CURRENT AND FUTURE PERSPECTIVES OF THERANOSTICS IN THE FIELD OF NETS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CURRENT AND FUTURE PERSPECTIVES OF THERANOSTICS IN THE FIELD OF NETS Philippe Ruszniewski1, Rachida Lebtahi2, Louis de Mestier1 Université de Paris, Department of Gastroenterology-Pancreatology, Beaujon Hospital (APHP), Clichy, France Université de Paris, Department of Nuclear Medicine, Beaujon Hospital (APHP), Clichy, France

LEARNING OBJECTIVES 1. Provide principles of the use of theranostics in NETs 2. Provide current applications of theranostics in NETs 3. Provide perspectives of theranostics in NETs
INTRODUCTION TO NEUROENDOCRINE TUMOURS (NETs) NETs are rare neoplasms with increasing incidence of approximately 7/100,000 per year1 Most NETs arise from the digestive (75%) and pulmonary (25%) systems Most NETs are associated with metastases Survival of patients with metastatic NETs is often prolonged (5-year OS rate, 50–70%) The main prognostic factors of NETs are the primary tumour site, stage, grade (Ki-67), tumour growth rate and tumour burden2,3 1. Dasari A, et al. JAMA Oncol 20173(10):1335–42; 2. Pavel M, et al. ESMO guidelines. Ann Oncol 2020;31(7):844–60; 3. de Mestier L, et al. French Intergroup Guidelines. Dig Liver Dis 2020;52(5):473–92. Images courtesy of Beaujon Hospital (APHP), Clichy, France.

INTRODUCTION TO NETs
Therapeutic options for non-resectable NETs include1,2,3
◆Long-acting somatostatin analogues (lanreotide, octreotide)
◆Systemic chemotherapy (alkylating agents, platinum-based)
◆Transarterial (chemo)-embolisation
◆Everolimus
◆Sunitinib
◆Peptide receptor-radionuclide therapy (177Lu-DOTATATE)
Therapeutic decision making mostly relies on prognostic factors1,2,3
◆These treatments have not/poorly been compared between them
◆Factors predictive of their efficacy have yet to be determined
◆Importance of multidisciplinary expert discussions
Need to move towards precision medicine!
1. Pavel M, et al. ESMO guidelines. Ann Oncol 2020;31(7):844–60; 2. de Mestier L, et al. French Intergroup Guidelines. Dig Liver Dis 2020;52(5):473–92.
3. Pavel M, et al. ENETS guidelines. Neuroendocrinology 2016;103(2):172–85.
Images courtesy of Beaujon Hospital (APHP), Clichy, France.
PRINCIPLES OF THE USE OF THERANOSTICS IN NETs
DEFINING « THERANOSTICS » Neologism deriving from the contraction of the terms "therapeutic" and "diagnostics” Use of a diagnostic test, identifying a marker, to guide the patient's therapy according to their status for the marker (positive or negative status for a binary marker)

PRINCIPLE OF THERANOSTICS:
TREATING WHAT WE SEE
Mechanisms of action of radiopharmaceuticals
Target Vector Link Chelator
Isotope
“Lock” “Key” (Diagnosis / Therapy)
Possible targets: Possible vectors Possible chelators
• G-protein receptors • Peptides agonists • Imaging:
• Somatostatin receptors (SSTR) (ex: edotretotide, oxodetreotide) • 99Tc, 111In
• Gastrin-releasing peptide receptor • Peptides antagonists • 68Ga, 64Cu
• Neurotensin receptor • Antibody • Therapy:
• Antigens: • Amino acids • 177Lu, 90Y
• PSMA • 225Ac
• CD20
• HER2
• Enzymes and inhibitors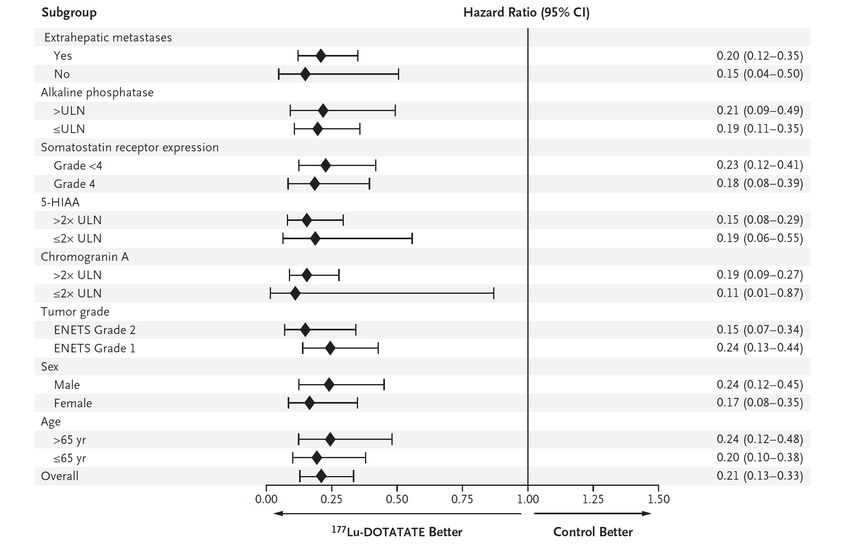
APPLYING THERANOSTICS TO NETs
Digestive NETs present
SSTR overexpression
SSTR imaging
SSTR imaging negative SSTR imaging positive
PRRT is not indicated PRRT could be considered
Image courtesy of Beaujon Hospital (APHP), Clichy, France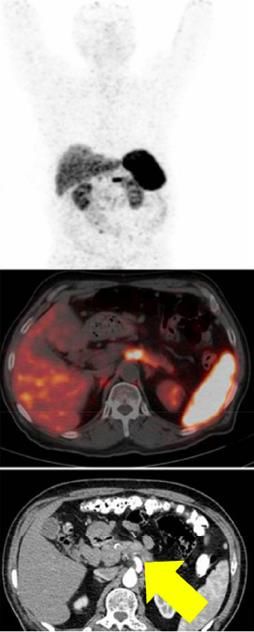
CURRENT APPLICATIONS OF THERANOSTICS IN NETs
SOMATOSTATIN RECEPTOR IMAGING IN NETs
>90% of well-differentiated NETs express somatostatin receptors (SSTR),
especially SSTR2
The fixation of radiolabelled somatostatin analogues on SSTR enables the
cartography of NET localisations1
Somatostatin receptor scintigraphy (111In-Octreoscan)
