Diabetes Update 2018: Pathogenesis of Diabetes - The Medical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Diabetes Update 2018:
Pathogenesis of Diabetes
Katherine Lewis, MD, MSCR
Assistant Professor, Endocrinology and Pediatric
Endocrinology
Endocrinology, Diabetes and Medical Genetics
Medical University of South Carolina
February 3, 2018
Disclosures
I have no relevant disclosures or conflicts of
interest related to this presentation
1Objectives
1. Review the pathogenesis of diabetes
mellitus (DM)
2. Describe and differentiate type 1 and type 2
diabetes
3. State diagnostic criteria
National Diabetes Statistics
• 30.3 million people or 12.2% of the U.S. population have
diabetes (2015)
• Diagnosed
– 23.0 million people
– 132,000 children and adolescents
– 5% with type 1 diabetes
• Undiagnosed
– 7.2 million people (23.8% are undiagnosed)
CDC, National Diabetes Statistics Report, 2017
2Prediabetes Statistics
Prediabetes among people aged 20 years or older,
United States, 2015
• 84.1 million Americans (33.9% of population) age 18
and older had prediabetes based on fasting glucose
or A1C
• 11.6% of these report being told by a health
professional that they had this condition
CDC, National Diabetes Statistics Report, 2017
CASE 1
A case of adolescent obesity
3CASE 1
18 year old man presents for evaluation of
abnormal TSH and weight gain
• He has no significant past medical history
• He has no symptoms of hypothyroidism
• He denies polyuria, polydipsia, or fatigue
• He enjoys playing video games
• His family history:
– hyperlipidemia and hypertension (father)
– Mother with gestational diabetes
– diabetes and hyperlipidemia (PGF)
– thyroid disease (MGF and p. aunt)
– Hispanic ethnicity
CASE 1
Exam: Lab results:
BMI: 29 TSH 6.29; Free T4 2.2
Mild acanthosis nigricans Cholesterol 196,
of neck Triglycerides 748, HDL 23
4CASE 1 Repeat labs: TSH 3.43, Free T4 0.99 Thyroid peroxidase Ab 34.8 Thyroglobulin Ab
CASE 1
Diabetes Screening Guidelines for Adults
Overweight (BMI ≥ 25)*
Plus additional risk factors
Physical inactivity
First‐degree relatives with diabetes
High‐risk ethnicity
Women who delivered baby >9 lb or who were diagnosed with GDM
Hypertension (≥ 140/90 or on therapy for hypertension)
PCOS
A1C ≥ 5.7%, IGT, or IFG on previous testing
Other clinical conditions associated with insulin resistance (severe
obesity, acanthosis nigricans)
History of CVD
In absence of above, screen starting at age 45 years
Repeat testing at 3‐year intervals if normal; more frequent testing if
higher risk or pre‐diabetes (yearly)
*At risk BMI may be lower in some ethnic groups.
CASE 1
Diabetes Screening Guidelines for Adults
Overweight (BMI ≥ 25)*
Plus additional risk factors
Physical inactivity
First‐degree relatives with diabetes
High‐risk ethnicity
Women who delivered baby >9 lb or who were diagnosed with GDM
Hypertension (≥ 140/90 or on therapy for hypertension)
PCOS
A1C ≥ 5.7%, IGT, or IFG on previous testing
Other clinical conditions associated with insulin resistance (severe
obesity, acanthosis nigricans)
History of CVD
In absence of above, screen starting at age 45 years
Repeat testing at 3‐year intervals if normal; more frequent testing if
higher risk or pre‐diabetes (yearly)
*At risk BMI may be lower in some ethnic groups.
6CASE 1
Would you screen him for diabetes?
