COVID-19 HAZARDS AMONG CALIFORNIA FAST-FOOD WORKERS - Physicians for Social ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

COVID-19 HAZARDS
AMONG CALIFORNIA
FAST-FOOD WORKERS
Rajiv Bhatia, MD, MPH, Veterans Affairs Physician & Clinical Professor (Affiliated),
Stanford University School of Medicine
Martha Dina Argüello, Executive Director, Physicians for Social Responsibility —
Los Angeles Physicians for Social Responsibility: Fast-Food COVID-19 Report 1
April 19, 2021
ABSTRACT
At the beginning of the COVID-19 pandemic, government officials designated certain classes
of work to be “essential” – that is, critical to social functioning. However, doing so created
a new class of occupational hazard that was particularly perilous for workers lacking access
to customary health and safety protections. Frontline workers, who are more likely to hail
from the demographic sectors bearing the brunt of the COVID-19 pandemic, have faced close,
frequent and/or prolonged indoor contact with others – the precise risk factor for COVID-19
infection motivating lockdown orders. Sadly, throughout the entire pandemic, essential work
continued without the necessary assurances of public health safety. In an industry like fast
food, a low-wage industry plagued with a history of labor abuses and longstanding structural
barriers to equity, self-interested managerial behavior and inadequate regulatory oversight
compounded these risks. In this study, observations of workplace conditions and COVID-19
infection by workers suggest that workplace transmission among fast-food restaurant workers
has been a potentially significant, ongoing contributor to the COVID-19 pandemic as well as
to disparities in COVID-19 disease burdens. Over a five-month period in mid-2020, 69 workers
at 35 fast-food establishments in seven California counties filed 55 complaints with local
public health and occupational safety agencies citing hazards pertaining to occupational
transmission of COVID-19. In the absence of systematic public health investigations for this
occupational sector, these complaints provide a rare lens for understanding COVID-19 impacts
on workers who lack comprehensive occupational protections. Based on worker observations
reported in the aforementioned complaints, most of the establishments cited (31 of 35;
89%) were noncompliant with five or more of 16 defined elements of public health guidance
for preventing workplace transmission.1 On average, workers reported nine elements of
noncompliance, with reports of 10 or more elements at 18 establishments. Within their
complaints, workers identified 124 confirmed and suspected cases of COVID-19 infection,
suggesting a minimum cumulative workplace attack rate of 8.9% (range 0% to 33%). In 24
of the establishments, workers documented outbreaks of two or more cases within a 21-day
period, suggesting a minimum average secondary infection risk of 17%. In two instances,
clusters of infection involved two or more fast-food establishments related by the same
employees or employees who shared households.
INTRODUCTION
I am writing this complaint because I am living in fear every day that I go to work. I
have a family of five, my three kids and my mother, who is 82 and has health problems.
Already I need to care for her because she cannot walk due to an injury. My kids are
28, 21 and 17. My oldest lost his job recently, so I am the only one providing for all five
of us. If I got COVID, it would be a disaster for my family. It would be hard to keep my
mother from catching it because I care for her so closely and she is very high risk if she
gets it.
— Worker, McDonald’s, Complaint filed with Los Angeles County Public Health
Department, May 26, 2020
2 Physicians for Social Responsibility: Fast-Food COVID-19 ReportGovernmental actions to mitigate the COVID-19 pandemic have involved trade-offs between
preventing infection and maintaining social functioning. The principal strategy of U.S. public
health agencies to control COVID-19 has relied, variously, on discouraging, restricting and
prohibiting opportunities for close contact among individuals who do not share households.
Yet many jobs considered essential require a physical presence at the job site, and a subset of
these involve close, frequent and/or prolonged public or co-worker contact, often in settings
where distancing is not possible.2 By distinguishing essential from nonessential work,
government mitigation policies accepted the fact that individuals working in some industries
and occupations, along with their families and households, would experience higher-than-
average infection and disease risks.3
Despite the evident risks, to date, neither U.S. federal nor state public health agencies have
systematically evaluated the risk of COVID-19 infection or disease across groups of non-
health care essential, frontline workers. More importantly, while public health agencies
have promulgated precautionary guidance for workers and employers, the actual safety of
essential work has never been established scientifically. Differences in occupational risk may
be the primary drivers of observed disparities in rates of infection and mortality both by race/
ethnicity and neighborhood of residence.
Workers in chain fast-food restaurants represent a class with particular vulnerabilities to
workplace COVID-19 transmission. In fast-food settings, employers have optimized work tasks
for efficiency, and work environments provide little opportunity for physical distancing. Low
levels of economic and job security, high frequencies of wage and other labor violations,
and limited control over work tasks and schedules all practically limit the power of workers
to ensure their own safety. A franchise business structure, in which the responsibility for
compliance falls to individual franchisees, limits corporate liability, reducing the likelihood of
cohesive, effective policies for worker protection, as well as the resources for implementing
them. These vulnerabilities persist for workers despite the existence of governmental
regulatory programs that routinely monitor establishments to prevent infectious disease
among restaurant customers.
