DIABETES CARE BEST PRACTICES COMPENDIUM - CENTER FOR BEST PRACTICES MEDICAID HEALTH PLANS OF AMERICA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Medicaid Health Plans of America
Center for Best Practices
Diabetes Care
Best Practices Compendium
DIABETES
CONTROL
table of contents | 3
Table of Contents
Welcome
About the MHPA Center for Best Practices ........................................................................................................................... 5
Welcome Letter: A Message from Michelle Martin ............................................................................................................. 7
Chapter 1: About Diabetes ................................................................................................................................................. 8
Chapter 2: Diabetes Prevention ........................................................................................................................................ 12
Chapter 3: Reducing Diabetes Racial and Ethnic Disparities..................................................................................... 13
Chapter 4: Medicaid Health Plans – Innovations in Improving Diabetes Care ................................................... 16
Chapter 5: Health Plan Best Practices ............................................................................................................................. 21
Buckeye Community Health Plan and AT&T mHealth Solutions Presents DiabetesManager®
[Buckeye Community Health Plan (Centene® Corporation) and AT&T/WellDoc]................................................ 21
Community Health Worker Program (UPMC for You) ........................................................................................................ 24
Diabetes Control Network (Midwest Health Plan) ............................................................................................................... 25
Diabetes Education for SMI [Nurse Wise/Nurse Response (Centene)] ............................................................................. 28
Diabetes Total Wellness Initiative: Learning to Live and Thrive with Diabetes (Amerigroup Maryland) ..................... 29
Drug Therapy Management (DTM) Program for Diabetics (PerformRx, AmeriHealth Mercy Health Plan and
Keystone Mercy Health Plan) ................................................................................................................................... 31
Get Control It Matters (Delaware Physicians Care, An Aetna Health Plan) ..................................................... 34
HealthConnections: Community-Based Disease Management Pilot - Diabetes (WellCare Health Plans, Inc.) .......... 37
Healthy Families Program (Amerigroup Corporation) ........................................................................................................ 38
In Control Diabetes Care Management (Select Health of South Carolina) ....................................................................... 40
MDwise Rewards Program (MDwise, Inc.) ........................................................................................................................... 41
The mHealth Program (DC Chartered Health Plan, Inc.) ................................................................................................... 43
Monitoring for Risk of Metabolic Syndrome (Value Behavioral Health of Pennsylvania) ............................................. 45
Nurtur’s Diabetes Program (Centene® Corporation) ............................................................................................................ 48
VSHP Diabetes Gaps-In-Care (Volunteer State Health Plan and BlueCross BlueShield of Tennessee) ......................... 49
YOU Count (Health Partners of Philadelphia, Inc.) ............................................................................................................. 51
Chapter 6: Diabetes Resources ........................................................................................................................................... 52
4 | Diabetes Care Best Practices Compendium Welcome | 5
MHPA Center for Best Practices
Best Practices Compendium on Diabetes Care
By Liza Greenberg, RN, MPH, MHPA Senior Consultant, Clinical Initiatives
Layout and design by Karen Seidman, Seidman Says Communications
~~~
The MHPA Center for Best Practices thanks the member plans that submitted best
practices for this publication. We are also grateful to the other MHPA members
who offered guidance, insights and comments on drafts of this document. About MHPA Center for Best Practices
Any errors in this compendium are the responsibility of the author.
The Medicaid Health Plans of America (MHPA)
Center for Best Practices (CBP) is a 501(c)(3) affiliate
~~~ organization created to support MHPA’s mission: to
provide efficient health care services and improve
Supported by an educational grant from Roche Diagnostics quality and access to care for Medicaid beneficiaries.
The CBP serves as a convener of Medicaid health
plans on research, quality improvement and
dissemination of health plan best practices in
both clinical and operational domains. With
guidance from the leadership of premier health
~~~ plans serving Medicaid populations and expert
stakeholders, the CBP uses data, information and
Copyright © 2013 knowledge transfer to disseminate innovative
Medicaid Health Plans of America Center for Best Practices solutions to caring for underserved populations.
~~~
MHPA Center for Best Practices
1150 18th Street, NW
Suite 1010
Washington, DC 20036
Tel: (202) 857-5720 | Fax: (202) 857-5731
info@mhpa.org | www.centerforbestpractices.org
6 | Diabetes Care Best Practices Compendium welcome | 7
Welcome Letter
A Message from the MHPA Center for Best Practices Director
Michelle M. Martin
Dear Colleagues:
On behalf of the MHPA Center for Best Practices, I am pleased to bring you this
Diabetes Care Best Practices Compendium. Diabetes is one of the most common
chronic diseases affecting members of Medicaid plans. More than 8% of the U.S.
population has diabetes and the risk of diabetes is higher in low income and some
minority groups — precisely the populations served by Medicaid health plans.
One of the key objectives of Medicaid health plans is to close these health care
quality gaps and reduce disparities.
This publication provides information on best practices in diabetes care and
highlights programs from MHPA health plans and partner organizations.
These descriptions illustrate efforts to educate, engage, and ensure high-quality
treatment for Medicaid enrollees with diabetes. Plans are offering specialized
programs to identify members with diabetes, link them with care managers and health care services, and
measure changes in delivery of essential diabetes treatments. Health plans are also taking a leadership role in
working with communities to improve health and prevent diabetes. Plans also educate physicians and other
health care providers, and often use health plan data to show providers where members are lacking in diabetes
care. These patient- and provider-directed efforts help to narrow the gaps in diabetes care quality.
Prevention of diabetes is a key area of emphasis for health plans. Medicaid health plans have a variety of diabetes
prevention programs and collaborations to promote physical activity, encourage healthy eating, and help people
maintain a healthy weight. Health plan prevention approaches are multi-faceted and include community-
based strategies, programs to support clinicians in improving care, and programs to educate patients. These
interventions are critical to stem the rising tide of diabetes.
This publication offers information for Medicaid health plans, state leaders, and other policymakers. It also lists
resources with website links that can help readers find information about preventing and managing diabetes.
We commend the health plans featured in this publication and encourage all stakeholders to work together in
the fight against diabetes.