◆ Sensitivity = 70%
◆ Specificity = 90%
◆ False negatives: accessory spleen, granulomatosis, other cancers, infections
Commonly used for the diagnosis, work-up and follow-up of patients with NETs
1. Ambrosini V, et al. Eur J Nucl Med Mol Imaging 2012;39 Suppl 1:S52–60.
Images courtesy of Beaujon Hospital (APHP), Clichy, France.CLINICAL BENEFIT OF 68GALLIUM-DOTA-X PET
68Gallium-DOTA-X PET developed in the last two decades1
◆ Quicker examination and less radiation used
◆ Increased spatial resolution and accuracy
◆ Increased sensitivity, similar specificity
68Gallium-DOTA-X PET identifies more lesions than 111In-scintigraphy
and can thus modify clinical management:
Identification of 78% additional lesions than 111In-scintigraphy1
◆
Identification of 60% additional lesions than CT/MRI scans2
◆
Impact on clinical management for 71% of patients who
◆
had 111In-scintigraphy3
111In-Octreoscan 68Ga-DOTATOC PET
1. Buchmann I, et al. Eur J Nucl Med Mol Imaging 2007; 2. Frilling A, et al. Ann Surg 2010; 3. Srirajaskanthan R, et al. J Nucl Med 2010.
Images courtesy of Beaujon Hospital (APHP), Clichy, France.CLINICAL BENEFIT OF 68GALLIUM-DOTA-X PET
Meta-analysis of 18 studies (1143 patients) on the detection rate of primary pNETs1
Pooled sensitivity was 79.6% (71–87)
◆
Pooled specificity was 95% (75–100)
◆
Per-lesion detection rate of primary pNETs was 92.1% Per-patient detection rate of primary pNETs was 80.6%
1. Bauckneht M, et al. Diagnostics 2020;10(8):598. Reproduced under the terms of the Creative Commons Attribution, Attribution 4.0 International licence (CC BY 4.0; available at:
https://creativecommons.org/licenses/by/4.0/; accessed Jul 2021).CLINICAL BENEFIT OF 68GALLIUM-DOTA-X PET
Meta-analysis of 22 studies on the diagnostic performances in digestive NETs1
68Gallium-DOTA-X PET impacted the clinical
management for 45% of patients
Diagnostic performances of
68Gallium-DOTA-X PET for
initial diagnosis and work-up
were:
Sensitivity 91% (85%-94%)
Specificity 94% (86%-98%)
1. Singh S, et al. t68Ga PET Imaging in Patients With Neuroendocrine Tumors: A Systematic Review and Meta-analysis,Clin Nucl Med 2018; 43(11):802–10.
Available at: https://journals.lww.com/nuclearmed/Abstract/2018/11000/68Ga_PET_Imaging_in_Patients_With_Neuroendocrine.3.aspx; accessed July 2021.PRACTICAL BENEFIT OF 68GALLIUM-DOTA-X PET
68Gallium-DOTA-X PET enables:
◆ Better spatial resolution than Octreoscan
◆ Quicker image acquisition (90 min, vs. 24–48 h for Octreoscan)
◆ Less patient (and caregivers) irradiation (effective dose in MBq is 111In-Octreoscan
3–5 times less than Octreoscan)
◆ No use of laxatives (required with Octreoscan)
68Ga-DOTATOC PET
Images courtesy of Beaujon Hospital (APHP), Clichy, France.APPLYING THERANOSTICS TO NETs
SSTR imaging positive
111In-Octreoscan
68Ga-DOTA-X PET
PRRT could be considered
177Lu-DOTATATE
(90Y-DOTATATE/TOC)
Image courtesy of Beaujon Hospital (APHP), Clichy, France.NETTER-1 STUDY: OBJECTIVES AND DESIGN
Evaluate the efficacy and safety of 177Lu-DOTATATE plus octreotide 30 mg compared with
Aim octreotide LAR 60 mg in patients with inoperable, SSTR positive, midgut NET, progressive
under octreotide LAR 30 mg
Design International, multicenter, randomised, comparator-controlled, parallel-group
Treatment and Assessments
Progression-free survival (RECIST criteria) every 12 weeks
Dose 1 Dose 2 Dose 3 Dose 4
4 administrations of 7.4 GBq of 177Lu-DOTATATE q6w
n=115
Baseline + Octreotide 30 mg
5 years
and
follow-up
randomisation
n=115 Octreotide LAR 60 mg every 4 weeks
Strosberg J, et al. N Engl J Med 2017;376(2):125–35.NETTER -1 STUDY: OBJECTIVES
Primary objective
Compare PFS after treatment with 177Lu-DOTATATE plus octreotide 30 mg vs. octreotide LAR 60 mg
◆
Secondary objectives
Compare the objective response rate between study arms
◆
Compare the overall survival between study arms
◆
Compare the time to progression between study arms
◆
Evaluate the safety and tolerability of 177Lu-DOTATATE
◆
Evaluate the health-related quality of life (QoL) as measured by the EORTC QLQ-G.I.NET21 questionnaire
◆
Hypotheses
Median PFS 30 months (177Lu-DOTATTATE) vs. 14 months (octreotide 60 mg)
◆
230 patients to randomise (115 in each arm)
◆
Strosberg J, et al. N Engl J Med 2017;376(2):125–35.NETTER -1 STUDY: MAIN INCLUSION CRITERIA Patients ≥18 years of age Metastatic or locally advanced, inoperable, histologically proven, midgut NET Ki67 index ≤ 20% (Grade 1-2) Progressive disease (RECIST Criteria 1.1 centrally confirmed) on uninterrupted fixed dose of octreotide LAR (20–30 mg every 3–4 weeks) Somatostatin receptor positive disease Karnofsky Performance Score ≥60 Including functioning and non-functioning Strosberg J, et al. N Engl J Med 2017;376(2):125–35.