In this study, we describe workplace hazards for COVID-19 infection at 35 fast-food
establishments in seven California counties, utilizing worker testimony from a convenience
sample of occupational health and safety complaints filed with local health departments and
the California Department of Industrial Relations Division of Occupational Safety and Health
(Cal/OSHA). Based on knowledge of confirmed and suspected cases volunteered by workers,
we estimate the lower-bound (e.g., minimum) cumulative attack rates and secondary infection
risks for workplace transmission. While we recognize potential biases both from the lack of
systematic case ascertainment, which would lead to an underestimation of cases, and from
worker observations, which may mis-identify suspected cases, overall we consider these
estimates to be conservative. In addition, we describe two instances of possible outbreak
chains of transmission involving multiple fast-food establishments.
Physicians for Social Responsibility: Fast-Food COVID-19 Report 3METHODS
Between March and September 2020, Fight for $15, a labor organization for fast-food workers,
aided California fast-food workers in filing 55 unique COVID-19 health and safety complaints
with local departments of public health and Cal/OSHA. Specifically, researchers working
on behalf of Fight for $15 interviewed 69 individuals using semi-structured questionnaires
to assess workplace hazards, then collaborated with these individuals to structure the
information gathered by the interviews into formal complaints and file them. The selection of
individuals interviewed stemmed from accounts of incidents or suspected incidents conveyed
by word of mouth to Fight for $15 organizers, and was not random.
The questionnaires, which were translated for monolingual Spanish speakers, included
questions to assess adherence to safety measures for preventing workplace transmission,
including: the use of and access to personal protective equipment; hand washing; physical
distancing; cleaning and disinfecting; screening employees for COVID-19 symptoms and
sending home workers with COVID-19 symptoms; closing an establishment to clean and
disinfect it; notifying and isolating those who came in close contact with a known or suspected
case; and encouraging sick or exposed workers to stay home, with quarantine pay or paid sick
leave as required. Interviewers focused on the areas of greatest concern to workers and did
not assess all issues in the questionnaire in each interview.
Interviewers also recorded worker-volunteered knowledge of COVID-19 cases at the workplace
and in households. Worker-identified cases included (1) laboratory-confirmed infections of
interviewed individuals or their household members, (2) laboratory-confirmed infections
reported by co-workers and (3) laboratory-confirmed infections reported by management.
Additionally, workers identified suspected cases – where they or a household member had
symptoms consistent with COVID-19 or they or a co-worker observed co-workers on the job
who were visibly sick with symptoms consistent with COVID-19.
While systematic case ascertainment among all workers did not occur, we used available
worker-identified cases to estimate a lower-bound cumulative workplace attack rate as the
average count of confirmed and suspected infections at each store during the study period
divided by an estimated count of employees. We further estimated a lower bound of the
secondary infection risk (SIR) as the average of the sum of secondary cases during a 21-day
period at each establishment with two or more cases divided by the estimated number of
workplace contacts of the primary case.
Estimates of the number of employees in an establishment combined worker estimates
and publicly available information. We estimated the typical employee’s number of usual
workplace contacts based on worker information about tasks and schedules and the physical
layout of establishments. We chose a 21-day (versus 14-day) follow-up period to ascertain
infections in contacts to account for lags in diagnosis and sharing information.
4 Physicians for Social Responsibility: Fast-Food COVID-19 ReportRESULTS
Information collected and recorded in worker-filed complaints indicated frequent
noncompliance with public health guidance to reduce the spread of COVID-19 at most
establishments (Table 1). Based on worker allegations reported in complaints, most
establishments (31 of 35; 89%) were noncompliant with five or more of 16 defined elements of
public health guidance for preventing workplace transmission. On average, workers reported
nine elements of noncompliance, with reports of 10 or more elements at 18 establishments.
Alleged noncompliance related to physical workspaces, essential work tasks and standardized
work practices. Noncompliance also involved the lack of training, resources, oversight and
enforcement in areas of preventive guidance. Worker testimony indicated that compliance
varied within the same establishment as a function of the intensity of work demands.
Table 1. Number and Percentage of establishments with worker-alleged noncompliance with
COVID-19 workplace transmission prevention guidance, by requirement.
Requirement Worker Assessment Select Testimony from Filed Complaints
of Non-Compliance
PPE: Masks and Gloves
Employer does not 54% “In the beginning, managers provided masks made
provide adequate out of doggie diapers or coffee filters. After workers
face coverings for complained, they provided disposable masks but said
employees. we needed to use them for multiple days, until they
stopped working or fell apart.”
Employer does not 60% “Management does not enforce mask wearing by
ensure proper use employees. Approximately half of the co-workers
of face coverings by wear the mask correctly all day. Some people wear it
workers. correctly about half the time, and the rest of the time
they take it off or put in on the chin. Some co-workers
wear the mask when they are talking to customers
but not when they are away from the customers,
even if they are working closely with co-workers.”