Sincerely,
Michelle M. Martin
Director,
MHPA Center for Best Practices
8 | Diabetes Care Best Practices Compendium Narrative | 9
to both lifestyle and medication recommendations remains
Chapter 1: About Diabetes low. The statistics outlined below demonstrate how diabetes
contribute to poor health outcomes. For example, according
to the National Institutes of Health:
Diabetes is a critical health issue for the United States and for Medicaid health plans. An estimated 26 million, Adults with diabetes have heart disease death rates
or approximately 8% of U.S. residents have diabetes. That number is higher among racial and ethnic minority about two to four times higher than adults without
populations; almost 13% of adult African-Americans and 12% of Hispanic populations have been diagnosed with diabetes.
diabetes. Diabetes is also more prevalent in the elderly and low income populations — meaning that it is an The risk for stroke is two to four times higher among
important issue for health plans serving these Medicaid beneficiaries. people with diabetes.
Also of great concern is the potential for future cases of type 2 diabetes: 35% of adults over 20 have signs and Up to 67% of diabetics have blood pressure greater
symptoms of prediabetes. Prediabetes may progress to type 2 diabetes unless people adopt healthy behaviors. It than or equal to 140/90 mmHg or use prescription
is often reversible through changes in diet and exercise resulting in weight loss. medications for hypertension.
Diabetes is the leading cause of new cases of
Obesity is a key driver of diabetes. With a third of the population now clinically obese, the toll of diabetes may blindness among adults ages 20–74 years.
continue to rise. Some racial or ethnic minority groups are at particularly high risk for the development of diabetes Diabetes is the leading cause of kidney failure, with
related to obesity. Preventing obesity as a nation, and treating weight problems for individuals with diabetes almost 50,000 new cases each year.
and prediabetes is an essential strategy. It is a national priority to improve nutrition and lifestyle — starting in
childhood — to prevent obesity. National efforts to prevent diabetes often focus on developing programs and Standards of Care for Diabetes 60-70% of people with diabetes have mild to severe
neuropathy (nerve damage), and 60% of non-
policies that will create a healthy environment that prevents obesity.
traumatic amputations are in people with diabetes. 1
Type 2 diabetes is a complex and
progressive condition. Treatment requires
control of the diabetes-specific symptoms
What is Diabetes? – high or low blood sugar – and also careful How Can Diabetes be Treated
Type 1 diabetes stems from the body’s inability to make insulin which helps process glucose (sugar) for energy. attention to preventing and treating More Effectively?
Type 1 represents a small percentage (5-10%) of all persons with diabetes. Type 2 diabetes is the most common complications.
form of diabetes. Type 2 diabetes is the result of both reduced insulin secretion and reduced insulin effectiveness, The goal of treatment for type 2 diabetes is maintaining near
conditions known as insulin resistance. Because insulin is necessary to metabolize glucose in the body, absent or Each year additional research results in new normal or target range blood sugar levels and preventing
insufficient insulin results in high blood sugar (hyperglycemia). recommendations for diabetes treatment. complications. Successful management includes both
The American Diabetes Association has medical interventions and patient adoption of a healthy
Type 2 diabetes can sometimes be taken the lead in convening physicians lifestyle with nutritious eating and regular exercise. High
controlled with diet and exercise, and other diabetes experts to establish quality diabetes care is often called “evidence-based care”
but medications are often required. standards of care for diabetes. because it is consistent with treatment that research evidence
Type 1 must be treated with insulin. shows will produce the best health outcomes. Treatment
Controlling diabetes will prevent In 2012 the American Diabetes Association goals for type 2 diabetes include:
damage to other body systems, partnered with the European Association
for the Study of Diabetes and issued new Hemoglobin A1c (HbA1c) control, with checks
including end stage kidney disease
recommendations on delivering treatments every three to six months
and blindness. Diabetes treatment also
focuses on controlling hypertension that meet the needs of specific types of Blood pressure control at 130/80 mm/Hg or lower
and elevated cholesterol, which lowers patients such as the elderly, chronically Cholesterol and triglyceride levels management
the patient’s risk for cardiovascular ill, and newly diagnosed. This is a change with annual checks
disease linked to diabetes. from prior treatment guidelines that had (LDL cholesterol levels below 70-100 mg/dL)
a uniform HbA1c management goal for all Annual kidney function tests (microalbuminuria
patients. and serum creatinine)
Annual eye exams to check for diabetic eye disease,
Why So Much Emphasis on Links to the 2012 standards, along with or more frequently as needed
Diabetes Care? a summary of changes and tools to Regular dental cleanings and exams
help physicians quickly identify care Smoking cessation treatment, if needed
Diabetes affects the health and management goals, are identified in the Adoption of regular exercise program
productivity of the patients and families Resources section of this Compendium.
who live with it. For most people, type Diabetes self-management education
2 diabetes is a progressive disease that
triggers a cascade of “co-morbidities”
or other health problems. Despite _________________________
knowledge of effective strategies to 1 http://diabetes.niddk.nih.gov/dm/pubs/statistics/#pdc
manage diabetes, treatment adherence
10 | Diabetes Care Best Practices Compendium Narrative | 11
Recommendations for treatments are reviewed and updated
each year by expert panels of the American Diabetes
Association. Medication treatments are intensified as Amerigroup Georgia AbsoluteCARE Quality Program
needed to achieve short-term blood glucose control, and to
affect a measure of long-term control called hemoglobin A1c
(or HbA1c). For patients who already have complications The AbsoluteCARE Quality Program, an Avesis company,
such as high blood pressure or eye problems, additional offers a specialized patient-centered medical home for
treatments are needed to prevent worsening of the members with medical conditions such as diabetes and
conditions. hypertension who do not have a strong, established
Patients with type 2 diabetes are generally treated either relationship with a primary care physician.
with “oral hypoglycemics” (pills to control blood sugar), or The medical home, created for these members through this pilot program, represents a
injectable insulin, along with lifestyle changes such as better
nutrition, exercise, and weight control. If blood glucose is comprehensive approach towards care that includes healthcare, wellness and prevention
Coordinated Care in not adequately controlled, additional medications may need services. This pilot program was developed as a solution to members who were in need
to be added over time. Patients may need insulin earlier if of recurring healthcare services but were disconnected from a primary care provider. This
Medical Homes May blood sugar cannot be controlled with lifestyle changes and approach incorporates disease management services into a comprehensive, integrated
Improve Diabetes Care medical therapy. patient centered medical home. The AbsoluteCARE Quality Program yielded extremely
For people who are severely overweight with a Body promising results. Average per member per month spending decreased by over 30%
Best practice approaches to diabetes Mass Index (BMI) of 35 or over and who also have poorly during the evaluation period. The most significant driver of savings was a decrease in
care often involve a multidisciplinary controlled diabetes, obesity surgery may also be part of the
team. This enables providers to offer inpatient care though spending increased for primary care services and prescription drug
treatment plan. Bariatric surgery, as it is called, has been
effective interventions across the shown to reverse diabetes in up to 80% of patients. However, spending. Emergency room visits decreased by over 45% among participants after the
diverse elements of diabetes self-care. bariatric surgery does have its own risks and complications. referral to AbsoluteCARE was made and members opted into the program.
