COVID-19 vaccines not registered in Australia but in current international use- TGA advice on 'recognition' - Edition 3 - January 2022
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID-19 vaccines not registered in Australia but in current international use- TGA advice on ‘recognition’ Edition 3 – January 2022
Therapeutic Goods Administration
Copyright
© Commonwealth of Australia 2021
This work is copyright. You may reproduce the whole or part of this work in unaltered form for your own personal use or, if
you are part of an organisation, for internal use within your organisation, but only if you or your organisation do not use the
reproduction for any commercial purpose and retain this copyright notice and all disclaimer notices as part of that
reproduction. Apart from rights to use as permitted by the Copyright Act 1968 or allowed by this copyright notice, all other
rights are reserved and you are not allowed to reproduce the whole or any part of this work in any way (electronic or
otherwise) without first being given specific written permission from the Commonwealth to do so. Requests and inquiries
concerning reproduction and rights are to be sent to the TGA Copyright Officer, Therapeutic Goods Administration, PO Box
100, Woden ACT 2606 or emailed to .
2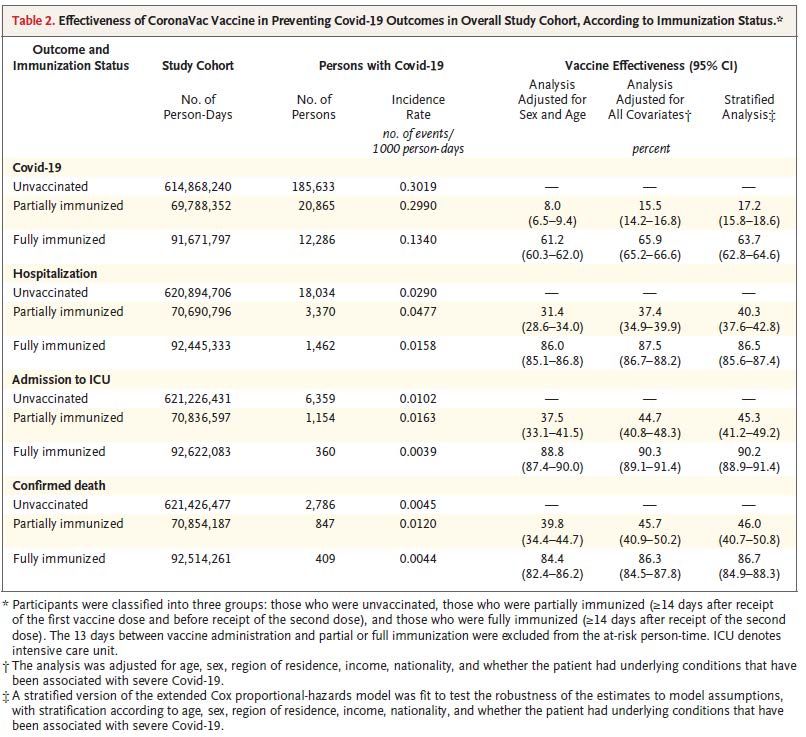
Therapeutic Goods Administration
Contents
Executive summary _____________________________6
Potential use of this information ____________________________________________ 7
Recommendations regarding TGA-registered vaccines _________________ 7
How the estimates were determined _______________________________________ 7
Vaccines approved in Australia______________________________________________ 8
TGA’s updated recommendations on the recognition of
vaccines not registered in Australia ________________9
Assessment of vaccination status in schedules containing
vaccines not registered in Australia _______________11
Omicron COVID-19 variant of concern ____________________________________ 11
Appendix 1.1 Coronavac ________________________12
Coronovac: countries deployed_____________________________________________ 12
Coronovac: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 13
Coronovac: data in non-standard schedules ______________________________ 15
Coronovac: main safety data ________________________________________________ 15
Coronovac: evaluator’s comments _________________________________________ 16
Coronovac: references _______________________________________________________ 20
Appendix 1.2 BBIBP-CorV (Sinopharm) ____________21
Sinopharm: countries deployed ____________________________________________ 21
Sinopharm: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 22
Sinopharm: main safety data _______________________________________________ 24
Sinopharm: evaluator’s comments _________________________________________ 28
Sinopharm: references _______________________________________________________ 31
Appendix 1.3 Covaxin ___________________________31
Covaxin: countries deployed ________________________________________________ 32
Covaxin: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 33
Covaxin: main safety data ___________________________________________________ 34
Covaxin: evaluator’s comments ____________________________________________ 35
3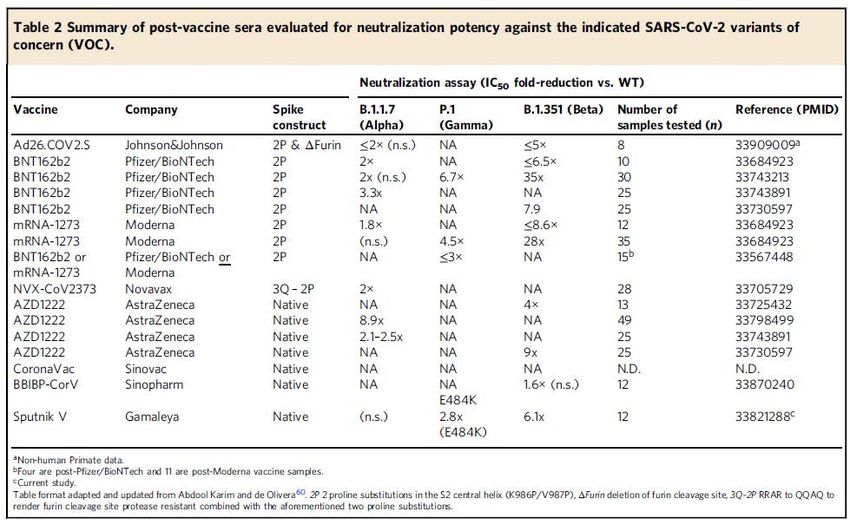
Therapeutic Goods Administration
Covaxin: references __________________________________________________________ 36
Appendix 1.4 Sputnik V _________________________37
Sputnik V: countries deployed ______________________________________________ 37
Sputnik V: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 39
Sputnik V: main safety data _________________________________________________ 41
Sputnik V: additional information _________________________________________ 44
Sputnik V: evaluator’s comments __________________________________________ 44
Sputnik V: references ________________________________________________________ 47
Appendix 1.5 Convidecia ________________________49
Convidecia: countries deployed ____________________________________________ 49
Convidecia: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 50
Convidecia: main safety data ________________________________________________ 51
Convidecia: additional information ________________________________________ 51
Convidecia: evaluator’s comments _________________________________________ 51
Convidecia: references _______________________________________________________ 51
Appendix 1.6 Vaxzevria/Covishield ________________52
Vaxzevria/Covishield: countries deployed _______________________________ 52
Vaxzevria/Covishield: main clinical efficacy and effectiveness data using
standard schedules ___________________________________________________________ 53
Vaxzevria/Covishield: data in non-standard schedules ________________ 54
Vaxzevria/Covishield: main safety data ___________________________________ 54
Vaxzevria/Covishield: evaluator’s comments ____________________________ 55
Vaxzevria/Covishield: references __________________________________________ 55
Appendix 1.7 Comirnaty _________________________57
Comirnaty: countries deployed _____________________________________________ 57
Comirnaty: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 58
Comirnaty: data in non-standard schedules ______________________________ 60
Comirnaty: main safety data ________________________________________________ 60
Comirnaty: evaluator’s comments _________________________________________ 61
Comirnaty: references _______________________________________________________ 61
4
Therapeutic Goods Administration
Appendix 1.8 Spikevax __________________________62
Spikevax: countries deployed_______________________________________________ 62
Spikevax: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 62
Spikevax: main safety data __________________________________________________ 63
Spikevax: evaluator’s comments ___________________________________________ 64
Spikevax: references _________________________________________________________ 64
Appendix 1.9 COVID-19 Vaccine Janssen __________66
Janssen: countries deployed ________________________________________________ 66
Janssen: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 66
Janssen: data in non-standard schedules _________________________________ 66
Janssen: main safety data ____________________________________________________ 66
Janssen: additional information ____________________________________________ 67
Janssen: evaluator’s comments _____________________________________________ 67
Janssen: references ___________________________________________________________ 67
Appendix 1.10 Sputnik Light _____________________68
Sputnik Light: countries deployed _________________________________________ 68
Sputnik Light: main clinical efficacy and effectiveness data using standard
schedules ______________________________________________________________________ 69
Sputnik Light: main safety data _____________________________________________ 70
Sputnik Light: additional information _____________________________________ 70
Sputnik Light: evaluator’s comments ______________________________________ 70
References ____________________________________70
5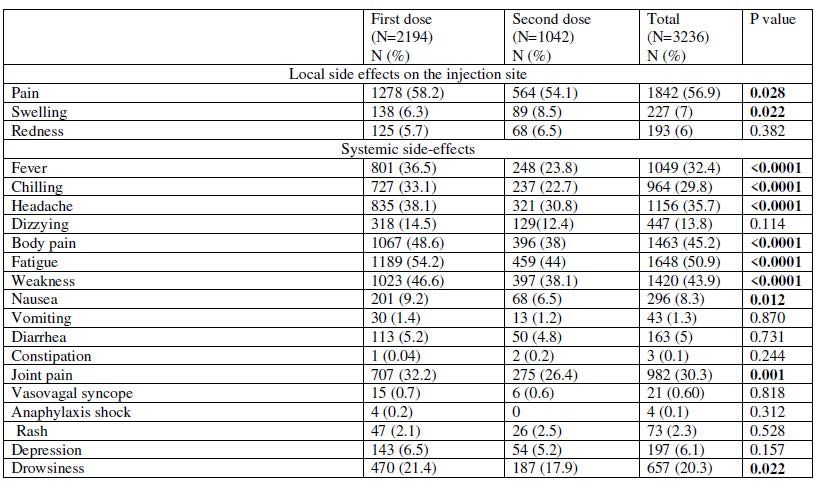
Therapeutic Goods Administration
Executive summary
This document provides an updated assessment by the Therapeutic Goods Administration
(TGA) of the protection offered by certain COVID-19 vaccines that are administered
internationally but are not currently registered in Australia. The advice is based on an
assessment of published data and, in some cases, regulatory information provided
in-confidence. This advice is subject to change as new information becomes available.