A) No, he is asymptomatic for
symptoms of hyperglycemia
B) No, he is too young to have Type
2 diabetes
C) Yes, he is obese, he has multiple
risk factors for type 2 diabetes
CASE 1
Prediabetes
• Impaired fasting glucose and
impaired glucose tolerance
are risk factors for
development of diabetes and
cardiovascular risk
• Associated with dyslipidemia
with elevated triglycerides
• low HDL,
• And hypertension
7CASE 1
Prediabetes • Fasting glucose 108
• A1C 6%
8CASE 1: Prediabetes
Lifestyle intervention (n = 1079):
• Weight loss ≥ 7% through low
cal/low fat diet
• ≥150 minutes/week of exercise
moderate intensity
Metformin 850 mg bid (n = 1073)
CASE 2
A case of increased thirst…
9CASE 2
• A 60 year old woman returns for
follow‐up of asymptomatic
primary hyperparathyroidism
• She notes increased fatigue,
thirst, and urination
• She has a past medical history of
discoid lupus, hypertension, CKD,
COPD, coronary artery disease,
and depression
CASE 2
• She smokes a half pack
a day and drinks 4‐5
beers on the weekends
• She has a family history • Exam:
of diabetes,
• b.p. 122/82
hyperlipidemia, and
hypertension in her • BMI 28
brother • She has acanthosis
nigricans noted on the
back of her neck.
10CASE 2
• Lab results:
– Calcium of 10.2 mg/dl
– PTH 82.4 pg/ml,
– 25‐OH vitamin D 25.4 ng/ml
However, you note that her
chemistry also shows…
Glucose 248 mg/dl
What is her diagnosis?
CASE 1
Diagnosis of Diabetes
A1C ≥ 6.5%*
OR
FPG ≥ 126 mg/dL *
OR
2‐hour PG ≥ 200 mg/dL* during an OGTT
OR
In patient with classic symptoms or hyperglycemic
crisis, random plasma glucose ≥ 200 mg/dL
A1C 6.6%
*In absence of unequivocal hyperglycemia, result
should be confirmed by repeat testing
11Classification of Diabetes
Classification of Diabetes Features
Type 1 diabetes β‐cell destruction leading to absolute
A. Immune mediated insulin deficiency
B. Idiopathic
Type 2 diabetes Insulin resistance +/‐ insulin deficiency
Other specific types A. Genetic defects of β‐cell funtion
B. Genetic defects in insulin action
C. Diseases of exocrine pancreas
D. Endocrinopathies
E. Drug or chemical induced
F. Infections
G. Uncommon forms of immune‐
mediated diabetes
H. Other genetic syndromes associated
with diabetes
Type 1 Diabetes
• 50% of patients diagnosed before age 20 years
• 50% of patients diagnosed after age 20 years
– Often mistaken for type 2 diabetes—may make up 10%
to 30% of individuals diagnosed with type 2 diabetes
• Type 1 diabetes is due to autoimmune ß‐cell destruction
– leading to absolute insulin deficiency
EURODIAB ACE Study Group. Lancet. 2000;355:873‐876;
Naik RG, Palmer JP. Curr Opin Endocrinol Diabetes. 1997;4:308‐315
12Type 1 Diabetes
Stage 1 Stage 2 Stage 3
Stage • Autoimmunity • Autoimmunity • New‐onset
• Normoglycemia • Dysglycemia hyperglycemia
• Presymptomatic • Presymptomatic • Symptomatic
Diagnostic • Multiple • Multiple antibodies • Clinical symptoms
Criteria autoantibodies • FPG 100‐125 mg/dl • FPF ≥ 126*
• No IGT or IFG • 2‐h PG 140‐199 • 2‐h PG ≥ 200*
mg/dl • A1C ≥ 6.5%*
• A1C 5.7‐6.4% or • Classic symptoms,
≥10% increase hyperglycemic crisis
Consider referring first degree relatives of those with type 1 DM to risk assessment
in clinical research study: www.diabetestrialnet.org
EURODIAB ACE Study Group. Lancet. 2000;355:873‐876;
Naik RG, Palmer JP. Curr Opin Endocrinol Diabetes. 1997;4:308‐315
Type 2 Diabetes:
Pathogenesis in a Nutshell
13CASE 2
Classification of Diabetes Features
Type 1 diabetes β‐cell destruction leading to absolute
A. Immune mediated insulin deficiency
B. Idiopathic
Type 2 diabetes Insulin resistance +/‐ insulin deficiency
Other specific types A. Genetic defects of β‐cell funtion
B. Genetic defects in insulin action
C. Diseases of exocrine pancreas
D. Endocrinopathies
E. Drug or chemical induced
F. Infections
G. Uncommon forms of immune‐
mediated diabetes
H. Other genetic syndromes associated
with diabetes
Type 2 Diabetes: Pathogenesis in a
Nutshell (cont.)
