to honor the memory of your loved one as we work to improve our system responses to
domestic violence.
INTRODUCTION
On May 2, 2002, then-Governor Howard Dean signed into law H.728, which created
Vermont’s Domestic Violence Fatality Review Commission (“Commission”). The
purpose of the Commission is to collect data and conduct in-depth reviews of domestic
violence-related fatalities in Vermont with the goal of making policy recommendations to
prevent future tragedies. There are now over 40 states that have active multi-
disciplinary domestic violence fatality review teams across the country. The purpose of
these review groups is to examine data and information so we can better understand
why and how the fatalities occurred and what can be done to prevent future deaths.
Pursuant to 15 V.S.A. § 1140, the Commission operates under the auspices of the
Office of Attorney General in consultation with the Vermont Council on Domestic
Violence (“Council”).
Under 15 V.S.A. § 1140, the purposes of the Commission are to:
• examine the trends and patterns of domestic violence-related fatalities in
Vermont;
• identify barriers to safety, the strengths and weaknesses in communities related
to domestic violence, and systemic responses to domestic violence;
• educate the public, service providers and policymakers about domestic violence
fatalities and strategies for intervention and prevention; and
• recommend policies, practices and services that will encourage collaboration and
reduce fatalities due to domestic violence.
This is the sixteenth Commission report. This report includes data regarding fatalities
for 2017 and updates the Commission’s statistical information from 1994-2017. In
2017-18, the Commission completed two in-depth case reviews and recommendations
from those reviews are discussed in this report. Finally, the report provides relevant
updates on the Commission’s previous recommendations.
The Commission asks all Vermonters to review this report and provide us with
comments and suggestions as we continue to study the trends and patterns of domestic
violence- related fatalities.
1EXECUTIVE SUMMARY OF COMMISSION DATA
The Commission data indicates:
• Between 1994 and 2017, 50% of all Vermont homicides were domestic violence-
related.
o 55% of Vermont’s adult domestic violence-related homicides were committed
with firearms.
o 77% of the suicides associated with the homicides (i.e. murder/suicides) were
committed with firearms.
o 80% of Vermont’s domestic violence-related fatalities were committed by
males.
o 53% of the decedents in domestic violence-related fatalities were female.
• Of the seventeen (17) homicides in Vermont in 2017, eleven (11) (65%) were
domestic violence-related.
o Of the eleven domestic violence-related homicides, three involved the use of
a firearm.
o Two responsible parties died by suicide, one by firearm and one by intentional
overdose.
o Of the eleven domestic violence-related homicides, six were intimate
partners. Of those, three were current partners and three were recently
separated. One had a relief from abuse order in effect at the time.
o Of the eleven domestic violence-related homicides, ten occurred in the home.
SUMMARY OF COMMISSION’S ACTIVITIES IN 2017
In 2017, the Commission issued its Annual Report. The report contained new statistical
information and updated charts. It did not include recommendations. This year’s report
includes recommendations from both 2016 and 2017. As required by 15 V.S.A. § 1140,
the Commission distributed its report to the General Assembly, the Governor, the Chief
Justice of the Vermont Supreme Court, and the Vermont Council on Domestic Violence.
A List of our commissioners is available on the Vermont Attorney General’s
website and can be found here: http://ago.vermont.gov/wp-
content/uploads/2018/05/2017-DVFRC-MEMBERS.pdf. We welcomed new members:
Tracy Shriver who replaced Deb Celis as the State’s Attorneys representative, Captain
Dan Trudeau and Victim Services Director Kate Brayton from the Vermont State Police,
2and Melissa Deas who stepped in to fill what had been an empty spot for the Vermont
Coalition of Domestic Violence Accountability Programs when funding was eliminated
for the Coordinator position. We also gained a physician representative appointed by
the governor, Dr. Mariah McNamara who replaced Dr. Gail Yanowich.
Over the course of 2018, long-term member Captain JP Sinclair from the Vermont State
Police retired, and Sarah Robinson from the Vermont Network Against Domestic
Violence and Sexual Assault stepped down and Auburn Watersong, Policy Director
from the Network stepped in as their new representative. JP and Sarah have been
amazing, insightful and dedicated members of our Commission and we wish to thank
them for their many years of service.
For the first time, the Commission joined with the Vermont Child Fatality Review team to
conduct a joint review. We wish to thank the specially appointed members for their
willingness to participate in this process on top of their regular duties. Those specially
appointed members are: Elizabeth Bundock, MD from the Medical Examiner’s Office,
Nancy Miller from the Department For Children and Families (“DCF”), Trevor Whipple,
Chief, South Burlington Police Department, and Debby Haskins from the Center of
Health and Learning.
During 2017 the Commission met bi-monthly, and the Chair of the Commission and the
Coordinator of the Vermont Council of Domestic Violence met monthly to work on
implementing past recommendations.
Pursuant to 15 V.S.A. § 1140, the purpose of the Commission includes identifying
strengths and weaknesses in systemic responses to domestic violence and making
recommendations that will encourage collaboration, intervention, and prevention. Below
please find relevant data regarding the completed case reviews and the Commission’s
findings regarding strengths in the community and recommendations to improve the
response to domestic violence.
SUMMARY OF THE 2017 CASE REVIEW PROCESS
While the Commission reviews and discusses all domestic violence-related homicides
every year, we also select one or two cases to review in depth from previous years.
The case review process includes creating a timeline for the case, identifying lethality
factors, reviewing all available documents, inviting witnesses to testify, taking testimony
from witnesses before the Commission, and discussing at length what we learned from
our review. The proceedings and records of the Commission are confidential to protect
the privacy of surviving family members.
It is always our intent to learn as much as possible from direct sources in every case.
We attempt to speak directly with police officers and others that were part of the
systemic response, as well as family members of the victim and the responsible party.
Thank you to all the family members, mental health professionals, advocates and
attorneys who shared their experience and perspective with us this year. We hope that
3we can use this report and our recommendations as a starting point to improve the
systemic response and make further strides in our efforts to prevent domestic violence
fatalities.
