CHILDREN AND NON-COMMUNICABLE DISEASE - Global Burden Report 2019 - NCD Child
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CHILDREN AND NON-COMMUNICABLE DISEASE Global Burden Report 2019

Authors:
Leonor Guariguata, MPH
Selvi Jeyaseelan, PhD
Editorial Committee:
Mychelle Farmer, MD, FAAP
Jonathan Klein, MD, MPH, FAAP
Marie Hauerslev, MD
Alafia Samuels, MBBS, MPH, PhD
© 2019, NCD Child
Table of Contents
Executive Summary 3
Introduction 6
Trends in major risk factors 8
How are children vulnerable? 10
The Global Burden 12
Cardiovascular disease 13
Cancer 16
Chronic respiratory disorders 19
Diabetes 22
Mental Health 24
Injuries and Violence 27
Cross-cutting issues 29
The social determinants of health 30
Early life experiences 32
Treatment and care 34
Systems and sustainability 37
Best practice and the future 38
Building for the future 39
Policy Best Buys 41
The work of NCD Child 43
Additional resources 45
NCD Child is a global multi-stakeholder the health of all children, has served as NCD
coalition, championing the rights and needs of Child Secretariat since 2014. NCD Child
children, adolescents, and young people living continues to be a voice for the rights of
with or at risk of developing NCDs. We work children, adolescents, and young people at risk
with health professionals, NGOs, government, of, living with and affected by NCDs through
private donors, and most importantly, young education, raising awareness, and broader
people, to advocate for the rights of children, participation in the global health and
adolescents, and young people and promote development discourse.
policies to minimize preventable death and
disability in young people. The American For additional information on NCD Child,
Academy of Pediatrics (AAP), a US-based please visit www.ncdchild.org, and follow us on
membership organization of 67,000 Twitter at @NCDChild.
pediatricians and pediatric medical sub-
specialists and surgical specialists dedicated to
2
“For goals to be met, it is
crucial that NCD
prevention and risk factor
EXECUTIVE control starts during
SUMMARY childhood.”
Young people under the age of twenty account changes to the environment in which NCDs
for more than one-third of the world’s develop.
population. In 2017, more than 2.1 billion The key drivers of NCDs in children are
children were affected by non-communicable unhealthy diet, obesity, physical inactivity,
diseases (NCDs). NCDs, a set of diseases alcohol and tobacco use. Risk for NCDs can be
resulting from the interaction of a combination established as early as life in the womb. All of
of genetic, physiological, environmental and these risk factors are on the rise. Three in every
behavioral factors, present a significant burden four adolescents are not getting enough
on individuals, communities and economic exercise and 42 million children are considered
resources. Children affected by NCDs often obese. These contribute to increases in the
face a lifelong challenge to manage and treat prevalence of type 2 diabetes in youth, high
their conditions. Much is written about NCDs blood pressure and cholesterol.
and premature mortality, but this definition starts In recognition of this increasing burden,
at 30 years of age. Indeed, children, heads of government and ministers of health
adolescents and young people are increasingly convened in 2011 for the United Nations
affected by NCDs and this population remains General Assembly Special Session (UNGASS)
hidden from global surveillance, targets and for the first ever UN High Level Meeting (HLM)
priorities. on non-communicable diseases (NCDs). They
For many NCDs, the best option for committed to a set of targets for reducing what
reducing the disease burden is prevention. was recognized as the overwhelming and rising
Over two thirds of the antecedents to NCDs burden of NCDs across the globe. Since then,
emerge during childhood and adolescence. leaders in government and health have
Thus, prevention must start with children and in reconvened to monitor progress on these
families, working with communities to make targets and evaluate new issues. The third HLM
Burden of major NCDs in children (
What are NCDs?
on NCDs was held in 2018 and continues the
important work set out to turn the tide on NCDs. Cardiovascular disease (CVD) in
Despite progress made in monitoring and children can be congenital or acquired.
combating the rising trends of NCDs and their Globally, 13.9 million children are
risk factors, many people, including children are
being left behind. Children represent a affected by CVD. Rheumatic heart
vulnerable group in health as they may have disease (RHD) is the most common
limited agency to advocate for their own care, or chronic heart disease in children.
depend on the knowledge and access to care of
a parent or guardian. They are often the most Cancer is a leading cause of death for
vulnerable to complex issues like violence and
children and adolescents worldwide.
injuries, poverty and a lack of education. As
such, systems must be coordinated to ensure Existing data suggests close to 6 million
the health and safety of children. children had cancer in 2017. This may
Many of the risk factors increasing NCDs in be an underestimate as many countries
children are driven by changes brought on by do not have adequate surveillance
economic development. NCDs systems for childhood cancer.
disproportionately affect people in low- and
middle-income countries where more than three
quarters of global NCD deaths. Although Chronic respiratory disorders (CRDs),
significant gains in child survival have been including asthma, respiratory allergies
achieved over the past 25 years, most of these and lung diseases, are a major source of
are the result of focused efforts on reducing disability in children. More than 108
under-5 mortality and especially in infectious million children in 2017 were affected by
disease. Trends in NCD burden are increasing.
These shifts require a more holistic approach CRDs. Children with CRD often
that includes all aspects of health across all experience high rates of hospitalization.
years of life.
In 2018, the World Health Organization Diabetes is a condition where the body
(WHO) set the 5 x 5 framework for tackling cannot adequately manage blood
NCDs including five diseases (cardiovascular glucose or insulin and affects more than
disease, chronic respiratory disease, cancer,
diabetes, and mental and neurological 8.8 million children. Children who do not
conditions) and five key risk factors (unhealthy have access to care and essential
diet, tobacco use, harmful use of alcohol, medicines, especially insulin, may face
physical inactivity, and air pollution). NCDs and serious complications or early death.
their risk factors rarely exist in isolation and
reducing the burden of even one of these
Mental health disorders (MHDs) affect
elements can affect the others. Indeed, NCDs
are themselves a risk factor for developing as many as 231 million children and
mental health disorders, whose complex adolescents are especially vulnerable.
determinants include: exposure to sexual MHDs encompass a wide range of
violence, bullying, experiencing discrimination, conditions from depression and anxiety
living in a conflict or early pregnancy. to psychosis. Mental health can have an
Early prevention of NCDs and their
impact throughout life, especially for
complications should be at the heart of health
policy and management. Effective policies people living with other NCDs.
cannot ignore the importance of the social
determinants of health including gender, Injuries affected about 131 million
socioeconomic status, age and ethnicity. These children in 2017. Injury can be divided
social determinants are can help highlight and into two categories: intentional or
understand inequalities in health. In general,
unintentional. Unintentional injuries
developing countries tend to have a more
limited capacity to respond to the rising NCD account for almost 90% of all injuries
burden, leading to misdiagnosis, a lack of but the Global Burden of Disease study
adequate treatment and thus higher mortality estimates 39 million children died as a
rates. NCDs disproportionately affect people in result of interpersonal violence. Sexual
low- and middle-income countries (LMICs) violence is the most prevalent type of
intentional injury for both boys and girls.
