Delay of Pregnancy Among Physicians vs Nonphysicians
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research
JAMA Internal Medicine | Original Investigation | PHYSICIAN WORK ENVIRONMENT AND WELL-BEING
Delay of Pregnancy Among Physicians vs Nonphysicians
Maria C. Cusimano, MD; Nancy N. Baxter, PhD; Rinku Sutradhar, PhD; Eric McArthur, MSc; Joel G. Ray, MD;
Amit X. Garg, MD; Simone Vigod, MD; Andrea N. Simpson, MD
Supplemental content
IMPORTANCE Women physicians may delay childbearing and experience childlessness
more often than nonphysicians, but existing knowledge is based largely on self-reported
survey data.
OBJECTIVE To compare patterns of childbirth between physicians and nonphysicians.
DESIGN, SETTING, AND PARTICIPANTS Population-based retrospective cohort study of
reproductive-aged women (15-50 years) in Ontario, Canada, accrued from January 1, 1995,
to November 28, 2018, and observed to March 31, 2019. Outcomes of 5238 licensed
physicians of the College of Physicians and Surgeons of Ontario were compared with those of
26 640 nonphysicians (sampled in a 1:5 ratio). Physicians and nonphysicians were observed
from age 15 years onward.
EXPOSURES Physicians vs nonphysicians.
MAIN OUTCOMES AND MEASURES The primary outcome was childbirth at gestational age
of 20 weeks or greater. Cox proportional hazards models were used to examine the
association between physician status and childbirth, overall and across career stage
(postgraduate training vs independent practice) and specialty (family physicians
vs specialists).
RESULTS All physicians (n = 5238) and nonphysicians (n = 26 640) were aged 15 years at
baseline, and 28 486 (89.1%) were Canadian-born. Median follow-up was 15.2 (interquartile
range, 12.2-18.2) years after age 15 years. Physicians were less likely to experience childbirth
at younger ages (hazard ratio [HR] for childbirth at 15-28 years, 0.15; 95% CI, 0.14-0.18;
P < .001) and initiated childbearing significantly later than nonphysicians; the cumulative
incidence of childbirth was 5% at 28.6 years in physicians and 19.4 years in nonphysicians.
However, physicians were more likely to experience childbirth at older ages (HR for 29-36
years, 1.35; 95% CI, 1.28-1.43; P < .001; HR for ⱖ37 years, 2.62; 95% CI, 2.00-3.43; P < .001),
and ultimately achieved a similar cumulative probability of childbirth as nonphysicians overall.
Median age at first childbirth was 32 years in physicians and 27 years in nonphysicians
(P < .001). After stratifying by specialty, the cumulative incidence of childbirth was higher in
family physicians than in both surgical and nonsurgical specialists at all observed ages.
CONCLUSIONS AND RELEVANCE The findings of this cohort study suggest that women
physicians appear to delay childbearing compared with nonphysicians, and this phenomenon
is most pronounced among specialists. Physicians ultimately appear to catch up to
nonphysicians by initiating reproduction at older ages and may be at increased risk of
resulting adverse reproductive outcomes. System-level interventions should be considered
to support women physicians who wish to have children at all career stages.
Author Affiliations: Author
affiliations are listed at the end of this
article.
Corresponding Author: Andrea N.
Simpson, MD, Department of
Obstetrics and Gynecology,
St Michael’s Hospital/Unity Health
Toronto, 507-55 Queen St E, Toronto,
JAMA Intern Med. doi:10.1001/jamainternmed.2021.1635 Ontario, M5C 1R6, Canada
Published online May 3, 2021. (andrea.simpon@unityhealth.to).
(Reprinted) E1
© 2021 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Duke Medical Center Library User on 05/12/2021Research Original Investigation Delay of Pregnancy Among Physicians vs Nonphysicians
D
espite increasing gender parity in the physician work-
force, a career in medicine is still frequently viewed Key Points
as a barrier to motherhood.1-4 Women physicians who
Question Are women physicians more likely to delay childbearing
wish to have children face demanding work hours, limited op- or less likely to have children compared with nonphysicians?