The information within this document has been prepared to serve as advice
only, it has no standing in law and does not represent assessment for
regulatory approval in Australia. However, this information will help inform
decisions made elsewhere in Government in relation to incoming travel across
Australia’s international borders in the coming months. It will be updated
regularly as new evidence on the effectiveness of globally used vaccines
emerges, and as assessments are completed by international regulatory bodies.
Note that while certain vaccines may be considered by the TGA as ‘recognised’,
decisions on inbound travel are made by the Department of Home Affairs. In
addition, State and Territory governments, or organisations such as
universities, may apply additional post-border considerations around vaccine
requirements.
This advice has been prepared by comparing the data available for selected vaccines with data
on efficacy and the protection offered by the vaccines that have been approved for use in
Australia. While this assessment is based on data for two-dose schedules of the vaccines not
registered in Australia, public health officials may wish to consider whether a post-arrival
booster dose of another vaccine should be considered.
• People’s Republic of China: Coronavac (Sinovac), BBIBP-CorV (Sinopharm), and Convidecia
(Cansino).
• India: Covishield (AstraZeneca-Serum Institute of India) and Covaxin (Bharat Biotech)
• Russian Federation: Sputnik V (Gamaleya Research Institute)
Effective 1 October 2021, Coronavac (Sinovac) and Covishield (AstraZeneca-Serum Institute of
India) were ‘recognised’ for the purposes of travel into Australia. In November 2021, the TGA
updated this advice to include the ‘recognition’ of BBIBP-CorV (Sinopharm) and Covaxin
(Bharat Biotech).
This January 2022 Update involves the ‘recognition’ of one further vaccine that has been
considered by TGA:
• Sputnik V
6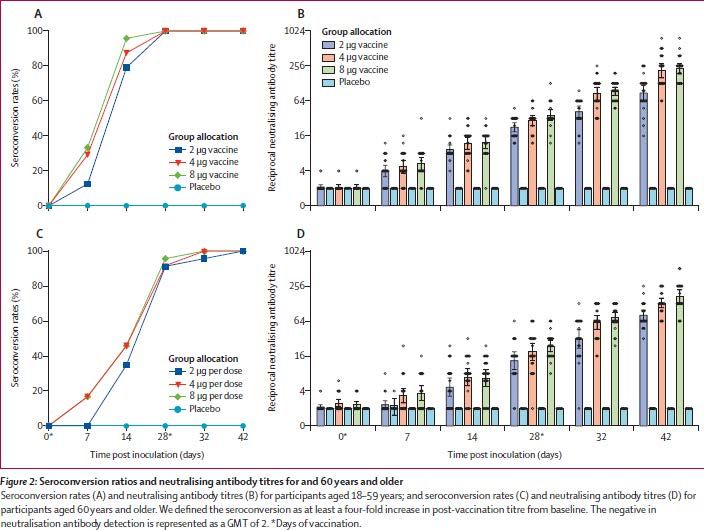
Therapeutic Goods Administration
Potential use of this information
Identifying incoming travellers as being fully vaccinated against COVID-19 (or, alternatively, not
fully vaccinated) helps to achieve two main outcomes. Effective vaccination reduces the
probability that an incoming traveller would:
1. transmit COVID-19 infections to others while in Australia
2. become acutely unwell due to COVID-19, potentially requiring acute healthcare services
Recommendations regarding TGA-registered vaccines
Four COVID-19 vaccines have been granted provisional approval in Australia from the following
sponsors:
1. Pfizer Australia Pty Ltd (Comirnaty)
2. AstraZeneca Pty Ltd (Vaxzevria)
3. Janssen-Cilag Pty Ltd (COVID-19 Vaccine Janssen)
4. Moderna Australia Pty Ltd (Spikevax)
The TGA and the Australian Technical Advisory Group on Immunisation (ATAGI) consider
people to be fully vaccinated if:
a. they have completed a two dose schedule of Comirnaty, Vaxzevria or Spikevax with the
two doses at least 14 days apart, or received a single dose of COVID-19 Vaccine Janssen
and
b. at least 7 days have elapsed since completing their vaccination schedule.
All TGA-approved vaccines are recognised for incoming international
travellers.
How the estimates were determined
The protection offered by a vaccine against a person requiring hospital care if they develop
COVID-19 is either directly measured in Vaccine Efficacy and Effectiveness (VE) data from
clinical trials, or inferred from protection against ‘severe’ infection. VE measures the reduction
in the odds of a person developing infection or hospitalisation, after vaccination, compared to
unvaccinated people with the same exposure to COVID. Vaccine Efficacy trials are designed to
directly measure the protection a vaccine offers against a person becoming infected with
COVID-19 when exposed to the virus. This can be used as an imperfect surrogate for reducing
the chance of transmitting COVID-19, because a person must first be infected with COVID-19 to
transmit it. There are also challenges in making accurate comparisons between the effectiveness
of vaccines, given the inconsistent effectiveness measures, study confounders and efficacy
endpoints used in clinical trials.
7
Therapeutic Goods Administration
Vaccines approved in Australia
Effectiveness information has been assessed for the four vaccines that are TGA-approved for use
in Australia (registered vaccines) for the sake of completeness and to provide comparative data.
All TGA approved vaccines are recognised for incoming travellers.
Vaccine Outcome prevented Average Vaccine Efficacy
Vaxzevria (AstraZeneca) Symptomatic infection 65%
Severe 85%
infection/hospitalisation
Comirnaty (Pfizer) Symptomatic infection 81%
Severe 88%
infection/hospitalisation
Spikevax (Moderna) Symptomatic infection 86%
Severe 81%
infection/hospitalisation
COVID-19 Vaccine Janssen Symptomatic infection 66%
(Janssen-Cilag)
Severe 85%
infection/hospitalisation
Table 1. Vaccine Efficacy of TGA-registered vaccines, adapted from National Centre
Immunisation Research and Surveillance update to ATAGI on 13 September 2021
Of the four vaccines currently granted provisional regulatory approval in Australia, the minimal
average vaccine effectiveness (VE) from two doses of Vaxzevria (AstraZeneca) has been used as
the minimal effectiveness comparator based on published results for Vaxzevria.