Employer does not 40% “I said to my manager, ‘I have a family to protect, I
ensure proper use can’t get sick. I have to do my part.’ And I asked her,
of face coverings by ‘Why do we give the customer service if they don’t
customers. wear a mask?’ And she said, ‘We aren’t going to lose
a customer by making those comments.’”
Employer does not 49% “McDonald’s regularly runs out of the correct types
provide adequate and sizes of gloves. McDonald’s regularly runs out of
gloves for employees. medium and large size gloves, and often McDonald’s
provides the wrong types of gloves and gloves of
very low quality that break easily. If the gloves are too
big, they allow for contamination because they are
loose and slip on and off. Also, if they are too big, you
can burn yourself because it makes it hard to hold on
to the coffee cups. If the gloves are too small, they
tear easily. Sometimes McDonald’s provides the type
of gloves that are very big and loose that slip off your
hands, and we can’t work with them.”
Physicians for Social Responsibility: Fast-Food COVID-19 Report 5Frequent Cleaning of High-Touch Surfaces
Employer does not 83% “The store has not changed its cleaning protocols
ensure frequent since the pandemic began, and there is no system
cleaning (between or training in place for how to clean safely. The
users and shifts) of lunchroom where we eat is small and dirty, they don’t
high-touch surfaces. disinfect it. … They don’t disinfect the area where
we clock in and out either. [The worker], who cleans
the lobby, got her hours reduced and now she only
comes in two or three times per week, so the rest of
the days, the lobby isn’t cleaned. … The bathroom is
cleaned maybe twice a day. Other areas in the store,
such as door handles, are not cleaned regularly.”
Hand Hygiene
Employer does 60% “Many co-workers only wash hands once per day,
not ensure that only briefly and without soap.”
workers wash hands
frequently (every 30
minutes).
Employer does 49% “McDonald’s does not provide masks, we have to
not provide hand bring our own masks. McDonald’s often runs out
sanitizer. of gloves, for example, sometimes there are only
medium-sized gloves, which do not work if you need
small or large. McDonald’s also runs out of sanitizers,
products to clean the grill, cleaning tablets for the
drink machines, disinfectants and hand sanitizer. They
even run out of basic supplies for serving customers,
like fry boxes and cups.”
Physical Distancing
Employer does 91% “In the kitchen where I work, we are usually only
not ensure that about two to three feet apart while we are working.
physical distance is The kitchen is very small. I am a cook and I usually
maintained. work three or four shifts a week. … This means I am
spending many hours each week working very close
to people who do not wear masks properly. … The
break room is very small, and three or four workers
sit right next to each other around a small table
without masks, one or two feet apart, like a normal
day, like how regular work should be without a global
pandemic.”
Prescreening for High Temperature
Employer does not 57% “Also at the June 3 meeting, the managers said
screen all workers that if we are sick we should not come to work. But
for high temperatures the managers DO have people work when they are
before shifts, sick. Around May 5th, a floor manager, took my
excluding those with temperature and it came out high, and she told me,
high temperatures. ‘No way are you going home,’ and then she took it
again and again and it kept coming out high, until the
4th time it came out low, and she told me to go to
work.”
6 Physicians for Social Responsibility: Fast-Food COVID-19 ReportIf Someone Is Sick
Exclusion of Sick Workers
Employer does 71%* “On Monday, May 18, I felt sick at work, I had a
not exclude from headache, my legs and feet ached and I felt very hot.
the workplace I told my manager that I felt sick and I wanted to
workers with high go home, and that wearing the mask made me feel
temperatures and/ worse because it was too hard to breathe. He said,
or obvious COVID-19 ‘There is no one to cover for you, just pull the mask
symptoms. down,’ so I did, and I continued to work sick. The next
day, I only felt a mild headache, so I took Advil and
went back to work.” [This worker was diagnosed with
COVID-19.]
Closing Immediately to Clean and Sanitize
When there is a 86%* “[A co-worker] notified the store on Friday, April
COVID-19 case, 3 that she tested positive. The store did not tell us
employer does that day and we kept working. … Between Saturday,
not close store April 4, and today, April 10, this single Domino’s
immediately for location has had four confirmed positive cases of
cleaning and COVID-19 among us workers, and instead of closing
disinfecting. the store temporarily and allowing exposed workers
to quarantine for 14 days with pay, in keeping with
[the Los Angeles County Department of Public Health]
order from March 25, Domino’s has stayed open
without even providing protective equipment to
workers or disinfecting the store.”
Notification and Quarantining of Close Contacts
When there is a 86%* “[A co-worker] and I worked very closely together
COVID-19 case, at the drive-through, even though we tried to stay
employer does not apart. … Around June 29, the manager, told us there
notify and quarantine was another COVID-19 case, and I believe it was [that
all close contacts. co-worker]. I asked the manager: ‘Was I exposed
to this person? Were my co-workers exposed?’ But
the manager did not answer, she walked away to
attend to someone else. I have never been told by
management that I had close contact with anyone
with COVID-19 exposure. [That co-worker] worked
so closely with us, now everyone is scared, we don’t
know who is next.” [The co-worker was diagnosed
with COVID-19.]