tions for parental leave and child support, and potential stig-
Findings In this population-based retrospective cohort study of
matization by peers and superiors.3-5 Women physicians
5238 reproductive-aged physicians matched 1:5 to nonphysician
may therefore remain childless or delay childbearing relative
counterparts, physicians significantly postponed the initiation of
to the general population; 50% to 60% report postponing childbearing. Despite this delay, physicians ultimately achieved a
pregnancy to independent practice,6,7 and 25% who attempt similar probability of childbirth as nonphysicians, owing to higher
conception report infertility.8,9 These factors may place women rates of pregnancy at advanced maternal ages; this phenomenon
physicians at risk of age-related adverse reproductive was most pronounced for specialists.
outcomes.10,11 Meaning Physicians appear to delay childbearing and may be at
Existing studies examining pregnancy and childbirth in increased risk of age-related adverse pregnancy outcomes.
women physicians are almost exclusively self-reported sur-
veys prone to sampling and information bias. To our knowl-
edge, only 1 observational study has described reproductive system evaluation and improvement (eTable 1 in Supple-
patterns in women physicians12; the authors found that ma- ment 2). The unique linkage of CPSO data to ICES data en-
ternal age at delivery was higher for physicians relative to non- abled identification of physicians and nonphysicians, physi-
physicians, but the study did not explore time to childbirth or cian characteristics (eg, specialty, date of licensing to train or
whether parity, specialty, or training status influenced the practice independently), covariates, and outcomes.14 Data sets
trends observed. were linked using unique encoded identifiers and analyzed at
Large epidemiologic studies using validated data sources ICES. The study followed the Strengthening the Reporting of
are needed to accurately characterize patterns of childbirth Observational Studies in Epidemiology (STROBE) reporting
among women physicians. These data would contextualize guideline.
pregnancy outcomes in this population and directly inform re-
productive planning and care. We therefore examined pat- Study Population and Exposure Assessment
terns of childbirth in physicians compared to nonphysicians Selection of Physicians
using population-based health administrative data. Women were classified as physicians if they had a record of
being licensed to practice medicine with the CPSO, either
as a postgraduate trainee or independent practitioner. We in-
cluded all women physicians (aged 15-50 years) who (1) were
Methods first licensed between January 1, 1995, and November 26, 2018;
Study Design and Data Sources (2) were Ontario residents on the date that they were granted
We performed a population-based retrospective cohort study their CPSO license; and (3) had been eligible for provincial
of reproductive-aged women in Ontario, Canada, where 14.6 health insurance since the age of 15 years. These strict criteria
million citizens reside and 40% of Canadian childbirths occur.13 enabled selection of women in which all childbirths over
All Ontario residents are eligible for universal health insur- the reproductive life span could be accurately detected in ICES
ance coverage for hospital and physician services. The study databases.
protocol was published14 and approved by the Research Eth-
ics Board at St Michael’s Hospital (Toronto, Ontario, No. 18- Selection of Nonphysicians
248) (Supplement 1). Nonphysician women (aged 15-50 years) were drawn from the
To practice medicine in Ontario, physicians must obtain ICES Registered Persons Database and randomly assigned a
a medical license from the College of Physicians and Sur- simulated medical licensing date according to the distribu-
geons of Ontario (CPSO), which is the sole regulatory body that tion of all licensing dates in physicians. Nonphysicians were
grants medical licenses in Ontario. Physicians are first granted included if they (1) were alive on their simulated licensing date;
a postgraduate education license at completion of medical (2) were Ontario residents on that date; and (3) had been eli-
school and initiation of residency training, and subsequently gible for provincial health insurance since the age of 15 years.
granted an independent practice license after examination and This approach mirrored the selection of physicians, who by
certification by either the College of Family Physicians of definition were alive on the date of licensing.
