Best Practice Statement - Compression hosiery: A patient-centric approach WUK BPS - Medi.de
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

WUK BPS
Best Practice Statement
Compression hosiery:
A patient-centric approach
2021
THIRD EDITION
Understanding medical
compression hosiery
construction
Individualised
hosiery selection
Shared decision-making
BEST PRACTICE STATEMENT: EXPERT WORKING GROUP:
COMPRESSION HOSIERY: Jacqui Fletcher OBE (Chair), Independent Nurse Consultant
A PATIENT-CENTRIC
APPROACH Leanne Atkin, Vascular Nurse Consultant, Mid Yorkshire
(3RD EDITION) NHS Trust; Lecturer, University of Huddersfield
Louise Bolton, Tissue Viability Lead Nurse, Anglian
PUBLISHED BY: Community Enterprise CIC
Wounds UK
A division of Alan Elstone, Vascular Nurse Specialist, Derriford Hospital,
Omniamed Communications Plymouth/Advanced Clinical Practitioner, University Hospitals
108 Cannon Street, Plymouth NHS Trust
London EC4N 6EU, UK
Tel: +44 (0)20 3735 8244 Patryk Gawrysiak, Specialist Physiotherapist in
www.wounds-uk.com Lymphoedema, St. George’s Hospital, London
Caitriona O’Neill, Director of Clinical Services & Clinical
Lead for Lymphoedema, Accelerate CIC
Georgina Ritchie, Deputy Director of Education, Accelerate
© Wounds UK, June 2021 CIC
This document has been developed REVIEW PANEL:
by Wounds UK and is supported by Philip Stather, Consultant Vascular Surgeon, Norfolk and
an educational grant from Norwich University Hospitals, NHS Foundation Trust
medi UK.
Peter Vowden, Honorary Consultant Vascular Surgeon,
Bradford Teaching Hospitals NHS Foundation Trust; Visiting
Honorary Professor, Wound Healing Research, University of
Bradford
Alison Hopkins MBE, Chief Executive, Accelerate CIC
The views expressed are those of the Document summary
Expert Working Group and Review
Panel and do not necessarily reflect ■ Medical compression is an effective and powerful therapy.
those of medi UK. ■ Compression hosiery has evolved considerably over the
last few years and is now a progressive therapy that exists
How to cite this document:
Wounds UK (2021) Best Practice beyond Compression Class I and Class II British Standard
Statement: Compression hosiery: A hosiery.
patient-centric approach (3rd edn).
Wounds UK, London. Available to ■ It is important to be familiar with the National Wound Care
download from: Strategy Programme (2020) guidelines and follow the
www.wounds-uk.com recommendations in practice.
■ It is important to be familiar with the types of compression
therapy used in clinical practice, the conditions that can be
treated, and the garments available on local formulary.
■ It should be possible to find compression therapy for
everyone with a thorough holistic assessment and taking
into account individual patient preferences.
■ Effective communication and shared decision-making
between the clinician and the patient and/or caregiver are
key to identifying the ‘best’ hosiery for the patient and to
ensuring concordance with care. Listen and understand
their concerns, expectations and motivations with regard to
their presenting condition(s). Avoid using terms the patient
may not understand.
Foreword
The third edition of the Best Practice The document is designed to be simple
Statement on Compression Hosiery focuses and user-friendly, and to put the patient
on improving the patient experience of at the centre of assessing for, selecting,
medical compression hosiery for the lower prescribing and delivering care with medical
leg, which include socks and stockings, by compression hosiery.
understanding the patient’s perspective and
fostering a patient–practitioner partnership Jacqui Fletcher OBE, Chair
for supported self-management.
