Blood haemoglobin is an independent predictor of B-type natriuretic peptide (BNP)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical Science (2005) 109, 69–74 (Printed in Great Britain) 69
Blood haemoglobin is an independent predictor
of B-type natriuretic peptide (BNP)
Cathrine WOLD KNUDSEN∗ , Harald VIK-MO† and Torbjørn OMLAND‡§
∗
Department of Cardiology, Ullevål University Hospital, Oslo, Norway, †Cardiology Division, Department of Medicine, St Olav’s
Hospital, Trondheim, Norway, ‡University of Oslo, Faculty Division Akershus University Hospital, Nordbyhagen, Norway, and
§Department of Medicine, Akershus University Hospital, Lørenskog, Norway
A B S T R A C T
BNP (B-type natriuretic peptide) and anaemia are both associated with adverse outcome in patients
with chronic heart failure. Whether low haemoglobin levels are independently predictive of ele-
vated BNP levels in subjects without heart failure is unknown. In the present study, we examined
the relationship between haemoglobin and BNP levels in 234 patients with suspected coronary
heart disease without a history of chronic heart failure, adjusting for known predictors of BNP
levels. By univariate analysis, haemoglobin levels were inversely related to logarithmically trans-
formed BNP values (r = − 0.30, P < 0.0001). After adjustment for patient age, gender, body mass
index, history of myocardial infarction, use of diuretics, angiotensin-converting enzyme inhibitors
and β-blockers, estimated creatinine clearance rate, extent of coronary disease, left ventricular
ejection fraction and left ventricular end-diastolic pressure, blood haemoglobin remained an
independent predictor of plasma BNP (standardized β-coefficient = − 0.253, P < 0.0001). A similar
relationship was observed between haematocrit and BNP (standardized β-coefficient − 0.215,
P < 0.0001). We conclude that haemoglobin levels are independently predictive of plasma BNP
levels in patients with suspected coronary heart disease without heart failure. Anaemia may contri-
bute to elevated BNP levels in the absence of heart failure, and may represent an important
confounder of the relationship between BNP, cardiac function and prognosis.
INTRODUCTION nary artery disease [10], in patients with heart failure
[11,12] and in the general population [13]. A number
BNP (B-type natriuretic peptide) is a 32-amino-acid of non-cardiac factors are associated with circulating
hormone derived predominantly from the ventricular BNP levels and may confound the relationship be-
myocardium [1]. The main stimulus for BNP secretion tween BNP and indices of cardiac function, including age
is stretch of cardiomyocytes [2]. Accordingly, circulating [14,15], gender [14,15], renal function [16] and BMI (body
BNP levels are elevated in conditions characterized by mass index) [17]. Whether anaemia is a confounding
volume overload and correlate with indices of haemo- factor for BNP is unknown.
dynamic status and ventricular function [3,4]. Over the Anaemia of chronic disease is a common cause of
past few years BNP has emerged as a reliable marker low haemoglobin levels in patients with chronic heart
of heart failure [5], and fully automated biochemical failure and is particularly prevalent in advanced heart fail-
assays have been developed for clinical use. BNP is also ure, where its presence is associated with an adverse
a powerful prognostic indicator in patients with acute prognosis [18–20]. Recently, an inverse association be-
coronary syndromes [6–9], in patients with stable coro- tween haemoglobin levels and BNP has been described
Key words: anaemia, B-type natriuretic peptide (BNP), haemoglobin, heart failure.
Abbreviations: ACE, angiotensin-converting enzyme; BMI, body mass index; BNP, B-type natriuretic peptide; LVEDP, left
ventricular end-diastolic pressure; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association.
Correspondence: Professor Torbjørn Omland, University of Oslo, Faculty Division Akershus University Hospital, NO-1474
Nordbyhagen, Norway (email torbjorn.omland@medisin.uio.no).