14Natural History of Type 2 Diabetes
Impaired Undiagnosed
glucose tolerance diabetes Known diabetes
Insulin resistance
Insulin secretion
Postprandial glucose
Fasting glucose
Microvascular complications
Macrovascular complications
Adapted from Ramlo‐Halsted BA, Edelman SV. Prim Care. 1999;26:771‐789
Etiology of Type 2 Diabetes
Impaired Insulin Secretion and Insulin Resistance
Genes and environment
Impaired insulin
Insulin resistance
secretion
Impaired glucose
tolerance
Type 2 diabetes
Progressive hyperglycemia
and high free fatty acids
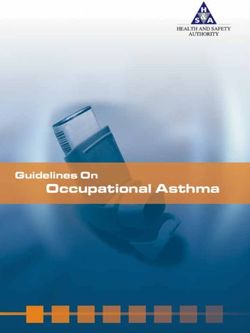
15Eight Mechanisms Which Lead to
Hyperglycemia in Type 2 Diabetes
1. Beta cells: Decreased insulin
Secretion
2. Skeletal Muscle: Decreased
Glucose Uptake
3. Adipose Tissue: Increased lipolysis
4. Alpha cells: increased glucagon
5. Liver: increased hepatic glucose
production
6. Neurotransmitter dysfunction
7. Decreased incretin effect
8. Increased glucose reabsorption
Illustration by Kaitlin Jones
Hyperglycemia In Type 2 Diabetes
Insulin Resistance: Receptor And Postreceptor Defects
Increased Glucose Insufficient Glucose
Production Disposal
Glucose
X
Liver Peripheral Tissues
(skeletal muscle)
Pancreas
Impaired Insulin Secretion
DeFronzo et al. Diabetes Care. 1992;15:318-368.
16Beta Cells of Pancreas Secrete Less
Insulin
Decline of ‐Cell Function in the
UKPDS Illustrates Progressive Nature
of Diabetes
‐cell function100 Time of diagnosis
(% of normal by ?
HOMA) 80
60
40
Pancreatic function
= 50% of normal
20
0
10 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6
Years
HOMA=homeostasis model assessment
Adapted from Holman RR. Diab Res Clin Pract. 1998;40(suppl):S21‐S25;
UKPDS. Diabetes. 1995;44:1249‐1258
17Altered ‐Cell Mass and Function in Islets From
Subjects With Type 2 Diabetes
Decreased Skeletal Muscle Glucose
Uptake
18Insulin Resistance and Skeletal Muscle
Insulin mediated glucose clearance rates in leg skeletal muscle
Dela, Int J Biochem & Cell Biology. 2013, 45: 11‐15.
Increased Lipolysis by Adipose Tissue
19Mechanism of Glucotoxicity and
Lipotoxicity
The Glucosamine Hypothesis
Glucose FFA
Glucose FFA
Other Increased Other
pathways glucosamine pathways
Impaired insulin Insulin resistance
secretion from ‐cell in muscle and fat
FFA=free fatty acid
Hawkins M et al. J Clin Invest. 1997;99:2173‐2182; Rossetti L. Endocrinology.