The average VE against symptomatic infection is 65% and severe infection and/or
hospitalisation is 85%.
8
Therapeutic Goods Administration
TGA’s updated recommendations on the
recognition of vaccines not registered in
Australia
Coronavac (Sinovac) showed an average VE against symptomatic infection of 64% and an
average VE against hospitalisation of 90%.
• VE against symptomatic infection (surrogate for transmission) of 54%, 54%, 64%, 66% and
84% in five studies.
• VE against severe infection/hospitalisation of 100%, 100%, 88% and 73% in four trials.
The standard schedule of Coronavac is two doses administered 14-28 days apart.
Based on regulatory, published and pre-print data this suggests the efficacy of Coronavac is
comparable to the Australian-approved vaccines, although marginally lower in protection
against symptomatic infection.
The TGA considers Coronovac (Sinovac) vaccine to be a ‘recognised’ vaccine.
BBIBP-CorV (Sinopharm) showed an average VE against symptomatic infection of 65%. VE
against hospitalisation has not been estimated.
• VE against symptomatic infection (surrogate for transmission) of 50% and 79% from two
studies.
• VE against severe infection/hospitalisation of 79% in people under 60 years of age based on
information provided in confidence to TGA.
Based on published and pre-print data this suggests that the average efficacy of BBIBP-CorV
against symptomatic infection is marginally lower than Australian-approved vaccines and the
VE effectiveness against severe infection/hospitalisation is 6% lower than Australian-approved
vaccines.
The TGA considers BBIBP-CorV (Sinopharm) to be a ‘recognised’ vaccine for people
59 years of age and under (inclusive) at the time of entry into Australia. In this case,
the TGA has recognised a slightly lower vaccine effectiveness against severe
infection/hospitalisation than Australian-appproved vaccines due to the lower
absolute risk of severe disease/hospitalisation in younger people contracting
COVID-19 compared to older cohorts.
Covishield (AstraZeneca/Serum Institute of India) is manufactured using the same
ChAdOx1-S recombinant virus as the AstraZeneca (Vaxzevria) vaccine to produce the same dose
of virus in the final product. The two are considered interchangeable by the World Health
Organisation. The TGA considers Covishield to have the same clinical efficacy as Vaxzevria for
this assessment. Two major global regulators, the UK Medicines and Health products Regulatory
Agency and Health Canada have provided regulatory approvals for the AstraZeneca vaccine
manufactured by the Serum Institute of India. These regulators are viewed as ‘Comparable
Overseas Regulators’ by the TGA.
Therefore, the clinical efficacy and effectiveness data for Vaxzevria (AstraZeneca) are relevant
in this case. The average VE against symptomatic infection is 65% and severe infection and/or
hospitalisation is 85%.
9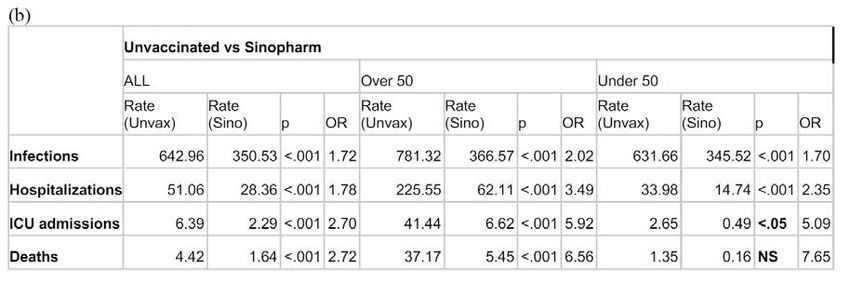
Therapeutic Goods Administration
The TGA considers Covishield (AstraZeneca- Serum Institute of India) vaccine to be a
‘recognised’ vaccine.
Covaxin (Bharat Biotech) showed an average VE against symptomatic infection of 78% and an
average VE against hospitalisation of 94%.
• VE against symptomatic infection (surrogate for transmission) of 78% in one study.
• VE against hospitalisation of 91% in two studies.
The standard schedule of Covaxin is two doses administered 28 days apart.
Based on additional information (provided in confidence) supporting the efficacy and
effectiveness of Covaxin (Bharat Biotech), the TGA considers it to be a ‘recognised’
vaccine.
Sputnik V (Gamaleya Institute) showed an average VE against symptomatic infection of 89%
and VE against hospitalisation of 100%.
• VE against symptomatic infection (surrogate for transmission) of 92% and 86% from two
studies.
• VE against hospitalisation of 100% from one study.
Based on published studies the vaccine efficacy of Sputnik V meets current criteria for efficacy.
The TGA considers Sputnik V to be a ‘recognised’ vaccine.
For Convidecia (Cansino), there is currently insufficient published data on which to base an
assessment of the efficacy of Convidecia and the TGA has not yet been provided with a
regulatory dossier.
As there is insufficient data to evaluate the efficacy Convidecia (Cansino) vaccine
against all of the criteria, the vaccine is not ‘recognised’ by the TGA.
For the unregistered vaccines that are ‘recognised’, effective vaccination would be considered to
extend from 7 days after the last dose of the schedule (which is currently two doses for all
TGA-registered vaccines except for Janssen), or a booster dose after the last dose of the
schedule. This is based on generalising the data from duration of immunity studies reviewed in
the absence of specific studies in the unregistered vaccines.
10Therapeutic Goods Administration
Assessment of vaccination status in schedules
containing vaccines not registered in Australia
The use of TGA-registered vaccines in Australia to complete vaccine schedules commenced with
vaccines not registered in Australia should follow the advice of the Australian Technical
Advisory Group on Immunisation (ATAGI).
ATAGI has considered several issues arising from the ‘recognition’ of vaccines not currently
registered in Australia including:
• The appropriate advice for people who have received vaccines that are not ‘recognised’
(either because TGA has not Recognised them or they are not registered in Australia) and
wish to become fully vaccinated to undertake activity in Australia.
• The status of mixed-product schedules where both products are ‘recognised’ vaccines
(e.g. Sinovac/Comirnaty).
The determination of the vaccination status of a person who has received a ‘recognised’ vaccine
(e.g. fully vaccinated, partially vaccinated, requiring a booster etc) will follow ATAGI’s advice on
these matters.
Omicron COVID-19 variant of concern
The TGA notes that the emergence of the Omicron Strain of COVID-19 (B.1.1.529) in November
2021 has posed challenges for the assessment of the efficacy of vaccines, as clinical trials may
have been conducted on other COVID-19 variants. It is likely that extended schedules
(i.e. ‘boosters’) will be required in some populations to provide additional protection.
The use of 2-dose primary schedules for vaccines not registered in Australia should be
considered in conjunction with ATAGI recommendations for third or further doses of
appropriate products (e.g. mRNA vaccines), and its advice regarding the definition of ‘fully
vaccinated’.
11Therapeutic Goods Administration
Appendix 1.1 Coronavac
Product Coronavac
Product Developer Sinovac
Country of origin China
Vaccine Type Inactivated virus/alum adjuvanted
SARS-CoV-2-HBO2 strain
Schedule 2 doses, 14-28 days apart
Coronovac: countries deployed
Deployed in 40 countries and listed by the WHO for emergency use.
Albania Argentina Armenia Azerbaijan Bangladesh
Benin Brazil Cambodia Chile China
Colombia Dominican Ecuador Egypt El Salvador
Republic
Georgia Hong Kong Indonesia Kazakhstan Lao Peoples Democratic
Republic
Malaysia Mexico Nepal Oman Pakistan
Panama Paraguay Philippines South Sri Lanka
Africa
Tajikistan Thailand Timor- Togo Tunisia
Leste
Turkey Ukraine Tanzania Uruguay Zimbabwe
12Therapeutic Goods Administration
Coronovac: main clinical efficacy and effectiveness data using standard schedules
Study Populatio Strain Schedul Primary VE VE VE VE Advantages Disadvantages
n e Endpoint
AS Sy Hos Deat
y h
• Randomise • Young population 60 years of
et al. 2020) exposed g antibodies day 0 PCR confirmed %
• Included age
HCW in to B1.1.128 and day COVID at least
PREPRINT cohort>60 • Gamma strain
two aged and P2 14-28 14 days after
years • Not peer reviewed (pre-
cohorts, (Gamma) second dose.