C 2005 The Biochemical Society70 C. Wold Knudsen, H. Vik-Mo and T. Omland
in patients with diastolic heart failure [21]. One contri- chilled plastic tube containing EDTA and aprotinin. The
buting factor to the anaemia in heart failure may be test tube was immediately placed on ice and centrifuged
haemodilution secondary to fluid retention, a mechanism at 4 ◦ C within 15 min of blood collection. After blood
that could explain an inverse association between BNP sampling, the catheter was first placed in the ascending
and anaemia in heart failure patients. However, factors aorta for aortic blood pressure recording, then introduced
other than haemodilution may potentially contribute to retrogradely into the left ventricle through the aortic valve
a relationship between BNP and haemoglobin levels. for intraventricular blood pressure recording. LVEF (left
To test the hypothesis that haemoglobin is an inde- ventricular ejection fraction) was ascertained by single-
pendent predictor of BNP in subjects without heart plane contrast ventriculography in the 30◦ right oblique
failure, we examined the association between haemo- position during held inspiration, using the area–length
globin and BNP levels in a large cohort of patients with method. Haemodynamic measurements were performed
suspected coronary artery disease, adjusting for estab- by a single investigator, who was blinded to the BNP
lished predictors of BNP. data. Significant coronary artery disease was defined as a
diameter stenosis of at least 50 % in any of the main epicar-
dial coronary arteries. Patients were classified according
MATERIALS AND METHODS to the number of main vessels affected as no significant
coronary artery disease, single-vessel disease, double-
Patients vessel disease, and triple-vessel disease.
A series of 263 patients, referred to diagnostic cardiac
catheterization for suspected coronary heart disease, were
included consecutively. Patients with a recent myocardial Biochemical analyses
infarction (< 2 weeks), significant valvular heart disease, The plasma samples were stored for a maximum of
significant cardiac arrhythmia (including atrial fibrilla- 12 months at − 70 ◦ C pending analysis of BNP. BNP in
tion), ongoing myocardial ischaemia as evidenced by plasma was determined using RIA after prior extraction
ST-T segment depression, manifest renal or hepatic fai- with Vycor glass (Crown Crossing, Liverpool, New
lure, or chronic symptomatic congestive heart failure South Wales, Australia) [22]. The intra- and inter-assay
[NYHA (New York Heart Association) class III and IV] coefficients of variation were 7 % and 10 % respectively.
were ineligible. Thirteen patients with mild exertional The blood concentration of haemoglobin, haematocrit
dyspnoea (NYHA function class II) were also excluded and the concentration of creatinine in serum were deter-
from the current analysis. Sixteen additional patients were mined by routine laboratory methods. The creatinine
excluded from the analysis because of cardiac arrhythmia clearance rate (in ml/min) was estimated using the Cock-
during the investigation (three patients), pronounced roft-Gault formula [(140 − age) × weight (kg)/serum cre-
vasovagal reaction requiring leg elevation during the in- atinine (µmol/l)] multiplied by a constant of 1.25 in men
vestigation (one patient), discovery of undiagnosed mitral and 1.03 in women.
valve prolapse (one patient), recent undiagnosed myocar-
dial infarction (one patient), technical errors in blood Statistical analysis
sample handling (three patients), and insufficient material We present categorical variables as counts and percentages
for analysis of BNP or haemoglobin (seven patients), of total and continuous variables as median and inter-
leaving 234 patients for data analysis. The baseline data quartile range. We analysed BNP as a continuous vari-
of this cohort have been published previously [6]. Prior able after logarithmic transformation to normalize its
to catheterization, all patients were interviewed and distribution. Differences between groups (anaemia com-
examined by two experienced physicians who followed pared with no anaemia) were assessed by the Mann–
a standardized procedure. The same morning a venous Whitney U test for continuous variables and by χ 2
blood sample for determination of haemoglobin and tests for categorical variables. The relationship between
serum electrolytes and creatinine was obtained. continuous variables, including haemoglobin, haemato-
All patients gave their informed written consent to crit, LVEF and LVEDP (left ventricular end-diastolic
participate in the study. The study protocol was approved pressure), and BNP was assessed by Pearson correlation
by the Regional Ethics Committee and was carried out in tests. Predictors of BNP and haemoglobin levels were
accordance with the Declaration of Helsinki. identified by least squares multivariate linear regression
analysis, using logarithmically transformed BNP and
Angiography and blood sampling blood haemoglobin respectively, as the dependent vari-
procedures ables. Potential confounders were forced into the model
After rest for at least 15 min, the femoral artery and vein and standardized β-coefficients were calculated. The ex-
were cannulated and a pigtail catheter introduced into the planatory power of the model was expressed as adjusted
aorta. Before contrast ventriculography, a 10 ml blood R2 values. A two-sided P value < 0.05 was considered
sample was drawn from the descending aorta into a pre- significant.
C 2005 The Biochemical SocietyB-type natriuretic peptide and anaemia 71
Table 1 Characteristics of patients in the study population and when divided into those without and with anaemia
Values are medians (interquartile range) or n (%). CCS, Canadian Cardiovascular Society.