4
where more than three quarters of global NCD
deaths occur. However, inequalities can exist
within countries so that the life of a child and
the likelihood of adequate prevention, treatment
and care for NCDs can depend greatly on their WHO Policy Best Buys for NCDS
socioeconomic status.
The rising trends of NCDs require a child- • Tobacco - Implement the WHO
centered and sustained effort to prevent Framework Convention on
disease and improve the quality of life and Tobacco Control. Ban smoking in
survival of children. This is especially true in public places, schools, and
developing countries where there is a double
burden of infectious diseases and NCDs. hospitals.
Prevention requires a reduction of risk and the • Alcohol - Tax alcoholic beverages.
adoption of a life-course approach, starting in Enforce age limits. Ban promotion
prenatal and neonatal care and continuing
through the development of a child into of alcohol to young people.
adulthood. Policy efforts must be supported by • Unhealthy diet - Reduce salt, fat,
a coherent and coordinated response from and sugar content in foods. Limit
government across sectors including education,
health, finance, labor and employment promotion of unhealhy foods to
strategies. Civil society also has a role to play in children.
the prevention, treatment, and management of
• Physical inactivity - Empower
NCDs, championing the needs of those at risk
and affected by NCDs with strong and schools and communities to
consistent advocacy. promote physical activity in safe
NCDs must have a permanent place on the and convenient spaces.
global agenda for all countries, and children
must be explicitly considered within that • Strengthen health systems -
agenda. To aid this goal the WHO has proposed Integrate NCDs into primary care.
a list of policy “best buys” for NCDs, many of Build capacity for care
which have a direct and important impact on the professionals managing children.
lives of children. Unfortunately, even in
countries where policies for adults are in place, • Essential medicines and care -
children are often left behind. One of the most Ensure equitable, affordable
significant gaps with regard to NCDs and access to essential medicines and
children is a lack of surveillance and monitoring palliative care.
for these age groups. Data on NCD risk factors
and prevalence along with appropriate research • Monitoring and surveillance - As
will enable the development of evidence based with adults, regular data on the
prevention and management strategies that are burden of NCDs and their risk
tailored to children. factors should be routinely
NCD Child advocates for the unique needs
collected for children.
of children, adolescents, and young people
through its collaborations with civil society,
government, youth advocates, and young
people affected by NCDs.
5“Seventy percent of the
preventable adult deaths
from NCDs are linked to risk
factors that start in
adolescence, providing a
key opportunity for INTRODUCTION
prevention.”
Defining children and NCDs linked to risk factors that start in adolescence,
There is no universally agreed age range for providing a key opportunity for prevention.
what constitutes childhood. It is a concept that The five most common NCDs in adults are:
varies considerably across cultures. This report cardiovascular diseases, cancer, chronic
uses the definition of a child specified in the respiratory disorders, mental health disorders,
Convention on the Rights of the Child (Table 1.1: Definitions of child and subcategories
Term Definition
Child Anyone under the age of 18.
Adolescents Children between the ages 10 and 19. Used more for understanding the
biological changes rather than social transitions. Recent literature suggests
extending the upper limit to 24 years.2
Infant and neonate A child younger below one year of age.
Young people Used interchangeably with “youth” the terms often are used for ages 15 to 24.
Although the UN recognize that member states may use different definitions.
Youth Persons between the ages 15 and 24.
for child health and is a major cause of
morbidity. Mental health is a term used to describe a
Cancer is a term used to describe a large group state of well-being that allows a person to
of diseases that involve the growth of abnormal realize their own potential, cope with the normal
cells. These abnormal cells grow beyond their stresses of life, work productively, and
usual boundaries and then invade other parts of participate in the community. Mental health
the body. Cancer can affect almost any part of disorders (MHDs) comprise a broad range of
the body and there are many different types, all problems that affect mental health (including
need specific treatment and management a n x i e t y, d e p r e s s i o n , b i p o l a r d i s e a s e ,
strategies. schizophrenia and other disorders). Symptoms
range from any of or a combination of abnormal
Chronic respiratory disorders (CRDs) are thoughts, emotions, behavior and relationships
chronic conditions affecting lungs, airways and with others.
related structures. CRDs range from rhino-
sinusitis, asthma, and chronic obstructive In addition to these five key NCDs, this report
pulmonary disease (COPD) to lung cancer. covers injuries and violence which also play an
important role in determining the health of
Diabetes (diabetes mellitus) is the result children.
reduced levels of insulin production or
ineffective insulin sensitivity. Increases in blood Injury is defined as “the physical damage that
glucose resulting from problems with insulin can results when a human body is suddenly
damage many of the body's systems. There are subjected to energy in amounts that exceed the
two main forms of diabetes: threshold of physiological tolerance – or else
• Type 1 diabetes occurs when the the result of a lack of one or more vital
pancreas does not produce the elements, such as oxygen.”3 They can be a
hormone insulin. This type develops result of intentional (acts of violence against
most commonly in children and others or oneself) or unintentional road traffic
adolescents. crashes, burns, drowning, falls, and poisonings.
• Type 2 diabetes is caused by the
body not responding properly when
insulin is released from the pancreas.
Type 2 diabetes becoming more
common in children. Unlike type 1
diabetes, many cases of type 2
diabetes may be preventable. Citations
1 UN General Assembly, Convention on the Rights of the Child, 20
Diabetes may also develop during pregnancy in November 1989, United Nations, Treaty Series, vol. 1577, p. 3
a condition known as gestational diabetes. 2 Sawyer, S. M., Azzopardi, P. S., Wickremarathne, D. & Patton, G.
Untreated gestational diabetes puts mothers C. The age of adolescence. Lancet Child Adolesc. Health (2018).
and children at risk for complications and 3 Holder Y, Peden M, Krug E, Lund J, Gururaj G, Kobusingye O.
Injury surveillance guidelines. Geneva: World Health Organization;
developing type 2 diabetes later in life. 2001.