Together these specialists cover: These must be weighed against the risk of complications
that occur with type 2 diabetes.
Nutrition and exercise
Weight management
Medication management Quality Gaps in Diabetes Care Provider Factors: Diabetes care is complex and requires visits to several different types of providers.
Prevention and smoking Physicians or other providers may not offer the proper treatments, tests and checks to manage
cessation In spite of the research showing the health consequences of diabetes, they may not intensify treatment when it is needed, or may not offer the right education that
Other diabetes self-care uncontrolled diabetes, patients very often do not get the best patients need to “self-manage” their care.
behaviors quality care. These gaps in care may be the results of any
combination of factors: Patient Factors: Patients may have language barriers, low literacy, depression or other mental health
problems that make it difficult to understand or carry out their treatments. Some patients may not be
In recent years many provider practices Health care system factors: The current health care ready to make lifestyle changes such as healthier eating or exercising and/or patients may experience
have adopted a model known as the system is not conducive to working through the health system/social barriers that affect adherence. All of these factors result in less than optimal “self-
“patient centered medical home.” significant barriers experienced by patients with management,” e.g. the eating, exercising, and health management activities needed to successfully
Medical homes are practices that have diabetes: visits are short, often acute illness prevents manage diabetes.
redesigned their office operations to attention to routine chronic health care needs, and
be more accessible to patients and to the system may not be set up to deliver culturally Social Factors: Patients may not have insurance coverage for the health services, medications, family
offer the full scope of multidisciplinary appropriate care. Often, care is poorly coordinated support or other support services they need to effectively manage diabetes. The Medicaid program
care needed by patients with diabetes between the various physicians, hospitals, and other makes important strides to ensuring health care access, but members may have disruptions in care
and other chronic conditions. Medical providers treating the patient. There may also be when they lose eligibility for the program.
homes also adopt more sophisticated missed opportunities to improve adherence with
The sections below illustrate how each of the key stakeholders – patients, physicians and other providers, and
information systems to enable them visits and treatments and to deliver preventive
health plans – can influence better diabetes care.
to more effectively track and meet treatments and counseling needed during visits.
patient’s health care needs and
integrate health information with that
of hospitals and specialty providers.
Many experts believe that providing
more coordinated care and helping
members to develop connections with
their medical providers will improve
diabetes care quality.
12 | Diabetes Care Best Practices Compendium Narrative | 13
Chapter 2: Diabetes Prevention While this compendium does not focus on diabetes prevention, a few of the health plan best practice examples in this
Prevention related to diabetes takes place on two levels. First, “primary prevention,” — preventing diabetes entirely — is publication describe plans’ community-based prevention strategies. In addition, the MHPA Center for Best Practices
an important goal. Second, for people who already have diabetes, preventing worsening of the disease or progression to Treatment Adherence Best Practice Compendium includes a number of outstanding examples of health plans’ community-
heart and vascular complications is an important goal. “Secondary prevention,” as it is called, is achieved by implementing based prevention initiatives. The compendium is available free from the CBP’s website, www.centerforbestpractices.org.
appropriate screening guidelines to ensure early identification of people who have diabetes, and by providing evidence-based Secondary Prevention: Prevention of complications of diabetes is the key objective in secondary prevention. Effective
diabetes care, which includes careful attention to preventing complications. management of diabetes essentially is designed to prevent worsening and complications of disease. Diabetes treatment
Primary Prevention: Type 2 diabetes is challenging to control yet largely preventable. Prevention of obesity is an important goals include management of blood sugar and cardiovascular problems to prevent complications, and regular assessment for
tactic for prevention of diabetes. Although individuals are accountable for maintaining a healthy weight, availability of complications of diabetes.
healthy food, places to exercise, and a culture that supports health have an enormous influence on individual choices. The Early identification is a crucial element of diabetes treatment. Physicians evaluate risk of diabetes in the course of care and
Institute of Medicine in a report, Accelerating Obesity Prevention, recently identified five strategies that prevent obesity and deliver screening services. Health plans also have a role in identifying members who are high risk (through activities such as
which they recommended be the core of community and national policy efforts. These are: health risk assessments and health fairs) and connecting those members to physician care. High-quality diabetes care is one
Integrate physical activity every day in every way of the most effective strategies for preventing complications and co-morbidities. Most of the best practice examples in this
Market what matters for a healthy life compendium describe health plan initiatives to identify members with diabetes, screen them for diabetes care quality gaps,
Make healthy foods and beverages available everywhere and help them to successfully manage their diabetes.
Activate employers and health care professionals
Strengthen schools as the heart of health
Many communities and health plans focus on improving overall health through better eating, weight management, and
more exercise, as a key diabetes prevention strategy. The federal Diabetes Prevention Program (DPP) evaluated a variety of
Chapter 3: Reducing Diabetes Racial and Ethnic Disparities
programs to assess their effect on diabetes prevention. The DPP shows that prediabetes can be reversed. High-risk people
and communities can take concrete action steps such as losing weight and exercising regularly to prevent diabetes, and move Racial and ethnic minority groups often have a higher rate of chronic diseases including diabetes and also have more risk
from prediabetes back to a normal risk level. The DPP offers many resources and recommendations to help individuals and factors such as obesity, smoking, and lifestyles. According to the National Diabetes Education Program:
communities take action to avoid diabetes.