Physicians for Social Responsibility: Fast-Food COVID-19 Report 7Use of Sick Leave and Sick Pay
Employer does not 54% “A co-worker of ours was sick at work on Saturday
provide sick and April 4th. [She] was very sick that day. She had a
quarantine pay per fever, she was coughing, and she had symptoms of
regulations. the flu. Please understand, we do not blame [her]
for coming in sick. Her husband had already been
laid off, her father was sick, she has seven young
children at home and our employer has a history of
not paying sick leave. Since she left sick on 4/4 [she]
has not been paid at all. … The failure to pay sick
leave is contributing to the public health risk at our
McDonald’s so I want to give you another example.
I myself was sick March 8 with sore throat. I would
ordinarily have worked, but the doctor told me stay
home for a week because of the public health threat
of COVID-19. McDonald’s did not pay me when I was
out.”
Employer does 57% “Three people in my house tested positive, but still
not ensure that I went to work one more day because I needed the
workers are aware money and my employer did not ever say we would
of sick leave and get paid leave if we were exposed. Even after I told
sick pay policies, per them I tested positive, they did not offer paid leave.”
regulations.
Retaliation
Employees face 31% “I was very scared, and I didn’t want to take the
retaliation for asking test because I was worried that I would have to
for or using paid sick stop working and that I wouldn’t get paid, and I have
or quarantine leave. to support myself and my family. Management never
told us that we needed to quarantine, or that we
would get paid during quarantine. I was afraid that if
I didn’t go in to work, I would be retaliated against,
and my hours would get cut. That week at work my
stomach hurt and I was very worried that I would get
sick. I went to take the COVID-19 test at 10am on June
2, and then I went to work for my regular shift, from
2pm until 9pm. I found out that I had tested positive
for COVID-19 on June 4.”
Employees face 23% “We urge the Los Angeles Department of Public
retaliation for raising Health to take immediate action to protect workers
safety issues. who speak out about COVID-19 at work from
retaliation. Both of us, along with two other co-
workers, were fired after filing complaints to the Los
Angeles Department of Public Health about COVID-19
cases and safety at the McDonald’s at 1716 Marengo
Street in Los Angeles, and speaking up about
COVID-19 safety at work.”
Source: Complaints filed with public health departments in Alameda, Contra Costa, Los Angeles,
Sacramento, San Bernardino, San Francisco and Santa Clara counties and CalOSHA, April 6, 2020 –
September 23, 2020.
*Of stores where workers identified one or more COVID-19 cases.
8 Physicians for Social Responsibility: Fast-Food COVID-19 ReportIn our sample, workers identified 124 workplace COVID-19 cases (82 laboratory-confirmed
and 42 suspected) at 28 of the 35 establishments with filed complaints; 25.7% (nine of 35)
establishments had one or two COVID-19 cases, 25.7% (nine of 35) had three to five cases
and 28.6% (10 of 35) had six to 12 cases. Assuming a combined workforce of 1,386 (13 to 78
per store), we estimated a lower-bound-period cumulative workplace attack rate at the 35
establishments of 8.9% (range 3% to 33%).
At 22 establishments, workers identified clusters of two or more cases within a consecutive
21-day period (mean 4.2 cases; range 2 to 10). Assuming that the first identified case was
the source of secondary workplace cases, we estimated a lower-bound workplace secondary
infection risk of 17% (range 3% to 42%).
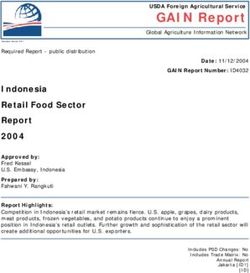
We identified two instances where outbreaks in distinct establishments appear to be related
to a common chain of transmission involving either shared infected workers or workers from
shared households. Many workers noted that they or their co-workers commonly worked part-
time at two or more establishments, were members of households with multiple fast-food
workers and were occasionally reassigned to cover sick workers’ shifts at a franchise’s related
establishments with COVID-19 outbreaks. In one instance, for example, an outbreak at a
McDonald’s franchise at 4514 Telegraph Avenue in Oakland, occurring May 8–27 and involving
10 workplace cases, appeared connected to an outbreak at a McDonald’s at 1998 Shattuck
Avenue in Berkeley involving 12 workplace cases. Three workers who reported testing positive
for COVID-19 worked at both establishments. Additionally, these two outbreaks may have
been related to an outbreak at a McDonald’s at 14480 San Pablo Avenue in San Pablo involving
six workplace cases. One worker from the Telegraph establishment, whose infection status
was unknown, continued to work at the San Pablo McDonald’s during the outbreak period
after the Telegraph McDonald’s was closed.