Patients
Variable Study population Without anaemia With anaemia P value
Demographics
Number 234 217 17
Age (years) 60 (52–67) 60 (52–67) 64 (57–71) 0.109
Male gender 178 (76.1 %) 163 15 0.222
Medical history
Myocardial infarction 109 (46.6 %) 101 8 0.967
Angina CCS class IV 12 (5.2 %) 9 3 0.015
Coronary artery bypass grafting 32 (13.7 %) 29 3 0.621
Percutaneous coronary intervention 39 (16.7 %) 35 4 0.430
Pulmonary disease 3 (1.3 %) 3 0 0.626
Arterial hypertension 77 (32.9 %) 72 5 0.750
Diabetes mellitus 11 (4.7 %) 10 1 0.811
Current status
Current smoker 56 (23.9 %) 50 6 0.264
BMI (kg/m2 ) 25.7 (23.5–28.4) 25.7 (23.3–28.4) 25.6 (24.9–28.2) 0.543
Drug treatment
Aspirin 180 (76.9 %) 165 15 0.250
β-Blockers 177 (75.6 %) 165 12 0.614
Calcium channel blockers 75 (32.1 %) 67 8 0.169
Lipid-lowering drugs 20 (8.5 %) 18 2 0.622
Diuretics 18 (7.7 %) 16 2 0.513
ACE inhibitors 23 (9.8 %) 20 3 0.261
Angiographic findings
LVEF (%) 67 (60–74) 67 (60–74) 69 (59–74) 0.659
LVEDP (mmHg) 14 (11–18) 15 (11–18) 12 (11–18) 0.552
No significant coronary artery disease 36 (15.4 %) 35 1 0.259
Single-vessel disease 52 (22.2 %) 48 4 0.893
Double-vessel disease 60 (25.6 %) 55 5 0.712
Triple-vessel disease 86 (36.8 %) 79 7 0.694
Biochemical markers
BNP (pg/ml) 45 (31–66) 41.6 (29.4–65.8) 52.0 (36.4–88.3) 0.07
Log BNP (pg/ml) 1.11 (0.95–1.28) 1.08 (0.93–1.28) 1.18 (1.02–1.41) 0.07
Creatinine clearance (ml/min) 83 (67–100) 83 (67–100) 87 (65–100) 0.817
Blood haemoglobin (g/dl) 14.1 (13.4–14.9) 14.2 (13.6–14.9) 12.4 (12.0–12.6) 0.000
Haematocrit 0.43 (0.41–0.44) 0.43 (0.41–0.45) 0.38 (0.37–0.38) 0.000
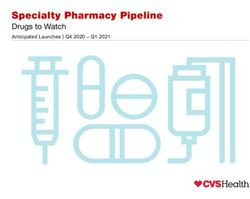
RESULTS 234), and were correlated inversely with blood haemo-
globin (r = − 0.30; P < 0.0001; n = 234; Figure 1) and
The characteristics of the patients are presented in haematocrit (r = − 0.294, P < 0.0001; n = 194). The rela-
Table 1. Using the World Health Organization definition tionship with haemoglobin was evident both in patients
(haemoglobin < 12 g/dl for women and < 13 g/dl for with (r = − 0.301, P < 0.0001; n = 198) and without (r =
men), 17 patients (7.3 %) were diagnosed with anaemia. − 0.424, P = 0.010; n = 36) angiographically significant
The characteristics of patients subdivided according to the coronary artery disease. In a multivariate linear regression
absence or presence of anaemia are also shown in Table 1. model, adjusting for patient age, gender, BMI, history of
Patients with anaemia had borderline significantly higher myocardial infarction, pulmonary disease, use of diuret-
plasma BNP levels than those without anaemia. ics, ACE (angiotensin-converting enzyme) inhibitors and
Logarithmically transformed BNP concentrations cor- β-blockers, estimated creatinine clearance, triple-vessel
related significantly both with LVEF (r = − 0.33, P < disease, LVEF and LVEDP, blood haemoglobin remained
0.0001; n = 234) and LVEDP (r = 0.39, P < 0.0001; n = an independent predictor of plasma BNP (standardized
C 2005 The Biochemical Society72 C. Wold Knudsen, H. Vik-Mo and T. Omland
Table 3 Predictors of blood haemoglobin using a multi-
variable model
Variable Standardized β-coefficient P value
Male gender − 0.449 0.000
Age − 0.047 0.597
BMI 0.048 0.514
Previous myocardial infarction 0.07 0.921
Pulmonary disease 0.027 0.642
Diuretic use 0.036 0.591
ACE inhibitors − 0.063 0.322
β-Blockers 0.038 0.527
Creatinine clearance − 0.071 0.488
Triple-vessel disease 0.028 0.656
LVEDP 0.100 0.125
LVEF − 0.105 0.121
Log BNP − 0.355 0.000
without heart failure. The association remained signifi-
Figure 1 Scatter plot of the relationship between blood cant after adjustment for a number of cardiac and non-
haemoglobin and logarithmically transformed values of cardiac determinants of BNP levels, including indices
plasma BNP of systolic (LVEF) and late diastolic (LVEDP) function,
extent of coronary artery disease (triple-vessel disease),
Table 2 Predictors of plasma BNP using a multivariable
demographic factors (age and gender), historical factors
model
(prior myocardial infarction, use of diuretics, ACE
Variable Standardized β-coefficient P value inhibitors and β-blockers) and renal function (estimated
creatinine clearance).