Non-Hispanic Whites: 15.7 million people, or 10.2 percent of all non-Hispanic whites aged 20 and older, have
From a health plan perspective, diabetes prevention activities must target both individuals and communities. People at-risk diagnosed and undiagnosed diabetes. 7.1 percent of all non-Hispanic whites aged 20 and older have diagnosed
for diabetes can be identified early through “health risk assessments” that identify lifestyle factors and family heritage that diabetes.
may put people at higher risk for diabetes. Communities at-risk can be identified through demographic data. Working to African-Americans: 4.9 million people, or 18.7 percent of all non-Hispanic blacks aged 20 and older, have diagnosed
care for high-risk individuals through care management, health promotion, and quality monitoring, health plans reduce risk and undiagnosed diabetes. 12.6 percent of all non-Hispanic blacks aged 20 and older have diagnosed diabetes.
of diabetes for members. Community efforts focus on helping to develop exercise, nutrition awareness, and other lifestyle Hispanics/Latinos: 11.8 percent of Hispanics/Latinos ages 20 or older have diagnosed diabetes. Among Hispanics/
improvement programs in the communities served by Medicaid health plans. Latinos, diabetes prevalence rates are 7.6 percent for both Cubans and for Central and South Americans, 13.3 percent
for Mexican Americans, and 13.8 percent for Puerto Ricans.
American Indians and Alaska Natives: About 16.1 percent of American Indians and Alaska Natives aged 20 years
Community-Based Prevention for Diabetes and older who are served by the Indian Health Service have diagnosed diabetes. Diabetes rates vary by region, from
5.5 percent among Alaska Natives to 33.5 percent among American Indians in southern Arizona.
MHPA member organization UnitedHealthcare announced in October that Asian-Americans: The rate of diagnosed diabetes in Asian Americans is 8.4 percent.
it is bringing JOIN for ME , a proven community-based, childhood obesity
sm
lifestyle-intervention program, to Medicaid beneficiaries who live in the
New Orleans area. Quality Evaluation for Health
JOIN for ME is a 12-month program that helps generally healthy children who are overweight or obese reach
sm
Medicaid health plans are taking action to reduce health care disparities. For example, many plans use community data to
healthier weights and reduce the risk of many related health issues. This evidence-based program emphasizes identify communities with the highest risk factors relating to age, race, income, and health status. Health plans can develop
whole-family lifestyle and behavior modification delivered in 16 weekly sessions, followed by monthly their own care management programs and partner with community organizations to develop culturally specific programs
maintenance sessions for up to one year. JOIN for ME , which engages the entire family, has demonstrated
sm
and information on prevention and health education.
promise to become a national model to meet the critical need for effective, accessible, and affordable treatment
Health plans also routinely examine their own health care data to identify disparities and develop culturally appropriate
for childhood obesity. prevention and treatment approaches. Many plans are making strides in improving the quality of data to enable them to
UnitedHealthcare and the Louisiana Alliance of Boys & Girls Clubs launched JOIN for ME at a Community
sm
evaluate quality by race and ethnicity. This will improve their ability to direct care to populations experiencing disparities in
Forum that served as a call to action for the community to join forces to fight the childhood obesity epidemic health outcomes.
that is taking a devastating toll on families, communities, and the country. UnitedHealthcare Community Plan
of Louisiana leaders noted that JOIN for ME will provide children with an engaging and practical solution that
sm
involves the entire family in adopting healthy eating and activity. Often, multiple members of the family lose
weight by making small changes in their daily routines. The initiative will help young people and their families
improve their health and quality of life.
Excerpted from: http://www.uhc.com/news_room/2012_news_release_archive/medicaid_program_fights_
childhood_obesity.htm
14 | Diabetes Care Best Practices Compendium Narrative | 15
Important strategies to reduce disparities include: Medicaid Health Plan Strategies to Measure and Reduce Disparities in Diabetes Care
Ensuring that data have enough information on race, ethnicity, and other patient factors to help analyze for
disparities In October 2012, the Medicaid Health Plans of America (MHPA) Center for Best Practices hosted a workshop on
Analyzing data to understand disparities strategies to ensure quality care and reduce disparities in diabetes
Developing culturally competent interventions care and outcomes. The AmeriHealth Mercy Family of Companies
Educating staff and providers on strategies for reducing disparities (AMFC) outlined some of the data on disparities in the Medicaid
Developing relationships with communities and individuals to build the trust needed for successful health population of Philadelphia, and discussed its strategies to reduce
partnerships, including use of peers and community health workers disparities.
Helping members to address their own priorities that may influence health, such as having adequate housing
or access to food AMFC examined information on the Medicaid-covered population
Seeking external guidance or standards to evaluate the organization’s cultural competency and identified 10 percent of adult members with diabetes. The
Preventing the chronic health conditions that underlie disparities in disease prevalence and outcomes. majority of members with diabetes are African-American and non-
Hispanic whites. Adult African-American members with diabetes
Disparities in care and outcomes occur in racial and ethnic minorities, and also in some high-risk populations were identified as more likely to have care gaps than other members. In addition, data showed high use of
such as the homeless, people with mental illness, or people in underserved communities. Many of the best emergency and hospital services. Of the adult African-American members with diabetes, 25.8 percent had at
practice examples in this publication describe health plan initiatives to meet the needs of specific populations with least one emergency room visit and 7.5 percent had at least one inpatient admission. This information shows
community-based services, peers, and culturally competent services. that more can be done to improve primary and outpatient care to reduce the need for hospital services.
AMFC adopted a number of strategies to reduce identified disparities. An example of these strategies includes:
Monitoring Healthcare Effectiveness Data and Information Set diabetes data by race and ethnicity to
identify gaps.
Collecting individual-level race, ethnicity and language data, in addition to population-level data
Reducing Diabetes Disparities in People with Serious Mental Illness evaluation strategies, to improve ability to analyze and meet member needs.
Providing cultural competency training to staff.
Value Behavioral Health of Pennsylvania (VBH-PA) implemented an intervention to increase the
monitoring of Medicaid patients with serious mental illness for risk factors related to metabolic As a result of adopting these strategies, AMFC’s health plans achieved the National Committee for Quality
syndrome, a precursor of diabetes. The initiative targets psychiatrists prescribing Second Assurance’s Multicultural Health Care Distinction.
Generation Atypical Antipsychotic Medications (SGAs). The goal is to increase screening for risk At the clinical level, AMFC interventions to reduce disparities include:
factors and improving coordination of care with primary care physicians. The program has resulted
in an increasing number of psychiatrists providing the appropriate screening and referrals to Intensified approach to members with diabetes with the highest number of emergency room and
primary care for their members with diabetes risk factors. Diabetes monitoring scores were 82 inpatient events, and on multiple medications.
percent in 2012, a dramatic increase from the 11% monitoring rate when the program began in Implementing home-based health care services and individualized member treatment plans to build
2006. VBH-PA providers are also improving in referring at risk members to primary care. trust with members, caregivers, and providers, as well as address “non-medical” issues, such as housing,
food, and the ability to adhere to treatment recommendations.