2000;141:1922‐1925
High FFA Levels Cause
Peripheral and Hepatic Insulin
Resistance
Glucose Measurements During High Insulin Levels
500 Insulin
Insulin + fat infusion
400
300 *
200 * *PIncreased Glucagon by Alpha Cells
Glucagon in Type 2 Diabetes
21Regulation of Postprandial Glucose
• A meal contains 6 to 20 times the glucose content of
the blood
• Normally, postprandial hyperglycemia is regulated by
– Clearance of ingested glucose by the liver
– Suppression of hepatic glucose production
– Peripheral clearance of glucose
Impaired Regulation of
Postprandial Glucose
• In impaired glucose tolerance or diabetes, glucose
regulation is impaired by
– Delayed and reduced insulin secretion
– Lack of suppression of glucagon
– Hepatic and peripheral insulin resistance
• Postprandial hyperglycemia results
22Increased Hepatic Glucose Production
Increased Hepatic Glucose Output
Correlates With Fasting Plasma Glucose
HGP observed via
Glucose output4.0 glucose
(mg/kg/min) turnover studies
3.5
during post absorptive
3.0 state
Normal
2.5 Type 2 diabetes
Conclusion:
FBG140. PNeurotransmitter Dysfunction
Energy Balance:
Afferent and Efferent Signals
24C
Substances That Promote Positive
Energy Balance (Weight Gain)
C
Substances That Promote Negative Energy
Balance (Weight Loss)
25Decreased Incretin Effect
Incretins and Glycemic Control
26Exenatide: Effect on the ‐Cell
Incretin Use
Schwartz, S. Postgraduate Medicine 2014, 5: 2757.
27Increased Glucose Reabsorption
Kidney
28CASE 2
• Lab results:
– Calcium of 10.2 mg/dl
– PTH 82.4 pg/ml,
– 25‐OH vitamin D 25.4 ng/ml
However, you note that her
chemistry also shows…
Glucose 248 mg/dl
What is her diagnosis?
Type 1 versus Type 2 Diabetes
Type 1 diabetes Type 2 Diabetes
Usual Clinical course Insulin‐dependent Initially non insulin‐
dependent
Usual age of onset 40 years but increasingly
20 years) earlier
Body weight Usually lean Usually obese
Clinical onset Often acute Subtle, slow
Ketosis‐prone Yes No
Family history ≤ 15% with first degree Common
relative
Ethnicity Predominantly white More common in
minorities
Frequency of HLD‐DR3, Increased Not increased
DR4, DQB1*0201, *0302
Islet Autoantibodies Present Absent
29CASE 2
• What is the next best step for this
patient?
A) Start a basal insulin
B) Start metformin
C) Diabetes education
D) Reassurance that her A1C is only mildly
elevated
E) B&C
F) None of the above
Type 2 Diabetes Agents
Agent Features
Metformin Low risk of hypoglycemia
Reduces hepatic glucose output, reduces GI side effects; risk of lactic acidosis
insulin resistance May see modest weight loss
Thiazolidinedione Low risk of hypoglycemia
Reduces insulin resistance in skeletal Fluid retention, increased fracture risk
muscle Weight gain
DPP‐4 Inhibitors Low risk of hypoglycemia
Increase endogenous GLP‐1 and GIP, Possible pancreatitis/pancreatic cancer risk
increasing endogenous insulin in glucose‐ Weight neutral
dependent fashion
GLP‐1 agonists Low hypoglycemic risk
Stimulates insulin through glucose‐ Possible pancreatitis; C‐cell hyperplasia in
dependent process; reduces glucagon and rodents
slows gastric emptying Weight loss
Sulfonylureas/Glinides Hypoglycemia risk
Release of insulin from beta cells Weight gain
30Type 2 Diabetes Agents
Medication Features
Alpha‐glucosidase inhibitors Bloating, flatulence, diarrhea
Inhibits polysaccharide absorption
Sodium‐glucose cotransporter 2 inhibitors Low risk of hypoglycemia
(SGLT2) Urinary and GU infections
Inhibition of glucose reabsorption in Weight loss
kidneys
Bromocriptine Mesylate Low hypoglycemia risk
Short acting dopamine agonist Nausea and orthostasis
Cannot be used in patients on anti‐
psychotic medications
Colesevelam Low hypoglycemia risk
Bile acid sequestrant GI side effects
31CASE 2
• What is the next best step for this
patient?