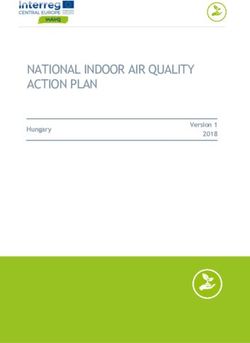
In a second instance, an outbreak at a McDonald’s franchise at 1716 Marengo Street in
Los Angeles involving five workplace cases, occurring June 16–July 4, may have been
associated with workplace COVID-19 exposure at four other franchises that share the same
owner. Several workers at the 1716 Marengo site reported living in households with infected
members who also worked at McDonald’s franchises, albeit different ones. Further, workers
describing the outbreak at 1716 Marengo reported that management moved workers among
establishments to clean and to staff operations during outbreaks.
Physicians for Social Responsibility: Fast-Food COVID-19 Report 9Figure 1. Workplace and household spread of COVID-19 reported by workers: McDonald’s restaurants, Telegraph Ave, Oakland and Shattuck Ave, Berkeley 10 Physicians for Social Responsibility: Fast-Food COVID-19 Report
Figure 2. Workplace and household spread of COVID-19 reported by workers: McDonald’s restaurant on
Marengo Street, Los Angeles
Physicians for Social Responsibility: Fast-Food COVID-19 Report 11DISCUSSION
This report has several important limitations. First, we rely on worker-volunteered information
from a convenience sample of workers publicly filing workplace health and safety complaints.
Workers and their establishments are represented based on their direct and indirect
relationships to labor organizers and their willingness to report their perspectives publicly.
Organizers communicated with additional workers who affirmed COVID-19 safety lapses but
were unwilling to participate in interviews or pursue complaints.
Because interviewers focused their questions on the particular concerns of workers, we
did not assess compliance in all domains of guidance for all establishments. Workers’
assessments of noncompliance reported in complaints, while credible, are unverified. Results
of related government complaint investigations have not yet generally become publicly
available.
In contrast to a more systematic outbreak investigation, assessment of case data from
complaints is insufficient to fully assess COVID-19 infection among all workers in the
establishments. Workers’ knowledge of infections is likely to be incomplete, particularly
with regard to co-workers who did not report symptoms or take absence from work. Only a
minority of the workers at the establishments volunteered information. Alleged management
practices discouraging reporting of COVID-19 symptoms and leave-taking for illness or
quarantine may further contribute to underreporting. We were aware of no establishment
that screened or tested all workers in the course of a worker-identified outbreak. Still, worker-
identified cases are a reasonable basis for lower-bound estimates of infection prevalence and
transmission risk.
Despite the several limitations, this report illustrates that workplace COVID-19 outbreaks
in fast-food restaurants and their extension through workers’ households and secondary
employment settings may be significant contributors to the COVID-19 pandemic. There
are 550,000 fast-food employees in California, representing 38% of the state’s food service
and drinking places sector.4 In Los Angeles County alone, 166,000 employees work at
approximately 7,500 fast-food establishments and serve 2.6 million customers daily.5 In a
vulnerable population where there has been limited regulatory oversight or enforcement, the
methods utilized in this report provide one pathway for assessing hazards during an ongoing
public health crisis.
Many governmental actions aimed to protect workers in essential, frontline roles. The federal
Families First Coronavirus Response Act, which expired on December 31, 2020, required
employers with 50 to 500 employees to offer two weeks of paid sick leave to employees
infected with COVID-19 or requiring quarantine, with similar legislation to cover employers
with more than 500 employees at state and local levels in California. The U.S. Centers for
Disease Control and Prevention, the U.S. Food and Drug Administration and the California
Department of Public Health issued and periodically updated guidance for preventing
COVID-19 in non-health care workplaces and specifically for restaurants.6 In November 2020,
12 Physicians for Social Responsibility: Fast-Food COVID-19 ReportCalifornia’s Department of Industrial Relations issued emergency temporary standards for
COVID-19 prevention in workplaces.7
However, as illustrated by worker testimony, the “real-world” protections offered by
unenforced or unenforceable occupational health and safety guidance may be limited. While
work that provides paid sick leave is associated with taking leave and seeking medical care
when ill, both employee and work characteristics influence access to leave, regardless of legal
mandates. Workers with lower wages, less job security and fewer alternative employment
options face barriers to utilizing leave.8 Similarly, effective occupational safety regulations
require an expectation and culture of valuing workplace safety. Insecure workers may be
reluctant to initiate complaints, and regulatory compliance often follows, rather than prevents,
injury or illness. The efficacy or adequacy of public health guidance is not established.
While many studies have predicted higher infection risks for frontline, essential workers, little
epidemiology has examined occupational data systematically. One large prospective study
conducted in the United Kingdom found that, relative to nonessential workers, essential
workers had significantly higher risks of severe COVID-19 disease.9 Similar studies in the
United States have not been reported. One U.S. study reported excess death during the
COVID-19 pandemic by occupation.10
Undermining the possibility of high-quality occupational epidemiology, U.S. public health
agencies have, thus far, neglected to systematically collect and report the occupation, industry
and workplace data necessary to scientifically monitor and manage occupational COVID-19
risks. Surveillance case reports include data elements for occupation and industry; however,
thus far, only one state, Washington, has published COVID-19 case rates by occupation and
industry, but incomplete collection of occupational data limits the validity of the state’s
estimates.11 Other states have not reported any data on COVID-19 infection or disease by
occupation or industry. Enumeration of workplace infection based on occupational injury
and illness reporting also appears unreliable. According to California’s OSHA data, in Los
Angeles County, only 220 of the more than 1 million confirmed cases of COVID-19 occurred
due to workplace transmission.12 The failure to monitor infection and disease burdens by
occupation and industry creates a blindness to occupationally related health disparities and
their contributions to the COVID-19 pandemic.