NETTER -1: POPULATION CHARACTERISTICS
177Lu-Dotatate Octreotide LAR 60 mg
(n=116) (n=113)
Gender, n (%)
Male 53 (46) 60 (53)
Female 63 (54) 53 (47)
Age (years), mean (SD) 63 (±9) 64 (±10)
Primary tumour site, n (%)
Jejunum 6 (5) 9 (8)
Ileum 86 (74) 82 (73)
Appendix 1 (1) 2 (2)
Right colon 3 (3) 1 (1)
Other 20 (17) 19 (17)
Site of metastases, n (%)
Liver 97 (84) 94 (83)
Lymph nodes 77 (66) 65 (58)
Bone 13 (11) 12 (11)
Lungs 11 (10) 5 (4)
Other 40 (35) 37 (33)
Strosberg J, et al. N Engl J Med 2017;376(2):125–35.NETTER -1: POPULATION CHARACTERISTICS
177Lu-Dotatate Octreotide LAR 60mg
(n=116) (n=113)
WHO grade, n (%)
Grade 1 76 (66) 81 (72)
Grade 2 40 (34) 32 (28)
SRS, Krenning scale, n (%)
Grade 2 11 (10) 12 (11)
Grade 3 34 (29) 34 (30)
Grade 4 71 (61) 67 (59)
Chromogranin A (µg/L), median (IQR) 604 (247–2626) 648 (290–2674)
5-HIAA (mg/24 h), median (IQR) 36 (17–126) 44 (21–92)
Strosberg J, et al. N Engl J Med 2017;376(2):125–35.NETTER -1: POPULATION CHARACTERISTICS
177Lu-Dotatate Octreotide
(n=116) (n=113)
Previous tumour resection, n (%) 90 (78) 93 (82)
Previous tumour ablation, n (%) 6 (5) 11 (10)
Targeted therapy 19 (16) 17 (15)
Embolisation, n (%) 18 (16) 13 (12)
Chemotherapy 11 (9) 14 (12)
Other treatments 20 (17) 18 (16)
Strosberg J, et al. N Engl J Med 2017;376(2):125–35.NETTER -1: 177LU-DOTATATE EXPOSURE
Patients who completed treatment phase (n=102*) Patients, n (%)
Drug exposure, n (%)
800 mCi (29.6 GBq) 81 (79)
400–800 mCi (14.8–29.6 GBq) 5 (5)
200–400 mCi (7.4–14.8 GBq) 9 (9)
200 mCi (7.4 GBq) 3 (3)
No administration 4 (4)
Number of administrations, n (%)
4 78 (76)
3 5 (5)
2 11 (11)
1 4 (4)
0 4 (4)
Dose-modifying toxicity, n (%)
All treated patients (N=111)
No DMT 105 (95)
DMT 6 (5)
*14 patients still under treatment
Strosberg J, et al. N Engl J Med 2017;376(2):125–35.NETTER -1: PROGRESSION-FREE SURVIVAL
All progressions centrally confirmed and independently reviewed for eligibility
177Lu-DOTATATE Control
(n=116) (n=113)
Events, n (%) 21 (18.1) 70 (61.9)
PFS, median (95% CI) Not reached (NR) 8.5 (5.8, 9.1)
Unstratified HR (95% CI) 0.177 (0.108, 0.289)
Unstratified p-valueNETTER -1: PFS BENEFIT IN ALL SUBGROUPS From N Engl J Med, Strosberg J, et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors,376, 125–35. Copyright © 2017 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
NETTER -1: PFS DEPENDING ON LIVER
TUMOUR BURDEN
Baseline Median PFS HR
Treatment arm N P-value
LTB (months) (95% CI)
177Lu-DOTATATE 71 28.35 0.22NETTER -1: TUMOUR RESPONSE RATE
177Lu-DOTATATE
Octreotide LAR 60 mg
+ octreotide LAR 30 mg
(n=100)
(n=101)
Complete response, n (%) 1 (1) 0
Partial response, n (%) 17 (17) 3
Stable disease, n (%) 77 (66) 70 (62)
Progressive disease, n (%) 5 (4) 27 (24)
Objective response rate 18% 3% PNETTER -1: OVERALL SURVIVAL (INTERIM ANALYSIS)
p=0.0094
Strosberg J, et al. ESMO 2018. With permission from Dr J. Strosberg.NETTER -1: ADVERSE EVENTS
177Lu-DOTATATE + octreotide 30 mg (n=111) Octreotide 60 mg (n=110)
% All grades Grade 3–4 All grades Grade 3–4
Nausea 59 4 12 2
Vomiting 47 7 10 0
Diarrhoea 29 3 19 2
Abdominal pain 26 3 26 5
Fatigue 40 2 25 2
Peripheral oedemas 14 0 7 0
Thrombocytopenia 25 2 1 0
Lymphopenia 18 9 2 0
Anaemia 14 0 5 0
Neutropenia 5 1 1 0
Musculoskeletal pain 29 2 20 1
Appetite loss 18 0 8 3
Headaches 16 0 5 0
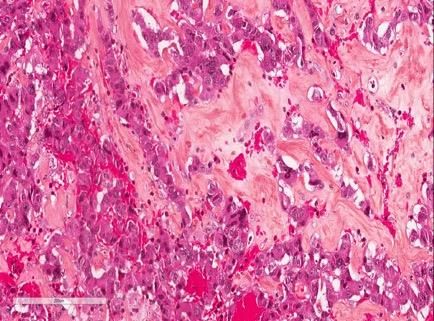
Strosberg J, et al. N Engl J Med 2017;376(2):125–35.NETTER -1: HEALTH-RELATED QUALITY OF LIFE
