Discussion Summaries - gijournal.org
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Discussion Summaries
A Minty Fresh Perspective: Clarifying the role of
peppermint oil in the management of irritable bowel syndrome
John A. Damianos, MD;
Department of Internal Medicine
Yale New Haven Health System
New Haven, CT, USA
Muddasir Ayaz, MD
Department of Internal Medicine, Division of Gastroenterology
University at Buffalo, Buffalo, NY, USA
Daniel Keszthelyi, MD PhD
Department of Internal Medicine, Division of Gastroenterology-Hepatology
Maastricht University Medical Center, Maastricht, the Netherlands
Xiao Jing Wang, MD
Department of Internal Medicine, Division of Gastroenterology-Hepatology
Mayo Clinic, Rochester, MN, USA
Corresponding author
John Damianos
20 York Street
Tompkins 266
New Haven, CT
06510
john.damianos@yale.edu
Keywords: peppermint oil, IBS, CAM, placebo
Financial Disclosures & Conflicts of Interest:
JD has no relevant financial disclosures or conflicts of interest.
MA has no relevant financial disclosures or conflicts of interest.
DK has received research funding from the Netherlands Organisation for Health
Research and Development (ZonMw), and Will Pharma for a study investigating the
efficacy of peppermint oil in IBS. DK has received research funding from Allergan,
Grunenthal, Rome Foundation, United Europe Gastroenterology, Dutch Foundation for
Gastroenterology, Horizon 2020, and the Netherlands Organisation for Health Research
and Development (ZonMw), unrelated to the current paper. DK has received a
speaker's fee from Dr Falk (paid to institution), unrelated to the current paper.
@Gijournal Volume 1, Issue 14, March 2022Discussion Summaries
XJW has no relevant financial disclosures or conflicts of
interest.
Abstract:
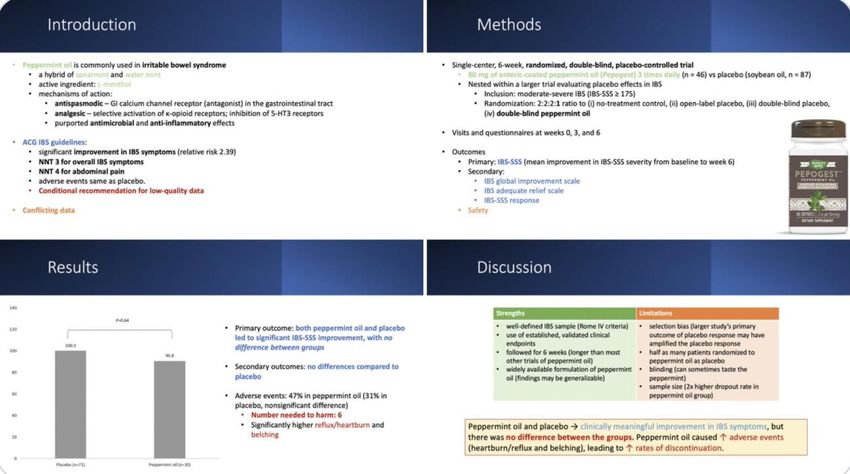
Peppermint oil is commonly used by patients for the management of irritable bowel
syndrome (IBS) and is even recommended in several professional society guidelines for
IBS. However, studies on its efficacy have been conflicting, with multiple studies finding
no benefit over placebo. We summarize the @GIJournal discussion on February 6,
2022 during which we presented the article by Nee et al. titled “Peppermint Oil
Treatment for Irritable Bowel Syndrome: A Randomized Placebo-Controlled Trial.” Key
findings were reviewed by our expert Dr. Daniel Keszthelyi (DK) and the session was
moderated by Dr. Iris Wang (IW).
Introduction: IBS is a highly prevalent disorder of gut-brain interaction whose
pathophysiology is incompletely elucidated. It is characterized by abdominal pain and
alteration in bowel habits (diarrhea, constipation, or both). Various pharmacologic and
nonpharmacologic treatments exist for IBS with variable efficacy. IBS is also susceptible
to a very high placebo response, which makes designing clinical trials challenging.