2017 CASE REVIEW INFORMATION
In 2016/7 the Commission reviewed two cases. Both cases involved long term
relationships in which the parties had children together. Both involved females who
were living separately from the responsible party and had custody of their children. In
both cases, the parties had recently separated and the responsible party was male.
Both females had close, supportive families who did everything they could to help once
they learned about the responsible parties’ abusive behavior. In both cases, the
responsible party took his own life after committing the murder.
In one case, the partners had been married for many years. The female sought police
assistance, but there was no arrest. She obtained a relief from abuse order, but the
judge granted the order only as to her, not the child. The decedent is a biological child
of both. In the other case, the parties had lived together and had a young child in
common. The decedent is the female ex-partner of the responsible party. The female
did not make a police report, but was considering applying for a relief from abuse order
when she was killed. She was concerned that her ex-partner was suicidal.
The following risk factors were identified by the Commission in these cases:
1. serious physical violence currently and in the past;
2. prior threats to kill in one case and prior threats with a firearm in the other;
3. recent separation; and
4. access to weapons.
STRENGTHS IN THE COMMUNITY
As noted above, part of the Commission’s statutory role is to identify strengths in
addition to barriers in responses to domestic violence cases. During the review, the
Commission identified the following positive strengths:
• Both females had very strong social support from her family.
• Both females were able to find resources in the community, in one case through
medical providers and in the other through the court process.
• Local community agencies and the family services division of DCF provided
exceptional support to one of the families when they became the primary
caretaker for their deceased daughter’s infant child.
4PART ONE: CASE REVIEW FINDINGS AND RECOMMENDATIONS
The Commission makes the following findings and recommendations related to our
review. We identify relevant professions and agencies that may be able to incorporate
our recommendations in their practices and protocols. We encourage these groups to
give careful consideration to these recommendations and we welcome the opportunity
to discuss our recommendations further.
In no way does the Commission intend to imply that any agency or policy is responsible
directly or indirectly for any death. The goal of the Commission in making these
recommendations is to increase the safety of all Vermonters. The findings and
recommendations are not prioritized and are of equal importance.
A. Child Custody and Visitation in Domestic Violence Cases
1. Family Court and Probate Court
One of the central issues in both case reviews is the need to properly address the
needs of children in situations involving domestic violence. In one case, the child was
quite young when her mother was murdered. Her family obtained guardianship through
probate court. Luckily, the family received strong support from a community social
worker and a DCF Family Services investigator who worked together to ensure that the
child and the child’s caregivers, who had just lost their daughter and were dealing with
their own trauma, got the support they needed. The Commission wishes to commend
them both for truly outstanding dedication and support.
However, the Commission is concerned that greater clarity is needed to ensure that
children of a parent/guardian who has been murdered by the other parent/guardian may
be seen as children in need of care and supervision (CHINS) by the court system.
Currently there are two paths forward in these cases: guardianship through probate
court or custody through family court. As mandated reporters, law enforcement have
twenty-four hours to notify the Family Services Division of DCF. However, the
Commission believes notification should take place as soon as possible in cases of a
domestic violence-related homicide or near homicide. Even if there are appropriate
family members to care for the child, DCF will conduct the necessary checks to ensure
that the child is in a safe environment and safety plan with the caregivers. In one case
review, the whereabouts of the responsible party was unknown. While police were
diligently investigating and most likely would have arrested him immediately if he
showed up demanding his child, this possibility must always be addressed once the
children are no longer in the presence of law enforcement.
In some cases, guardianship proceedings through probate court and custody through
family court may both be options. If the caregiver can provide a stable and safe home
for the child, probate court may be an appropriate avenue. The downside to this path is
that currently probate court lacks the ability to do any independent investigation.
Probate court lacks access to criminal histories, police reports, DCF reports, and filings
5in other courts that might prove useful if the guardianship is ever contested, for
example, if family members of the responsible party choose to get involved. Probate
court also does not have the capacity to address emergency situations and families may
experience additional stress from the period of time spent waiting for the court’s
decision. Guardianship through probate court also lacks permanency for the child. If
the guardian decides that the arrangement is no longer working, the guardian can ask
probate court to allow the guardian to withdraw, and the child may suffer from the lack
of a stable home.
Family court may also be the best option. The caregiver may experience stress from
having less control over the child’s placement, however, trained DCF workers can
assure families that placement with a caregiver-relative who the child knows well and
who can offer a stable and safe home is the preferable course of action. Moreover, this
path allows the caregiver to pursue adoption which provides permanency for the child.
Should the responsible party’s family assert an interest in visitation/custody, a skilled
DCF Family Services worker can act as a buffer in the arrangements. DCF is also able
to help safety plan, help with financial concerns, counselling referrals and offers
expertise in dealing with trauma. Family court also has access to court records and
other information that probate court currently does not.
There seems to be confusion within the systems between the family court process and
the probate court. The child welfare system response directs cases through a CHINS
process because there is a foster care reimbursement and the opportunity for an
adoption subsidy to meet any special needs. These cases are high risk from a
permanency point of view and have a high likelihood of adoption. There is also an
ongoing need for decisionmakers from both systems to collaborate on how both
processes can work together to improve outcomes for children and their caregivers.
2. Supervised Visitation
The Commission looked closely at the process for supervised visitation when a
supervised visitation center in not involved. The victim in the reviewed case sought a
relief from abuse order on behalf of her and her children. The court granted a
temporary order that permitted defendant to call plaintiff’s home to speak with the
children and indicated that parent-child contact/custody issues would be addressed at
the final hearing. The final hearing was continued for approximately a month, and while
this was pending, a family member was asked to supervise visitation. The court set up
a custody sharing arrangement with one child and the older child had visitation at the
child’s discretion. That older child elected not to have any visitation. The younger child
was not given any discretion in whether to have visitation with defendant. The court
never asked the family member who supervised visitation about the status. Despite the
allegations of abuse toward the younger child, the final order was granted with respect
to the mother only. The final order permitted contact with the plaintiff by email to
arrange parent/child contact and indicated the exchange should take place “at school or
other mutually agreeable place.” At that point, visitation with the children became
unsupervised.
6Although the court and the parties agreed on a family member to supervise visitation
before the final hearing, the family member received no information about the role or the
court’s expectations. While that family member was amenable to the arrangement, the
lack of guidance was difficult. The lack of an opportunity to report to the court about the
status of the visits made it difficult to express any concerns.