Adopting a multidisciplinary team approach to helping members and overcoming barriers. Teams
include physicians, behavioral health consultants and bilingual community health workers, with
additional services supplemented by a home health nurse, physical therapist, dietitian and pharmacist.
Case Study: Mr. S, a a boarding home resident suffering from unmanaged type 1 diabetes, had been in the
hospital for a total of 101 days during 15 different visits since the beginning of 2012. Mr. S was instructed
how to use a glucometer, and care managers monitored his daily insulin compliance in consultation with
his primary care physician and boarding home staff. During the intake process, the care management team
discovered Mr. S was living on a fixed income and made poor nutritional choices for a diabetic. He would
purchase a lot of junk food at the beginning of the month, but would then eat sparingly later in the month as
his funds began to run out until his next paycheck. Care managers arranged a stable source of food for Mr. S
in collaboration with a community resource that will also provide nutritional education. Since entering the
program at the end of June, Mr. S had only one 11-day visit to the hospital, and as of September 2012, had not
returned to the hospital in 66 consecutive days.
16 | Diabetes Care Best Practices Compendium Narrative | 17
Chapter 4: Medicaid Health Using care management programs to educate and support patients in making lifestyle choices that
Midwest Health Plan prevent and manage diabetes. Amerigroup’s AbsoluteCARE medical home initiative and the Select
Plan Innovations in Improving Diabetes Control Network: Health In Control program are examples of innovative care management programs.
Diabetes Care Midwest Health Plan created the
Engaging members with diabetes or those at risk for diabetes with prevention, treatment, and health
education programs. For example, Delaware Physicians Care (an AETNA Health Plan) Get Control
Diabetes Control Network to identify It Matters program uses innovative visual aids to show members a “Healthy Plate” and to help them
Diabetes affects both physical health and quality of life of members with diabetes and help understand healthy eating for diabetes prevention and control.
patients. States’ Medicaid costs for diabetes are high, and the improve care. The Diabetes Control
condition is challenging for physicians and other providers to Connecting with members on health education through interactive websites that offer health
Network identifies members with information, health risk assessments, and games. The Buckeye Community Plan’s collaboration with
identify and manage. Medicaid health plans are positioned diabetes through a comprehensive
to leverage their influence with a variety of stakeholders to AT&T on cell phone-based diabetes education shows how health plans are testing and trying out new
software system that supports technologies to improve health.
improve diabetes care.
Midwest Health Plan’s (MHP) disease
Health plans have an important role in using information, management, case management, and Offering diabetes disease management directly to patients in need of additional support and education.
patient and provider contacts, and payment incentives to utilization management functions. WellCare Health Plans, Inc. is implementing the HealthConnections: Community-Based Disease
improve diabetes care. Many health plans have developed care This system provides for an integrated Management Pilot in partnership with a Texas-based academic institution, with the goal of increasing
coordination programs to help members navigate their health and efficient way to identify members availability of trained practitioners to improve diabetes care.
care needs. Health plans also deliver “disease management” eligible for the program, stratify based Contracting with high-quality physicians and increasing patient awareness of high-quality diabetes
services that offer education, counseling, and information on on severity of disease, and track providers such as those recognized in diabetes care by NCQA.
treatment to members identified as having diabetes. member interventions. Members
enrolled in the Diabetes Control Partnering with physicians and other practitioners to help them understand opportunities to improve
Using data and information effectively is an important element diabetes care. Volunteer State Health Plan’s program to educate physicians on comprehensive diabetes
of finding which patients have or are at risk for diabetes, and Network receive information and other
care is an example of this approach.
helping to close gaps in quality for these groups. Health materials focusing on the disease
plans use their claims (provider bills) and enrollment data process and complications, medication Using incentives to encourage members to use high-quality providers and to participate in diabetes
systems to identify patients with diabetes and understand use and adherence, nutrition, caregiver management programs. The MDwise program and the Health Partners’ You Count program both
which services they are receiving. Health plans may also offer resources, self-management skills, include incentives for members to engage in prevention and health improvement behaviors.
“risk assessment” surveys online or in person to help patients treatment plan, lifestyle issues affecting
Collaborating with communities and community organizations such as schools, health departments
understand familial and behavioral factors that might put the disease state, depression, and
and fitness organizations to develop prevention and wellness programs. UPMC for You’s Community
them at risk of diabetes. Plans use this information to develop the importance of follow up with Health Worker Program hires members of the community to build trust and carry out a neighborhood-
patient and provider education and care management services physicians. Members also receive based health and wellness initiative.
that support the patients and improve care. reminders and incentives to complete
recommended diabetes visits and Partnering with states to carry out payment incentive demonstration programs to reward providers
Through use of data, health plans can also see whether for better quality care.
testing. Primary care providers receive
patients are going to their doctor for diabetic screening tests
and can alert providers and patients of needed care. For education and information to improve Medicaid health plans are accountable for their diabetes care results and report HEDIS measures to show
example, pharmacy claims serve as a source of information the diabetes services they provide their performance. Many state Medicaid programs use health plans’ HEDIS reports to produce health plan
on how frequently patients are refilling medications and to members. Midwest Health Plan performance report cards or other information for patients. The National Committee for Quality Assurance
whether they are getting essential medications. Plans use this has seen improvements in all HEDIS® also reports data on diabetes care quality. The following tables show health plan performance on multiple
information to address adherence to medications, either by measures for comprehensive diabetes diabetes indicators. The lower performance of Medicaid plans shows the challenges of working with a low-
alerting the doctor or contacting the member directly. They care during the past three years. income, high-disparities population. But, the steadily improving performance illustrates that plans’ strategies
may also identify safety concerns if there are duplicates or HbA1c testing increased from 82% to are evolving to effectively serve the Medicaid population.
drug interactions. The best practice example from PerformRx 93%; Eye exams increased from 60%
in this publication shows how one plan uses pharmacy data to 62%; LDL screening from 79% to
to identify members who have 15 or more prescriptions and 80%, and monitoring for nephropathy
helps those members get on the right medications. increased from 87% to 98%.