• Examines print)
18-59 and tested
HCW at
60+ years
relatively
of age with
high risk
CORONA0 COVID Not noted 2 doses PCR confirmed 64.3
6 exposed COVID at least %
HCW aged Day 0 14 days after
(Dossier) second dose.
13Therapeutic Goods Administration
18-59 in Day 14
Indonesia
• Large real- • Observational, non-
(Alencar et 313228 Gamma 2 doses. Death 99.1
world study randomised
al. 2021) recipients Interval %
• Examines • Only assessed Death as
of COVID not
people >75 an endpoint
vaccines specified.
years of age • Gamma strain
>75 years
of age in
Brazilian
vaccination
program
• Large real- • Observational, non-
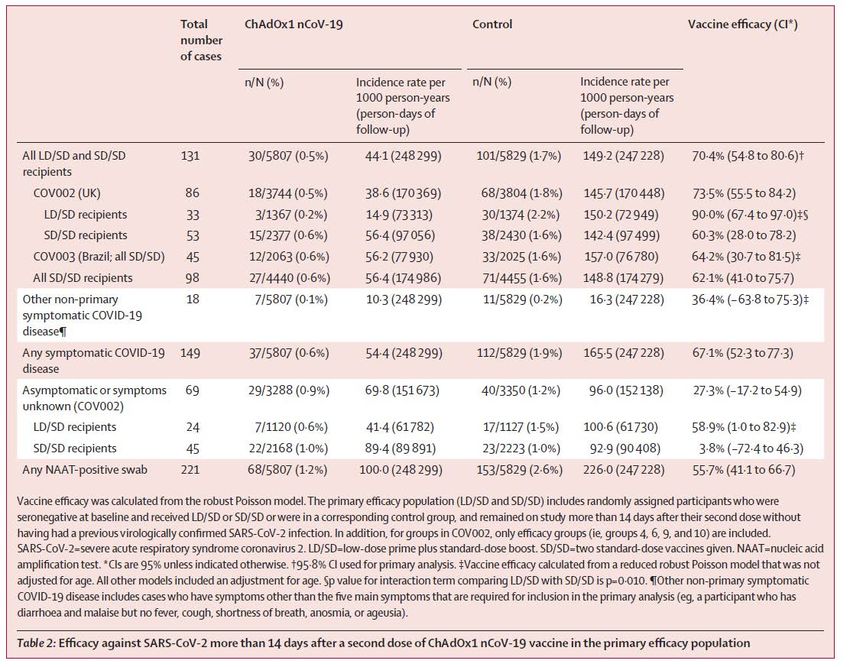
(Jara et al. 10187720 Alpha and 2 doses. Symptomatic 65.9 87.5% (all) 86.3
world study randomised
2021) recipients Gamma Day 0 COVID, % %
90.3% • Examines • Reports VE against ICU as
of COVID and 28 Hospitalisation
(ICU) all age a subset (90.3%)
vaccines days. , ICU admission
groups >16 • Alpha and Gamma strain
>16 years and Death in
years
of age in people >14
Chilean days post
vaccination second dose
program.
• Large real- • Not peer reviewed (Pre-
(Cerqueira 21933237 Alpha and 2 doses Symptomatic 54.2 72.6% (all) 74%
world study print)
-Silva et al. recipients Gamma at 0 and COVID, %
74.2%(ICU • Examines • Alpha and Gamma Strain
2021) of 28 days Hospitalisation
) all age • May have
Coronavac , ICU admission
PREPRINT groups >18 overestimated
>18 years and death
years protection against
of age in
• Prospective hospitalisation/IC
Brazilian
cohort U due to capacity
vaccination
study constraints in-
program country.
14Therapeutic Goods Administration
Coronovac: data in non-standard schedules
(Li et al. 2021) is a preprint study examining the use of a third booster dose in older people
receiving Sinovac. It examined 303 patients over 60 years of age recruited from a phase I/II trial
in whom neutralising antibody levels were recorded at 6 months. Neutralising antibodies had
fallen to below cut-off in 70% of recipients by 6 months after the primary course of vaccination.
A third booster was given at 8 months after the primary vaccination course. This led to a 7-fold
increase in neutralising antibodies compared to 28 days after the second dose. The duration of
this response is not noted.
(Pan et al. 2021) is a pre-print of a placebo controlled, double blinded phase II study in 18-59
year olds who were assigned to receive a third dose either 28 days or 6 months after completing
a primary vaccination schedule in which doses were at 0 and 14, or 0 and 28 days. Only a
portion of subjects in each schedule were randomised to receive the presentation of Sinovac
marketed. Overall, 540 subjects received a third dose. Subjects who received the third dose
recorded an increase of 3-5 fold in neutralising antibody titres compared to 28 days following
their second dose.
Coronovac: main safety data
TGA has reviewed the first Periodic Safety Update Report (PSUR) for Coronavac, covering the
reporting period between 5 Feb 2021 and 14 March 2021. The estimated exposure to vaccine
covered in this report is 17.91 million people in China and an estimated 71.06 million people
worldwide. No safety related action by regulatory agencies was reported in the PSUR.
The most common Adverse Events among the 1109 cases reported were fever (12.5%), asthenia
(9.85%), dizziness (8.90%), allergic dermatitis (8.34%), nausea (6.50%), headache (4.12%),
myalgia (7.18%). A total of 49 cases of serious adverse events were reported in which
relatedness to vaccination was not ruled out, including 6 cases of anaphylactic shock. A total of 6
deaths occurred among reported Adverse Events, of which 4 were considered unrelated to
vaccination and 2 in which the cause of death was unclear.
15Therapeutic Goods Administration
Palacios et al Palacios et al Tanriovier et al
AE within 28 days or AE within 14 days of AE from day 0 to
2nd dose 1st dose unblinding
Vac Plac Vac Plac Vac Plac
Number 6202 6194 6196 6200 6646 3568
Local pain 3742 2014 2750 1387 157 40
Local swelling 359 130 162 72 4 4
Local pruritis 263 181 147 126 2 2
Local redness 241 89 95 48 12 4
Local paraesthesia N.A. N.A. N.A. N.A. 9 5
Local induration 235 67 88 34 3 2
Headache 2128 2157 1944 1996 393 212
Fatigue 989 922 860 798 546 248
Myalgia 727 648 604 545 315 106
Nausea 490 522 423 445 46 7
Diarrhoea 492 501 451 454 106 59
Arthralgia 353 321 293 276 47 18
Cough 343 322 337 318 50 24
Chills 309 313 252 266 164 63
Pruritis 263 225 213 194 3 0
Decreased appetite 217 243 188 213 1 2
Vomiting 61 61 47 49 17 8
Hypersensitivity 58 58 47 44 5 1
Rash 49 42 36 30 7 6
Fever 9 4 7 8 120 52
Table 2. Consolidated rates of elicited adverse events from Tanrovier et al. and Palacios
et al.
Tanrovier et al.and Palacios et al. examined the rates of a set of elicited adverse reactions and
provide placebo controlled rates of these, as shown in the table above.
Coronovac: evaluator’s comments
(Tanriover et al. 2021) was an interim analysis that examined a cohort of 10 214 (ITT)
participants randomised to vaccination (n=6646) or placebo (n=3568). Included subjects were
initially HCW exposed to COVID patients, and then non-HCW volunteers recruited via a web
system. This study was conducted in Turkey between Sep 2020 and Jan 2021. Symptoms were
measured according to the WHO scale outlined in (Marshall et al. 2020) as >=3. It is noted that
the relatively young subjects (mean age of 45) had a low risk of severe disease or death. The
short follow-up for infection of 43 days may limit validity of more severe disease endpoints.