This was not an isolated occurrence, family members are often tapped to be
supervisors and they are given no formal guidance or support in that role. In cases
involving domestic violence, the commission does not believe it is best practice to
appoint a family member to supervise visitation, but understands that often there is no
other choice available. While Vermont has excellent supervised visitation centers in
some communities, they are not an option in some cases. Courts often have no other
option than to appoint a family member or friend and face a difficult task in creating
orders that provide appropriate supervision and safety in those circumstances.
The Commission recommends that the judiciary work with child advocacy specialists
and domestic violence experts to develop basic guidelines for supervised visitation in
domestic violence cases. Even if a supervised visitation center is not involved, the
Coalition for Supervised Visitation Centers in Vermont provides valuable resources and
guidelines. There are also resources available from the National Council of Family and
Juvenile Court Judges, for example http://www.ncjfcj.org/resource-
library/publications/judicial-guide-child-safety-custody-cases
We recommend that the judiciary, in partnership with these resources, develop
guidelines to create a case-specific contract in each proceeding that all parties and the
supervisor must agree to before supervision begins. The contract should outline the
court’s expectations, be very specific, and include periodic compliance review. Before
any decision is made to alter or discontinue supervision, the court should solicit
feedback from the supervisor and the child if the child is of an appropriate age to do so.
3. School Notification Process in Abuse Prevention Orders
The Commission discussed the process when the plaintiff chooses to notify his/her
child’s school if the child is included in the abuse prevention order or if child custody
arrangements are taking place at the school as part of the order. When the victim
chooses to notify the school, the Commission wondered if there was a safe way for the
judiciary to collect this information and assist the plaintiff with notification by providing a
copy to the school. We identified many reasons why this might be difficult. In some
cases the plaintiff may wish to keep the school that the child attends confidential from
the defendant for safety reasons, and the location of the school should not be in the
order. We also realize that asking the court to provide this service is adding to the
workload of staff who are already stretched thin. We also identified privacy concerns
that might occur if the information, for instance, was emailed to the school. A
notification process, if not handled well, could take agency away from the plaintiff and
7cause greater harm. However, we do think that a notification process that supports the
plaintiff and the child, when it is requested as part of the order, would be helpful.
Past practice has been to require the plaintiff to think about and take full responsibility
for notifying the school about the order and providing a copy. Any changes to the order
require the plaintiff to repeat the process. Often this does not happen. In some cases,
the plaintiff is unsure who to contact, overwhelmed with other economic or criminal
justice issues as a result of the abuse, or does not have a copy of the required
documentation. The Commission recommends that the judiciary work with advocates to
create a protocol to support the plaintiff when she/he wishes to provide notification to a
school. Advocates should advise plaintiffs of the protocol and be familiar with the
resources that school guidance counsellors can provide to support the student. The
school guidance counsellor can be a great resource for a child who is experiencing
trauma associated with domestic violence in the home and needs support.
Communities can work together to increase the opportunity to provide confidential
support for a child who may not have any other outlet to discuss the impact that the
order is having on him or her.
Law Enforcement Recommendations
• Law enforcement provide notification to DCF Family Services division as soon as
possible in homicides or near homicides involving intimate partner domestic
violence when the victim and/or perpetrator have custody of their children and
there is no other uninvolved parent/guardian.
• Law enforcement should develop a protocol to notify family court if the supervisor
reports a violation of the court’s order regarding supervised visitation in domestic
violence cases even in cases where criminal charges are not filed.
• Law enforcement agencies work with family court to support plaintiffs who
request assistance with notifying schools about relief from abuse orders,
including creating a process to notify the court promptly of any violation of child
visitation/custody orders in domestic violence cases.
DCF Recommendation
Work with probate and family courts to develop informational brochures for all
caregivers to explain guardianship and custody and what services and support
may be available to families.
Judiciary Recommendations
• The judiciary develop a method to share information with probate court about
other pending cases and criminal and family court history.
8• Family and Probate courts distribute informational brochures prepared by DCF-
Family Services to all caregivers when a guardianship or custody order is filed
and provide a link to this information online on their website.
• The judiciary work with child advocacy specialists to create guidelines for
supervised visitation in domestic violence cases when a supervised visitation
center is not involved.
• The judiciary develop a template form that can be used to create a specific and
detailed contract of expectations that will be signed by the parties and the
appointed supervisor in domestic violence cases before visitation begins.
• The judiciary receive education on when the use of family members to provide
supervised visitation may not be appropriate in domestic violence cases.
• The judiciary should develop a system for compliance review of supervised
visitation in domestic violence cases. The system should solicit feedback from
supervisors and age-appropriate children when changing or eliminating
supervised visitation even in cases in which the parties are stipulating to the new
terms.
• The judiciary work with domestic violence advocates, schools, and law
enforcement to develop a protocol and process to support plaintiffs who wish to
have a school notified about a relief from abuse order.
B. Improving Vermont’s Response to the Intersection of Domestic Violence and
Mental Health
While there is some overlap in mental health and domestic abuse, the overlap is not
complete. The Commission recommends that Vermont craft a consistent statewide
message to improve the connections between service providers and reduce stigma.
The intersection between domestic violence and mental health must be examined at the
leadership level. As a state, we have yet to intently focus on this intersection. The
Commission recommends that the Agency of Human Services (AHS) convene a
statewide work group of leaders including representatives from Department of Mental
Health (DMH, Department of Health, Department for Children and Families, law
enforcement, Vermont Council on Domestic Violence and the Vermont Network to begin
this important work. We hope this leadership group will consider an assessment of
existing curriculum in undergraduate and graduate programs for social workers, health
care professionals and mental health professionals regarding how the dynamics of
domestic violence are incorporated into their educational programs.
Over the past year, the Commission looked closely at what community resources are
currently available to families who have a loved one who is perpetrating domestic
violence. Families are often in the best position to recognize when a loved one who is
9perpetrating domestic violence is considering harm. In one case, the Commission
noted that the responsible party’s parents were aware that he had threatened the victim
with a firearm. They had firearms in their home and were aware that the responsible
party was in possession of firearms. The victim was concerned that the responsible
party was suicidal. In the other case, the responsible party had taken several steps to
get his affairs in order and had contacted family members for assistance with this.