Some of the approaches health plans use to improve diabetes
care include:
Measuring the quality of care provided to members
with diabetes and developing focused efforts to
increase evidence-based care. All of the health plan
practices in this publication use measurement to
evaluate baseline and follow up improvements in
diabetes care, often using the HEDIS data set.
18 | Diabetes Care Best Practices Compendium 60 N A T I O N A L C O M M I T T E E F O R Q U A L I T Y A S S U R A N C E • E A R L Y E D I T I O N , O C T O B E R Narrative
2012 | 19
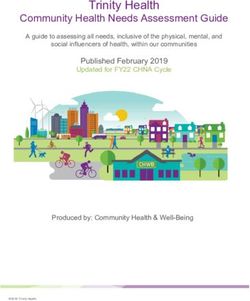
T H E S TAT E O F H E A L T H C A R E Q U A L I T Y 2 0 1 2 • H E D I S M E A S U R E S O F C A R E 59
The following charts were reprinted from the National Committee for Quality Assurance (NCQA)
from the “Focus on Obesity and on Medicare Plan Improvement” report.
The entire State of Health Care Quality, 2012 report can be accessed at:
http://www.ncqa.org/Portals/0/State%20of%20Health%20Care/2012/SOHC%20Report%20Web.pdf.
CHRONIC CONDITION MANAGEMENT
LDL CHOLESTEROL SCREENING LDL CHOLESTEROL CONTROL
(20 | Diabetes Care Best Practices Compendium Best Practices | 21
Chapter 5: Diabetes Care Best Practices Submissions
Buckeye Community Health Plan (Centene® Corporation) and
AT&T/WellDoc
Buckeye Community Health Plan and AT&T mHealth Solutions
Presents DiabetesManager®
description: This targeted pilot program initiative offered a group of high-risk diabetes patients
(cared for by Centene’s Buckeye Community Health Plan) access to AT&T mHealth Solutions Presents
DiabetesManager®, the enterprise mHealth solution from AT&T and WellDoc®. The FDA-cleared application
is a self-management tool that enables patients to manage their diabetes. Members can track food
consumption and blood sugar levels by logging their activity via a secure mobile application software. A group
of 59 program participants reduced their average hemoglobin A1c (HbA1c) results from 9.4% to 8.7% after
using the application. A decrease in hospital (-55%) and emergency room (-16%) utilization was also observed
in the program’s participants.
According to 2010 data from the CDC, it is estimated that 10.1% of Ohio adults have been diagnosed with
diabetes. In 2000, it was 6.5%. If current trends continue in Ohio as they have nationally, one in three
Ohioans will develop diabetes during their lifetime.
In adults, type 2 diabetes accounts for about 90 to 95% of all diagnosed diabetes cases. Inactive lifestyles,
obesity, and smoking are all contributing factors that may increase the risk of developing type 2 diabetes. A
2007 American Diabetes Association report indicated that the annual costs associated with diabetes in Ohio
were $5.9 billion, including $3.9 billion in medical expenditures and $2 billion in reduced state productivity
and premature mortality. The total charges of hospital discharges in 2007 with a primary diagnosis of diabetes
were approximately $442 million.
The WellDoc® DiabetesManager System was designed to address the health and cost issues associated with
diabetes in Ohio. The System is indicated for use in adults — aged 21 years and older — who have type 2
diabetes. It is designed to provide secure capture, storage, and transmission of blood glucose data as well as
information to aid in the support of diabetes self-management.
key objectives:
Enhance the patient experience of care (including quality, access, and reliability) by leveraging mobile
technology to improve diabetic member outcomes.
Improve quality of care in a specific clinical area (e.g. prenatal care, diabetes, asthma, etc.).
Make a positive impact in the care of individuals struggling to manage their diabetes by extending care
beyond the physician’s office.
actions taken: With the help of case managers and staff at Buckeye Community Health Plan, we identified
a pool of high risk type II diabetic members who were potential candidates for the program — with the final
pool of 200 type II diabetics that was also 50% minority. Candidates were identified through a coordinated
member enrollment initiative — sign-up events, invitation letters, member training, etc. Health plan staff
(i.e., case managers, coordinators, and other support staff) were trained on the phone application and portal
entry system. Work flows were then developed from a clinical, member support, and registration perspective.
Finally, metrics were selected to measure outcomes — for example, hemoglobin A1c tests, member
participation and engagement, emergency department and hospital admissions, etc.22 | Diabetes Care Best Practices Compendium Best Practices | 23
Once program participants were enrolled, they were trained on how to use the phone and the application for
entering blood glucose levels and other clinical information — carbohydrate consumption, activity, medications, etc.
Participants were required to make an average of seven blood glucose entries per week. Health plan case managers
and staff monitored activity and followed up as needed to address engagement issues and out of range blood sugar
results entered by members.
Of the 200 potential candidates for the program, 145 completed the pilot on the AT&T mHealth Solutions Presents
DiabetesManager® application. Of those individuals completing the program, we had 59 members with verifiable
hemoglobin A1c(HbA1c) readings prior to the start of the pilot.
outcomes:
A. For the group of 59 members with verifiable hemoglobin A1c (HbA1c) results prior to the start of the
program, we showed an average decrease in HbA1c from 9.4% to 8.7% after 1-5 months of using the mobile
application.
The hemoglobin A1c test is an important blood test used to determine how well a person’s diabetes is being
controlled. For people without diabetes, the normal hemoglobin A1c range is between 4% and 5.6%. In
uncontrolled diabetes, sugar builds up in the blood and combines with hemoglobin. Hemoglobin A1c levels
between 5.7% and 6.4% indicate increased risk of diabetes, and levels of 6.5% or higher indicate diabetes.
Because studies have repeatedly shown that out-of-control diabetes results in complications from the disease,
the goal for people with diabetes is a hemoglobin A1c less than 7%. The higher the hemoglobin A1c, the
higher the risks of developing complications related to diabetes.
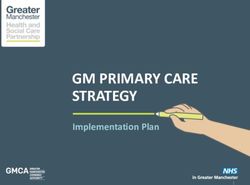
geographic location: Buckeye Community Health Members in the Southwest, Northwest, Northeast and East
B. Comparisons were made between the program participants and a similar population (high-risk, type II Central areas of Ohio (see service map below):
diabetics, etc.) for hospital and emergency room utilization 90 days prior to program registration compared
to 90 days after registration. The results (shown below) reflect a 55% decrease in hospital utilization and a
decrease of 16% in emergency room utilization for program participants compared to members who did not
participate.