Global Health Status Physical
functioning
Role (social) functioning Fatigue
Strosberg J, et al. Health-Related Quality of Life in Patients With Progressive Midgut Neuroendocrine Tumors Treated With 177Lu-Dotatate in the Phase III NETTER-1 Trial. J Clin Oncol
2018;36(25):2578–84. Available at: https://ascopubs.org/doi/abs/10.1200/JCO.2018.78.5865; accessed Jul 2021. © 2018 by American Society of Clinical Oncology.NETTER -1: HEALTH-RELATED QUALITY OF LIFE
Pain Diarrhoea
Disease-related
Body image
worries
Strosberg J, et al. Health-Related Quality of Life in Patients With Progressive Midgut Neuroendocrine Tumors Treated With 177Lu-Dotatate in the Phase III NETTER-1 Trial. J Clin Oncol
2018;36(25):2578–84. Available at: https://ascopubs.org/doi/abs/10.1200/JCO.2018.78.5865; accessed Jul 2021. © 2018 by American Society of Clinical Oncology.NETTER -1: SUMMARY AND CONCLUSIONS
First prospective randomised study in patients with progressive metastatic midgut NETs
177Lu-Dotatate
+ Octreotide 30 mg was superior to Octreotide 60 mg in terms of PFS (NR vs. 8.4 months; pPRRT SHORT- AND LONG-TERM TOXICITY
Nausea and vomiting1
◆≈50% of patients
◆IV bolus of antiemetic medication at least 30 minutes prior to amino acid solution
Renal toxicity1,2,3
◆ Chronic failure is rare (HIGHER RISK OF ADVERSE EVENTS DURING
177LU-DOTATATE TREATMENT
Bone
metastases
Previous oncologic radiometabolic therapies Renal or urinary tract
with 131I-compounds abnormalities
Recommendation to
History of other malignant tumours monitor these Hematologic toxicity ≥G2
unless in remission for ≥5 years patients more (CTCAE) before treatment
frequently during
treatment
Urinary incontinence Mild to moderate chronic
kidney disease
Previous
chemotherapyCURRENT INDICATIONS OF PRRT IN NETs
Lutathera®: 4 infusions of 7,4 MBq each, every 8 weeks + amino acid solution IV
over 4 hours, starting 30 minutes prior to start of Lutathera® infusion
Therapeutic indications Contraindications
◆ Age ≥18 years ◆ Hypersensitivity to the active substance, to any of the excipients
◆ Gastro-enteropancreatic NETs ◆ Established or suspected pregnancy
◆ Well differentiated Grade 1 or Grade 2 ◆ Kidney failure with creatinine clearanceMODERN PIVOTAL PHASE 3 TRIALS IN
ADVANCED NETs
Randomised Tumour Tumour Objective PFS
Agent OS Tolerance
trial(s) type status response (%) (m)
Octreotide1 PROMID Midgut UnknownESMO 2020 GUIDELINES FOR ADVANCED NEUROENDOCRINE NEOPLASMS1 1. Pavel M, et al. Ann Oncol 2020;31(7):844-860. © 2020 European Society for Medical Oncology. Published by Elsevier Ltd. All rights reserved.
PERSPECTIVES OF THERANOSTICS IN NETs
PERSPECTIVE OF UTILISATION OF PRRT IN NETs
Current indication:
“Treatment of unresectable or metastatic, progressive, well differentiated (G1 and G2), somatostatin-receptor
positive gastroenteropancreatic neuroendocrine tumours (GEP-NETs) in adults”
◆ Unresectable – For ever? Could neoadjuvant PRRT render a NET amenable to surgery?
◆ Progressive – After SST analogues? Further line? What about first-line PRRT for more aggressive NETs?
◆ G1 and G2 NETs – What about G3?
◆ Gastroenteropancreatic – What about other primaries?
◆ Retreatment with additional PRRT courses – possible and useful when disease progresses after
initial response?
◆ Other routes of administration – selective intra-arterial PRRT?PRRT AS A NEOADJUVANT THERAPY?