7TRENDS IN MAJOR
RISK FACTORS
A risk factor is any characteristic or exposure of
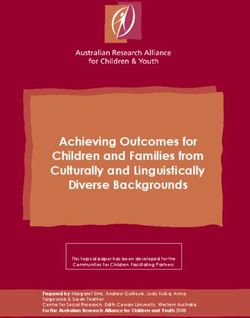
an individual that increases their likelihood of Fig. 1.2. Prevalence (%) of insufficient
developing a disease or injury. These include physical activity (11-17 years), by sex
and income group, 2010
but are not limited to pollution, obesity, unsafe
sex, high blood pressure, poor sanitation, 100 Boys
tobacco and alcohol consumption and others. Girls
Source: WHO, Global Health Observatory
These risk factors often combine to increase the
chances that children to develop certain NCDs. 75
Understanding risk factors is key to the
prevention and control of NCDs. Policies Prevalence (%)
geared towards risk factors can have benefits 50
for the whole population, but understanding
which groups are most at risk can also provide
a targeted approach to prevention. 25
Tobacco use
Globally, an estimated 24 million children aged 0
LIC LMIC UMIC HIC Global
13 to 15 years smoke. Girls smoke at higher
Income Group
rates in high income countries than in middle or
low income countries. Globally, boys smoke at
almost twice the rate of girls (Fig. 1.1). Between
2000 and 2015, the prevalence of tobacco
Fig. 1.1. Prevalence (%) of tobacco use smoking among children decreased in all age
(13-15 years) by income group, 2014 groups and this reduction is expected to
15 continue until 2025. However, not all tobacco
Boys
Girls
use involves smoke, an estimated 13.4 million
Source: WHO, Global Health Observatory
(3.6%) of the world’s population aged 13 to 15
12 years use smokeless tobacco products with
rates almost twice as high in boys than in girls.
Prevalence (%)
9
Physical inactivity
Physical activity is an important protector
6 against a range of NCDs. Worldwide, 3 in 4
adolescents aged 11 to 17 years do not
currently meet the World Health Organization
3 global recommendations for physical activity
(Fig. 1.2). Physical inactivity is higher in girls
0 across all income groups but especially in low-
Global HIC UMIC LMIC LIC
Income Group
Key Messages
• NCDs are driven by several risk factors, but most importantly unhealthy diet and
obesity, physical inactivity, tobacco use and alcohol abuse.
• Both the prevention of risk factor development (primordial prevention) and
modification of risk factors once they are established (primary prevention) are
important.
• Income disparities exist in the distribution of major preventable risk factors.
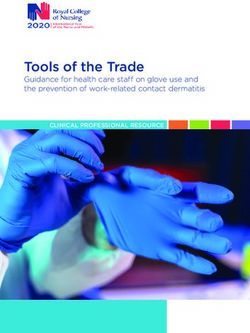
8Fig. 1.3. Trends in prevalence (%) of obesity (5-19 years) by sex
10%
Boys
Girls
7.5%
Prevalence (%)
5%
2.5%
0%
1975 1978 1981 1984 1987 1990 1993 1996 1999 2002 2005 2008 2011 2014
Years Source: WHO, Global Health Observatory
and middle-income countries with the highest age of 19 were overweight or obese (Fig. 1.3).
levels of inactivity seen in low- and upper- The onset of obesity during childhood can lead
middle income countries. Estimates suggest to severe health risks; obesity is a key risk
that physical activity may be in decline in both factor for orthopedic issues, diabetes and
sexes starting from as early as six years old. cardiovascular disease. A population-based
study estimated that 70% of obese children and
Unhealthy diet adolescents between the ages of 5 to 17 have
An unhealthy diet (including insufficient fruit, at least one risk factor for CVD.4
vegetable, legume and nut consumption and/or
consumption of energy dense foods) is one of High blood pressure
the major risk factors for a range of NCDs.1 High blood pressure, or hypertension, is an
Malnutrition in utero and in early childhood have important risk factor for cardiovascular disease
been shown to increase a child’s vulnerability to in both children and adults. Increases in
over-nutrition later in life and into adulthood. childhood blood pressure have been reported
Unhealthy diets are associated with overweight by national surveys in the US and in other
and obesity, which rank globally as the fifth countries.5 These increases were observed in
leading cause of death. Children are especially all ethnicities for diastolic blood pressure and in
high consumers of sugar-sweetened beverages most ethnicities for systolic blood pressure
including sodas, sugary juices, and other drinks (including, boys, girls, and those aged 8 to 12
w h i c h d r i v e u p r a t e s o f o b e s i t y, a n d years).
independently of type 2 diabetes.2 Increases in blood pressure are partially
driven by the rising rates of obesity in children
Alcohol over the last three decades (Figure 1.3).
From conception onwards, the human body is Overweight in adulthood is a known risk factor
susceptible to the harmful effects of alcohol and for cardiovascular disease, but the effect of
use during pregnancy can result in a range of overweight on hypertension in children is less
lifelong conditions. Globally, 155 million 15 to 19 understood.
year olds consume alcohol. Alcohol use in
adolescents is associated with negative effects High levels of fat in blood
on the brain, gut and circulatory system as well Atherosclerosis has been shown to begin as
as increasing sexual risk-taking behavior, early as nine years of age. Amounts of
mental health disorders, and injuries and triglycerides, total cholesterol, low density
violence.3 lipoprotein cholesterol, and high density
lipoprotein cholesterol are all more likely to be
Obesity abnormal in overweight children than in normal
The prevalence of obesity is increasing and in weight children. With treatment, these
2016 an estimated 42 million children under the
9Key Figures: Risk Factors
Prevalence Prevalence
Number Girls (%) Boys (%)
Smoking any tobacco (13-15 years),
24 million 8.3 18.2
2014
Insufficient physical activity (11-17
NA 83.9 77.6
years), 2010
Current alcohol drinking (15-19
155 million 26.5 (total)
years), 2016
Obesity (5-19 years), 2014 42 million 5.6 7.8
Deaths due to air pollution
395 thousand 6.4 5.7
(HOW ARE CHILDREN
VULNERABLE?
Children have made significant gains in health Article 24 of the Convention states that all
over the past 25 years. The rates of under-5 children have the right to “the highest attainable
mortality across the globe have decreased and standard of health and access to facilities for
the gaps between the richest and poorest the treatment of illness and rehabilitation of
countries are closing.1 Most of these gains are health.” Since the adoption of the Convention,
the result of focused efforts on reducing under-5 progress has been made in securing an
mortality through the control of infectious improved prospect for children and their future.
diseases, reducing malnutrition and improving However, more work must be done, and
maternal care. However, trends in NCDs are especially in the poorest countries, to ensure
increasing. that these gains are equally shared and
While stunting and malnutrition rates have accessible to all children.
dropped by 40%, overweight in children has Emergent epidemics of NCDs have yet to
increased by a third since 1990.1 These shifting be explicitly named and, in practice, healthcare
trends require a shifting resources are often
response away from a geared towards other
focus on just the first priorities, especially in
five years of life toward “Shifting trends require … a developing countries.
a more holistic
approach that includes response away from a focus This gap is contrary to
rising trends discussed
all aspects of health. on just the first five years of in this report and the
In 1990, the United high burden of some
Nations and 194 life toward a more holistic NCDs in the world.
countries ratified the approach.…” Children represent
Convention on the a vulnerable group in
Rights of the Child, health as they may
enshrining the principle have a decreased ability
that children hold fundamental economic, to advocate for their own care, or depend on
social, cultural, civil and political rights in which the knowledge and access to care of a parent
they play a critical role as holders of those or guardian. They are often the most vulnerable
rights. It asserts that all children – without to complex issues like violence and injuries,
discrimination in any form – benefit from special poverty, and a lack of education. As such,
protection measures and assistance; have systems must be coordinated and implemented
access to services such as education and to ensure the health and safety of children.
health care; can develop their personalities,
abilities and talents to the fullest potential; grow
up in an environment of happiness, love and
understanding; and are informed about and
participate in, achieving their rights in an Citations
accessible and active manner.2 1 UNICEF, For every child a fair chance: the promise of equity.