Published reports on workplace COVID-19 outbreaks have called attention to wholesale food
processing and other industrial settings. Relative to other essential, frontline work, workplace
transmission hazards for fast-food restaurant establishments appear to have particularly low
visibility.
Because of the demographics of employment in essential, frontline work, workplace outbreaks
have a disproportionate impact on low-income communities of color.13 In the United States,
Hispanic/Latino persons have experienced a disproportionate burden of COVID-19. Nationally,
compared to white non-Hispanics, Hispanic/Latino persons are 1.3 times more likely to have a
confirmed case of COVID-19, 3.2 times more likely to be hospitalized with the disease and 2.3
Physicians for Social Responsibility: Fast-Food COVID-19 Report 13times more likely to die from it.14 In California, Latinos comprise about 40% of the population
but 55% of the COVID-19 cases and 46% of the COVID-19 deaths.15 Some research also looks at
within-household transmission risk for Hispanic/Latino households compared to white non-
Hispanic households (SIR 63% versus 51%).16 Eighty-four percent of Los Angeles fast-food
employees are people of color, and a majority are Latino (Latino 62%, white 16%, Black 4%).17
Hazards during an emerging infectious disease epidemic for fast-food and other essential,
frontline workers call for several actions. First, public health agencies must systematically
collect data on occupation, industry and business location for all essential workers. This
will support timely identification and control of workplace outbreaks.18 Workers in fast-food
settings should be among occupation groups prioritized for enhanced screening and contact
tracing. Public health and occupational safety agencies should use monitoring data to
demonstrate the sufficiency of workplace COVID-19 infection prevention rules under real-world
conditions.
To further transparency, OSHA and its state-level counterparts should report complaints
by workplace in real time, along with, ultimately, findings from investigations and actions.
Corporate parents that franchise chain fast-food restaurants should share liability for
occupational hazards with franchisees. Corporations have the capacity and resources to
develop and oversee standardized systems for worker safety in the same fashion used to
ensure quality and standardized food products.
Public health departments, which have a day-to-day presence in food establishments to
ensure food safety for consumers, should monitor businesses to ensure their operations are
in compliance with workplace safety laws. In California, local agencies have the authority to
revoke and suspend restaurant permits for noncompliance with local, state and federal law.19
Workers must have the tools and capacities to protect their health and realize their rights.
Because many fast-food workers are economically insecure and live with other essential
workers or vulnerable populations, access to medical isolation housing at the onset of
symptoms, along with immediate income support, could enhance compliance with isolation
requirements and limit subsequent workplace and household spread of COVID-19. In the long
term, fundamental changes in the legal responsibility of employers or the culture of low-wage
employment may be required before workers are able to utilize sick leave when sick or speak
up without fear when practices are unsafe.
14 Physicians for Social Responsibility: Fast-Food COVID-19 ReportSUPPLEMENTARY MATERIALS
COVID-19 HEALTH AND SAFETY INTERVIEW QUESTIONS
About You
• Name, address, email (if an email user).
• Where do you work? How long have you worked there? How long have you worked in
fast food? What job do you work? What is your typical shift and schedule? Do you hold
a second job?
• Do you have vulnerable household members? Who depends on your income? Do
household members work with vulnerable populations?
• What are you concerned about?
COVID-19 Prevention Practices
• PPE: Does management provide masks and gloves? Does management enforce proper
mask wearing by workers and customers (drive-through and lobby)?
• Is there frequent (between users and shifts) cleaning of high-touch surfaces (restrooms,
headsets, utensils, knobs, touchscreens, etc.)? Are there adequate cleaning and
sanitizing supplies?
• Hand hygiene: Does management enforce regular, frequent hand washing (every 30
minutes), even when the restaurant is busy? Do workers and customers have access to
hand sanitizer?
• Does management enforce physical distancing, even when the restaurant is busy?
• Is there a COVID-19 safety plan? Have you received training to prevent the spread
of COVID-19 (through hand washing, wearing masks and gloves, distancing and
cleaning)?
• Is there COVID-19 screening (for fever, exposure or symptoms)? Are workers sent home
if they fail the screening?
Cases, Outbreaks, Notification and Quarantine, Close Contacts, Quarantine Pay
• Have there been COVID-19 cases at work? When? Were they confirmed or suspected?
Were there cases among workers’ household members (confirmed or suspected)? How
do you know? What did management say and do in response?