Peppermint oil is a common supplement used and recommended in IBS, due to historic
traditional use of peppermint to alleviate gastrointestinal distress, preclinical mechanistic
studies that support its use, and clinical trials affirming its benefit. However, clinical trials
have found conflicting results, with some showing benefit, and others showing no
benefit over placebo. The most recent trial assessing its efficacy was a double-blind
placebo controlled trial described below.1
Article summary
@Gijournal Volume 1, Issue 14, March 2022Discussion Summaries
Discussion:
@Gijournal Volume 1, Issue 14, March 2022Discussion Summaries
n = 123
When do you recommend using peppermint oil?
IW: I think about peppermint oil when the patient’s pain is spasmodic in nature. The listed
indications include functional dyspepsia, IBS, childhood final abdominal pain, and post-
operative nausea. My practice is an early, short term trial for mild symptoms in patients hesitant
to try medications, OR a late, limited trial (4-6 weeks), in patients who have chemical
sensitivities and have no other medical options.
DK: I generally recommend at least 4 weeks and ideally 8 weeks. In our previous trial,
therapeutic effect seemed to increase after 6 weeks. The evidence is there for certain
formulations that contain at least 182 mg of peppermint oil. So lower doses might not be as
effective.2
IW: This is super key--we need to know what doses were studied in trials, especially for CAM
so that real-world use can be tailored. When the FDA is not involved, we have to pay closer
attention!
@LindaNguyenMD :I use peppermint as first line since the risk is low. Additionally, most
therapies are not effective alone and require augmentation, and there are emerging studies about
active placebo, which speaks to the power of the doctor-patient relationship.
@TennysonMD:Peppermint oil in IBS is what I offer to certain patients, particularly those not
ready for a neuromodulator & who don’t have GERD. I see them back in 6-8 weeks and reassess;
some feel better and eventually stop, but the same number have no effect and are more willing
try other therapies.
@john_damianosMD: I recommend a trial of peppermint oil as a first line therapy in functional
dyspepsia and mild-moderate IBS. I tell patients
-studies have been conflicting
-many have shown No entry difference from placebo
-effects may be placebo
-can be expensive
-can cause side effects
-if no benefit, then stop
DK: As for costs, we actually performed a cost-effectiveness study and this showed some
positive effects.3
@Gijournal Volume 1, Issue 14, March 2022Discussion Summaries
@GIPearls: The problem is – many choices, yes – but it’s
unregulated. What percent do you think has "peppermint" in it versus recycled newspaper? (One
study of supplements showed that something like 1 out of 5 didn't contain the listed ingredients).
@AllonKahn: This is really critical. We don’t know the “true” dose in each pill OR the right
dosimetry for the condition, so that makes using it or studying it really challenging
Placebo response was exceptionally high in this trial. Any comments on that?
@john_damianosMD: The primary outcome of the larger study was to assess the
effects of open label placebo, so it was powered for this and there may be an aspect of
selection bias here too of selecting patients more susceptible to the placebo effect.
IW: ·This speaks well to the global study that our current paper is nested in: what IS the placebo
effect? Especially in DBGI, therapeutic alliance is SO KEY that I think the strength of your
placebo effect hangs on it! Sadly this is so lacking for many of our patients due to time
constraints.
@muddasir_ayazMD : I do think this study highlights an important point on the role of
placebo. Independent of the mechanism of action, there is something to be said even if patients
are told “this is safe, we don’t know if or how it works, but you may find some relief.” I also
think the challenge that studies like these highlight the discomfort we have with prescribing or
recommending treatment when we don’t understand composition or MOA — my argument
would be that we do this all the time; most of us only know the active metabolite. I think a lot of
vitamins and supplements used ARE by placebo and I think an important point noted in the study
is the minimal harm in the formulation — recommending it may not be an issue when the
indication, documentation and patient-physician relationship create space for it.
@MujagicZlatan: Also in this case, patient selection is the key. We need clinical characteristics
or biomarkers to predict response to peppermint oil (and other therapies). Certainly, it is not a
treatment for every IBS patient, but it is effective in many.
@mgrover_gi: We need to get to a stage where we stop recruiting “Rome IV IBS”.