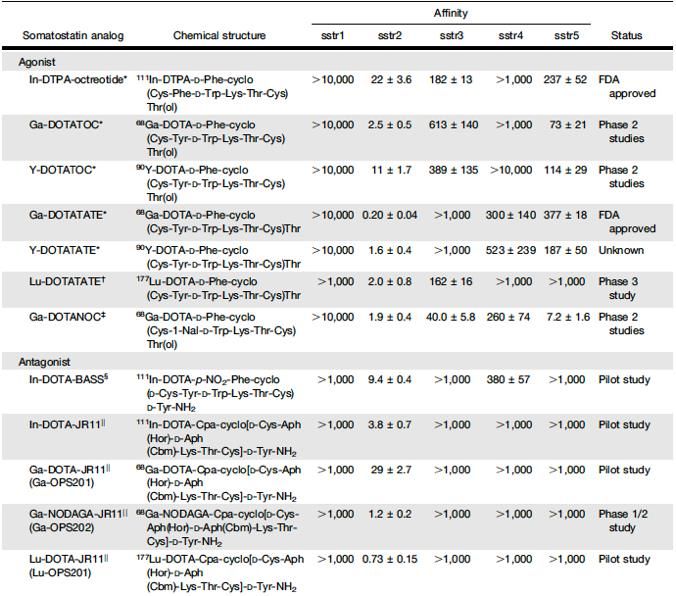
Mrs E, 35 y, jaundice, NET G2 of the pancreatic head encasing the SMV,
with 4 liver metastases
Cycle 1
Cycle 4
Courtesy of Beaujon Hospital (APHP), Clichy, France.Lame Superior mesenteric
rétroporte vein
Posterior
Anterior
face
face
NET
Central
necrosis
Duodenum
Courtesy of Beaujon Hospital (APHP), Clichy, France.PRRT AS A NEOADJUVANT THERAPY?
Retrospective study of 29 patients with non-functioning pancreatic NETs1
All pancreatic NETs were locally borderline or unresectable
Group 1: no metastases; group 2: ≤3 metastases; group 3: >3 metastases
9/29 patients (31%) had PNETs resectable after neoadjuvant PRRT
Characteristic Successful surgery Unresectable P-value
Patients, n 9 20
Men, n 5 9 0.70
Mean age, y 52 (41–71) 56 (32–81) 0.46
Mean longest-diameter tumour at baseline, mma 72 (36–100) 69 (21–120) 0.79
Tumour uptake on 177Lu-octreotate
Equal to normal liver 0 2 0.47
More than normal liver 4 11
More than kidneys 5 7
Previous therapy 3 5 0.68
Octreotide 0 3 0.53
Surgery 3 4 0.64
Radiotherapy 0 1 1.00
Chemotherapy 0 0 NA
Median total administered dose, GBq 30.0 (22.3–30.3) 29.8 (11.2–30.2) 0.10
Regression (complete response/partial
8 11 0.11
response/minor response) as treatment outcome†
Mean alkaline phosphatase level at baseline, U/L‡ 470 (210–954) 383 (134–1109) 0.74
Location of tumour
Pancreatic head 8 15 0.63
Pancreatic body or tail 1 5
*Data on longest-diameter pancreatic tumour available for all patients with and 18/20 patients without successful surgery after 177Lu-octreotate (in 2 patients only liver metastases could be measured).
† Confirmed response 3 mo after treatment according to Southwest Oncology Group solid tumour response criteria.
‡ In patients with elevated levels at baseline (normal level,PRRT AS A NEOADJUVANT THERAPY?
Surgical feasibility, efficacy and determinants of neoadjuvant PRRT with
177Lu-DOTATATE for locally advanced unresectable GEP-NETs (n=57)
Group 1: Without liver Group 2: Without potentially
metastases resectable liver metastases
177Lu-DOTATATE PRRT (n=57)
[dose = 7.4 GBq (200 mCi) per cycle]
26.3% primary became resectable Factors associated with higher rate of
Complete or partial response resectability following PRRT:
◆ Symptomatic: 84% ◆ Size of primary tumourPRRT FOR G3 NETs?
Retrospective cohort study in 12 European Centres1
149 NET patients Pancreas 60%, GI 23%, unknown primary 17%
G3 NENs G3 NETs 40%, NEC 42%, unknown 18%
PRRT First line 20%, second line 42%, later lines 39%; progressive 70%
114 evaluable CR 1%, PR 41%, SD 38%, PD 20%
PRRT Response (n=114) and outcomes (n=149) in GEP NEN G3
CR, n (%) PR, n (%) SD, n (%) PD, n (%) PFS, m (95% CI) OS, m (95% CI)
All patients 1 (1) 47 (41) 43 (38) 23 (20) 14 (10.4, 17.6) 29 (23.3, 34.7)
Performance status
0 1 (2) 21 (36) 26 (45) 10 (17) 16 (11.0, 21.0) 39 (28.1, 49.9)
1 0 17 (53) 8 (25) 7 (22) 14 (8.2, 19.8) 23 (16.2, 29.8)
2 0 3 (38) 2 (25) 3 (38) 3 (0, 6.2) 4 (0, 12.6)
Primary tumour site
Pancreas 0 32 (48) 23 (34) 12 (18) 14 (10.4, 17.6) 29 (21.7, 36.3)
Gastrointestinal 0 11 (42) 9 (35) 6 (23) 10 (0, 21.2) 31 (7.5, 54.5)
Unknown 1 (5) 4 (19) 11 (52) 5 (24) 16 (8.4, 23.6) 29 (11.4, 46.6)
Differentiation and proliferation
NETcG3 0 18 (42) 22 (51) 3 (7) 19 (14.4, 23.6) 44 (25.3, 62.7)
NEC; Ki-67 21–54% 1 (3) 16 (41) 12 (31) 10(26) 11 (5.4, 16.6) 22 (16.0, 28.0)
NEC; Ki-67 ≥55% 0 5 (45) 1 (9) 5 (45) 4 (0.8, 7.2) 9 (1.6, 16.4)
Statistically significant results are in bold text
1. Used with permission of the Society for Endocrinology from Endocr Relat Cancer, Carlsen EA, et al. Endocr Relat Cancer 2019;26(2):227–39. Permission conveyed through the
Copyright Clearance Center Inc.OTHER PRIMARY NETs?