New York, November, 2015.
2 UN General Assembly, Convention on the Rights of the Child,
20 November 1989, United Nations, Treaty Series, vol. 1577, p. 3.
Key Messages
• Public health policy must refocus efforts towards all children and include NCDs.
• Prevention policies and programs must begin with a preconception plan and adopt
a whole-of-life approach.
11“For many children,
surviving the first years of
life with an NCD is a serious
THE GLOBAL challenge and many do not
reach the age of five.”
BURDEN
Fig. 2.2. Deaths due to NCDs in children
(CARDIOVASCULAR
DISEASE
Cardiovascular disease is broad term Management of heart disease
encompassing a number of conditions that Heart disease resulting from RHD is treatable:
affect the heart and circulation. These can be some children need heart surgery, but in many
congenital or acquired. While many are highly cases early intervention with a single procedure
treatable, their prevention and control in will lead to a normal or near-normal life. Basic
children is often inadequate partly due to a lack primary healthcare services can provide primary
of resources or awareness for early detection and secondary prevention of RHD, which
and management. More than 13.9 million includes administration of basic medications like
children in 2017 had some form of CVD. penicillin. Early identification and treatment of
the infection that can cause rheumatic fever is
Pediatric CVD is a term used to describe the best form of prevention. Secondary
several different heart conditions in children. prevention protects children who have had
The most common type of pediatric heart rheumatic fever from the recurrences that cause
disease is congenital, which means that heart damage to progress.
children are born with the defect. Globally, one
million children a year are born with a heart Pediatric stroke
defect and 90% of these are born in areas Pediatric stroke has varying mortality rates
where appropriate medical care is limited or depending on the type of stroke: arterial
unavailable.1 ischemic stroke (AIS) mortality ranges from 7%
to 28% and hemorrhagic stroke (HS) between
Rheumatic Heart Disease (RHD) is the most 6% to 54%.3 However, mortality rates for HS
common chronic heart disease in children. RHD are decreasing.4
is a caused by rheumatic fever, which is brought Pediatric arterial ischemic stroke (AIS) can
on by common infections of the throat. RHD can be divided into two main types: perinatal and
result in irreversible damage to the heart valves. childhood. Perinatal stroke occurs between 20
Without surgery and life-long medical treatment weeks of fetal life through the twenty-eighth
RHD can be fatal. Better living conditions and postnatal day. Childhood arterial ischemic
access to antibiotics have meant that in stroke defines those who have pediatric AIS
developed countries, rheumatic fever has been beyond the first month of life. The incidence of
nearly eradicated. Now it is almost exclusively a perinatal AIS is considerably higher than that of
disease of poverty RHD and is estimated to childhood AIS; with current estimates likely to
affect at least 15.6 million people each year.2 be an underestimate. Estimates of the
incidence of childhood AIS are variable and
highly dependent on the search strategy
Key Figures: Cardiovascular disease
Key Messages Measure Rate
• Deaths due to CVD are highest in (Fig. 2.3. Deaths due to CVD in children
(management. Painful blockages in blood flow
known as vasco-occlusive crises are common
in SCD. These are responsible for most of the
major complications as many organs of the
body can be affected. In childhood, infection,
stroke and acute chest syndrome (ACS)
dominate as causes of morbidity and death. In
adolescence, bacteraemias, dactylitis, ACS,
and stroke decrease in frequency, and
gallstones, episodes of severe pain, and leg
ulceration increase in frequency. Those with the
disease face the physical limitations and the
psychological impact of a serious chronic
condition. In adulthood, complications
associated with pregnancy, the eyes, and
chronic organ damage become increasingly
prevalent.
Policy frameworks
For the prevention and management of adult
CVD, the WHO has developed the Global
HEARTS Initiative, however, there is no Citations
pediatric equivalent, partly due to the fact that 1 NCD Alliance. A Focus on Children and NCDs: Remembering
our future at the UN Summit on NCDs, September 2011.
pediatric CVD has a broad etiology.12 In 2011,
the US National Heart, Lung and Blood Institute 2 Carapetis JR, Steer AC, Mulholland EK, Weber M, The global
burden of group A streptococcal diseases. The Lancet Infectious
released its Integrated Guidelines for Diseases. 2005;5(11):685-694
Cardiovascular Health and Risk Reduction in
3 Blom I, De Schryver EL, Kappelle LJ, Rinkel GJ, Jennekens-
Children and Adolescents. The guidelines’ Schinkel A, Peters AC.Prognosis of haemorrhagic stroke in
recommendations were controversial and not childhood: a long-term follow-up study.Dev Med Child Neurol.
2003; 45:233–239.
universally embraced, but they did suggested
potential avenues for key research. In the same 4 Fullerton HJ, Chetkovich DM, Wu YW, Smith WS, Johnston
SC.Deaths from stroke in US children, 1979 to 1998.Neurology.
year, the WHO released the Global Atlas on 2002; 59:34–39.
Disease Prevention and Control. Although the
5 Felling, Sun, Maxwell et al Cardiovascular disease risk in
document does not specifically address the healthy children and its association with body mass index:
issues of CVD in children, it does address systematic review and meta-analysis Blood Cells, Molecules and
Diseases 67 (2017) 23–3.
several contributing factors, such as obesity,
rheumatic fever and Chagas disease. 6 Greenham M, Gordon A, Anderson V, Mackay MT. Outcome in
Childhood Stroke. Stroke 2016;47:1159–1164.