• How many cases were there? What shifts and positions did infected workers hold? Who
worked closely with them recently?
• Does anyone at work have COVID-19 symptoms right now? How do you feel?
• What happens when a worker is sick at work? Can they go home? Are they called back
for their next shift?
• If and when has the store been closed for cleaning and disinfecting?
• Was anyone notified as a close contact and quarantined? Who? How long was the
quarantine? Were workers provided quarantine pay, as required?
Physicians for Social Responsibility: Fast-Food COVID-19 Report 15Sick Pay, Retaliation
• Are workers encouraged to quarantine when sick? Are workers informed of sick pay and
extended sick leave policies?
• Can workers call in sick, take sick days and ask for sick pay without retaliation (threats or actual
cutting of days or hours off shift) and without having to find someone to cover their shifts?
Does the employer pay sick pay properly and in a timely way (including before the COVID-19
pandemic)? Examples?
• Can workers speak up about safety without fear of retaliation? Examples?
Potential for Spread of COVID-19 Among Stores
• Do you or co-workers have second jobs in fast food (who and where)?
• Do your household members work in fast food (who and where)?
• Are workers moved among stores within the franchise group for staffing and cleaning during
outbreaks?
16 Physicians for Social Responsibility: Fast-Food COVID-19 ReportEndnotes
1 See Table 1 for a full list of the 16 elements. Generally, they fall into the following categories: per-
sonal protection equipment, cleaning and hygiene, physical distancing, screening for and response to
COVID-19 infection, sick leave/pay and retaliation.
2 M. G. Baker, T. K. Peckham and N. S. Seixas, “Estimating the Burden of United States Workers Exposed
to Infection or Disease: A Key Factor in Containing Risk of COVID-19 Infection,” PLoS One 15, no. 4 (April
28, 2020): e0232452, doi: 10.1371/journal.pone.0232452; M. G. Baker, “Nonrelocatable Occupations at
Increased Risk During Pandemics: United States, 2018,” American Journal of Public Health 110, no. 8
(August 2020): 1126–32, doi: 10.2105/AJPH.2020.305738.
3 D. Michaels and G. R. Wagner, “Occupational Safety and Health Administration (OSHA) and Worker
Safety During the COVID-19 Pandemic,” JAMA 324, no. 14 (October 13, 2020): 1389–90, doi: 10.1001/
jama.2020.16343.
4 2020 U.S. Industry & Market Report (NAICS 722513): Fast Food Restaurants Industry (Bonita Springs,
FL: Barnes Reports, 2020), 34. “Quarterly Census of Employment and Wages (QCEW) Industry De-
tail,” California Employment Development Department, 2021, https://www.labormarketinfo.edd.ca.gov/
qcew/CEW-Detail_NAICS.asp?MajorIndustryCode=1026&GeoCode=06000000&Year=2020&Own-
Code=50&Qtr=01.
5 C.D. Fryar, J.P. Hughes, K.A. Herrick, N. Ahluwalia, “Fast food consumption among adults in the United
States, 2013–2016,” National Center for Health Statistics Data Brief, no. 322 (2018), https://www.cdc.
gov/nchs/products/databriefs/db322.htm. Safegraph, “The Impact of Coronavirus (COVID-19) on Foot
Traffic,” https://www.safegraph.com/data-examples/covid19-commerce-patterns. U.S. Census Bureau,
“Los Angeles County, California; Santa Clara County, California; Alameda County, California; San Francis-
co city, California; California” (2019 Population Estimates), https://www.census.gov/quickfacts/fact/table/
losangelescountycalifornia,santaclaracountycalifornia,alamedacountycalifornia,sanfranciscocitycalifornia,-
CA/PST045219.
6 “Best practices for retail food stores, restaurants, and food pick-up/delivery services during the
COVID-19 pandemic,” U.S. Food & Drug Administration, April 21, 2020, https://www.fda.gov/food/
food-safety-during-emergencies/best-practices-retail-food-stores-restaurants-and-food-pick-updelivery-
services-during-covid-19. “Considerations for Restaurants and Bars,” U.S. Center for Disease Control,
updated October 29, 2020. https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/busi-
ness-employers/bars-restaurants.html. “COVID-19 Industry Guidance: Restaurants providing takeout,
drive-through, and delivery,” California Department of Public Health, July 29, 2020. https://files.covid19.
ca.gov/pdf/guidance-takeout-restaurants.pdf.
7 “COVID-19 Prevention Emergency Temporary Standards — Fact Sheets, Model Written Program and
Other Resources,” State of California Department of Industrial Relations, 2021, https://www.dir.ca.gov/
dosh/coronavirus/ETS.html.
8 J. D. Roberts, K. L. Dickinson, E. Koebele, L. Neuberger, N. Banacos, D. Blanch-Hartigan, C.
Welton-Mitchell and T. A. Birkland, “Clinicians, Cooks and Cashiers: Examining Health Equity and the
COVID-19 Risks to Essential Workers, Toxicology and Industrial Health 36, no. 9 (September 2020):
689–702, doi: 10.1177/0748233720970439.