RETROSPECTIVE ERASMUS STUDY1
Patients received ≥100 mCi
177Lu-DOTATATE
N=1214
Objectives Dutch patients Foreign patients
Evaluate efficacy and tolerance of 177Lu-DOTATATE
◆
n=810 n=404
(4 cycles of 7.4 GBq every 8 weeks) together with
amino acid perfusion Bronchial and GEP-NET
Other tumours
Objective response rate patients
◆
n=114
n=696
Clinical and biological tolerance
◆
PFS, OS, QoL
◆
Did not meet all Patients treated
Inclusion criteria inclusion criteria* according to the protocol Safety analysis
Digestive/bronchial SSTR+ NETs
◆ n=86 n=610
Nonresectable with curative intent
◆
Life expectancy >12 weeks
◆ Treated with ≥600 mCi
Treated with 50
◆ 177Lu-DOTATATE n=88 177Lu-DOTATATE Efficacy and
before 2013 survival analysis
Adequate organ functions or after 2013 n=79
◆ n=610
1. Brabander T, et al. Clin Cancer Res 2017;23(16):4617–24.OTHER PRIMARY NETs?
RETROSPECTIVE ERASMUS STUDY1
Characteristics Patients, n (%) Characteristics Patients, n (%)
Male gender 230 (52) Bone metastases 70 (16)
Median age (range) 60 years (30–83) Liver metastases 346 (78)
Primary tumour site Functional pancreatic NET 21 (5)
Midgut 181 (41) Median time since diagnosis (range) 14 months (0–371)
Hindgut 12 (3) Baseline progression 239 (54)
Pancreas 133 (30) Extent of disease
Bronchial 23 (5) Limited 62 (14)
Other foregut 12 (3) Moderate 314 (71)
Unknown 82 (19) Extensive 67 (15)
Pretreatment Uptake on Octreoscan
Surgery 190 (43) Grade 2 35 (8)
Chemotherapy 28 (6) Grade 3 278 (63)
Somatostatin analogues 271 (61) Grade 4 130 (29)
1. Brab Brabander T, et al. Clin Cancer Res 2017;23(16):4617–24.OTHER PRIMARY NETs?
RETROSPECTIVE ERASMUS STUDY1
Best response, PFS, TTP and OS after therapy with 177Lu-DOTATATE
Primary NET Total CR PR SD PD NE Median PFS Median TTP Median OS
Location n n (%) n (%) n (%) n (%) n (%) (months) (months) (months)
Midgut 181 2 (1) 55 (30) 99 (55) 16 (9) 9 (5) 30 42 60
Non-PD 32 0 (0) 10 (31) 18 (56) 3 (9) 1 (3) 24 45 82
PD 94 1 (1) 28 (30) 50 (53) 9 (10) 6 (6) 29 40 50
Hindgut 12 0 (0) 4 (33) 6 (50) 1 (8) 1 (8) 29 29 Not defined
Pancreatic 133 6 (5) 66 (50) 40 (30) 17 (13) 4 (3) 30 31 71
Non-PD 21 1 (5) 9 (43) 10 (48) 1 (5) 0(0) 31 31 Not defined
PD 66 2 (3) 36 (55) 15 (23) 10 (15) 3 (5) 31 36 71
Functional 21 1 (5) 12 (57) 4 (19) 3 (14) 1(5) 30 33 Not defined
Nonfunctional 112 5 (4) 54 (48) 36 (32) 14 (13) 3 (13) 30 31 69
Bronchial 23 0 (0) 7 (30) 7 (30) 6 (26) 3 (13) 20 25 52
Other foregut ͣ 12 1 (8) 4 (33) 5 (42) 2 (17) 0 (0) 25 Not defined Not defined
Unknown 82 0 (0) 29 (35) 35 (43) 11 (13) 7 (9) 29 37 53
Total 443 9 (2) 165 (37) 192 (43) 53 (12) 24 (5) 29 36 63
ͣincluding five tumours of the stomach, five of the duodenum and two of the thymus
1. Brabander T, et al. Clin Cancer Res 2017;23(16):4617–24.OTHER PRIMARY NETS? RETROSPECTIVE ERASMUS STUDY1 In the total population: Median OS: 63 months (95% CI: 55, 72) Median PFS: 29 months (95% CI: 26, 33) Median OS in according to location of the primary tumour1 Median OS in according to tumour Grade2 1. Reprinted from Clin Cancer Res, 2017, 23(16), 4617–24, Brabander T, et al. Long-Term Efficacy, Survival, and Safety of [177Lu-DOTA0,Tyr3]octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors, with permission from AACR; 2. Courtesy of Prof T Brabander; unpublished data from Erasmus MC.