Canada or the Royal College of Physicians and Surgeons of We aimed to determine whether patterns of childbirth dif-
Canada. fered for physicians and nonphysicians over the reproduc-
To complete this study, we obtained a data set of Ontario tive life span. To do so, we observed physicians and nonphy-
physicians licensed by the CPSO and linked this data set to sicians from the date of their 15th birthday. For each physician,
population-based databases held at ICES, a nonprofit re- we sampled 5 eligible nonphysicians born in the same year to
search institute and prescribed entity under section 45 of On- ensure that groups were balanced on age and era of cohort en-
tario’s Personal Health Information Protection Act, which au- try. It should be recognized that a period of immortal time was
thorizes ICES to collect personal health information on all introduced in this process; however, its extent was similar in
Ontario residents, without consent, for the purpose of health physicians and nonphysicians, as neither could die prior to
E2 JAMA Internal Medicine Published online May 3, 2021 (Reprinted) jamainternalmedicine.com
© 2021 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Duke Medical Center Library User on 05/12/2021Delay of Pregnancy Among Physicians vs Nonphysicians Original Investigation Research
their actual or simulated licensing date, respectively, and it was birth. Individuals were observed from age 15 years and cen-
unlikely to bias results because the cumulative probability of sored at death, loss to follow-up (ie, loss of eligibility for pro-
death after licensing was also very low (Research Original Investigation Delay of Pregnancy Among Physicians vs Nonphysicians
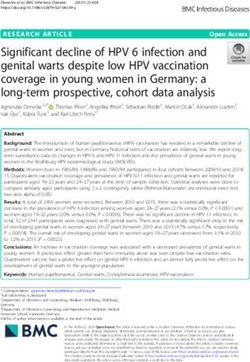
Figure 1. Flow Diagram of Included Patients
16 920 Women physicians (aged 15-50 y) who 3 247 000 Nonphysician women (aged 15-50 y)
became licensed from January 1, 1995, alive on simulated licensing date from
to November 26, 2018 January 1, 1995, to November 26, 2018
11 592 Excluded 1 927 006 Excluded
11 051 Noncontinuous provincial 1 730 780 Noncontinuous provincial
health insurance from health insurance from
age 15 y age 15 y
541 Non-Ontario residents 196 226 Non-Ontario residents
5328 Physicians eligible for inclusion 1 319 994 Nonphysicians eligible for inclusion
5328 Physicians included 26 640 Nonphysicians included (sampled in a 5:1
ratio of nonphysicians to physicians)
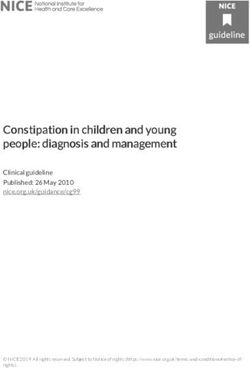
son for loss to follow-up. Analyses were performed using physicians (Figure 2A). However, by age 37 years, the cumu-
SAS, version 9.4 (SAS Institute). lative incidence of childbirth was similar in both groups (62.7%
in physicians, 62.1% in nonphysicians; Figure 2A). Median (IQR)
age at first childbirth was 27.0 (22.6-30.2) years for nonphy-
sicians and 31.6 (29.8-33.6) years for physicians (P < .001)
Results (Table 2).
Study Population After stratifying by specialty, unadjusted rates of child-
We identified 16 920 physicians of reproductive age who reg- birth were higher in family physicians (2.83 per 100 person-
istered with the CPSO between January 1, 1995, and Novem- years) than in specialists (2.42 per 100 person-years). The cu-
ber 26, 2018. After excluding those who had not resided in mulative incidence of childbirth was also higher in family
Ontario since age 15 years, our cohort included 5328 physi- physicians than in specialists at all observed ages (Table 2;
cians who could be observed over their reproductive life Figure 2B).
span; 2442 (45.8%) were training or practicing in family After restricting to nonphysicians in the highest income
medicine, 1878 (35.2%) were training or practicing in other quintile only, physicians still appeared to delay childbirth rela-
specialties, 900 (16.9%) had not completed training at any tive to nonphysicians to a similar degree (eFigure 2A in Supple-
point during follow-up and were categorized as specialty not ment 2). After stratifying by era of birth, physicians born re-
yet determined, and 108 (2.0%) were missing data on spe- cently (1985-1994) had a lower cumulative incidence of
cialty. Physicians were successfully frequency matched to childbirth than physicians of the same age but born earlier
26 640 nonphysicians at age 15 years (Figure 1). (1976-1984; log-rank P < .001; eFigure 2B in Supplement 2). Af-
ter further stratifying by specialty, patterns of childbirth did
Timing of Childbirth not differ substantially for surgical and nonsurgical special-
At baseline (age 15 years), women who were ultimately li- ists, but both had a lower cumulative incidence of childbirth
censed as physicians were more likely to live in high-income relative to family physicians at all ages (log-rank P < .001; eFig-
urban areas (2092 of 5328 [39.3%] vs 4653 of 26 640 [17.5%]; ure 2C in Supplement 2).