7 Lo WD, Hajek C, Pappa C, Wang W, Zumberge N.Outcomes in
children with hemorrhagic stroke.JAMA Neurol. 2013; 70:66–71
8 Monagle, P, Chan A.K.,Goldenberg N.A.et al, American College
of Chest P, Antithrombotic therapy in neonates and children:
antithrombotic therapy and prevention of thrombosis, 9th ed:
American College of Chest Physicians Evidence-Based Clinical
Practice Guidelines, Chest 141 (2 Suppl) (2012) e737S–e801S,
9 Roach, ES, Golomb, MR. Adams R,et al, American Heart
Association Stroke C, Council on Cardiovascular Disease in the
Y. Management of stroke in infants and children: a scientific
statement from a Special Writing Group of the American Heart
Association Stroke Council and the Council on Cardiovascular
Disease in the Young, Stroke 39 (9) (2008) 2644–2691.
10 Weatherall DJ, Clegg JB. Inherited haemoglobin disorders: an
increasing global health problem. Bull World Health Organisation
2001; 79(8):704-712.
11 World Health Organization. Joint WHO/TIF Meeting on the
Control of Haemoglobinopathies. Report of the VIIth Meeting of
the WHO Working Group on the Control of Hereditary Anaemias,
Nicosia, Cyprus, 3-4 April, 1994. (unpublished document WHO/
HDP/TIF/HA/93.1). 1994. Geneva, WHO.
12 Global Atlas on Cardiovascular Disease Prevention and
Control. Mendis S, Puska P, NorrvingB editors. World Health
Organization, Geneva 2011.
15CANCER
The term “childhood cancer” is most commonly Although many studies have tried to identify
used to designate cancers that arise before the the causes of childhood cancers, the vast
age of 15. The most common categories of majority have no known cause, with a minimal
childhood cancers include leukemias, brain number of cancers in children being due to
cancers, lymphomas and solid tumors (Table environmental or lifestyle factors. Only 10% of
2.1). Acute lymphoblastic leukemia is the most all children with cancer are attributable to
common type of cancer, except in sub-Saharan genetic factors.
Africa, where children are more prone to Some infections are risk factors for
develop non-Hodgkin’s lymphomas and childhood cancer, while others increase the risk
Kaposi’s sarcoma (related to HIV infection). of developing cancer as an adult. As a result of
Cancer in childhood represents between the limited understanding of the causes of
0.5% and 4.6% of the total number of cancer c h i l d h o o d c a n c e r s , t h e Wo r l d H e a l t h
cases in the world. Overall, annual incidence Organization (WHO) suggests that cancer
rates vary between 9 and 22 per 100,000 in prevention in children should aim to promote
children and around 14 per 100,000 in behaviors that will prevent the child from
adolescents (Fig. 2.4). The youngest age group, developing preventable cancer as an adult. In
1 to 4 years, has the highest incidence relative LMICs, efforts should include vaccination,
to other groups, possibly due to genetically screening and early diagnosis of chronic
linked diseases, with girls having a higher infections that lead to cancer.
prevalence of cancer in each age group than
boys (Fig. 2.5).
Fig. 2.4. Incidence of cancer in children
Cancer is a leading cause of death for (Fig. 2.5. Prevalence of cancer in children (
Table 2.1. Top cancers in children (
CHRONIC
RESPIRATORY
DISORDERS
In children, chronic respiratory disorders barriers to optimal treatment. These barriers
(CRDs) contribute to disability and range from reduced availability of medications
hospitalization in children (Fig 2.6). Some of to more societal factors such as poverty and
these respiratory disorders are preventable literacy. In LMICs, this reduced access to
including asthma and respiratory allergies. treatment is compounded by the lack of
Preventable CRDs affect millions, especially the resources to enable diagnosis of CRDs.
young and elderly, with more than 500 million of Allergic rhinitis (AR) and asthma are the
these people living in low- and middle-income most common preventable CRDs in children.
countries (LMICs). The most common AR is characterized by one or more symptoms,
preventable CRDs are: chronic obstructive such as sneezing, itching, nasal congestion and
respiratory disease (COPD), sleep apnea, runny nose. If treatment is not adequate,
allergic rhinitis, and asthma. Of these, the last children can experience chronic inflammation
two greatly affect child health. which can induce a range medical
There are many risk factors for preventable complications, learning and behavioral issues,
CRDs but the most significant fall into three as well as aggravate conditions such as
categories: sinusitis and asthma.
• indoor (pollution, pets, and insects), Children and adolescents are the most
• outdoor (pollution, pollens and molds), commonly affected by AR with a prevalence up
• and occupational agents (platinum salts, to 40% of the population.2 AR is a multifactorial
flour and latex) that more common for disease with genetic as well as environmental
working adults.
In LMICs, solid fuels are a major source of Fig. 2.7 Deaths due to CRD in children
indoor pollution with children under 5 and (factors influencing disease development. variability in the prevalence and severity of
Sensitization to allergens at an early age along asthma between regions and countries as well
with a range of maternal and in utero factors as within countries.4
contribute to the risk of developing AR. Not Asthma is rarely a cause of death in
surprisingly, outdoor allergens appear to children, but it can be an important source of
constitute a greater risk for seasonal rhinitis disability and hospitalization. Childhood asthma
while indoor allergens pose a greater risk for can result in many lost school days and may
perennial rhinitis. deprive the affected children of both academic
achievement and social interaction.
Asthma There are genetic and non-genetic factors
Another common cause of CRDs in children, contributing to asthma with the disease often
asthma is described as a heterogeneous running in families. Although a number of
disease usually characterized by chronic airway factors that can cause exacerbations in
inflammation. Symptoms include wheeze, symptoms have been identified, there is no
shortness of breath, chest tightness, cough and recognized cause. Environmental factors,
expiratory airflow limitation that vary over time particularly indoor allergens (including smoking
and in intensity.3 in the household) are more likely to be
The prevalence of asthma in children is responsible for a large portion of the numbers
rising and is highest among children under 9 of people with asthma. In addition to this focus
years. The International Study of Asthma and on environmental factors, it is now understood
Allergies in Childhood highlighted the wide that allergic mechanisms are only responsible
Fig. 2.7 Prevalence of asthma in children (for no more than 50% of asthma cases. 3. Encouraging the implementation of health
However, the non-allergic mechanisms are not promotion and CRD prevention policies;
fully understood. 4. Developing simple and affordable strategies
for the control of CRDs.