OCCLURANDOM TRIAL Ongoing Phase 2 trial (n=80) Will provide prospective results for pancreatic NETs Comparator as per guidelines and more “credible” than high-dose SST analogues Patients with 177Lu-DOTATATE (7.4 GBq x pancreatic NETs: 4 cycles every 8 weeks) Primary endpoint: Advanced non-resectable 12-month PFS rate Progressive post-1st line R 1:1 SSTR uptake ≥ liver OS, response, QoL, Evaluable by RECIST 1.1 Sunitinib (37.5 mg/d) toxicity Life expectancy >8 mo
COMPETE TRIAL
Ongoing open-label Phase 3 trial (n=300)
Will provide prospective results for pancreatic NETs, 177Lu-DOTATOC
Comparator as per guidelines and more “credible” than high-dose SST analogues
177Lu-DOTATATE (7.5 GBq x
Patients with pancreatic or
4 cycles every 3 months) Primary endpoint:
gastroenteric NETs:
PFS
Advanced non-resectable
R 1:1
Progressive post-1st line
OS, response, QoL,
SSTR uptake ≥ liver
Everolimus (10 mg/d) toxicity
Evaluable by RECIST 1.1NETTER-2 TRIAL
Ongoing open-label Phase 3 trial (n=222)
Will provide prospective results for NET with high Ki67, and pancreatic NETs
Will provide prospective results in the first-line setting
Patients with pancreatic or
177Lu-DOTATATE (7.5 GBq x
gastroenteric NETs:
4 cycles every 8 weeks) Primary endpoint:
Ki-67 between 10 and 55%
PFS
Diagnosed within 6 months
R 1:1
Non-progressive
OS, response, QoL,
Advanced non-resectable Octreotide high dose toxicity
SSTR uptake > liver (60 mg every 4 weeks)
Evaluable by RECIST 1.1RECHALLENGING PRRT UPON PROGRESSION? Mr K, 74 y, asthenia, flushes and diarrhoea, ileal NET G1 with liver metastases and carcinoid syndrome Primary tumour/LN surgery, transarterial liver embolisation June 2015: clinical and morphological progression: PRRT → Symptomatic and morphological responses → PFS1 = 36 months (June 2018) August 2018: progression: decision of 2 new cycles of PRRT → Symptomatic response, morphological stability → PFS2 = 18 months (February 2020) February 2020: new liver transarterial embolisation September 2020: everolimus February 2021: still under treatment Images courtesy of Beaujon Hospital (APHP), Clichy, France.
RECHALLENGING PRRT UPON PROGRESSION?
PFS (initial PRRT)
Patients with advanced GEP or bronchial NETs with initial benefit of 4 cycles of
PRRT (PFS >18 months)1
168 patients: new treatment with 2 additional cycles of PRRT
◆
13 patients: third treatment with 2 additional cycles of PRRT
◆
Control group: 99 patients without salvage PRRT (insufficient SRS
◆
uptake, renal/haematological impairment, other treatments)
No. of Best response OS (initial PRRT)
NE Clinical PD
patients CR PR SD PDa
After I-PRRT
Control group 99 0 (0.0) 36 (36.4) 58 (58.6) - 5 (5.1) -
Salvage group 168 1 (0.6) 93 (55.4) 73 (43.5) - 1 (0.6) -
After salvage PRRT
R-PRRT 168 - 26 (15.5) 100 (59.5) 33 (19.6) 1 (0.6) 3 (1.8)
RR-PRRT 13 - 5 (38.5) 7 (53.8) 1 (7.7) - -
aSalvage patients were those with PD after I-PRRT and an initial tumour response of at least SD lasting for at least 18 months from the first
administration of the I-PRRT
1. van Der Zwan WA, et al. Eur J Nucl Med Mol Imaging 2019;46(3):704–17. reproduced under the terms of the Creative Commons CC BY license (available at:
http://creativecommons.org/licenses/by/4.0/; accessed Jul 2021).SELECTIVE INTRA-ARTERIAL PRRT?
Perfusion of NET-related liver metastases is nearly exclusively arterial
Selective intra-arterial infusion of 68Ga-DOTATOC resulted in a 3.75-fold
increase in SUV, compared with IV infusion
No difference in non-tumour liver
Decrease in other non-tumour tissues
intravenous Intra-arterial
68Ga-DOTATOC 68Ga-DOTATOC
Reprinted from Clin Cancer Res, 2019, 16(10), 2899–905, Kratochwil C, et al. Intraindividual Comparison of Selective Arterial versus Venous 68Ga-DOTATOC PET/CT in Patients with
Gastroenteropancreatic Neuroendocrine Tumors, with permission from AACR.SELECTIVE INTRA-ARTERIAL PRRT? 15 patients treated with selective arterial 90Y/177Lu-DOTATATE 60% objective response Acceptable liver/hematologic/renal tolerance 1. Used with permission of the Society for Endocrinology from Endocr Relat Cancer, Kratochwil C, et al. Endocr Relat Cancer 2011;18(5):595–02. Permission conveyed through the Copyright Clearnace Center Inc.