P < .001), less likely to live in rural areas (390 of 5328 [7.3%]
vs 4141 of 26 640 [15.5%]; P < .001), and more likely to be im- Supplemental Analysis
migrants (881 of 5328 [15.2%] vs 2671 of 26 640 [10.0%]; Approximately 98% of physicians (n = 5227) were nullipa-
P < .001) than women who were nonphysicians (Table 1). rous at the time of licensing (eTable 3 in Supplement 2). In
Median (interquartile range [IQR]) follow-up was 16.7 (14.7- supplemental analyses comparing these physicians with nul-
19.1) years in physicians and 14.8 (11.6-17.9) years in nonphy- liparous nonphysicians, physicians had a decreased rate of
sicians (Table 2). Over the reproductive life span, physicians childbirth (HR, 0.79; 95% CI, 0.74-0.85; P < .001) compared
on average had a decreased rate of childbirth compared with with nonphysicians while in postgraduate training, but an in-
nonphysicians (HR, 0.62; 95% CI, 0.59-0.65; P < .001). In piece- creased rate (HR, 2.23; 95% CI, 2.10-2.36; P < .001) while in in-
wise models, physicians had a markedly decreased rate of dependent practice (eTable 4 in Supplement 2). Results were
childbirth from age 15 to 28 years (HR, 0.15; 95% CI, 0.14- similar whether a marginal or conditional approach was used
0.18; P < .001), slightly increased rate of childbirth from age to account for matching.
29 to 36 years (HR, 1.35; 95% CI, 1.28-1.43; P < .001), and mark- After stratifying by specialty, specialists had a decreased
edly increased rate of childbirth after age 37 years (HR, 2.62; rate of childbirth compared with nonphysicians while in post-
95% CI, 2.00-3.43), compared with nonphysicians (Table 3). graduate training (HR, 0.71; 95% CI, 0.64-0.70; P < .001) but
Age at initiation of childbearing was later for physicians an increased rate while in independent practice (HR, 2.13;
than nonphysicians: the cumulative probability of childbirth 95% CI, 1.92-2.36; P < .001). In contrast, family physicians had
was 5% at age 19.4 years in nonphysicians and 28.6 years in a rate of childbirth comparable to nonphysicians while in post-
E4 JAMA Internal Medicine Published online May 3, 2021 (Reprinted) jamainternalmedicine.com
© 2021 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Duke Medical Center Library User on 05/12/2021Delay of Pregnancy Among Physicians vs Nonphysicians Original Investigation Research
Table 1. Baseline Characteristics of Physicians and Nonphysicians at Age 15 Years
No. (%)
Physicians Nonphysicians
Characteristic (n = 5328) (n = 26 640) Standardized difference
Age at index date, median (IQR), y 15 (15-15) 15 (15-15) 0
Era of cohort entry
1995-2006 2750 (51.6) 13 750 (51.6)
0
2007-2018 2578 (48.4) 12 890 (48.4)
Residential income urban quintile
1 (Lowest) 445 (8.4) 4231 (15.9) 0.23
2 548 (10.3) 4256 (16.0) 0.17
3 733 (13.8) 4533 (17.0) 0.09
4 1094 (20.5) 4709 (17.7) 0.07
5 (Highest) 2092 (39.3) 4653 (17.5) 0.50
Rural residence 390 (7.3) 4141 (15.5) 0.26
Missing 26 (0.5) 117 (0.4) 0.01
Immigration status
Canadian-born 4517 (84.8) 23 969 (90.0)
0.16
Immigrant 881 (15.2) 2671 (10.0)
Comorbidities (Johns Hopkins ADGs)
0 757 (14.2) 3750 (14.1) 0
1-5 3707 (69.9) 18 121 (68.0) 0.03
6-9 797 (15.0) 4157 (15.6) 0.02
≥10 67 (1.3) 612 (2.3) 0.08
Previous live births
0 5328 (100.0) 26 612 (99.9) 0.04
1 0 Abbreviations: ADG, Aggregated
28 (0.1) 0.04 Diagnosis Group; IQR, interquartile
≥2 0
range.