The Commission was unable to verify if either family recognized warning signs and tried
to get help. However, even when families try to get help, the process can be difficult.
Resources vary from county to county. Families may hesitate to contact professionals
because they fear criminal prosecution of their loved one. They may not realize that a
perpetrator of domestic violence who is considering harming himself may also pose a
significant risk of harm to his family. In our 2016 report, we discussed the prevalence of
suicide in Vermont and the increased risk of suicide for persons who have experienced
domestic violence.
The mental health subcommittee of the Commission spent time learning about what
resources are currently available in Vermont. Vermont has a mental health crisis line.
The caller defines the crisis. First Call, Chittenden County’s mobile crisis unit, uses a
continuum of care model that starts with the lowest level of intervention, such as
community support and referrals.
About half of the calls they receive are made on behalf of another person. First Call can
offer community support and safety planning to a third party caller. If a person in need is
reluctant or unwilling to engage in mental health services, mental health clinicians are
able to initiate a “cold call” and reach out to the person. If warranted, the clinician may
come to the home and try to do an assessment. The clinician may only enter the home
if invited in by a third party caller who has authority to grant access. Screening would
include questions related to concerns about violence, suicide and firearm access. If the
person being screened doesn’t show up for an appointment or stops answering his/her
phone, the clinician can call the police to do a welfare check. There is a program
available to family members of a child up to age 24 even if the child is not interested in
treatment. http://centerpointservices.org/our-services/family-support
Clinicians for First Call mobile crisis unit carry gun locks. Locks are available from
community mental health clinics and at other locations, like town clerks’ offices and
some libraries. Some police departments have the capacity to store firearms for a
limited period of time, but federally licensed firearm dealers are in a better position to
store firearms long term. While gun or trigger locks may provide some level of
deterrence, removal of the firearm entirely is a better alternative. The Commission
recommends that all mental health and health care providers are familiar with the
process for storing firearms in their community and the legal methods for removing
firearms in dangerous situations such as relief from abuse and extreme risk protection
orders.
10We reviewed a standard crisis assessment form. The subcommittee noted that there
are no questions that ask directly about domestic violence concerns. In the risk
assessment, there is a question about homicidal ideation. The form asks for legal
history and relevant family history and if law enforcement was involved in the situation.
The last section on “issues that apply” asks about homicide, family conflict, concerns
about sexual behavior, incarceration and legal issues/history. The Commission
believes that the standard intake forms used should be revised to provide universal
domestic violence screening and to align with other screening efforts in the state, such
as Healthy Moms, Happy Babies and the Blueprint Women’s Health Initiative.
There is a free online training program on Counselling on Access to Legal Means
(CALM) and other clinical interventions that may be useful for clinicians to complete
such as Collaborative Assessment and Management of Suicidality (CAMS). We
recommend that all health care providers be required to complete evidence-based
online training such as these. The statewide work group is encouraged to explore a
system of accountability to promote these best practices.
The Commission also looked at the challenges posed when the victim has mental
health issues that may make it difficult for him or her to get help. In some cases, the
victim may have repeatedly contacted police with complaints that stem from his/her
illness and as a consequence police are uncertain how to respond. The victim may fear
that she is less likely to be believed because of her mental illness and the responsible
party may have reinforced this fear. In some cases, the responsible party may have
convinced authorities that her complaints are unwarranted and a symptom of mental
illness. Family members may be confused as well, as mental illness may prevent them
from recognizing that a loved one is experiencing domestic violence. The Commission
recommends that all mental health agencies designate a person to serve on their local
county Domestic and Sexual Violence task force and ensure their providers are familiar
with local domestic violence advocacy programming and local Domestic Violence
Accountability Programs.
Like mental illness, domestic violence has a stigma attached to it. We are often
reluctant to speak openly about it. By encouraging our community to speak more
openly about both, we may encourage those who are experiencing domestic violence to
speak up. Mental health and health care professionals are critical resources who can
open this conversation by asking about domestic violence in routine screening.
Agency of Human Services
• Convene a statewide leadership group from the Agency of Human Services, to
include the AHS Domestic Violence Steering Committee, Department of Mental
Health (DMH), Department of Children and Families, Department of Health,
Vermont Council on Domestic Violence, the Vermont Network, law enforcement,
emergency medical technicians and dispatcher services to begin developing a
consistent approach to the intersection of domestic violence and mental health.
11Department of Mental Health
• With help of the AHS leadership group, develop a system of accountability to
promote statewide use of online clinical training opportunities in best practices for
clinical interventions, such as Counselling on Legal Means (CALM) and
Collaborative Assessment and Management of Suicidality (CAMS) within their
designated agencies.
• Ensure all mental health service providers in designated agencies incorporate
screening methods that address whether a person who has suicidal ideation also
poses a homicidal risk to partners and children in domestic violence cases,
including those who conduct screening for courts.
• Revise standard intake forms for designated agencies to provide universal
domestic violence screening, including specific questions about thoughts to harm
intimate partners or children, and to align with other screening efforts in the state,
such as Healthy Moms, Happy Babies and the Blueprint Women’s Health
Initiative.
• Increase visibility of services available to family members and third parties who
are concerned that a loved one who has perpetrated domestic violence may
pose a risk of harm to him or herself or others.
• Develop a plan of how we can best target our resources toward reducing the
stigma of both domestic violence and mental illness in our communities.
Mental Health/Health Care Provider Recommendations
• Ensure all mental health and health care providers are familiar with the process
for storing firearms in their community and the legal methods for removing
firearms in dangerous situations such as relief from abuse and extreme risk
protection orders.
• All mental health clinicians should be trained to address issues of domestic
violence and coordinate safety planning with domestic violence experts, including
understanding lethality factors and when to encourage removal of firearms.
• All mental health agencies should designate a person to serve on their local
countywide Domestic and Sexual Violence task force.
• All mental health and health care providers should be familiar with Domestic
Violence Accountability Programs in their community and consider referring
clients who are perpetrators of domestic violence to them.