A) Start a basal insulin
B) Start metformin
C) Diabetes education
D) Reassurance that her A1C is only mildly
elevated
E) B & C
F) None of the above
CASE 2
• Diabetes education
– Medical nutrition therapy
• Diet history revealed poor food choices including
regular soda, potato chips, hot dogs, candy, and
cookies
– Physical activity
– Tobacco counseling
– Recommendation of yearly eye exam and
dental care
– Encouraged follow‐up of hypertension and
hyperlipidemia
32CASE 3
A case of childhood obesity
CASE 3
7 year old girl presents for evaluation of
abnormal TSH and weight gain
• She has no significant past medical history
• She has no symptoms of hypothyroidism
• She denies polyuria, polydipsia, or fatigue
• There is no history of gestational diabetes
in her mother
• Her family history:
– hyperlipidemia and hypertension (father)
– diabetes and hyperlipidemia (PGF)
– thyroid disease (MGF and p. aunt)
33CASE 3
Exam: Lab results:
BMI 26.9 (99th percentile TSH 6.29; Free T4 2.2
for age); 111/52 Cholesterol 196,
Mild acanthosis nigricans Triglycerides 748, HDL 23
of neck
She is pre‐pubertal
CASE 3
Repeat labs:
TSH 3.43, Free T4 0.99
Thyroid peroxidase Ab 34.8
Thyroglobulin AbCASE 3
Criteria for Screening for Type 2 Diabetes in Children
Overweight (BMI >85th percentile, weight for height >85th
percentile, or weigh >120% of ideal for height
Plus 2 of the following:
Family history of type 2 diabetes in 1st or 2nd degree relative
Race/ethinicity (Native American, African American, Latino,
Asian American, Pacific Islander)
Signs of insulin resistance or conditions associated with insulin
resistance (Acanthosis nigricans, hypertension, dyslipidemia,
PCOS, born SGA)
Maternal history of diabetes or gestational diabetes during
child’s gestation
Age of initiation: 10 years or onset of puberty
Frequency: every 3 years
Glucose 103, A1C 5.7%
CASE 3
Prediabetes
35CASE 3
The family was counseled on
lifestyle intervention, and she
was referred to a multi‐
disciplinary clinic for childhood
obesity
CASE 3
She returned 4 months later:
• She lost 7lbs but family reported no recent
efforts at lifestyle modification due to recent
death in the family, winter weather, etc.
• She had been ill and was diagnosed with Strep
throat so she had not been eating well due to
sore throat
• She had been complaining of some abdominal
pain
• She had some possible increased thirst and
urination but this was thought to be related to
trying to soothe her sore throat
36CASE 3
Labs done 2 months prior:
• Cholesterol 199, Triglycerides
260, HDL 37, LDL 110
• Glucose 103, insulin 19.5
CASE 3
Would you repeat screening for diabetes?
A) No, recent screening showed IFG
B) Yes, she has weight loss and possibly
some increased thirst and urination in
the setting of past IFG
C) No, she is pre‐pubertal and therefore
low risk for Type 2 diabetes
37CASE 3
Would you repeat screening for diabetes?