Instead ,complement that with pathophysiology. The classic example is the glutamine
trial enrolling IBS patients with increased permeability; the results were very
encouraging.4
@Gijournal Volume 1, Issue 14, March 2022Discussion Summaries
@DrBloodAndGuts: Is it unethical to give pts a substance
that has no greater benefit than placebo (and worse AEs) just to ride the high placebo
response? Medical ethicist Sissela Bok thinks so (see influential article in Scientific
American titled ‘‘The Ethics of Giving Placebos.’’5
IW: Let's reiterate the cons too
- Side effects: Heartburn, nausea, dry mouth, gas, headache, rash
- Can cause allergic reaction
- Unknown effects in pregnancy and breastfeeding
- These are not essential oils. Patients should be using enteric coated or food safe
oils.
@john_damianosMD: Per @AnthonyLemboMD's open-label placebo work, certain
patients are very responsive to the concept. I think similarly here, certain patients are
more likely to benefit.6
@SultanMahmoodMD: I always wonder what the ethics are for using a medication
for placebo benefit . Even peppermint oil has some side effects and my experience has
been that the more you “sell” the treatment the better it works.”
DK: Any therapeutic benefit has two components: the placebo effect and the
biological or chemical one. The way you present the treatment to the patients will
increase placebo effects.
@mgrover_gi: Another huge issue is a quick secondary non-response, as in the drug
working for a short period of time. Which although can be an early placebo effect, also
might reflect layering of peripheral and central mechanisms where targeting one may
not suffice or may be overwhelmed quickly.
How do the results compare to another recent trial in Gastro 2020;158(1):123-126.7
IW: 26 of 63 patients in the ileocolonic-release peppermint oil group had a response
(41.3%, P = 0.385 vs placebo), 22 of 64 patients in the placebo group had a response
(34.4%) Small intestinal peppermint > placebo in the secondary outcome of abdominal
pain, discomfort, and IBS severity. So overall, the results are quite similar: abdominal
pain response didn’t differ, no differences overall, and 29 of 62 patients in the small-
intestinal-release peppermint oil group had a response (46.8%, P = .170 vs placebo).
@LinChangMD: The Gastro study comparing peppermint oil with a small intestinal vs
ileocolonic release was informative because it suggests that treatment may need to
@Gijournal Volume 1, Issue 14, March 2022Discussion Summaries
target the small bowel and not only colon to effectively relieve
pain. It made me think about the true mechanisms of pain in IBS.
Summary:
Peppermint oil is commonly used in IBS, but the literature has been conflicting. The
most recent study, a double-blind placebo controlled trial, found that both peppermint oil
and placebo significantly improved IBS symptoms, with no difference between the
groups. Importantly, patients in the peppermint oil group reported more adverse events,
especially reflux, heartburn, and belching. Peppermint oil may indeed be effective for
certain patients, although its effects may largely be driven by the placebo effect. It is
important to discuss this fact with patients, as well as the potential adverse effects.
Peppermint oil is a reasonable first line option for IBS, especially in patients with IBS-D,
unwilling or unable to take medication, and open to the placebo effect. Therapeutic
alliance, shared decision making, and partnering with the patient are beneficial.
References:
1. Nee, Judy, et al. "Peppermint oil treatment for irritable bowel syndrome: a
randomized placebo-controlled trial." The American journal of gastroenterology
116.11 (2021): 2279-2285.
2. Weerts, Zsa Zsa RM, et al. "Efficacy and safety of peppermint oil in a
randomized, double-blind trial of patients with irritable bowel syndrome."
Gastroenterology 158.1 (2020): 123-136.
3. Weerts, Zsa Zsa RM, et al. "A trial‐ based economic evaluation of peppermint oil
for the treatment of irritable bowel syndrome." UEG Journal 9.9 (2021): 997-
1006.
4. Zhou, QiQi, et al. "Randomised placebo-controlled trial of dietary glutamine
supplements for postinfectious irritable bowel syndrome." Gut 68.6 (2019): 996-
1002.
5. Bok, Sissela. "The ethics of giving placebos." Scientific american 231.5 (1974):
17-23.
6. Lembo, Anthony, et al. "Open-label placebo vs double-blind placebo for irritable
bowel syndrome: a randomized clinical trial." Pain 162.9 (2021): 2428-2435.
7. Weerts, Zsa Zsa RM, et al. "Efficacy and safety of peppermint oil in a
randomized, double-blind trial of patients with irritable bowel syndrome."
Gastroenterology 158.1 (2020): 123-136.
@Gijournal Volume 1, Issue 14, March 2022You can also read