12Emergency Relief from Abuse Order Process
In one of our case reviews, the Commission looked closely at the process for obtaining
a relief from abuse order outside of normal court hours. Vermont has had a process in
place for victims to seek an emergency protection order against a family or household
member at any time of day. During regular court hours, the order is available from
family court. If it is outside of normal business hours, the plaintiff contacts an after-
hours court worker who will have the plaintiff prepare an affidavit and then the court
worker will contact a judge. The judge can grant an ex parte emergency order if she
finds that there is an immediate danger of further abuse.
Some after-hours court workers are full-time court employees, but the positions can be
difficult to fill, and the court contracts with non-employees as well to provide this service.
After-hours coverage is provided by relatively few people over large geographical
distances which can create long wait times for plaintiffs who are meeting them in
person. Training of new after-hours workers is generally done by job shadowing and
there are no formal training requirements. After-hours workers who are contract
workers have little opportunity to interact with other after-hours workers or full-time court
staff in their region. There are few 24-hour police agencies in many areas of the state,
and it can be difficult to find a safe, secure location to meet the plaintiff.
In order to address some of these issues, the judiciary asked the legislature to amend
the relief from abuse order statute to allow electronic filing. On April 25, 2018, Governor
Scott signed H.836 which amended 15 V.S.A. § 1106 to provide for electronic filing of
emergency orders: 1) where a secure setting is not available, 2) when the worker
determines electronic filing is “appropriate”, a broad catch-all category that can include
bad weather conditions, lack of child care and other obstacles to meeting in person. 15
V.S.A. §1106.
Electronic filing is in the planning stages as a pilot program. The judiciary also arranged
with the state police to provide safe meeting locations in state police barracks in those
areas of the state where there is no 24-hour police agency. The state police took on
this additional service. The Commission wishes to thank the judiciary and the state
police for their efforts to ensure that after-hours emergency orders are available
statewide.
The Commission has identified other obstacles that also need to be addressed. After-
hours workers need structured and ongoing domestic violence training. The
Commission is pleased that the court administrator’s office now includes them in the in-
service training days for judiciary staff. However, all after-hours workers need
formalized, intensive training in the dynamics of domestic violence. Hiring criteria
should reflect a preference for persons who have prior experience working with families
who have experienced domestic violence. All family court staff, including after-hours
workers, should have domestic violence training that incorporates trauma-informed
practices.
13The Commission believes that the relief from abuse order process itself needs revision.
After-hours workers are given a prepared script that they are expected to follow for
consistency. While not intentional, some of the preliminary scripted questions can feel
discouraging to plaintiffs. An after-hours worker who strictly follows the script may find
that it is at odds with the trauma-informed practice of building rapport with the person
first. The plaintiff may not understand why the worker is asking the preliminary scripted
questions and may interpret as it discouraging the need for an after-hours order. For
example, by asking if the person is in a safe place now and can you stay there, the
plaintiff may feel that the worker is questioning whether he/she really needs an
emergency order if the plaintiff has a safe place to be until regular court hours. The
plaintiff may feel that by asking these questions first, the worker is not really interested
in hearing what happened. Moreover, these questions can be difficult for a plaintiff to
accurately determine. Research suggest that victims of domestic violence tend to
underestimate, rather than overestimate, their risk. The subcommittee of the
Commission also developed detailed suggestions for improving the after-hours relief
from abuse order process which are set forth in our recommendations.
Currently there is no expectation that an after hours-workers keep a log of all calls
received. While the after hours worker does track of the number of calls and the
number of times that the worker is called out to meet with a plaintiff, this is only for
compensation purposes. The Commission believes that it is important for accountability
to track information about all calls received. The worker should keep a detailed record
of all calls, including those that do not result in an order. We recommend that the Court
Administrator’s office create a logging system for after-hours workers to track all calls,
including the name of the caller, location, police agency if involved, potential defendant
and the disposition of the call. Workers should be required to use the log.
Court Administrator’s Office Recommendations
• Create a formalized training process for after-hours workers that ensures they
are trained in trauma-informed practices and understand the dynamics of
domestic violence. Create opportunities for after-hours workers who are not part
of full-time staff to connect to other court personnel and advocates in their region,
and also with each other.
• Expand the electronic filing option to all counties.
• Eliminate these preliminary questions from the after-hours script: Are you in a
safe place now and will you be able to remain in a safe place until (the next court
day)? Do you feel safe waiting until tomorrow (next court day) to go to court to
file your complaint and are you willing to wait?
• Revise the questions to obtain the necessary information in a neutral and trauma
informed way. For example, what relief are you looking for? Are you interested
in an emergency order?
14• Consider incorporating the following suggestions into the after-hours relief-from-
abuse-order process:
1. Begin with an introduction of yourself and some acknowledgement of the
person to build rapport. Explain why you need to ask some preliminary
questions first to determine if the relationship would qualify for an order. If
it does not, explain the other non-emergency orders that the person might
be eligible for and how to get more information about them.
2. Ask if the person has had an opportunity to speak with an advocate.
Know the name of your local program(s). Have the phone number of the
24-hour hotline available. Let the plaintiff know that he/she can expedite
the process by filling out and affidavit with an advocate before the worker
arrives and that the forms are available online.
3. If you are meeting in person, incorporate trauma-informed practices into
your work. This would include, for example, offering the plaintiff a choice
of seating if possible, introducing yourself and your role, and
acknowledging that you are sorry that they have had this experience. Use
open-ended questions and give the person time to pause before
answering if needed. Don’t expect a chronological narrative.
4. Ask what type of relief the person is requesting. Because of the
heightened lethality risk when firearms are involved, it is important to ask if
the defendant has firearms and if the plaintiff has any concerns about
defendant’s access to firearms.
5. If the emergency order is not granted, let the plaintiff know about the
option to file for a non-emergency order during regular court hours and
other types of orders that might be available, such as stalking or sexual
assault protection orders.
6. If the order is granted, confirm the best method for law enforcement to
contact the plaintiff when the order is served and let the plaintiff know if
there is any reason that might delay law enforcement from attempting to
serve the order right away. Plaintiffs should be encouraged to speak with
an advocate who can assist him/her in creating a safety plan and the
importance of having a safety plan even if the order is granted and served.