A) No, recent screening showed IFG
B) Yes, she has weight loss and possibly
some increased thirst and urination in
the setting of past IFG
C) No, she is pre‐pubertal and therefore at
low risk for Type 2 diabetes
CASE 3
A1C and glucose were checked in clinic:
• Glucose: 403
• A1C: 10.4%
• Urine dipstick: negative ketones
Diagnosis: Diabetes mellitus—Type 1 diabetes or Type 2 diabetes
38CASE 3
She was admitted to the hospital for
initiation of insulin and diabetes education:
• She was started on 0.6 units/kg/day for
doses of a basal‐bolus regimen
• Glargine 13 units hs, and Aspart 1/20g
• She was seen by the diabetes educator,
registered dietician, and social worker
• Family committed to increased efforts at
lifestyle modification
CASE 3
Six weeks later, she returned to
clinic having tapered off of insulin:
• 11 pound weight loss and poor
appetite
• A1C improved to 7.5%
• Diabetes antibodies positive:
– Glutamic acid decarboxylase Ab
>250
– Human insulin Ab 0.5
39CASE 3
Classification of Diabetes Features
Type 1 diabetes β‐cell destruction leading to absolute
A. Immune mediated insulin deficiency
B. Idiopathic
Type 2 diabetes Insulin resistance +/‐ insulin deficiency
Other specific types A. Genetic defects of β‐cell funtion
B. Genetic defects in insulin action
C. Diseases of exocrine pancreas
D. Endocrinopathies
E. Drug or chemical induced
F. Infections
G. Uncommon forms of immune‐
mediated diabetes
H. Other genetic syndromes
associated with diabetes
Classification of Diabetes
Classification of Diabetes Features
Type 1 diabetes β‐cell destruction leading to absolute
A. Immune mediated insulin deficiency
B. Idiopathic
Type 2 diabetes Insulin resistance +/‐ insulin deficiency
Other specific types A. Genetic defects of β‐cell funtion
B. Genetic defects in insulin action
C. Diseases of exocrine pancreas
D. Endocrinopathies
E. Drug or chemical induced
F. Infections
G. Uncommon forms of immune‐
mediated diabetes
H. Other genetic syndromes associated
with diabetes
40Ketosis‐prone Type 2 Diabetes
• “Flatbush diabetes”, area in city of Brooklyn, NY where this
type of DM first described
• Commonly nonwhite and overweight or obese with acute
defects in insulin secretion and no islet cell autoantibodies
• Following treatment, some insulin secretory capacity is
recovered
• Initially Rx with insulin, then treated as type 2 diabetes with
oral agents +/or diet
Up to Date. Syndromes of ketosis‐prone diabetes mellitus. January 2017.
Latent Autoimmune Diabetes in
Adults (LADA)
• Heterogeneous group
• On spectrum of insulin deficiency between type 1 and type 2
diabetes
• Those with high titers of GAD65 antibodies have lower body
mass index and less endogenous insulin secretion
• Anti‐GAD antibodies (or ICA) indicate need for insulin and
increase risk for developing ketoacidosis
Up to Date. Classification of diabetes mellitus and genetic diabetic syndromes, 2017.
41Maturity Onset Diabetes of the Young
(MODY)
• Heterogeneous disorder characterized by non‐insulin dependent
diabetes diagnosed at a young age (Genetic Syndromes Associated with
Diabetes Mellitus
Thomas, CC. Med Clin N Am. 99 (2015): 1‐16.
Drug Associated Diabetes Mellitus
Thomas, CC. Med Clin N Am. 99 (2015): 1‐16.
43Newer Atypical Antipsychotics
• Side effects: weight gain
• Diabetogenic effects: glucose dysregulation
– Clozapine
– Olanzapine
– Risperidone
– Quetiapine
– Aripiprazole
• Increased risk of T2DM, metabolic syndrome and
dyslipidemia
• Rare cases of DKA
Guenette, et. al. Psychopharmacology. 2013, 226: 1‐12.
Summary of Pathophysiology
• Type 1 diabetes
– The main abnormality is insulin deficiency
• Type 2 diabetes
– Both insulin deficiency and insulin resistance
contribute
• Glucotoxicity and lipotoxicity
– Poor metabolic control worsens insulin deficiency and
insulin resistance
44Summary of Pathophysiology
• Basal hyperglycemia
– Basal insulin levels and hepatic response mainly
determine fasting plasma glucose
• Postprandial hyperglycemia
– Early insulin release, glucagon suppression, and hepatic
and muscle responses to insulin response determine
postprandial glucose
Questions?
45You can also read