FUTURE PERSPECTIVES OF THERANOSTICS:
ALTERNATIVE RADIOPHARMACEUTICALS
Future radiopharmaceuticals could involve alternative…
…Targets …Vectors …Chelators
• G-protein receptors • Peptides agonists (ex: edotretotide, • Imaging:
• Somatostatin receptors (SSTR) oxodetreotide) • 99Tc, 111In
• Gastrin-releasing peptide receptor • Peptides antagonists • 68Ga, 64Cu
• Neurotensin receptor (ex: satoreotide) • Therapy:
• Antigens: • Antibody • 177Lu, 90Y
• PSMA • Amino acids • 225Ac
• CD20
• HER2
• Enzymes and inhibitors
Target Vector Link Chelator
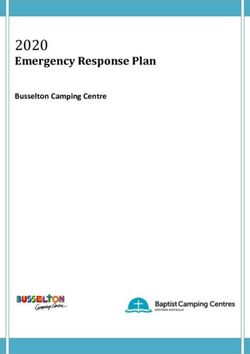
“Lock” “Key” IsotopeALTERNATIVE CHELATOR/VECTORS:
SSTR ANTAGONISTS
Alternative radiolabelled SST analogues could have
increased affinity to SSTRs (especially SSTR2)
JR11 is a high-affinity SSTR antagonist
◆Diagnostic: combined with 68Ga-NODAGA
◆Therapeutic: combined with 177Lu-DOTA
Fani M, et al. J Nucl Med 2017;58(Suppl 2):61S-66S. © 2017 by the Society of Nuclear Medicine and Molecular Imaging, Inc. Available at:
https://jnm.snmjournals.org/content/58/Supplement_2/61S.long; accessed Jul 2021.ALTERNATIVE CHELATOR/VECTORS: SSTR ANTAGONISTS
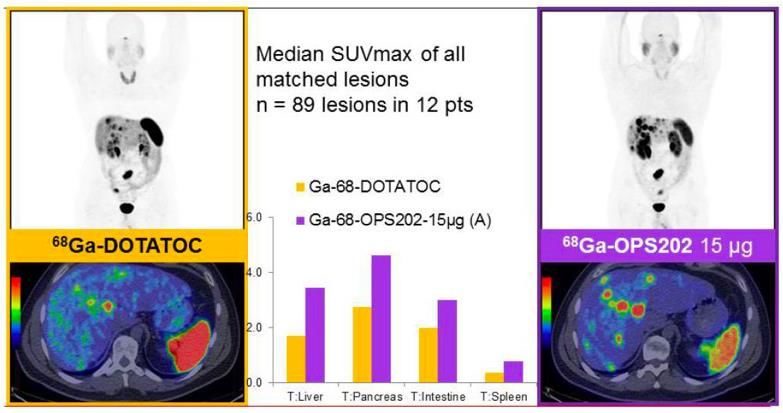
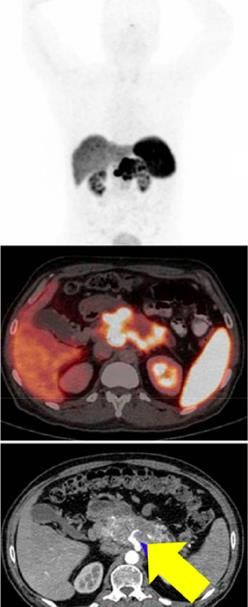
68Ga-NODAGA-JR11 (68Ga-OPS202) was compared with 68Ga-DOTA-TOC
in a Phase 1/2 study in 12 patients with advanced G1/G2 NETs
Sensitivity:
68Ga-NODAGA-JR11: 94%
◆
68Ga-DOTA-TOC: 59%
◆
Tumour uptake was higher using
68Ga-NODAGA-JR11, for lesions of
all localisations
Nicolas GP, et al. J Nucl Med 2018;59(6):915–21. © 2018 by the Society of Nuclear Medicine and Molecular Imaging, Inc. Available at: https://jnm.snmjournals.org/content/59/6/915;
accessed Jul 2021.SOMATOSTATIN RECEPTOR ANTAGONISTS:
PRO/CONS1,2
PROS CONS
Higher specificity to SSTR than agonists Higher organ uptake
Diagnostic: higher tumoural uptake, increased sensitivity Possibly higher toxicity at similar doses
Treatment: possible higher efficacy
Possibly effective in patients with negative SSTR
agonist imaging
1. Wild D, et al. J Nucl Med 2014; 2. Krebs S, et al. Eur J Nucl Med Mol Imag 2020.ALTERNATIVE RADIOPHARMACEUTICALS
Potential targets beyond SSTR1,2,3 Alternative radioisotopes1,2
PSMA: prostate specific membrane antigen
• SST analogues labelled with
177Lu-PSMA and 225Ac-PSMA-617
◆
alpha-emitters
Metastatic castration-resistant prostate cancer
◆ • 225Ac-DOTATATE
• 225Bi-DOTATOC
FAP: fibroblast activation protein (cancer-associated fibroblasts)
177Lu-DOTA-SA-FAP
◆
• Advantage: higher probability of
DNA double strand breaks
Breast cancer ± pancreatic and colon cancers
◆
Others: GLP-1R, CCK2R, CXCR4, HER2
1. Loktev A, et al. J Nucl Med 2018; 2. Ballal S, et al. Eur J Nucl Med Mol Imag 2021; Blakkisrud J, et al. J Nucl Med 2017.TAKE-HOME MESSAGES Theranostics = identifying a marker, to guide the patient's therapy according to their status for the marker SSTR expression can be visualised on 68Gallium-DOTA-X PET → clinical benefit (diagnostic/work-up) If strong uptake on SSTR imaging → clinical benefit of PRRT (177Lu-DOTATATE) PRRT = effective in patients with GEP-NETs (EMA approved) Exact place in the treatment strategy remains to be defined Should be relevant in neoadjuvant setting, G3 NETs, salvage therapy, other primary NETs (e.g., lung NETs) New pharmaceuticals (SSTR antagonists) should be further explored
THANK YOU!
You can also read