• Create a log for after-hours workers to use to track information about each
call, including the name of the caller, location, police agency if involved,
potential defendant and the disposition of the call.
15PART TWO: DOMESTIC VIOLENCE 2017 HOMICIDE DATA
• In 2017, there were 17 homicides total and 11 of those were domestic violence
related (65%). Domestic violence decedents ranged in age from 27 to 70 years
old. Of these, nine of the victims were white, one asian, and one black. Of these
responsible parties, eleven were white, and one was asian.
• Overall, nearly three-fourths of domestic violence-related decedents were female
(73%). Gender breakdown of the decedents in the domestic violence-related
homicides was as follows:
Gender of Decedent #
Male 3
Female 8
Males accounted for 67% of the responsible parties. In one homicide, there were two
responsible parties. Gender breakdown of the responsible parties in the domestic
violence-related homicides was as follows:
Gender of Responsible Parties #
Male 8
Female 4
The majority of the domestic violence homicides involved either current or former
intimate partners. The relationship between the victim and the responsible party was:
Relationship between Victim and RP #
Intimate Partners: 6
(1) Current 3
(2) Recently Separated 3
Family member 3
Household Member 1
Other DV Related (Law Enforcement Involved Shooting) 1
Half of the counties in Vermont had at least one domestic violence homicide. Counties
where the homicides occurred:
County #
Chittenden 1
Franklin 2
Essex 2
Rutland 2
Washington 2
Windham 1
Windsor 1
In 27% of the homicides and in one of the suicides, firearms were involved.
Cause of Death #
Sharp Object Impact/Stabbing 4
16Firearm 2
Strangulation 2
Neglect of Care 1
Blunt Force 1
Firearm and Stabbing 1
Ten of the eleven domestic violence homicides occurred in the home (91%) and one
occurred in an unknown place (victim found near a roadway).
Two of the twelve responsible parties died by suicide, one involved a firearm and the
other an intentional overdose of prescribed medication.
One of the domestic violence victims had a current relief from abuse order in effect
against the responsible party at the time of her death.
There were young children present in the home at the time of one domestic violence
homicide and a young child who lived in the home but was not immediately present at
the time of death in another.
In four of the eleven homicides, substance and/or alcohol use was involved.
Police Response
In 2017, 62 law enforcement agencies responded to 1,213 incidents involving domestic
violence. Fifty-six (56) agencies were involved in 1,424 incidents involving service of an
abuse prevention order, for a total of 2. 637 incidents. This number decreased from the
3,491 calls received in 2016.
Vermont Network Against Domestic and Sexual Violence
Vermont Network member programs responded to 17,616 hotline calls and served
8,878 individuals, including 7004 victims of domestic or sexual violence. These
numbers also decreased from the 19,816 hotline calls and 9.376 individuals served in
2016.
DCF-Family Services Division
In 2017 DCF Family Services Division received 2,904 domestic violence-related intake
calls. It accepted 898 calls for child safety intervention and 183 of those were
substantiated for child maltreatment.
Vermont Department of Corrections
As of December 31, 2017, there were 9,167 individuals in the custody of the VT
Department of Corrections (DOC). Of these, 1,687 were DV offenders.
17389 individuals were incarcerated with at least one DV offense. Of these, 13 were
female, 371 were male, and five did not identify as male/female. 144 were detained
awaiting disposition, and 245 were sentenced. Of the females, 12 were held on felony
charges, one was held on a misdemeanor. Of the males, 333 were held on felony
charges and 38 were held on misdemeanors. Of those who did not identify as
male/female, all five were held on felony charges.
In the probation and parole offices, 1,298 individuals were convicted of at least one DV
offense. Of these, 124 were on Missing status, with a warrant issued for their arrest.
Of the total filed DV population of 1,298, 158 were female, 1,139 were male, and in one
no gender was designated. Of the females, 46 had felony convictions and 112 were
misdemeanants; of the 46 felons, 39 had DV felonies. Of the males, 640 were felons,
and 499 were misdemeanants; of the 640 felons, 478 had DV felonies. The one person
who did not have a gender designated was a misdemeanant.
Of the 1,687 DV offenders in DOC custody, 525 had been sentenced for the first time
during 2017. At the other end of the spectrum, 52 had begun their DOC involvement
during the 1980s.
1,687 Total DV Offenders
389 Incarcerated
1,298 Community Supervision
These numbers decreased from 1,723 total DV offenses, 477 of them incarcerated and
1,276 under community supervision as of December 30, 2016.
Criminal Charges for Vermont District Court
I. Misdemeanor domestic assault charge dispositions by county
Of the total 11,159 misdemeanors filed in the Criminal Division of the Vermont Superior
Court in FY17, 702 were domestic assault charges according the statistics available
from the Court Administrator’s Office.1 Misdemeanor domestic assault charges declined
3% from the previous year and 12% over the last five years.2
There were 797 misdemeanor domestic assault charges under 13 V.S.A. § 1042
disposed in 2017. Of the 797 cases, resolutions were fairly evenly split between 369
(46%) resolved by pleas and 366 (46%) dismissed by the prosecutor. Very few cases
(24 or .3%) went to either a jury or court trial. Windham and Bennington counties had
half, or 12 of the 24 cases that went to trial.
1 Appendix I to the Vermont Judiciary Annual Statistical Report for FY17 (“Appendix”)
2 Vermont Judiciary Annual Statistical Report for FY17, p. 28.
18Misdemeanor Domestic Assault
Dismissed No
Dismissed
County Total Plea Trial By Probable
By Court
Prosecutor Cause
Addison 22 13 1 8 0 0
Bennington 68 33 6 27 2 0
Caledonia 42 21 1 17 1 0
Chittenden 160 55 1 100 1 0
Essex 5 4 0 1 0 0
Franklin 96 53 0 41 2 0
Grand Isle 4 1 3 0 0 0
Lamoille 32 16 1 14 1 0
Orange 21 8 0 6 0 0
Orleans 58 37 3 17 1 0
Rutland 65 39 0 18 4 0
Washington 61 27 0 29 1 1
Windham 85 30 6 48 0 1
Windsor 78 32 2 40 0 2
Total 797 369 24 366 13 4
The total 797 cases also includes 21 cases that were resolved by change of venue,
diversion, drug court, mental health court, youthful offender or transfer to juvenile court.3
II. Felony domestic assault charge dispositions by county
Of the 3,396 felonies filed in the Criminal Division of the Vermont Superior Court in
FY17, 497 were felony domestic violence charges.4 Although this represents a small
decrease (503 v. 497) from last year, felony domestic charges have increased 47% in
the last 10 years.5
There were 409 felony domestic assault charges brought pursuant to 13 V.S.A. § 1043
and 1044 that were disposed in 2017. Of those, the largest number of cases were
dismissed by the prosecutor, 256 (63%) followed by 126 resolved by plea (31%).