Table 2. Rate of First Childbirth, Age at First Childbirth, and Cumulative Probability of First Childbirth Among Physicians and Nonphysicians
Observed From Age 15 Years
Physicians
Nonphysicians Total Family physicians Specialists
Outcome (n = 26 640) (n = 5328) (n = 2442) (n = 1878)
Follow-up, median (IQR), y 14.8 (11.6-17.9) 16.7 (14.7-19.1) 16.5 (14.6-18.8) 17.9 (16.1-20.3)
Rate of childbirth per 100 person-years 3.40 2.31 2.83 2.42
Time to childbirth, median (95% CI), y 32.7 (32.5-32.9) 34.7 (34.5-35.0) 33.6 (33.4-33.9) 35.6 (35.2-36.0)
Age at first childbirth, median (IQR),a y 27.0 (22.6-30.2) 31.6 (29.8-33.6) 31.4 (29.6-33.3) 32.1 (30.4-34.2)
Cumulative probability of childbirth, %
At 20 y 6.2 0.1 0.02 0.01
At 25 y 18.6 0.5 0.05 0.04
At 30 y 37.7 12.3 16.1 9.4
At 35 y 57.8 52.0 61.3 46.2
At 40 y 65.2 70.1 76.7 67.8
Abbreviation: IQR, interquartile range.
a
Age at first childbirth among women who experienced a first childbirth during observed follow-up.
graduate training (HR, 0.93; 95% CI, 0.81-1.03; P = .17) but an career in medicine delay childbearing relative to the general
increased rate while in independent practice (HR, 2.18; population. Physicians almost universally remained nullipa-
95% CI, 2.03-2.35; P < .001) (eTable 4 in Supplement 2). rous prior to age 28 years but had high rates of childbirth
thereafter, particularly on entering independent practice. As
a result, physicians were often pregnant at advanced mater-
nal ages, when the risks of infertility and adverse maternal
Discussion and fetal outcomes are more pronounced.10,11
This population-based retrospective cohort study of more The present study demonstrates that delay of childbirth
than 5300 physicians suggests that women pursuing a in physicians begins early and is directly associated with ca-
jamainternalmedicine.com (Reprinted) JAMA Internal Medicine Published online May 3, 2021 E5
© 2021 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Duke Medical Center Library User on 05/12/2021Research Original Investigation Delay of Pregnancy Among Physicians vs Nonphysicians
reer stage and specialty. Only 2% of physicians had children ternal age at admission for childbirth ranged from 31 to 33 years
before completing medical school; while family physicians for physicians and 27 to 31 years for nonphysicians from 1996
went on to have rates of childbirth that were comparable to to 2013; however, this study did not account for parity or as-
nonphysicians during residency, specialists continued to have sess outcomes by specialty or career stage. The present work
decreased rates of childbirth until they began independent not only confirms that physicians delay childbearing, but also
practice. This complements the observations of previous sur- identifies the time period when this delay occurs and sug-
veys, which have found that mean physician age at first child- gests that the duration of delay may be lengthening over time
birth ranges from 30 to 33 years8,21 and that only 14% to 40% rather than shortening.
of physicians experience a pregnancy during postgraduate The present study is the first to map the trajectory of child-
training.6,7,22 To our knowledge, only 1 other observational birth in women physicians using epidemiologic data and di-
study has compared reproductive patterns between physi- rectly model rates of childbirth for both postgraduate train-
cians and nonphysicians. Using the Taiwan National Health In- ees and independent practitioners in differing specialties. In
surance Database, Wang et al12 showed that the median ma- contrast to previous surveys, we studied a large population-
based cohort of physicians licensed to practice in an entire prov-
ince. By using validated administrative data, we observed in-
Table 3. Relative Rate of First Childbirth Among Physicians
and Nonphysicians Observed From Age 15 Years dividuals over prolonged follow-up and identified childbirths
with little risk of misclassification. This work also provides the
Exposure group Hazard ratio (95% CI)a P value
context required to understand the factors that contribute to
Reproductive period
adverse reproductive outcomes among physicians. We show
Nonphysician 1 [Reference] NA
that physicians experience childbirth at an advanced mater-
Physician 0.62 (0.59-0.65)bDelay of Pregnancy Among Physicians vs Nonphysicians Original Investigation Research
and illustrated when most physicians initiate childbearing. that could be considered to ensure that women physicians
Second, the study cohort does not include women who can pursue pregnancy if and when they desire include
moved to Ontario after age 15 years. While it is possible that adequate parental leave, remuneration for physicians during
the results may not reflect the experiences of international parental leave, options for childcare that extend beyond the
medical graduates or mobile physicians, we would not traditional workday, increased flexibility in both under-
anticipate these groups to be any less likely to delay child- graduate and postgraduate training schedules, and a culture
birth. Third, we lacked data on relationship status, race/ of leadership that supports physician mothers and promotes
ethnicity, use of assisted reproductive technology, preg- the importance of shared parenting and domestic tasks.4,30
nancy intent, and occupation for nonphysicians. Delay of
childbirth may also occur in other professions that require
prolonged training, such as basic science, law, and engineer-
ing. These factors should be studied further; however, the
Conclusions
consistency noted even after restricting to high-income non- Women physicians appear to postpone childbearing com-
physicians and the dramatic shift in rates of childbirth after pared with nonphysician counterparts, and this phenom-
the completion of postgraduate training suggest that volun- enon is more pronounced in specialists. Although physicians
tary childlessness or a preference for delay is unlikely to ultimately achieve a similar cumulative probability of preg-
explain the findings. Whether delay of pregnancy is due to nancy as nonphysicians, they do so by initiating reproduc-
career-related concerns,23,24 demanding academic schedules tion at older ages and may be at increased risk of adverse re-
and limited support, 4, 25-29 or simply personal choice, productive outcomes. System-level interventions are required
women physicians in our current system must complete to support women physicians who wish to have children at
training during their primary reproductive years. Strategies all career stages.