Female gender − 0.018 0.774 Following the recent development of rapid fully
Age 0.259 0.000 automated assays, BNP measurement has been widely
BMI − 0.079 0.206 adopted for the diagnosis of heart failure. However,
Previous myocardial infarction 0.159 0.004 BNP elevation is not specific for heart failure, but is
Pulmonary disease − 0.028 0.568 associated with a variety of factors, including advanced
Diuretic use − 0.027 0.632 patient age and female gender [14,15], decreased BMI
ACE inhibitors 0.073 0.171 [17], decreased renal function [16] and increased left
β-Blockers 0.135 0.007 ventricular mass [4]. The present findings suggest that the
Creatinine clearance − 0.014 0.872 presence of anaemia is another important confounder of
Triple-vessel disease 0.120 0.021 the relationship between BNP levels and cardiac function
LVEDP 0.309 0.000 and prognosis. Blood haemoglobin appeared to be a
LVEF − 0.210 0.000 stronger determinant of BNP levels than factors such
Haemoglobin − 0.253 0.000 as BMI and renal function, and the association was of
comparable strength with that between BNP and LVEDP
and LVEF, factors traditionally considered to be major
β-coefficient = − 0.253, P < 0.0001; Table 2). These vari-
determinants of BNP production.
ables explained 50 % of the variability of BNP (adjusted
In heart failure, BNP elevation has been associated
R2 = 0.497). Similar results were obtained for haematocrit
previously with anaemia and the severity of disease. In
(standardized β-coefficient = − 0.215, P < 0.0001). Pre-
a recent study of 74 patients with chronic heart failure,
dictors of haemoglobin levels are presented in Table 3.
haemoglobin and erythropoietin levels were associated
These variables explained 30 % of the variability of
with the severity of heart failure, BNP levels and pro-
haemoglobin (adjusted R2 = 0.296).
gnosis, and in a multivariable model BNP did not provide
independent prognostic information after adjustment for
DISCUSSION haemoglobin and erythropoietin [20]. In another study
of 137 patients with heart failure and a normal ejection
The new important finding of the present study is that fraction, anaemia was associated with greater elevation of
blood haemoglobin (and haematocrit) is an indepen- BNP, the severity of diastolic dysfunction and prognosis
dent predictor of circulating levels of BNP in subjects [21]. In heart failure, the classic assumption is that
C 2005 The Biochemical SocietyB-type natriuretic peptide and anaemia 73
plasma volume is expanded and can be monitored by BNP, cardiac function and prognosis, and should be
assessing degree of oedema [23]. On the other hand, adjusted for in future studies of the diagnostic and
in heart failure patients treated with diuretics, plasma prognostic value of BNP.
volume may be decreased [24]. Accordingly, the haemo-
globin concentration in heart failure patients may differ ACKNOWLEDGMENTS
considerably depending on volume state (pseudo-
anaemia secondary to haemodilution, increased haemo- C. W. K. is a recipient of a grant from the Research Found-
globin concentration due to diuretic-induced hypo- ation of Health and Rehabilitation in Norway. We are
volaemia, or true erythrocyte depletion). indebted to Dr Timothy G. Yandle in the Christchurch
In the present study, we found an independent asso- Cardioendocrine Research Group, Christchurch, New
ciation between haemoglobin concentration and BNP Zealand, for performing the BNP analyses.