Felony Domestic Assault
Dismissed
Dismissed No
County Total Plea Trial By
By Court Probable
Prosecutor
Cause
Addison 9 4 0 3 0 0
Bennington 47 12 3 32 0 0
Caledonia 25 11 0 12 1 0
3 Data provided by the Crime Research Group, http://www.crgvt.org. Note this data is for calendar year
2017. (“CRG”)
4
Appendix I
5 Vermont Judiciary Annual Statistical Report for FY17, p. 27.
19Chittenden 91 20 0 67 4 0
Essex 5 2 0 2 1 0
Franklin 41 16 0 25 0 0
Grand Isle 3 0 1 1 1 0
Lamoille 15 3 0 10 1 1
Orange 4 2 0 2 0 0
Orleans 40 16 1 22 1 0
Rutland 53 20 1 26 5 1
Washington 27 7 0 20 0 0
Windham 16 5 0 11 0 0
Windsor 33 8 0 23 0 0
Total 409 126 6 256 14 2
Note that the 409 total cases also includes 5 cases not reflected in the subcategories
above that were resolved by a change of venue or youthful offender program. The total
does not include 7 cases filed in Chittenden county on human trafficking charges
pursuant to 13 V.S.A. § 2652.6
Violations of Abuse Prevention Order dispositions by county
There were 471 violations of abuse orders under 13 V.S.A. § 1030, both felony and
misdemeanor charges, disposed in 2017. Most charges were misdemeanor charges,
409 misdemeanors compared to 62 felonies. Grand Isle, Lamoille, Orleans, and
Windsor had no felonies.
Most cases, 230 of the 471 (49%) were resolved by plea. One hundred and ninety-nine
(199 or 42%) were dismissed by the prosecutor. Eight were resolved by trial.
Abuse Prevention Order Violations, Felony & Misdemeanor
Dismissed Dismissed No
County Total Plea Trial
By By Court Probable
Prosecutor Cause
Addison 20 12 0 4 0 4
Bennington 38 22 0 13 1 2
Caledonia 33 20 1 12 0 0
Chittenden 116 42 1 67 1 5
Essex 6 6 0 0 0 0
Franklin 48 29 0 17 0 1
Grand Isle 2 2 0 0 0 0
Lamoille 14 3 0 5 1 5
Orange 13 7 0 5 0 0
Orleans 20 9 2 7 0 1
Rutland 49 29 0 16 0 2
Washington 35 9 2 19 3 1
6 Data provided by CRG.
20Windham 49 21 2 25 1 0
Windsor 28 19 0 9 0 0
Total 471 230 8 199 7 21
Categories above do not include the following dispositions: change of venue (2), drug
court (2), diversion (1), transfer to juvenile court (1).7
Civil Relief from Abuse Orders in Vermont Family Court
According to the Court Administrator’s office, there were 3,125 relief from abuse orders
added in FY17 and 3,156 disposed. The total number of orders have declined slightly
over the past five years.8
Of the 3,156 disposed, 2,386 (76%) were granted temporary orders and 759 were
denied. Of the 2,386 granted temporary orders, 1,142 (48%) were granted a final
order.9 Of the 3,125 added in FY17, 725 of these were applied for after regular court
hours.
Relief from Abuse Orders by County10
Total Temp Order Final Order
County Relief From Abuse Granted/ Granted/
Disposed % %
Addison 147 111 (76%) 56 (50%)
Bennington 292 240 (82%) 122 (51%)
Caledonia 166 140 (84%) 47 (34%)
Chittenden 572 515 (90%) 212 (41%)
Essex 27 26 (96%) 9 (35%)
Franklin 297 217 (73%) 107 (40%)
Grand Isle 32 23 (72%) 15 (65%)
Lamoille 133 103 (77%) 49 (48%)
Orange 105 78 (74%) 39 (50%)
Orleans 185 168 (91%) 88 (52%)
Rutland 454 309 (68%) 188 (61%)
Washington 327 199 (61%) 77 (39%)
Windham 213 134 (63%) 81 (60%)
Windsor 195 123 (63%) 52 (42%)
Total 3,145 2,386 1,142
7 Data provided by CRG.
8 Vermont judiciary Annual Statistical Report for FY17, p. 16. Note there were 11 cases statewide that
involved a change of venue that are reflected in the total disposed but do not count toward the
percentage of orders granted.
9 Id. At 21, Appendix I.
10
Appendix II
21Civil Stalking and Sexual Assault Orders in Vermont Superior Court
Title 12 provides for protection orders for non-household and non-family members
regarding stalking and sexual assault. According to the Court Administrator’s Office,
there were 883 orders against stalking or sexual assault added in FY17 and 852 orders
disposed.11 Unlike abuse prevention orders, orders against stalking or sexual assault
are handled by the Civil Division of the Vermont Superior Court. There is no after-hours
process currently available for these orders. Although most civil cases types have
declined, the number of protection orders filed has increased 29% over the last five
years.12
Of the 850 orders disposed in FY17 (not including two change of venue cases), 602 or
71% resulted in a temporary order and 260 or 43% received final orders.