Management and care
The most common diagnostic tests for AR are In addition to these objectives, GARD also has
the percutaneous skin test and allergen specific 6 areas of focus, one of which is pediatric
IgE antibody test. Treatment of AR includes the asthma.
avoidance of allergens, use of antihistamine
tablets or nasal sprays and in some cases In 2017, the Forum of International Respiratory
desensitization. Societies (FIRS) called for eight essential
Asthma treatment comprises actions to reduce the burden of respiratory
“relievers” (bronchodilators that reverse airway disease. These actions supported the WHO
narrowing) and “controllers” (inhaled strategy goals and included improved early
corticosteroids) that reduce the underlying diagnosis of respiratory diseases, ultimate
airway inflammation. Diagnosis and treatment elimination of tobacco products and increased
for CRDs are more widely available in high education of health professionals.5 Their first
income countries. With rising air pollution in essential action specifically mentioned children:
many developing countries, rates of asthma
and AR are expected to rise in the coming “Increase public and policy makers’
decades. awareness that respiratory health is
essential to global health and that
childhood respiratory disease may have
Policy frameworks
long-term negative consequences on
In 2002, the WHO launched its strategy on
adult health by advocating at world
CRDs; the strategy has three key objectives:
health meetings and through
• Improved surveillance to enable mapping publications and media postings.”
of the magnitude of CRDs and analyze
their determinants; Formed in 2001 FIRS comprises the leading
• Reductions in the level of exposure of international respiratory societies with the goal
individuals and populations to common of promoting worldwide respiratory health.
risk factors, particularly tobacco, poor
nutrition, frequent lower respiratory
infections during childhood, and
environmental air pollution (primary
prevention);
• Secondary and tertiary prevention to
strengthen health care for people with
CRDs by identifying cost-effective
interventions, upgrading standards and
accessibility of care at different levels of
the health care system.3
This was followed by the launch of the Global
Alliance Against Respiratory Diseases (GARD) Citations
which in 2006 brought together a range of 1 Bousquet J, Khaltaev N. Global surveillance, prevention and
control of Chronic Respiratory Diseases. A comprehensive
international and national organizations with the approach. (2007), WHO, Geneva, Switzerland
aim of improving the lives of those affected by
2 Mims JW. Epidemiology of allergic rhinitis. Int Forum Allergy
respiratory diseases. It initiated the Rhinol 2014;4 Suppl 2:S18-20
i m p l e m e n t a t i o n o f t h e C R D s t r a t e g y.
3 Global Initiative for Asthma (GINA), Global strategy for asthma
Consequently, the main objective of GARD is to management and prevention. 2018. Available from http://
apply a comprehensive approach to combat www.ginasthma.org/
CRDs by: 4 Mallol J, Crane J, von Mutius E, Odhiambod J, Keile U, Stewart
A, et al. The International Study of Asthma and Allergies in
1. Developing standardized methods for Childhood (ISAAC) Phase Three: A global synthesis. Allergol
surveillance of the burden of chronic Immunopathol (Madr). 2013; 41: 73–85
respiratory diseases and their risk factors; 5 Forum of International Respiratory Societies. The Global Impact
of Respiratory Disease – Second Edition. Sheffield, European
2. Advocating for action on chronic respiratory Respiratory Society, 2017.
diseases;
21DIABETES
More than 8 million children in 2017 were leading to a life threatening condition called
affected by diabetes. There are three main diabetic ketoacidosis (DKA). While DKA is also
types of diabetes which affect children. Type 1 found in type 2 diabetes, it is more common and
diabetes, representing up to 25% of cases of more severe in people with type 1 diabetes and
diabetes, is characterized by an inability to is often the first sign of the disease.
produce the hormone insulin due to inactive Type 1 diabetes is more common in high
beta cells in the pancreas, leading to an income countries which is largely due to high
uncontrolled rise in blood glucose. People with mortality rates in developing countries. Still, the
type 2 diabetes produce insulin, but their cells incidence of type 1 diabetes is increasing
and tissues become insensitive to the hormone, globally for reasons that are not clear (Fig. 2.9).
leading to high blood glucose. The prevalence Mortality rates in developing countries, where
for both types of diabetes is highest in access to insulin is limited are higher, leading to
adolescents (Fig. 2.8). A third kind of diabetes, fewer children overall living with the disease.
gestational diabetes, arises during pregnancy Indeed, many deaths due to diabetes occur in
and can pose risks to both mother and child. children under 14 often at the point of diagnosis
More detail is given on gestational diabetes in (Fig. 2.10).1
the chapter discussing early life development.
Type 1 and type 2 diabetes require lifelong Fig. 2.8. Prevalence of diabetes in children
careful self-management and care. People with (Fig. 2.9 Deaths due to diabetes in Fig. 2.10. Trends in incidence of type 1
children (MENTAL HEALTH
DISORDERS
Mental health disorders are the most prevalent
NCD in children under 20 years affecting more
than 231 million children. They encompass a Fig. 2.11. Deaths due to self-harm in
children (Fig. 2.13. Trends in substance abuse disorders in children
(not just on children with mental health disorders
but also in preventing new cases from
developing.5 They have also shown great
promise in resource-limited settings both with
low income communities and in low- and
middle-income countries.6,7
Policy frameworks
Healthcare providers and caregivers must be
made aware of the warning signs and risk
factors of mental health disorders and risky
behavior. The WHO, respecting the United
Nations Convention on the Rights of the Child,
recommends targeting multiple mental health
problems at diagnosis, using supervised staff
trained in managing adolescents’ specific
needs, engaging and empowering caregivers,
guided self-help methods, and cautions against
the overuse of psychotropic medication as only “Treatment of mental health
appropriate for those with moderate-severe
mental health conditions.
disorders is still hampered
Nevertheless, developing countries and by stigma and a lack of
low-resource areas struggle to provide awareness of the prevalence
adequate mental health support and
adolescents may remain in a precarious of these conditions in
position if their needs are not met. children.”
References
1 World Health Organization (2019). Adolescent mental health.
[online] Who.int. Available at: https://www.who.int/news-room/
fact-sheets/detail/adolescent-mental-health [Accessed 8 May
2019].
2 O’Donnell KJ, Meaney MJ. Fetal origins of mental health: the
developmental origins of health and disease hypothesis. Am J
Psychiatry. 2017 Apr 1; 174(4):319-328.
3 Hawkes, N. (2018). Barriers for mental health services for
children and adolescents are too high, finds regulator. BMJ,
k1093. doi:10.1136/bmj.k1093
4 MacDonald, K., Fainman-Adelman, N., Anderson, K. K., & Iyer,
S. N. (2018). Pathways to mental health services for young
people: a systematic review. Social psychiatry and psychiatric
epidemiology, 53(10), 1005–1038.
5 Christensen, H., Pallister, E., Smale, S. et al. J Primary Prevent
(2010) 31: 139.
6 Farahmand, F. K., Grant, K. E., Polo, A. J. and Duffy, S. N.
(2011), School‐Based Mental Health and Behavioral Programs for
Low‐Income, Urban Youth: A Systematic and Meta‐Analytic
Review. Clinical Psychology: Science and Practice, 18: 372-390.
7 Barry M.M., Clarke A.M., Jenkins, R. and Patel, V. (2013) A
systematic review of the effectiveness of mental health promotion
interventions for young people in low and middle income
countries. BMC Public Health, 13: 835.