There were no fatal cases of COVID noted, and hence no estimate of VE against death.
16Therapeutic Goods Administration
(Palacios et al. 2020) examined a cohort of 12396 participants randomised 1:1 to vaccine
(n=6195) or placebo (n=6201). Included subjects were mostly 18-59 years of age, but 5.1%
were >60 years of age. This study was conducted in Brazil between Jul and Dec 2020. Subjects
were followed for the duration of the study to detect COVID cases. The authors postulate that
the relatively low efficacy may indicate the detection of very mild symptoms. Vaccine efficacy
was 83.7% (95%CI 58.0-93.7) against cases scoring >=3 on the WHO scale (Marshall et al. 2020)
and 100% against cases scoring >4 (hospitalised). Vaccine efficacy against the primary endpoint
was 62.3% (95%CI 13.9-83.5) for a small subgroup with dose intervals >21 days.
The Evaluator notes that a review of the regulatory dossier of this trial (COR04) provided a
sensitivity analysis based on the case definition. The pre-specified case definition included
saliva-positive PCR tests, which is a potentially less accurate methodology and PHLN currently
does not generally support its use in Australia 1. The Evaluator has therefore used the results of
a sensitivity analysis which excluded saliva PCR tests in this analysis.
Figure 1. WHO working group symptom scoring system used in (Tanriover et al. 2021)
and (Palacios et al. 2020), from (Marshall et al. 2020)
1file:///U:/WORK/COVID%20papers/Downloaded/phln-guidance-on-laboratory-testing-for-sars-cov-2-
the-virus-that-causes-covid-19.pdf
17Therapeutic Goods Administration
(Alencar et al. 2021) is an observational study in 313,328 elderly recipients of COVID vaccines
in Brazil between Jan and May 2021. The study compares rates of death in vaccinated and
unvaccinated individuals using state death records and immunisation registers. Two doses of
Coronavac were received by 159,970 of the people examined. This indicated an attributable
protection ratio (e.g. Death rate vaccinated/death rate unvaccinated) of between 86.3% in
75-79 year olds and 99.3% in over 90-year olds. This study is subject to the biases found in
observational studies. It does, however, provide evidence to balance the relatively young cohort
in the phase III trials.
Table 3. Summary of efficacy results from (Alencar, Cavalcanti et al. 2021)
While this paper did not directly compare the efficacy of AstraZeneca’s ChAdOx1 based vaccine
with Coronavac, the Evaluator notes that the effect on rates of death were similar.
(Cerqueira-Silva et al. 2021) was a pre-print of large retrospective study of people who received
either AstraZeneca or Coronavac in the Brazilian mass vaccination program between January
and June 2021. It estimated the rates of infection, hospitalisation, and death from administrative
records in the Brazilian public medical system. There would be overlap between the
populations in this study and (Alencar et al. 2021), but since Coronavac was only used in Brazil
from April 2021 this study provides a larger cohort vaccinated with this product. Biasing in the
allocation of people to Coronavac or Vaxzevria was not controlled for, and the cohort receiving
Coronavac was older than that receiving Vaxzevria.
(Jara et al. 2021) is a very large prospective cohort study that included all recipients of
Coronavac >16 years of age in the Chilean mass vaccination program between Feb and May
2021. Cases of COVID were acquired through a national mandatory notification system, and
correlated with administrative data on hospitalisations, deaths etc. Of the 10187720 people
included in the cohort, 5,471,728 were unvaccinated, 542,418 had received one dose of vaccine
and 4,173,574 had received two doses of vaccine at the time of reporting.
18Therapeutic Goods Administration
Table 4. Single and two dose vaccine efficacy data for Coronavac from (Jara et al. 2021)
It was noted by the Authors that ICUs were operating near capacity at the time of the study,
which might have biased estimates of efficacy as people could not be admitted according to
need.
Cor06 was a study reviewed in a submitted regulatory dossier. It was an interim analysis of VE
in health-care workers aged 18-59 years of age in Indonesia. This provides an additional
estimate of vaccine efficacy that is somewhat higher than in the Brazilian and Chilean data.
The Evaluator concludes that there is sufficient evidence of the effectiveness of Coronavac to
support Recognition, although the estimates of VE against infection are wide and the average is
only just 65%. The VE against hospitalisation is measured in multiple studies, with good
evidence from South American studies.
19Therapeutic Goods Administration
Coronovac: references
Alencar, C. H., L. P. G. Cavalcanti, M. M. Almeida, P. P. L. Barbosa, K. K. S. Cavalcante, D. N. Melo, B.
C. F. de Brito Alves, and J. Heukelbach. 2021. 'High Effectiveness of SARS-CoV-2 Vaccines
in Reducing COVID-19-Related Deaths in over 75-Year-Olds, Ceara State, Brazil', Trop
Med Infect Dis, 6.
Cerqueira-Silva, Thiago, Vinicius de Araújo Oliveira, Julia Pescarini, Juracy Bertoldo Júnior, Tales
Mota Machado, Renzo Flores-Ortiz, Gerson Penna, Maria Yury Ichihara, Jacson Venâncio
de Barros, Viviane S. Boaventura, Mauricio L. Barreto, Guilherme Loureiro Werneck, and
Manoel Barral-Netto. 2021. 'The effectiveness of Vaxzevria and CoronaVac vaccines: A
nationwide longitudinal retrospective study of 61 million Brazilians (VigiVac-
COVID19).', PRE.
Jara, A., E. A. Undurraga, C. Gonzalez, F. Paredes, T. Fontecilla, G. Jara, A. Pizarro, J. Acevedo, K.
Leo, F. Leon, C. Sans, P. Leighton, P. Suarez, H. Garcia-Escorza, and R. Araos. 2021.
'Effectiveness of an Inactivated SARS-CoV-2 Vaccine in Chile', N Engl J Med, 385: 875-84.
Li, Minjie, Juan Yang, Lin Wang, Qianhui Wu, Zhiwei Wu, Wen Zheng, Lei Wang, Wanying Lu,
Xiaowei Deng, Cheng Peng, Bihua Han, Yuliang Zhao, Hongjie Yu, and Weidong Yin. 2021.
'A booster dose is immunogenic and will be needed for older adults who have
completed two doses vaccination with CoronaVac: a randomised, double-blind,
placebo-controlled, phase 1/2 clinical trial ', PRE.
Marshall, John C., Srinivas Murthy, Janet Diaz, N. K. Adhikari, Derek C. Angus, Yaseen M. Arabi,
Kenneth Baillie, Michael Bauer, Scott Berry, Bronagh Blackwood, Marc Bonten, Fernando
Bozza, Frank Brunkhorst, Allen Cheng, Mike Clarke, Vu Quoc Dat, Menno de Jong, Justin
Denholm, Lennie Derde, Jake Dunning, Xiaobin Feng, Tom Fletcher, Nadine Foster, Rob
Fowler, Nina Gobat, Charles Gomersall, Anthony Gordon, Thomas Glueck, Michael
Harhay, Carol Hodgson, Peter Horby, YaeJean Kim, Richard Kojan, Bharath Kumar, John
Laffey, Denis Malvey, Ignacio Martin-Loeches, Colin McArthur, Danny McAuley, Stephen
McBride, Shay McGuinness, Laura Merson, Susan Morpeth, Dale Needham, Mihai Netea,
Myoung-Don Oh, Sabai Phyu, Simone Piva, Ruijin Qiu, Halima Salisu-Kabara, Lei Shi,
Naoki Shimizu, Jorge Sinclair, Steven Tong, Alexis Turgeon, Tim Uyeki, Frank van de
Veerdonk, Steve Webb, Paula Williamson, Timo Wolf, and Junhua Zhang. 2020. 'A
minimal common outcome measure set for COVID-19 clinical research', The Lancet
Infectious Diseases, 20: e192-e97.
Palacios, R., E. G. Patino, R. de Oliveira Piorelli, Mtrp Conde, A. P. Batista, G. Zeng, Q. Xin, E. G.