Orders against Stalking or Sexual Assault by County13
County Orders Temporary Final
Disposed granted/% granted/%
Addison 34 22 (65%) 11 (50%)
Bennington 89 72 (81%) 36 (50%)
Caledonia 66 57 (86%) 15 (26%)
Chittenden 146 101 (69%) 46 (46%)
Essex 9 9 (100%) 0 (0%)
Franklin 127 108 (85%) 39 (36%)
Grand Isle 15 6 (40%) 2 (33%)
Lamoille 40 29 (73%) 11 (38%)
Orange 24 19 (79%) 6 (32%)
Orleans 44 37 (84%) 14 (38%)
Rutland 133 86 (65%) 43 (50%)
Washington 21 3 (14%) 2 (67%)
Windham 39 18 (46%) 9 (50%)
Windsor 63 35 (56%) 26 (74%)
Total 850 602 260
Participants in Domestic Violence Accountability Programs
According to data provided by the Vermont Council on Domestic Violence, who
oversees domestic violence accountability programming in Vermont, there were a total
of 385 participants for FY2017. The following is a breakdown by county:
11
Appendix I
12 Vermont Judiciary Annual Statistical Report for FY17, p. 33
13
Appendix II
22DV Accountability
Programs
46 46 48
41
38
32 32
25 24 24
21
8
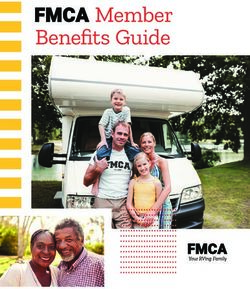
HISTORICAL DATA – 1994 TO 2017
From 1994-2017, there were a total of 296 adult homicides. Of those, there have been
148 adult, domestic-violence-related homicides (50%).
Total # DV Homicides
11 11
10 10
8 8
7 7 7 7 7 7
6 6 6
5 5
4 4 4
3
2 2
1
Homicide and Fatality Chart 1994 to 2017
Total # Family Household Other Total Total RP
Year Adult Partner Ex Member Member DV # % Suicide
Homicides Partner Non Non Related DV DV /Att
Partner Partner Suicide
2017 17 3 3 3 1 1 11 65% 2 / 0
2016 15 4 0 1 1 0 6 40% 1 / 0
2015 16 0 1 4 0 1 6 38% 1 / 0
2014 11 3 0 1 1 1 6 55% 1 / 0
2013 12 3 1 1 0 2 7 58% 3 / 2
2012 13 0 1 3 0 0 4 31% 1 / 0
2011 8 3 1 0 0 0 4 50% 0 / 0
2010 9 0 0 2 0 1 3 33% 1 / 0
232009 4 0 1 0 0 1 2 50% 1/1
2008 15 5 0 3 0 3 11 73% 0/1
2007 11 1 2 2 2 0 7 64% 3/0
2006 16 2 1 2 1 1 7 44% 0/0
2005 12 0 0 0 0 2 2 17% 0/0
2004 10 3 1 0 0 0 4 40% 1/0
2003 15 1 2 4 1 2 10 67% 0/0
2002 10 1 0 0 0 0 1 10% 0/0
2001 13 0 0 3 1 1 5 38% 0/0
2000 16 3 1 2 0 2 8 50% 1/0
1999 18 2 1 3 2 2 10 56% 2/0
1998 12 3 2 1 0 1 7 58% 3/0
1997 11 2 1 2 0 2 7 64% 2/0
1996 12 1 2 2 1 2 8 67% 3/0
1995 13 6 0 0 0 1 7 54% 4/0
1994 7 1 1 1 0 2 5 71% 1/0
TOTAL 296 47 22 40 11 28 148 49% 29/ 4
80% of the responsible parties are male. Females account for 53% of the decedents in
adult, domestic violence related homicides.
Gender
Decedents Total 148
Male 70
Female 78
Responsible Parties
Responsible Parties Total 148
Male 118
Female 30
Relationship
Most adult, domestic violence-related homicides have involved a current intimate
partner:
Relationship #
Partner 47 (32%)
Ex-partner 22 (15%)
Family 40 (27%)
Household 11 (7%)
Other 28 (19%)
24County
Rutland County, with a population of 61,642, has experienced the most adult, domestic
violence related homicides. Chittenden County, Vermont’s most populated county with
156,545 residents had the second largest number. All counties have experienced at
least two adult, domestic violence-related homicides. These homicides by county are
broken down as follows:
Addison 9
Bennington 9
Caledonia 13
Chittenden 24
Essex 4
Franklin 6
Grand Isle 2
Lamoille 5
Orange 7
Orleans 9
Rutland 27
Washington 12
Windham 8
Windsor 13
Total 148
Method
Most domestic violence-related homicides have been committed with firearms (55%).
Cause of Death
Motor Vehicle 1
Firearm and Stabbing 1
Blunt Trauma and Strangulation 1
Neglect 2
Firearm 2
Strangulation 7
Other 7
Sharp Object/Stabbing 22
Blunt Trauma 23
Firearm 82
25Child Witnessing
Between 1994 and 2017, there were 50 children who were either at the scene of the
domestic violence related homicide when the incident occurred or who were at the
crime scene immediately before or after the incident.
Abuse Prevention Orders
From 1994-2017, there were 19 victims of domestic violence related homicide (13%)
who had a current Relief from Abuse Order in effect against the responsible part.
Officer Involved Shooting
From 1994-2017, there have been four domestic violence suspects killed by law
enforcement.
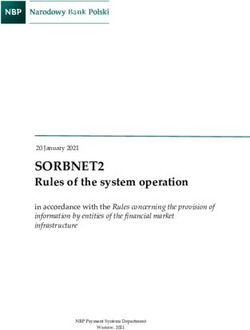
Suicide
There have been 39 domestic violence-related suicides, 35 men and 4 women. Most
(31) of these are responsible parties who have died by suicide after committing a
homicide. The number also includes a very small number of persons who have died by
suicide as a result of trauma related to domestic violence. This is very likely an
underrepresentation of the true number. The Commission knows of an additional four
responsible parties who attempted suicide following a homicide. Most domestic
violence-related homicides involve the use of a firearm.
Jump/Fall
Suicides Related to DV
1 (2.5%) Asphyxia by Fire Intentional
1 (2.5%) Overdose
Stabbing 1 (2.5%)
1 (2.5%)
Hanging
2 (5%)
Asphyxia by
Carbon Monoxide
3 (8%)
Firearm
30 (77%)
26You can also read