26INJURIES AND
VIOLENCE
In 2017, injury was responsible for more than violence including: economic development,
707,000 deaths in children and young people status, age, sex and gender. The rate of
under 20 years. Injury can be divided into two intentional injury in children is higher in upper-
categories: intentional (including sexual middle income countries (2,086 per 100,000)
violence, homicide, and suicide) or than the global average (1,512 per 100,000).
unintentional (including drowning, falls, The GBD Study estimates that in 2017,
poisoning and road traffic accidents).1 27.1 million girls and 8.6 million boys
Intentional injury to self or by others experienced sexual violence. The majority of
(violence) against children occurs regardless of this sexual violence is committed by family
geography, race, class, religion and culture. members or other people staying or visiting a
Perpetrators can be from inside or outside the child’s family home. A review of epidemiological
family and it occurs in a range of settings. Of surveys from 21 countries, mainly high- and
these child victims, most were between 15 and middle-income countries, found that at least 7 to
19 years of age; 75% of these deaths occurred 36% of females and 3 to 29% of males reported
in boys (Table 2.2).2 sexual victimization during their childhood.3
For infants the risk of death is about three
times greater for children under one year old Unintentional injuries
than for those aged 1 to 4. The younger the Unintentional injuries (Table 2.3) account for
child, the more likely their death will be caused almost 90% of all injuries and they are the
by a close family member. There are many leading cause of death for children aged 10 to
factors associated with the risk of lethal 19 years. These include falls, the most common
Table 2.2. Top prevalence per 100,000 of causes of intentional injuries for children
(Table 2.3. Prevalence and deaths due to unintentional injuries in children (
“At each stage, the
environment a child is
exposed to will influence
his or her chances of CROSS-CUTTING
developing an NCD.”
ISSUES
The health of a child and the future risk for
developing disease is influenced by more than
just biology. The environment the child lives in,
the care available to him or her and interactions
with peers and society all have a powerful
influence on health. That environment starts in
the earliest development in the womb, through
early life through to young childhood and
adolescents. At each stage the environment a
child is exposed to will influence his or her
chances of developing an NCD. Factors such
as air pollution, nutrition, social norms around
physical activity and other behaviors, the
influence of peers, exposure to violence,
access to education, and household income all
play a role.
The requirements for care for children then
become important to be tailored not just to the
individual, but to the circumstances of the
community in which the child lives and the
stage of development. This chapter examines
the social determinants of health that have a
strong influence on the development and
management of NCDs, the influence of the
earliest life experience on the future risk of
NCDs, and how treatment and care can
respond for the prevention and control of NCDs.
It discusses the earliest ages of development
through to the impact of communities,
environment, health care, and government
policies.
Key Messages
• The health of a child is determined not only by biological factors, but also by their
social and economic realities.
• A lifetime risk for NCDs can start in the womb.
• Managing NCDs in children requires a tailored approach with training and education
for the workforce and community engagement
29THE SOCIAL
DETERMINANTS OF
HEALTH
In 2003, the World Health Organization Within countries, those at lower
recognized that health is influenced by the socioeconomic levels are more likely to be
conditions in which people are “born, grow, obese, have an increase risk of NCDs, and less
work, live, and age, and the wider set of forces likely to have access to care. 2 These
and systems shaping the conditions of daily inequalities extend to several NCDS. Mental
life.”1 These forces are influenced by policy, health issues, in particular, tend to be higher in
economics, development, social norms and children of lower socioeconomic status because
political systems, all of which play a role in the of complex drivers such as more exposure to
health and development of a child. Together violence and bullying, less family support, and
these elements are known as the “social discrimination.1
determinants of health” and are often used to
discover and understand inequalities in health Gender and ethnicity
among and between groups. Identifying Gender and ethnicity can also play a role in
inequalities can help to target aid and treatment driving inequalities. For example, girls are more
to specific groups who may be more vulnerable likely than boys to be physically inactive which
to disease or its effects. In general, children are can have effects on obesity, cardiovascular
considered a vulnerable group when compared health, mental health, and other risk factors for
to adults because they are less able to NCDs.3 Girls are also at risk of early pregnancy
advocate for themselves, are socially and and NCD-related complications such as
economically dependent on others and often preeclampsia and maternal mortality. On the
suffer the worst effects from inequalities. other hand, boys are more likely to engage in
risky behaviors leading to injuries and violence,
Socioeconomic status more likely to smoke, and more likely to
The socioeconomic status of a household can consume harmful amounts of alcohol.3
have a profound influence on health. The most Some ethnic groups are more likely to
obvious way in which this may happen is the develop NCDs. Diabetes is high among Pacific
ability to purchase food, access healthcare, or Islanders, Southeast Asians, and native
provide for the basic needs of survival. populations around the world and gestational
However, social factors may also play a role. As diabetes in these populations means that
countries and economies have developed, children born of mothers with high blood
issues related to poverty such as malnutrition glucose during pregnancy carry a greater risk
have decreased. However, access to cheap for type 2 diabetes later in life.4 Sickle cell
and unhealthy foods is on the rise and disease, a condition where hemoglobin is
especially in developing countries, leading to an produced abnormally in red blood cells, is more
increase in prevalence of obesity in children prevalent in people of African descent and can
(Fig 3.1). lead to lifelong risks for pain, infection, organ
Key Messages
• Several factors can contribute to the health and development of a child including:
gender, access to education, household income, ethnicity, and socioeconomic status.
• With economic development, NCDs in children has also increased.
• Adequate care and resources for health are lacking in developing countries,
contributing to a higher mortality for children there with NCDs.
30Fig. 3.1. Trends in prevalence of obesity (%) in children (
EARLY LIFE
EXPERIENCES
A person’s lifelong risk for NCDs can start as experience extreme stress or trauma during
early as development in the womb, where the pregnancy can lead to a uterine environment for
intrauterine environment can play a significant a developing fetus that will affect their genetic
role in the later development of NCDs and propensity to develop mental health problems
obesity. For example, mothers with untreated later in life.5 Even after birth, the life experience
high blood glucose during pregnancy can of children in their earliest years can have a
experience greater risks of complications great impact on their risk for developing MHDs.