P‐Values
Program
Program Member Pre 90 Post 90 Hospital
Participation ER Visits
Participation Status Count MM MM Visits
Status
No 677 1,762 1,641 No 0.363 0.106
Yes 145 421 421 Yes 0.044 0.001
Grand Total 822 2,182 2,062 Grand Total 0.143 0.282
P‐value < .05 is considered to be statistically significant.
Pre 90 Post 90
Program % Pre 90 Post 90 Per
Hospital Hospital
Participation Status Change Per 1,000 1,000
Visits Visits
No 139 149 7% 315.6 363.2
Yes 56 25 ‐55% 532.5 237.6
Grand Total 195 174 ‐11% 357.4 337.6
Program Pre 90 ER Post 90 % Pre 90 Post 90 Per
Participation Status Visits ER Visits Change Per 1,000 1,000
No 484 442 ‐9% 1,098.9 1,077.5
Yes 145 122 ‐16% 1,378.9 1,159.3
Grand Total 629 564 ‐10% 1,152.8 1,094.2
C. We also measured member engagement and utilization throughout the initiative as number of blood contact: Artie Paniagua MBA, BSN, RN
sugar entries through the mobile application. Prior to implementation, the decision was made to require Director Clinical Policy and Support, Centene Corporation
participants to record a minimum of seven entries per week (one entry per day average). As shown below, (314) 725-4706 ext. 25038; apaniagua@centene.com
members maintained an average level of five to six entries per week throughout the initiative.24 | Diabetes Care Best Practices Compendium Best Practices | 25
UPMC for You UPMC’s Community Health Workers (CHW) have received specific training on diabetes through a program
developed by the University of Pittsburgh’s Department of Family Medicine. Their role in supporting those with
Community Health Worker Program diabetes is to act as an advocate, liaison and role model. The CHWs have completed an inventory of the health
and wellness services that are available within the communities they are serving and at the community center they
are located. They will help link a person with diabetes to the services that they may need, including those lifestyle
description: The Community Health Worker Program is a collaborative effort between UPMC for You and classes offered at the community centers, such as exercise. We are currently in the process of working on scheduling
various community centers located in areas with a high concentration of African Americans. These communities the Stanford chronic education classes in each of the four community centers. They CHWs will help to organize
have health care disparities. The program is a neighborhood-based health and wellness initiative. The objectives and promote the event. Those with diabetes will be invited to attend these classes.
of the program are to develop relationships with key stakeholders in those communities through the use of
Community Health Workers. Through those relationships, we will engage not only our members, but residents of outcomes: The evaluation for this program is not set until 2013.
the community, in chronic condition education programs, lifestyle management, and to connect them to needed
health care and social resources. Engagement of Medicaid members in health or care management programs
through telephonic methods can be successful only to a point. The current rate of reaching our members geographic location: The program has been implemented in Pittsburgh, Pennsylvania in four communities
hovers around 35 to 40%. Poor addresses and phone numbers, and lack of relationships with the health care through the Hosanna House, Inc., Bidwell Presbyterian Church and Manchester Youth Development Center, Hill
community make it difficult to reach a large portion of our members. Community-based programs, placed in House, Association and the Kingsley Association.
the communities where the members reside, offered through peers, in a culturally sensitive manner can greatly
improve the engagement of members; improve access to services, quality of care, appropriate utilization of contact: Debra Smyers
services, and satisfaction with the experience of care. Senior Director Program Development, UPMC for You
(412) 454-7755; smyersd@upmc.edu
The four communities identified for the Community Health Worker Program have almost 18,000 members.
Of those, 70% are African American. The UPMC for You rate of African Americans over the age of 18 with
diabetes is 10.39%. By comparison, the rate of diabetes in our Caucasian members over the age of 18 is 7.94%.
The high rate of diabetes and other chronic conditions with corresponding gaps in care has been identified as an
opportunity. Our experience with programs such as the Patient Centered Medical Home and the community-
based care teams, which are based on face-to-face interactions with members, have a higher engagement rate
and can be more successful in helping members to access health care services and manage their care. The
implementation of the community heath workers will assist us in reaching and engaging more members who have Midwest Health Plan
chronic conditions, in addition to providing support to non-UPMC for You community residents. Diabetes Control Network
key objectives: description: Midwest Health Plan created the Diabetes Control Network to identify members with diabetes
Improve the health of the population and help improve care. The Diabetes Control Network identifies members with diabetes through a comprehensive
Enhance the patient experience of care (including quality, access and reliability) software system that supports Midwest Health Plan’s (MHP) disease management, case management, and utilization
Control or reduce the per capita cost of care or increase efficiency management functions. This system provides for an integrated and efficient way to identify members eligible for the
Reduce disparities in care of racial and ethnic minorities program, stratify based on severity of disease, and track member interventions. Members enrolled in the Diabetes
Control Network receive information and other materials focusing on the disease process and complications,
actions taken: UPMC for You has provided the funding to hire four Community Health Workers in May 2012. medication use & adherence, nutrition, caregiver resources, self-management skills, treatment plan, lifestyle issues
These individuals were hired in conjunction with the community centers and are residents of the community. affecting the disease state, depression, and the importance of follow up with physicians. Members also receive
They have begun to talk with community stakeholders, identified the health care and other social support services reminders and incentives to complete recommended diabetes visits and testing. Primary care providers receive
available, and are gathering information on the unique needs of those communities. UPMC for You partnered education and information to improve the diabetes services they provide to members. Midwest Health Plan has
with UPMC Family Medicine to develop a training program for the Community Health Workers. A UPMC seen improvements in all HEDIS® measures for comprehensive diabetes care during the past three years. HbA1c
physician provided key elements of that training. The Community Health Workers devote 40% of their time to testing increased from 82% to 93%; Eye exams increased from 60% to 62%; LDL screening from 79% to 80%, and
activities directed by the centers and 60% on health plan directed activities. The Community Health Workers are monitoring for nephropathy increased from 87% to 98%.
meeting with individuals in the communities with the goals to: Midwest Health Plan continues to implement the Diabetes Control Network program to address the following
Identify needed health care or social services and assist residents in accessing those services issues:
Provide culturally appropriate health care related information According to the 2011 Michigan Diabetes Burden Report, Diabetes affects 25.8 million Americans (8.3%
Give informal counseling and guidance on heath behaviors and self-management of chronic conditions of the population) and an estimated 1.65 million Michigan citizens. Diabetes costs the United States
Identify health and wellness programs that can benefit the resident $174 billion annually and over $9 billion per year in Michigan. Total medical costs for Midwest Health
Advocate for the individual Plan’s members with diabetes were $14,492,819 and prescription costs were $6,773,941 for a total cost of
Coordinate the promotion of health and wellness programs $21,266,760.