ARTICLE INFORMATION Supervision: Baxter, Sutradhar, Simpson. Ontario; and Service Ontario. However, the
Accepted for Publication: March 15, 2021. Conflict of Interest Disclosures: Dr Cusimano conclusions, opinions, and statements expressed
reported being supported by the American College herein are solely those of the authors and not those
Published Online: May 3, 2021. of the bodies listed. No endorsement by these
doi:10.1001/jamainternmed.2021.1635 of Surgeons (ACS) Resident Research Scholarship
and the Canadian Institutes of Health Research bodies is intended or should be inferred.
Author Affiliations: Department of Obstetrics and (CIHR) Vanier Canada Graduate Scholarship. Additional Information: The data set from this
Gynaecology, University of Toronto, Toronto, Dr Baxter reported receiving grants from Physician study is held securely in coded form at ICES. While
Ontario, Canada (Cusimano, Simpson); Li Ka Shing Services Incorporation Foundation during the data sharing agreements prohibit ICES from making
Knowledge Institute, St Michael’s Hospital, Toronto, conduct of the study. Dr Garg reported being the data set publicly available, access may be
Ontario, Canada (Cusimano, Baxter, Simpson); supported by the Dr Adam Linton Chair in Kidney granted to those who meet prespecified criteria for
Melbourne School of Population and Global Health, Health Analytics and a CIHR Clinician Investigator confidential access, available at https://www.ices.
University of Melbourne, Melbourne, VIC, Australia Award. Dr Vigod reported receiving royalties for on.ca/DAS.
(Baxter); ICES (formerly the Institute for Clinical authorship from UpToDate Inc outside the
Evaluative Sciences), Ontario, Canada (Baxter, submitted work. No other disclosures were REFERENCES
Sutradhar, McArthur, Ray, Garg, Vigod, Simpson); reported.
Division of Biostatistics, Dalla Lana School of Public 1. Canadian Institute for Health Information.
Health, University of Toronto, Toronto, Ontario, Funding/Support: This study was conducted with Physicians in Canada. Accessed March 30, 2020.
Canada (Sutradhar); Department of Medicine, grant funding from Physicians’ Services https://www.cihi.ca/en/physicians-in-canada
St Michael’s Hospital/Unity Health Toronto, Incorporated (PSI) Foundation. This study was also 2. Giantini Larsen AM, Pories S, Parangi S,
Toronto, Ontario, Canada (Ray); Department of supported by ICES, which is funded by an annual Robertson FC. Barriers to pursuing a career in
Medicine, London Health Sciences Centre, London, grant from the Ontario Ministry of Health and surgery: an institutional survey of Harvard Medical
Ontario, Canada (Garg); Department of Psychiatry, Long-Term Care (MOHLTC). School students. Ann Surg. Published online October
Women’s College Hospital, Toronto, Ontario, Role of the Funder/Sponsor: The funders had no 9, 2019. doi:10.1097/SLA.0000000000003618
Canada (Vigod); Women’s College Research role in the design and conduct of the study; 3. Halley MC, Rustagi AS, Torres JS, et al. Physician
Institute, Women’s College Hospital, Toronto, collection, management, analysis, and mothers’ experience of workplace discrimination:
Ontario, Canada (Vigod); Department of Obstetrics interpretation of the data; preparation, review, or a qualitative analysis. BMJ. 2018;363:k4926. doi:10.
and Gynecology, St Michael’s Hospital/Unity Health approval of the manuscript; and decision to submit 1136/bmj.k4926
Toronto, Toronto, Ontario, Canada (Simpson). the manuscript for publication.