Kallas, J. Flores, C. F. Ockenhouse, and C. Gast. 2020. 'Double-Blind, Randomized,
Placebo-Controlled Phase III Clinical Trial to Evaluate the Efficacy and Safety of treating
Healthcare Professionals with the Adsorbed COVID-19 (Inactivated) Vaccine
Manufactured by Sinovac - PROFISCOV: A structured summary of a study protocol for a
randomised controlled trial', Trials, 21: 853.
Pan, Hongxing, Qianhui Wu, Gang Zeng, Juan Yang, Deyu Jiang, Xiaowei Deng, Kai Chu, Wen
Zheng, Fengcai Zhu, Hongjie Yu, and Weidong Yin. 2021. PRE.
Tanriover, M. D., H. L. Doganay, M. Akova, H. R. Guner, A. Azap, S. Akhan, S. Kose, F. S. Erdinc, E.
H. Akalin, O. F. Tabak, H. Pullukcu, O. Batum, S. Simsek Yavuz, O. Turhan, M. T. Yildirmak,
I. Koksal, Y. Tasova, V. Korten, G. Yilmaz, M. K. Celen, S. Altin, I. Celik, Y. Bayindir, I.
Karaoglan, A. Yilmaz, A. Ozkul, H. Gur, S. Unal, and Group CoronaVac Study. 2021.
'Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac):
interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in
Turkey', Lancet, 398: 213-22.
20Therapeutic Goods Administration
Appendix 1.2 BBIBP-CorV (Sinopharm)
Product BBIBP-CorV (CorV)
Product Developer Sinopharm
Country of origin China
Vaccine Type Inactivated virus/ alum adjuvanted
Schedule Strain SARS-CoV-WIV04
Sinopharm: countries deployed
Sinopharm is deployed in 65 countries and listed by the WHO for emergency use.
Angola Argentina Bahrain Bangladesh Belarus
Belize Bolivia Brazil Brunei Darussalam Cambodia
Cameroon Chad China Comoros Cuba
Equatorial
Egypt Gabon Gambia Georgia
Guinea
Guyana Hungary Indonesia Iran Iraq
Lao People’s Democratic
Jordan Kenya Kyrgyzstan Lebanon
Republic
Malaysia Maldives Mauritania Mauritius Mexico
Mongolia Montenegro Morocco Mozambique Namibia
Nepal Niger Nigeria North Macedonia Pakistan
Papua New
Paraguay Peru Philippines Congo
Guinea
Solomon
Senegal Serbia Seychelles Sierra Leone
Islands
Somalia Sri Lanka Thailand Trinidad and Tobago Tunisia
United Arab
Vanuatu Venezuela Vietnam Zimbabwe
Emirates
21Therapeutic Goods Administration
Sinopharm: main clinical efficacy and effectiveness data using standard schedules
Study Population Strain Schedule Primary Endpoint VE VE VE VE Advantages Disadvantages
ASy Sy Hos Death
• Randomised • Strain prevalent
(Al Kaabi et People >18 Not Two 5µg Laboratory 64% 72.8%
in the trial not
al. 2021) years of age noted dose at day confirmed
noted
without known 0 and 21 symptomatic COVID
• Mainly enrolled
history of from 14 days after
healthy young
COVID, MERS the second dose
men, mean age of
or SARS, or
36.2%.
symptoms at
screening.
(Xia et al. 192 healthy Not Two does Phase I/II safety
2021) people aged 18- relevant on day 0 study with
80 with 2 to 8 µg and day seroconversion
negative 14,21 or endpoints
screening. 28
• Large real- • Lambda and
Silva- 400 000 HCW Lambda Two doses Symptomatic 50.4% 94%
world study in Gamma strain
Valencia, and infection and Death
Interval 400 000 • Only reported VE
Javier et Gamma
unknown people in Peru against
al.2021
• Provides symptomatic
PREPRINT estimate of infection and
protection death in
against death. tabulated results
• Not peer-
reviewed (Pre-
print)
22Therapeutic Goods Administration
• Large
(AlQahtani 569054 people Beta and Two doses Symptomatic 45.5% 44.5% 63% Relatively young
study
et al. 2021) residents of infections, population
Delta (72% • Includes
Bahrain hospitalisations,
over delta
ICU admissions,
50 strain
Deaths
years
old)
• Relatively young
(Al-Hosani 176640 Alpha Two doses Hospitalisation, ICU 79.8% 97.1% Large study
population
2021) residents of and Beta admissions and
• Observational
UAE Death
PREPRINT • Not peer
reviewed
23Therapeutic Goods Administration
Sinopharm: main safety data
(Saeed et al. 2021) was a cross-sectional survey of recipients of BBIBP-CorV in the UAE between
January and April 2021. The survey was voluntary and self-administered, and offered to
potential recipients over 18 years of age who had received 1 or 2 doses of vaccine by email or
social media sites. 1102 survey responses were received, of whom 1080 were included in the
study as being from people 18 years and old. The number of vaccines administered to the
survey population was not reported.
Adverse event reported After 1st dose (rate) After 2nd dose (rate)
Number of participants 1080 1080
Local pain (normal) 456 352
Local pain (severe) 28 88
Tenderness 56 108
Local pruritis 12 12
Local redness 8 16
Headache 104 108
Fatigue 132 176
Lethargy 100 148
Myalgia 68
Nausea 16 12
Diarrhoea 8 8
Cough 12 8
Hypersensitivity 12 0
Fever 12 32
Abdominal pain 20 16
Backpain 44 32
Other 8 8
None 264 152
Table 5. Rate of adverse events reported in survey of recipients, Saeed et al. (PREPRINT)
(Hatmal et al. 2021) was a study that administered a self-administered survey to a randomised
cross section of the adult Jordanian population between 9 and 15 April 2021. Participants were
invited through social media (Whatsapp, Facebook, Instagram) to go to the survey website, and
a total of 2213 participants provided information. The vaccinated population of Jordan was
550,000, who had received Comirnaty (BNT162b2), Vaxzevria (AZ1222) or BBIBP-CorV. The
response rate was not reported.
24Therapeutic Goods Administration
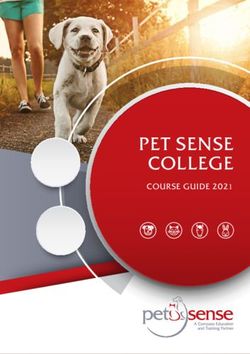
Table 6. Adverse reactions by vaccine type reported in (Hatmal et al. 2021)
25Therapeutic Goods Administration
Figure 2. Adverse event severity by vaccine type from (Hatmal et al. 2021)
The most common adverse events with BBIPB-CorV were fever, tiredness, headache, and
injection site pain. Overall, more BBIBP-CorV recipients reported no adverse events or milder
adverse events than recipients of Comirnaty or Vaxzevria. Other vaccines in this analysis
included small numbers of Covaxin, Sputnik V and other vaccines.
(Cai et al. 2021) is a significant meta-analysis of published studies of several vaccines, including
BBIBP-CorV, which examined reported adverse events. It has referenced the main studies used
in the analyses of efficacy presented in this assessment.
26Therapeutic Goods Administration
Figure 3. Reported adverse events for Comirnaty, Vaxzevria, BBIBP-CorV, Sputnik V and
Spikevax from (Cai et al. 2021)
27Therapeutic Goods Administration
The paper only presents the vaccine sub-analysis graphically, although there is a tabulated
comparison of adverse events by platform (e.g. non-replicating virus vs mRNA) but this merges
several products. Overall the low rate of severe adverse events compared to Comirnaty and
Vaxzevria reported by (Hatmal et al. 2021) using real world data is repeated in this analysis.
The Evaluator notes that there appears to be no data for BBIPB-CorV on the incidence of
myalgia, arthralgia or chills, which may reflect the limitations of published trial data, but these
are reported in the survey based studies.
The WHO (SAGE 2021) has reported two serious adverse events potentially linked to
vaccination with BBIBP-CorV in clinical trial data it has reviewed. These are Inflammatory
Demyelination Syndrome/Disseminated Encephalomyelopathy and Severe Nausea.