levels in patients without a history of heart failure. The
exact mechanism cannot be deduced from the present REFERENCES
data. Our data do not suggest that variability of BMI,
diuretic use, pulmonary disease or renal dysfunction can 1 de Lemos, J. A., McGuire, D. K. and Drazner, M. H. (2003)
explain this association. It is well known that patients with B-type natriuretic peptide in cardiovascular disease. Lancet
362, 316–322
severe chronic anaemia often retain salt and water [25]. 2 Ruskoaho, H. (2003) Cardiac hormones as diagnostic tools
Potential mechanisms include reduction of renal blood in heart failure. Endocr. Rev. 24, 341–356
3 Omland, T., Aakvaag, A. and Vik-Mo, H. (1996) Plasma
flow and glomerular filtration rate and neurohormonal cardiac natriuretic peptide determination as a screening test
activation. However, unlike patients with myocardial dis- for the detection of patients with mild left ventricular
ease, patients with anaemia have increased cardiac output impairment. Heart 76, 232–237
4 Yamamoto, K., Burnett, Jr, J. C., Jougasaki, M. et al. (1996)
and low systemic vascular resistance [25]. It is conceivable Superiority of brain natriuretic peptide as a hormonal
that the natriuretic peptide system is activated to counter- marker of ventricular systolic and diastolic dysfunction
and ventricular hypertrophy. Hypertension 28, 988–994
act the haemodynamic and renal effects of vasocon- 5 Maisel, A. S., Krishnaswamy, P., Nowak, R. M. et al. (2002)
strictor neurohormones that may occur even in mild Rapid measurement of B-type natriuretic peptide in the
forms of anaemia [26]. Moreover, many of these vaso- emergency diagnosis of heart failure. N. Engl. J. Med. 347,
161–167
constrictor neurohormones are powerful stimuli for 6 Omland, T., Aakvaag, A., Bonarjee, V. V. et al. (1996)
BNP production [2]. To elucidate the association be- Plasma brain natriuretic peptide as an indicator of left
ventricular systolic function and long-term prognosis after
tween BNP and haemoglobin further, investigations acute myocardial infarction. Comparison with plasma
concerning the acute effects of blood transfusion and atrial natriuretic peptide and N-terminal proatrial
natriuretic peptide. Circulation 93, 1963–1969
the chronic effect of iron or erythropoietin treatment 7 de Lemos, J. A., Morrow, D. A., Bentley, J. H. et al. (2001)
on circulating levels of BNP and vasoconstrictor neuro- The prognostic value of B-type natriuretic peptide in
hormones, including noradrenaline, angiotensin II and patients with acute coronary syndromes. N. Engl. J. Med.
345, 1014–1021
endothelin, may be required. 8 Richards, A. M., Nicholls, M. G., Espiner, E. A. et al.
The limitations of our present study include the gen- (2003) B-type natriuretic peptides and ejection fraction for
prognosis after myocardial infarction. Circulation 107,
eralizability of our results. The majority of our patients 2786–2792
had coronary artery disease and were using antianginal 9 Sabatine, M. S., Morrow, D. A., de Lemos, J. A. et al.