4. Rangel EL, Smink DS, Castillo-Angeles M, et al.
Author Contributions: Dr Simpson had full access Disclaimer: The analyses, conclusions, opinions, Pregnancy and motherhood during surgical
to all of the data in the study and takes and statements expressed herein are solely those training. JAMA Surg. 2018;153(7):644-652. doi:10.
responsibility for the integrity of the data and the of the authors and do not reflect those of the 1001/jamasurg.2018.0153
accuracy of the data analysis. funding or data sources; no endorsement by ICES
Concept and design: Cusimano, Sutradhar, or the MOHLTC is intended or should be inferred. 5. Adesoye T, Mangurian C, Choo EK, Girgis C,
McArthur, Vigod, Simpson. Sabry-Elnaggar H, Linos E; Physician Moms Group
Additional Contributions: The authors thank Peter Study Group. Perceived discrimination experienced
Acquisition, analysis, or interpretation of data: Tanuseputro, MD, Manish Sood, MD, and Emily
All authors. by physician mothers and desired workplace
Rhodes, MSc, at the Ottawa Hospital Research changes: a cross-sectional survey. JAMA Intern Med.
Drafting of the manuscript: Cusimano, Sutradhar, Institute, for their assistance with data acquisition.
Vigod. 2017;177(7):1033-1036. doi:10.1001/jamainternmed.
They were not compensated for their contributions. 2017.1394
Critical revision of the manuscript for important Parts of this material are based on data and
intellectual content: All authors. information compiled and provided by the 6. Turner PL, Lumpkins K, Gabre J, Lin MJ, Liu X,
Statistical analysis: Sutradhar, McArthur, Ray. Canadian Institute for Health Information; Ontario Terrin M. Pregnancy among women surgeons:
Obtained funding: Baxter, Simpson. Ministry of Health and Long-Term Care; trends over time. Arch Surg. 2012;147(5):474-479.
Administrative, technical, or material support: Immigration, Refugees and Citizenship Canada doi:10.1001/archsurg.2011.1693
Cusimano, Baxter, Garg. Permanent Resident Database; Cancer Care
jamainternalmedicine.com (Reprinted) JAMA Internal Medicine Published online May 3, 2021 E7
© 2021 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Duke Medical Center Library User on 05/12/2021Research Original Investigation Delay of Pregnancy Among Physicians vs Nonphysicians
7. Troppmann KM, Palis BE, Goodnight JE Jr, administrative health database. BMC Med Inform perceived career threats? Acad Med. 2010;85(4):
Ho HS, Troppmann C. Women surgeons in the new Decis Mak. 2016;16(1):135. doi:10.1186/s12911-016- 640-646. doi:10.1097/ACM.0b013e3181d2cb5b
millennium. Arch Surg. 2009;144(7):635-642. 0375-3 24. Kin C, Yang R, Desai P, Mueller C, Girod S.
doi:10.1001/archsurg.2009.120 16. Canadian Institute for Health Information. Female trainees believe that having children will
8. Stentz NC, Griffith KA, Perkins E, Jones RD, Health Indicators 2013: Definitions, Data Sources, negatively impact their careers: results of a
Jagsi R. Fertility and childbearing among american and Rationale. Canadian Institute for Health quantitative survey of trainees at an academic
female physicians. J Womens Health (Larchmt). Information; 2013. medical center. BMC Med Educ. 2018;18(1):260.
2016;25(10):1059-1065. doi:10.1089/jwh.2015.5638 17. Wilkins R. Neighbourhood income quintiles doi:10.1186/s12909-018-1373-1
9. Aghajanova L, Hoffman J, Mok-Lin E, derived from Canadian postal codes are apt to be 25. Rangel EL, Castillo-Angeles M, Changala M,
Herndon CN. Obstetrics and gynecology residency misclassified in rural but not urban areas. Accessed Haider AH, Doherty GM, Smink DS. Perspectives of
and fertility needs. Reprod Sci. 2017;24(3):428-434. April 1, 2021. https://www.researchgate.net/ pregnancy and motherhood among general surgery
doi:10.1177/1933719116657193 publication/301488517_Neighbourhood_income_ residents: a qualitative analysis. Am J Surg. 2018;
10. Lean SC, Derricott H, Jones RL, Heazell AEP. quintiles_derived_from_Canadian_postal_codes_are_ 216(4):754-759. doi:10.1016/j.amjsurg.2018.07.036
Advanced maternal age and adverse pregnancy apt_to_be_misclassified_in_rural_but_not_urban_ 26. Humphries LS, Lyon S, Garza R, Butz DR,
outcomes: a systematic review and meta-analysis. areas Lemelman B, Park JE. Parental leave policies in
PLoS One. 2017;12(10):e0186287. doi:10.1371/ 18. Johns Hopkins University Bloomberg School of graduate medical education: a systematic review.