For UPMC for You members, provide referrals to health plan care management programs and coordinate Michigan’s 2011 Behavioral Risk Factor Survey reports that diabetes was the seventh leading cause of
accessing services for those members death in 2010. In 2011, an estimated 10% of Michigan adults reported being told by a doctor that they had
diabetes. The prevalence of diabetes increases with age and decreases with increasing household income
level. Disabled adults (18.4%) were more likely to have been diagnosed than non-disabled adults (6.6%). In
2011, 72% of members with diabetes were in the aged, blind and disabled (ABAD) Medicaid group.Briefly identify specific outcomes / data related to the initiative identified in question 3. Use speci
where possible. (Limit to one to two paragraphs)
26 | Diabetes Care Best Practices Compendium Best Practices | 27
MHP measures the effectiveness and outcomes of our programs through annual HEDIS indicator
®
results. Processes are then refined based on these outcomes. Annually, MHP performs program-s
chart audits to ascertain the effectiveness of the interventions using HEDIS indicators. The HEDI
®
indicators used are: HbA1c testing; LDL-screening; eye exam (retinal) performed; kidney disease
key objectives: outcomes : MHP measures
(nephropathy) monitored.
the effectiveness and outcomes of our programs through annual HEDIS®
Improve the health of the diabetic population indicators and results. Processes are then refined based on these outcomes. Annually, MHP performs
Enhance the patient experience of care (including quality, access and reliability) program-specific chart audits to ascertain the effectiveness of the interventions using HEDIS® indicators.® The
MHP provides
used provider-specific HEDIS performance feedback annually. HEDIS
diseasemeasures are
®
Improve quality of care in a specific clinical area (medication adherence, patient education, lifestyle HEDIS® indicators are: HbA1c testing; LDL-screening; eye exam (retinal) performed; kidney
changes, specialty care, etc)
assess the
(nephropathy) effectiveness of health management programs, so this intervention provides information
monitored.
PCP’s on the extent to HEDIS®
MHP provides provider-specific which members
performance arefeedback
receiving care in
annually. compliance
HEDIS® measureswith the to
are used clinical guidelin
assess senior memberofofhealth
the effectiveness the Quality
managementManagement
programs, so Department confers
this intervention withinformation
provides physicianstoregarding
PCP’s their ou
actions taken: The initiatives of the Diabetes Control Network include: on thecompliance
extent to which members are receiving care in compliance with the clinical guidelines. A senior
members, engages in instructional dialogue, and provides patient-specific compliance
Members enrolled in the Diabetes Control Network receive information and other materials quarterly member of the Quality
for follow up and Management Department confers with physicians regarding their out of compliance
documentation.
which focus on disease process and complications, medication use & adherence, nutrition, caregiver members, engages in instructional dialogue, and provides patient-specific compliance tools for follow up and
resources, self-management skills, treatment plan, lifestyle issues affecting the disease state, depression, documentation.
and the importance of follow up with physicians.
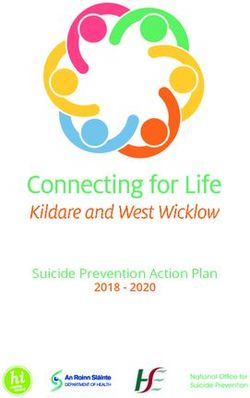
The ongoing
The ongoing interventions
interventions of the
of the diabetes diabetes
disease diseaseprogram
management management program have
have demonstrated demonstrated an
an improvement
Community health fairs are held where diabetes services are performed such as dilated eye exams, blood in the improvement in the
delivery of services and delivery of services
better patient andawareness.
& physician better patient
This is& physician
evidenced awareness.
by the This is evidenc
HEDIS® results
pressures, and podiatrist foot exams. below:the HEDIS® results below:
Educational materials and preventive health guidelines are distributed to members to assist in self- ®
management. HEDIS Measure
A Health Risk Assessment (HRA) is sent to all new health plan members upon enrollment. Members are Comprehensive Diabetes Care (CDC) 2010 2011 2012
eligible for a $5 gift card incentive for the return of an HRA. Basic educational material is sent when the *HbA1c testing 82.1% 88.5% 92.7%
form is returned with a positive response on the diabetes question and members are also enrolled in the *Eye Exam 59.7% 61.3% 61.5%
disease management program.
*LDL‐C Screening 79.2% 83.4% 84.7%
Incentive reminder letters are sent to members who are due for the following annual diabetes screening *Monitoring for Nephropathy 86.5% 92.3% 97.8%
tests:
Lipid screening
Microalbuminuria 8. location
geographic Geographic Location
: Southeast Michigan
Dilated eye exam Southeast Michigan
Hemoglobin A1C contact: Andrea Fogarty
9. Director,
ContactHealth Management,
Information Midwest
(to be listedHealth
in thePlan
publication)
Members can receive a $10 gift card per completed test. Members must return the form via fax/mail with their (313) 586-6071; afogarty@midwesthealthplan.com
Primary Care Physician’s (PCP) signature to receive the gift card.
Contact Name: Andrea Fogarty
Opportunity Reports are available to physicians on the MHP website. The reports allow providers to
access administrative/clinical data through a secure website. These reports allow providers to view
services completed and services due for their patients.
3
PCP’s are notified about our free glucometer program via the Provider Newsletter and MHP website.
Members are informed via the member newsletter and DM mailings. Members are also informed about
the program when they are in communication with a DM Nurse who will order a meter for the member if
needed.
A diabetes satisfaction survey is sent to members enrolled in the Diabetes Control Network program
annually. The survey is used to obtain comments and feedback from the members and also to review any
complaints the member may have regarding the program.
Members with diabetes who had 3 or more hospital admissions during the preceding three months are
automatically referred to Case Management. Health Services nurses then follow-up with members for
evaluation and possible entry into case management.
Members are also stratified based on other comorbidities including hypertension and hyperlipidemia.
Members are tracked and follow up is done through additional interventions.You can also read