Sinopharm: evaluator’s comments
Al Kaabi, Zhang et al. 2021) is an interim analysis of the the main phase III data available for the
Sinopharm/WIV04 vaccine. The study was conducted in 40411 healthy adults in the UAE
between Jul and Dec 2020. Subjects were randomised equally to receive either BBIBP-CorV,
another inactivated vaccine strain (HBO2) or alum adjuvant only, giving 13066 subjects with
two doses of BBIBP-CorV and 13071 with alum only. The study enrolled mainly men (84%) of
young age (mean 36.2 years). The primary endpoint was PCR confirmed symptomatic COVID,
with a vaccine efficacy of 72.8% (95%CI 58.1-82.4). A post-hoc analysis identified an additional
42 asymptomatic cases, which would lower the total vaccine efficacy (symptomatic and
asymptomatic) to 64% (95%CI 48.4-74.7). There were only 2 ‘severe’ cases of COVID and the
Authors note this as a limitation in the study, giving an estimate VE of 100% but with very
broad confidence intervals. The grading scale for symptoms used was not described in the
publication.
WHO’s sage committee provided TGA with a summary of updated data at a median of 112 days
followup. This indicated that there was a VE against hospitalisation of 78.7% (95%CI 26-93.9).
Vaccine Efficacy in people >60 years of age was not estimated.
Table 7. SAGE estimate of vaccine efficacy
The SAGE summary noted that there was a ‘low level of confidence’ that 2 doses of BBIBP-CorV
provides efficacy against infection in older adults.
28Therapeutic Goods Administration
(Xia et al. 2021) was a phase I/II study that mainly examined safety in escalating doses of
BBIBP-CorV, as well as seroconversion. In part 1 of the study, subjects were randomised equally
to receive either placebo or vaccine at 2, 4, or 8 µg doses on day 0 and 28. In part 2 of the study,
subjects were randomised equally to receive placebo of vaccine at 8 µg on days 0 and day 14, 21
or 28. The mean age of participants was 53 years of age. The study was conducted in China in
2020 (exact dates unclear).
Figure 4. Seroconversion following BBIBP-CorV vaccination in phase I/II study
The study indicates that seroconversion occurs in response to vaccination, with uncertain
relevance to clinical outcomes given there is not a clear correlate of immunity for COVID.
(Silva-Valencia) was a large study examining vaccine efficacy and mortality among 400,000
Peruvian healthcare workers between February and Jun 2021. The pre-print of the study was in
Spanish and so the Evaluator cannot comment on methodology, however the table presents
clinical endpoints which translate readily into English. The results of this trial were reported in
English in Reuters, at https://www.reuters.com/world/americas/peru-study-finds-sinopharm-
covid-vaccine-504-effective-against-infections-2021-08-13/.
(AlQahtani et al. 2021) is a study from the deployment of several vaccines, including Sinopharm,
in Bahrain between December 2020 and July 2021. In this, 569,054 individuals with a median
age of 38 years were vaccinated. Delta and Beta strain COVID were isolated from PCR results
during the period of deployment. The paper does not present vaccine effectiveness, which the
Evaluator has calculated from the rates of endpoints presented below. This is notable in that
there is a relatively low level of effectiveness even against Death compared to other trials.
29Therapeutic Goods Administration
Table 8. Pairwise comparisons of effectiveness of Sinopharm BBIBP-CorV in Bahrain
Table 9. Outcomes from Silva-Valencia, J et al. Note the IC 95% is not the CI for the
Vaccine Efficacy
(Al-Hosani 2021) is an observational study based on administrative records from the
deployment of BBIP-CorV in the UAE between September 2020 and May 2021. A total of 214940
cases of COVID were reported to the UAE Dept of Health, of whom 176,640 could be linked to
vaccine status records and were included in the study. The estimate of vaccine effectiveness is
not presented stratified by age.
(Ferenci and Sarkadi 2021) published a review of neutralising antibody levels after two doses of
BBIBP-CorV. This study found that age was a significant factor in the antibody response to
BBIBP-CorV. 25% of recipients at 60 years of age, and 50% of recipients at 80% of age did not
produce protective antibodies.
The Evaluator concludes that there is a wide range of the VE of BBIPV-CorV, but the VE against
infection appears at most 73% and VE against hospitalisation is at most 80%. Partly because of
the demographics of the populations in which the vaccine has been deployed there is a paucity
of VE evidence in people >60 years of age. There is some evidence that immune response in
older people is low. Overall, the Evaluator concludes that there is not sufficient data to conclude
that BBIBP-CorV meets the criteria for Recognition in all age groups.
30Therapeutic Goods Administration
Sinopharm: references
Al-Hosani, F, Stanicole, A et al. 2021. 'Sinopharm’s BBIBP-CorV vaccine effectiveness on
preventing hospital
admission and deaths: results from a retrospective study in the Emirate
of Abu Dhabi, United Arab Emirates (UAE)', PRE.
Al Kaabi, N., Y. Zhang, S. Xia, Y. Yang, M. M. Al Qahtani, N. Abdulrazzaq, M. Al Nusair, M. Hassany,
J. S. Jawad, J. Abdalla, S. E. Hussein, S. K. Al Mazrouei, M. Al Karam, X. Li, X. Yang, W.
Wang, B. Lai, W. Chen, S. Huang, Q. Wang, T. Yang, Y. Liu, R. Ma, Z. M. Hussain, T. Khan, M.
Saifuddin Fasihuddin, W. You, Z. Xie, Y. Zhao, Z. Jiang, G. Zhao, Y. Zhang, S. Mahmoud, I.
ElTantawy, P. Xiao, A. Koshy, W. A. Zaher, H. Wang, K. Duan, A. Pan, and X. Yang. 2021.
'Effect of 2 Inactivated SARS-CoV-2 Vaccines on Symptomatic COVID-19 Infection in
Adults: A Randomized Clinical Trial', JAMA, 326: 35-45.
AlQahtani, Manaf, Sujoy Bhattacharyya, Abdulla Alawadi, Hamad Al Mahmeed, Jaleela Al Sayed,
Jessica Justman, Wafaa M. El-Sadr, Jack Hidary, and Siddhartha Mukherjee. 2021.
Cai, C., Y. Peng, E. Shen, Q. Huang, Y. Chen, P. Liu, C. Guo, Z. Feng, L. Gao, X. Zhang, Y. Gao, Y. Liu, Y.
Han, S. Zeng, and H. Shen. 2021. 'A comprehensive analysis of the efficacy and safety of
COVID-19 vaccines', Mol Ther, 29: 2794-805.
Ferenci, Tamás, and Balázs Sarkadi. 2021.
Hatmal, M. M., M. A. I. Al-Hatamleh, A. N. Olaimat, M. Hatmal, D. M. Alhaj-Qasem, T. M. Olaimat,
and R. Mohamud. 2021. 'Side Effects and Perceptions Following COVID-19 Vaccination in
Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for
Predicting Severity of Side Effects', Vaccines (Basel), 9.
Saeed, Balsam Qubais, Rula Al-Shahrabi, Shaikha Salah Alhaj, Zainab Mansour Alkokhardi, and
Ahmed Omar Adrees. 2021. PRE.
SAGE. 2021. 'Evidence Assessment: Sinopharm/BBIBP COVID-19 Vaccine'.
Silva-Valencia, Javier. '', PRE.
Xia, S., Y. Zhang, Y. Wang, H. Wang, Y. Yang, G. F. Gao, W. Tan, G. Wu, M. Xu, Z. Lou, W. Huang, W.
Xu, B. Huang, H. Wang, W. Wang, W. Zhang, N. Li, Z. Xie, L. Ding, W. You, Y. Zhao, X. Yang,
Y. Liu, Q. Wang, L. Huang, Y. Yang, G. Xu, B. Luo, W. Wang, P. Liu, W. Guo, and X. Yang.
2021. 'Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: a
randomised, double-blind, placebo-controlled, phase 1/2 trial', Lancet Infect Dis, 21: 39-
51.