journal.pone.0186287 Public Health, Health Services Research & Am J Surg. 2017;214(4):634-639. doi:10.1016/j.
11. Frederiksen LE, Ernst A, Brix N, et al. Risk of Development Center. The Johns Hopkins ACG amjsurg.2017.06.023
adverse pregnancy outcomes at advanced maternal Case-Mix System Version 10.0 Release Notes. 27. Phillips SP, Richardson B, Lent B. Medical
age. Obstet Gynecol. 2018;131(3):457-463. doi:10. The Johns Hopkins University; 2011. faculty’s views and experiences of parental leave:
1097/AOG.0000000000002504 19. Austin PC. Balance diagnostics for comparing a collaborative study by the Gender Issues
12. Wang YJ, Chiang SC, Chen TJ, Chou LF, the distribution of baseline covariates between Committee, Council of Ontario Faculties of
Hwang SJ, Liu JY. Birth trends among female treatment groups in propensity-score matched Medicine. J Am Med Womens Assoc (1972). 2000;
physicians in Taiwan: a nationwide survey from samples. Stat Med. 2009;28(25):3083-3107. 55(1):23-26.
1996 to 2013. Int J Environ Res Public Health. 2017; doi:10.1002/sim.3697 28. MacVane CZ, Fix ML, Strout TD,
14(7):E746. doi:10.3390/ijerph14070746 20. Sutradhar R, Baxter NN, Austin PC. Terminating Zimmerman KD, Bloch RB, Hein CL.
13. Statistics Canada. Live births and fetal deaths observation within matched pairs of subjects in a Congratulations, you’re pregnant! now about your
(stillbirths), by place of birth (hospital or matched cohort analysis: a Monte Carlo simulation shifts…: the state of maternity leave attitudes and
non-hospital). Accessed April 12, 2020. https:// study. Stat Med. 2016;35(2):294-304. doi:10.1002/ culture in EM. West J Emerg Med. 2017;18(5):
www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid= sim.6621 800-810. doi:10.5811/westjem.2017.6.33843
1310042901 21. Lerner LB, Stolzmann KL, Gulla VD. Birth trends 29. Hutchinson AM, Anderson NS III, Gochnour GL,
14. Cusimano MCBN, Baxter NN, Sutradhar R, et al. and pregnancy complications among women Stewart C. Pregnancy and childbirth during family
Reproductive patterns, pregnancy outcomes and urologists. J Am Coll Surg. 2009;208(2):293-297. medicine residency training. Fam Med. 2011;43(3):
parental leave practices of women physicians in doi:10.1016/j.jamcollsurg.2008.10.012 160-165.
Ontario, Canada: the Dr Mom Cohort Study 22. Gabbe SG, Morgan MA, Power ML, Schulkin J, 30. Juengst SB, Royston A, Huang I, Wright B.
protocol. BMJ Open. 2020;10(10):e041281. doi:10. Williams SB. Duty hours and pregnancy outcome Family leave and return-to-work experiences of
1136/bmjopen-2020-041281 among residents in obstetrics and gynecology. physician mothers. JAMA Netw Open. 2019;2(10):
15. Chiu M, Lebenbaum M, Lam K, et al. Describing Obstet Gynecol. 2003;102(5 Pt 1):948-951. e1913054. doi:10.1001/jamanetworkopen.2019.13054
the linkages of the immigration, refugees and 23. Willett LL, Wellons MF, Hartig JR, et al.
citizenship Canada permanent resident data and Do women residents delay childbearing due to
vital statistics death registry to Ontario’s
E8 JAMA Internal Medicine Published online May 3, 2021 (Reprinted) jamainternalmedicine.com
© 2021 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Duke Medical Center Library User on 05/12/2021You can also read