including macrosomia, obstructed labor, and Left untreated or unmanaged, this pattern can
other immediate issues but also will have set up a cycle of MHDs generations.5
babies who have a higher lifelong risk of
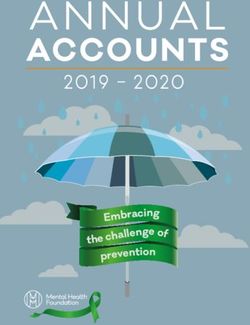
developing type 2 diabetes.1 As the epidemic of Infant feeding and early life experience
type 2 diabetes increases, and more women of After birth, what mother and child eat and the
reproductive age experience high blood environment in which they live can also have a
glucose, more babies will be born with an profound impact on a child’s future risk for
added future risk for obesity and type 2 NCDs. The World Health Organization
diabetes (Fig 3.2).2 recommends an early introduction to
These increases are expected especially in breastfeeding - within the first hour after birth -
developing countries where the rate of new and exclusive breastfeeding for at least 6
cases of type 2 diabetes is highest.3 The months. A child who follows these
mechanisms for these changes are being recommendations is less likely to develop
described in research which indicates that the obesity and type 2 diabetes later in life and
nutrition and health status of the mother can more likely to have greater educational
have permanent effects on the growth and achievement.6 The benefits of breastfeeding
structure of the child in a phenomenon known have shown to reduce a mother’s risk of ovarian
as ‘fetal programming.’4 Growing evidence and breast cancer, type 2 diabetes, and
suggests that the presence of NCDs or obesity, cardiovascular disease and hypertension.7-9
in particular, can have a detrimental effect on
the development of the child leading to the Early pregnancy and NCDs
development of metabolic and other problems Adolescent pregnancy carries a number of risks
later in life.4 These changes can lead to a related to NCDs for mother and child. An
generational transmission of NCDs from mother adolescent pregnancy is more likely to
to child, especially in the absence of adequate experience complications such as low birth
treatment and prevention. weight, preeclampsia (high blood pressure
during pregnancy), anemia, and preterm
Mental health disorders and early life delivery and is a leading cause of death for
One of the most prevalent NCDs in children, the girls.9 While some of these are related to
risk for mental health disorders (MHDs) can biological factors, there is evidence that
develop as early as in the womb. Mothers who pregnant adolescents do not access antenatal
Key Messages
• Risk for NCDs can be established as early as the womb.
• Early life experiences and exposures can strongly affect a child’s risk for NCDs and
their outcomes.
• Mothers experiencing NCDs or their risk factors during pregnancy are at future risk
for illness.
32Fig. 3.2. Pregnancies affected by high blood glucose, by age, 2013
9M Number of pregnancies 60%
Prevalence (%)
Number of pregnancies
7M
Prevalence (%)
5M 30%
2M
0M 0%
20 to 24 25 to 29 30 to 34 35 to 39 40 to 44 45 to 49
Age (years) Source: Adapted from Guariguata et al2
care at the same rates as older women putting and management of women with high blood
themselves and their babies at risk.10 glucose in pregnancy.14 In addition, guidelines
Other factors, such as poor dietary habits, on breastfeeding also reinforce the links to
tend to be higher in adolescents and can affect obesity and NCD risk reduction for children and
both mother and child.11 In many parts of the mother.15
world, adolescent pregnancy can result from a
lack of agency for girls, early marriage Citations
influenced by social and family pressures, lack 1 International Diabetes Federation, IDF Diabetes Atlas 6th
Edition. Brussels, Belgium. 2013.
of awareness on sexual education, and sexual
violence.12 Girls who become pregnant earlier 2 Guariguata L, Linnenkamp U, Beagley J, Whiting DR, Cho NH.
Global estimates of the prevalence of hyperglycaemia in
are also less likely to achieve education goals, pregnancy. Diabetes Res Clin Pract. 2014 Feb;103(2):176-85.
thus setting them up for a higher risk of poverty
3 Institute of Health Metrics and Evaluation, University of
and lower socioeconomic status which is Washington. Global Burden of Disease (GBD) Study 2017.
increasingly linked to obesity (see chapter on Seattle, WA, 2017. http://ghdx.healthdata.org/gbd-results-tool
Social Determinants of Health). 4 Fall C. H. (2012). Fetal programming and the risk of
Early screening for NCDs in pregnancy, noncommunicable disease. Indian journal of pediatrics, 80 Suppl
1(0 1), S13–S20.
comprehensive antenatal care, and family
planning can all help improve outcomes for 5 McGowan PO, Syzf M. The epigenetics of social adversity in
early life: implications for mental health outcomes. Neurbiol Dis.
mothers and children - preventing future cases 2010 Jul;39(1):66-72.
of NCDs. Special attention and care should be
6 Lutter C, Lutter R. Fetal and Early Childhood Undernutrition,
given to delaying pregnancy in girls and Mortality, and Lifelong Health. Science, 337 (6101): 1495-1499.
promoting their education achievement. The
7 Danforth, D.N. et al. Breastfeeding and risk of ovarian cancer in
early life experience of the child can also have two prospective cohorts. Cancer Causes Control. 2007. 18 (5):
a great impact on future NCD risks thus making 517-23.
it important for mothers to receive care and 8 Martin, R.M. et al. Breastfeeding and cancer: the Boyd Orr
support for nutrition and breastfeeding, even cohort and a systematic review with meta-analysis. J Natl Cancer
Inst. 97 (19): 1446-57 (2005)
after the birth of a child.
9 Conde-Agudelo, A., Belizán, J. M., & Lammers, C. (2005).
Maternal-perinatal morbidity and mortality associated with
Policy frameworks adolescent pregnancy in Latin America: Cross-sectional study.
The World Health Organization has produced a American Journal of Obstetrics and Gynecology, 192(2), 342-349.
comprehensive guide for essential practice in 10 Loto, O., Ezechi, O., Kalu, B., Loto, A. B., Ezechi, L. O., &
pregnancy, childbirth, postpartum and newborn Ogunniyi, S. (2004). Poor obstetric performance of teenagers: is it
age- or quality of care-related? Journal of Obstetrics and
care.13 The guideline stresses the importance of Gynaecology, 24(4), 395-398.
antenatal care, an attended birth, and continued
11 Gutierrez, Y., & King, J. C. (1993). Nutrition During Teenage
monitoring in the first few weeks and months of Pregnancy. Pediatric Annals, 22(2), 99-99.
life for both mother child. These guidelines have
12 Plan International. (n.d.). Teenage pregnancy. Retrieved from
contributed greatly to the overall global https://plan-international.org/sexual-health/teenage-pregnancy
reduction in maternal and child mortality. They
13 World Health Organization. Pregnancy, childbirth, postpartum
also include recommendations on tobacco use and newborn care: a guide for essential practice - 3rd ed.
and postpartum depression but do not address Geneva, Switzerland. 2015.
NCDs during pregnancy in any specific way. 14 World Health Organization. Diagnostic criteria and
But awareness is growing. In 2013, the classification of hyperglycaemia first detected in pregnancy.
Geneva, Switzerland. 2013.
WHO produced guidelines on the screening
15 World Health Organization. Global strategy for the infant and
young child feeding. Geneva, Switzerland. 2003.
33You can also read