medication. We therefore cannot automatically extra- (2002) Multimarker approach to risk stratification in
non-ST elevation acute coronary syndromes:
polate the results to healthy individuals. However, our simultaneous assessment of troponin I, C-reactive
observation that the association between haemoglobin protein, and B-type natriuretic peptide. Circulation 105,
1760–1763
and BNP tended to be stronger in subjects without sig- 10 Omland, T., Richards, A. M., Wergeland, R. and
nificant coronary artery disease than in those with signifi- Vik-Mo, H. (2005) B-type natriuretic peptide
and long-term survival in patients with stable coronary
cant disease suggests that a similar relationship exists in artery disease. Am. J. Cardiol. 95, 24–28
healthy individuals. Nevertheless, our results need to be 11 Tsutamoto, T., Wada, A., Maeda, K. et al. (1997)
confirmed in larger populations of healthy subjects. Attenuation of compensation of endogenous cardiac
natriuretic peptide system in chronic heart failure:
Although the association between BNP and haemo- prognostic role of plasma brain natriuretic peptide
globin was statistically significant and of the same order concentration in patients with chronic symptomatic
left ventricular dysfunction. Circulation 96, 509–516
of magnitude as the associations between BNP and LVEF 12 Anand, I. S., Fisher, L. D., Chiang, Y. T. et al. (2003)
and BNP and LVEDP, the variability in BNP explained Changes in brain natriuretic peptide and norepinephrine
by the variability of haemoglobin was modest. It should over time and mortality and morbidity in the Valsartan
Heart Failure Trial (Val-HeFT). Circulation 107,
be emphasized therefore that haemoglobin is only one 1278–1283
out of many determinants of circulating BNP levels. 13 Wang, T. J., Larson, M. G., Levy, D. et al. (2004) Plasma
natriuretic peptide levels and the risk of cardiovascular
In conclusion, blood haemoglobin levels are inde- events and death. N. Engl. J. Med. 350, 655–663
pendently associated with plasma BNP levels in subjects 14 Redfield, M. M., Rodeheffer, R. J., Jacobsen, S. J.,
Mahoney, D. W., Bailey, K. R. and Burnett, Jr, J. C. (2002)
without heart failure. Haemoglobin appears to be a strong Plasma brain natriuretic peptide concentration: impact of
and important confounder of the relationship between age and gender. J. Am. Coll. Cardiol. 40, 976–982
C 2005 The Biochemical Society74 C. Wold Knudsen, H. Vik-Mo and T. Omland
15 Wang, T. J., Larson, M. G., Levy, D. et al. (2002) Impact of 21 Brucks, S., Little, W. C., Chao, T. et al. (2004) Relation of
age and sex on plasma natriuretic peptide levels in healthy anaemia to diastolic heart failure and the effect of outcome.
adults. Am. J. Cardiol. 90, 254–258 Am. J. Cardiol. 93, 1055–1057
16 McCullough, P. A., Duc, P., Omland, T. et al. (2003) B-type 22 Yandle, T. G., Richards, A. M., Gilbert, A., Fisher, S.,
natriuretic peptide and renal function in the diagnosis of Holmes, S. and Espiner, E. A. (1993) Assay of brain
heart failure: an analysis from the Breathing Not Properly natriuretic peptide (BNP) in human plasma: evidence
Study. Am. J. Kidney Dis. 41, 571–579 for high molecular weight BNP as a major plasma
17 Wang, T. J., Larson, M. G., Levy, D. et al. (2004) Impact of component in heart failure. J. Clin. Endocrinol. Metab. 76,
obesity on plasma natriuretic peptide levels. Circulation 832–838
109, 594–600 23 Kalra, P. R., Anagnostopoulos, C., Bolger, A. P., Coats,
18 Anand, I., McMurray, J. J., Whitmore, J. et al. (2004) A. J. and Anker, S. D. (2002) The regulation and
Anaemia and its relationship to clinical outcome in heart measurement of plasma volume in heart failure.
failure. Circulation 110, 149–154 J. Am. Coll. Cardiol. 39, 1901–1908
19 Horwich, T. B., Fonarow, G. C., Hamilton, M. A., 24 Feigenbaum, M. S., Welsch, M. A., Mitchell, M.,
MacLellan, W. R. and Borenstein, J. (2002) Anemia is Vincent, K., Braith, R. W. and Pepine, C. J. (2000)
associated with worse symptoms, greater impairment Contracted plasma and blood volume in chronic heart
in functional capacity and a significant increase in failure. J. Am. Coll. Cardiol. 35, 51–55
mortality in patients with advanced heart failure. 25 Anand, I. S., Chandrashekar, Y., Ferrari, R., Poole-Wilson,
J. Am. Coll. Cardiol. 39, 178–186 P. A. and Harris, P. C. (1993) Pathogenesis of oedema in
20 van der Meer, P., Voors, A. A., Lipsic, E., Smilde, T. D., chronic severe anaemia: studies of body water, sodium,
van Gilst, W. H. and van Veldhuisen, D. J. (2004) renal function, hemodynamic variables, and plasma
Prognostic value of plasma erythropoietin on mortality in hormones. Heart 70, 357–362
patients with chronic heart failure. J. Am. Coll. Cardiol. 44, 26 Isbister, J. P. (1997) Physiology and pathophysiology of
63–67 blood volume regulation. Transfus. Sci. 18, 409–423
Received 10 December 2004/9 February 2005; accepted 8 March 2005
Published as Immediate Publication 8 March 2005, DOI 10.1042/CS20040349
C 2005 The Biochemical SocietyYou can also read