9 Miriam Mutambudzi, Claire Niedwiedz, Ewan Beaton Macdonald, Alastair Leyland, Frances Mair, Jana
Anderson, Carlos Celis-Morales, John Cleland, John Forbes, Jason Gill, et al., “Occupation and Risk of
Severe COVID-19: Prospective Cohort Study of 120 075 UK Biobank Participants,” Occupational and Envi-
ronmental Medicine (December 9 2020), doi: 10.1136/oemed-2020-106731.
10 Y. H. Chen, M. Glymour, A. Riley, J. Balmes, K. Duchowny, R. Harrison, E. Matthay and K. Bibbins-Domin-
go, “Excess Mortality Associated With the COVID-19 Pandemic Among Californians 18–65 Years of Age,
by Occupational Sector and Occupation: March Through October 2020,” medRxiv, doi: https://doi.org/10.1
101/2021.01.21.21250266.
11 “COVID-19 Confirmed Cases by Industry Sector,” Washington State Department of Health and Washing-
ton State Department of Labor and Industries, November 10, 2020, https://www.doh.wa.gov/Portals/1/
Documents/1600/coronavirus/IndustrySectorReport.pdf.
12 J. Pole, D. Kassler and P. Reese, “’Major, major problem’: California Failing to Track Workplace COVID
Infections, Deaths,” Sacramento Bee, February 2, 2021, https://www.sacbee.com/news/coronavirus/arti-
cle248847034.html.
13 N. Goldman, A. R. Pebley, K. Lee, T. Andrasfay and B. Pratt, “Racial and Ethnic Differentials in
COVID-19-Related Job Exposures by Occupational Status in the U.S.,” medRxiv, November 16, 2020,
Physicians for Social Responsibility: Fast-Food COVID-19 Report 17doi: 10.1101/2020.11.13.20231431; D. Hawkins, “Differential Occupational Risk for COVID-19 and Other
Infection Exposure According to Race and Ethnicity, American Journal of Industrial Medicine 63, no. 9
(September 2020): 817–20, doi: 10.1002/ajim.23145.
14 “COVID-19 Hospitalization and Death by Race/Ethnicity,” U.S. Centers for Disease Control and Preven-
tion, February 12, 2021, https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/
hospitalization-death-by-race-ethnicity.html.
15 “COVID-19: Cases,” CA.gov, https://public.tableau.com/views/COVID-19CasesDash-
board_15931020425010/Cases?:embed=y&:showVizHome=no.
16 Carlos G. Grijalva, Melissa A. Rolfes, Yuwei Zhu, Huong Q. McLean, Kayla E. Hanson, Edward A. Be-
longia, Natasha B. Halasa, Ahra Kim, Carrie Reed, Alicia M. Fry, et al., “Transmission of SARS-COV-2
Infections in Households — Tennessee and Wisconsin, April–September 2020,” Morbidity and Mortality
Weekly Report 69, no. 44 (November 6, 2020): 1631–34, https://www.cdc.gov/mmwr/volumes/69/wr/
pdfs/mm6944e1-H.pdf.
17 Current Population Survey, Annual Social and Economic (March) Supplement, March 2019.
18 J. Sugerman-Brozan, “Measures to Protect the Health and Safety of Massachusetts Employees Who
Must Work at the Workplace During the SARS-CoV-2 Pandemic,” New Solutions 30, no. 3 (2020): 249–53,
doi: 10.1177/1048291120960229.
19 Rajiv Bhatia, Megan Gaydos and Karen Yu, “Defending and Advancing Labor Standards: Roles for
Public Health,” Public Health Reports 128, no. 6 (supplement 3) (November–December, 2013): 39–
47, doi: 10.1177/00333549131286S307.
18 Physicians for Social Responsibility: Fast-Food COVID-19 ReportAbout the Authors
Rajiv Bhatia, MD, MPH
Dr. Bhatia is a physician practicing internal medicine at the Veterans Affairs Palo Alto Health
Care System and a Clinical Assistant Professor (Affiliated) at the Stanford University School
of Medicine. From 1998 through 2014, he served as Deputy Health Officer for the City of San
Francisco, where he pioneered work on health impact assessment (HIA), community health
indicators, and open civic data. Dr. Bhatia founded the Civic Engine to advise civil society
organizations, businesses, and governments on innovations to address the community and
economic roots of health.
Martha Dina Argüello
Martha Dina Argüello is the Executive Director of Physicians for Social Responsibility – Los
Angeles, joining in 1998 to launched environmental health programs. She is a board member
of Californians for Pesticide Reform, the California Environmental Rights Alliance, and
Californians for a Healthy and Green Economy. She also co-founded the Los Angeles County
Asthma Coalition and the Coalition for Environmental Health and Justice, and was appointed
to Cal/EPA’s Environmental Justice Committee and the California Air Resources Board’s
Global Warming Environmental Justice Advisory Committee.
Physicians for Social Responsibility: Fast-Food COVID-19 Report 19You can also read