Appendix 1.3 Covaxin
Product Covaxin
Product developer Bharat Biotech
Country of origin India
Vaccine type Inactivated virus with alum adjuvant
Schedule Strain NIV-2020-770
31Therapeutic Goods Administration
Covaxin: countries deployed
Deployed in 9 countries and was listed by the WHO for emergency use in November 2021.
Guyana India Iran Mauritius Mexico
Nepal Paraguay Philippines Zimbabwe
32Therapeutic Goods Administration
Covaxin: main clinical efficacy and effectiveness data using standard schedules
Study Population Strain Schedule Primary VE VE VE VE Advantages Disadvantages
Endpoint
ASy Sy Hos Death
• Randomised • Not peer
(Ella et al. Adults 18-98 Many, Two doses PCR confirmed 63.6 77.8% 93.4 2
• Includes Delta reviewed (pre-
2021) years including at day 0 symptomatic
(65.2% strain patients print)
Delta and and 28 COVID >14
PREPRINT vs • Estimate of
Kappa days after last
Delta) efficacy in people
dose
>60 years of age
very poor due to
low numbers
(median age 40.1
years)
• Provides estimate
of asymptomatic
infection in
protocol defined
subgroup
• Large cohort Short report does
Indian Adults >18 Not Two doses Hospitalisation 88.2% 96.3%
including not include full
Department years of age noted.
Death middle age population
of Health
Delta and older demographics
prevalent • Delta strain
at the likely to be
time prevalent
2 Based on severe-symptomatic rate
33Therapeutic Goods Administration
Covaxin: main safety data
(Ella et al. 2021) elicited reactogenic adverse events from all 25798 participants in the trial. The
study reported no deaths which were considered related to vaccination, and only 40 serious
adverse events (not otherwise described in the report). The rates of adverse events were higher
for the first than the second dose. The Evaluator notes that the incidence of adverse events was
very low compared to that reported for other inactivated virus vaccines (e.g. Coronavac and
Sinopharm). It is not clear which data set has the more accurate evaluation of the true incidence
of adverse reactions, however.
Figure 5. Rates of adverse events reported in (Ella et al. 2021) for Covaxin after 1 or 2
doses
34Therapeutic Goods Administration
Covaxin: evaluator’s comments
(Ella et al. 2021) was reviewed as a non-peer reviewed pre-print of an interim analysis of an
ongoing phase III trial. The study involved 25 798 volunteers recruited at 25 Indian hospitals
between November 2020 and Jan 2021. Subjects were PCR screened to exclude COVID at
enrolment and before each dose. Subjects were randomised 1:1 to receive vaccine (n=12221) or
placebo (n=12198). Follow-up was stratified into three categories by study site. At Category 1
sites, post-dose phone calls were made every two weeks to detect symptoms (n=16477), at
Category 2 sites swabs were taken every month to detect asymptomatic infection (n=8721) and
at Category 3 sites blood samples were taken for immunological analysis (n=600). Patients were
asked to contact the team on an as-needs basis. The protocol for follow-up and symptom
assessment was not available in the pre-print.
The authors reported 27 variants identified during the study, but did a sub-analysis of 50 Delta-
confirmed participants. This indicated a VE against symptomatic infection of 65.2% (95%CI
33.1-83). This is useful information but the small numbers make the error on this estimate too
broad to be reliable.
Table 10. Efficacy results for (Ella, Reddy et al. 2021)
The Evaluator notes that the median age of the subjects was young (40.1 years) with a relatively
few patients at high risk of illness or hospitalisation due to age. This may explain the
imprecision of the estimate of efficacy in the older age group (>60 years age) which is too
underpowered to be meaningful. Similarly, the imprecision of the estimate on asymptomatic
COVID is too broad to allow clinically meaningful interpretation.
The TGA has reviewed a regulatory dossier that confirms the results presented in (Ella et al.
2021).
The TGA has been provided with an unpublished study of vaccine effectiveness by the Indian
Council of Medial Research of the Indian Ministry of Health. This assessed the effectiveness of
Covaxin against mortality and hospitalisation using linked health data in people eligible for
35Therapeutic Goods Administration
vaccination between April and August 2021. Over this period 1,599,723 individuals received
two doses of Covaxin vaccine. This vaccination program included people >18 years of age and
those over 60 years of age. This indicated a VE of 88.2% (95% 87.9-88.5) against hospitalisation
and 96.3% (95%CI 95.4-96.9) for recipients of two doses of Covaxin.
The Evaluator concludes that there is sufficient evidence to conclude the efficacy of Covaxin
exceeds the threshold required for Recognition, with a fair amount of leeway in these estimates
and in populations exposed to Delta strain COVID.
Covaxin: references
Ella, R., Reddy, S., Blackwelder, W., Potdar, V., Yadav, P., Sarangi, V., Aileni, V. K., Kanungo, S., Rai,
S., Reddy, P., Verma, S., Singh, C., Redkar, S., Mohapatra, S., Pandey, A., Ranganadin, P.,
Gumashta, R., Multani, M., Mohammad, S., Bhatt, P., Kumari, L., Sapkal, G., Gupta, N.,
Abraham, P., Panda, S., Prasad, S., Bhargava, B., Ella, K., & Vadrevu, K. M. 2021. Efficacy,
safety, and lot to lot immunogenicity of an inactivated SARS-CoV-2 vaccine (BBV152): a,
double-blind, randomised, controlled phase 3 trial. PREPRINT.
36Therapeutic Goods Administration
Appendix 1.4 Sputnik V
Product Sputnik V/Gam-COVID-Vac
Product Gamaleya Research Institute
Developer
Country of origin Russia
Vaccine Type Recombinant adenoviruses (rAd26 and rAd5 in heterologous dose
schedule)
Schedule Two doses at day 0 and 21.
Sputnik V: countries deployed
Sputnik V is approved for use in 71 countries and is not WHO listed for emergency use.
Albania Algeria Angola Antigua and Argentina
Barbuda
Armenia Azerbaijan Bahrain Bangladesh Belarus
Bolivia Brazil Cameroon Chile Djibouti
Ecuador Egypt Gabon Guatemala Guinea
Guyana Honduras India Indonesia Iran
Iraq Jordan Kazakhstan Kenya Kyrgyzstan
Lao People’s Lebanon Libya Maldives Mali
Democratic
Republic
Mauritius Mexico Mongolia Montenegro Morocco
Myanmar Namibia Nepal Nicaragua Nigeria
North Macedonia Oman Pakistan Panama Paraguay
Philippines Republic of Congo Russian St Vincent and the
Moldova Federation Grenadines
San Marino Serbia Seychelles Sri Lanka Syrian Arab
Republic
37Therapeutic Goods Administration
Tunisia Turkey Turkmenistan United Arab Uzbekistan
Emirates
Venezuela Vietnam West Bank Zimbabwe
38Therapeutic Goods Administration
Sputnik V: main clinical efficacy and effectiveness data using standard schedules
Study Population Strain Schedule Primary VE VE VE VE Advantages Disadvantages
Endpoint
ASy Sy Hos Death
• Randomised • No estimate of VE
(Logunov, People >18 Not noted Two doses PCR confirmed 91.6% 100%
• Peer reviewed against
Dolzhikova years of age but VOC 21 days symptomatic
asymptomatic
et al. 2021 with not apart COVID
transmission
negative prevalent (rAd26 infection after
• No direct estimate
COVID PCR, in Russia then rAd5) second dose.
of VE against
IgG and IgM during
hospitalisation
on screening. period of
• Relatively few
the trial
patients >60 years
(median age 45.3
years)
• Relatively short
period of follow-
up (48 days) in
interim analysis of
180-day trial
• Large real • Alpha strain
(Voko et 3740066 Alpha 2 doses Infection 85.7% 97.5%
world study
al. 2021)) residents of
Mortality • Peer
Hungary 16+
Reviewed
years of age
• Includes
vaccinated
broad
between Jan
population
and Jun 2021
recruitment
• Large real • Single dose
(González 415995 Not noted First dose Infection, 78.6% 87.6% 84.4%
world study only
et al. residents of Hospitalisation
• Includes
2021) Argentina and Mortality
hospitalisation
aged 60-79
data
39You can also read