It is often easy to label a patient ‘uncooperative’ Glossary Progress since the
or ‘non-concordant’ if the outcomes of (page 2) second edition
(page 4)
treatment are not as anticipated. However,
it is unlikely that any patient is truly non-
concordant, rather, they have not yet received
the right treatment, education, support and
follow-up for their individual needs. Clinicians Chapter 1: Principles of assessment (page 5)
should employ a positive, confident, competent - Factors that influence medical compression
and knowledgeable attitude when discussing hosiery selection
medical compression therapy with patients,
which may help to influence the patient to
become interested and engaged with their Chapter 2: Medical compression hosiery
treatment. construction explained (page 7)
- The role stiffness plays in compression hosiery
The COVID-19 pandemic has accelerated garments
initiatives towards greater patient and carer - Myths and truths surrounding round-knit
versus flat-knit hosiery
supported self-management (NHS England
and NHS Improvement, 2020). Consultations
have increasingly been undertaken by
telephone and video call, and patients have Chapter 3: Patient considerations during medi-
cal compression hosiery selection (page 10)
been able to text or send photos directly to
- Clinical and patient-related factors that
their clinician. Evidence shows that when impact on hosiery selection
people are supported in self-management,
they benefit from better health outcomes,
improved experiences of care and fewer
unplanned care admissions (NHS England Chapter 4: Encouraging shared
and NHS Improvement, 2020). A growing decision-making (page 13)
number of people with wounds are willing - Practical guidance on partnership working and
to participate in supported self-management concordance alongside the patient
if they are given the right support and tools
(Adderley, 2020).
Chapter 5: Measuring and sizing (page 15)
An Expert Wound Group met online to
- Myths and truths surrounding off-the-shelf
discuss the advances in medical compression and made-to-measure hosiery
hosiery since the second edition of the Best - FAQs on fitting medical compression hosiery
Practice Statement: Compression Hosiery
(Wounds UK, 2015) and to agree on Best
Practice Statements to guide compression
hosiery selection for patients. Best Practice Chapter 6: Key elements of supported
Statements are accompanied by Patient self-management: Hosiery application, removal
and care and skin care (page 17)
Expectations to encourage shared decision-
- Quick guide for good medical compression
making and foster a supportive patient– hosiery fit
practitioner partnership at every stage of care.
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 1
Glossary
Ankle–brachial pressure index (ABPI): A management of lower limb lymphoedema
screening tool to determine the presence and and oedema. Hosiery can also be used
extent of peripheral arterial disease (PAD). The to manage conditions associated with
result of the ABPI rules out PAD, but it does CVI (NICE, 2012). Medical compression
not confirm whether a patient will benefit from hosiery options vary in stiffness, levels of
compression therapy – meaning that an ABPI compression delivered, fabric, colour, size,
cannot diagnose venous insufficiency or the length, and whether they are closed or open-
cause of oedema. toe. Medical compression hosiery is a single
garment and can be selected off-the-shelf or
Chronic venous insufficiency (CVI): A made-to-measure for the patient.
condition whereby blood pools in the veins,
straining the walls of the vein and making Compression hosiery kits: A type of
it difficult for blood to return to the heart medical compression therapy most
from the legs. It can be caused by venous commonly used for the management and
hypertension or venous obstruction/occlusion, healing of venous leg ulceration. Kits consist
such as a deep vein thrombosis. of two medical compression garments
designed to be worn one on top of the
Compression: A treatment whereby the other. Hosiery kits are designed to be worn
application of external pressure counteracts 24 hours a day but the outer layer can
the loss of capillary fluid by squeezing fluid be removed at night, although this is not
into the veins and lymph vessels. Compression essential. Hosiery kits are most commonly
therapy improves venous return to the heart available in off-the-shelf sizes but can also be
and initiates a variety of complex physiological made-to-measure.
and biochemical effects involving the venous,
arterial and lymphatic systems. The effects Compression standards: National
of compression can be dramatic, reducing and international standards for medical
oedema and pain while promoting healing of compression hosiery have been developed to
ulcers caused by venous insufficiency (Harding ensure compression stockings and socks meet
et al, 2015). certain technical parameters, such as testing
methods, yarn specification and durability
Compression bandages: A type of (Lymphoedema Framework, 2006). There are
medical compression garment that is a variety of quality standards against which
composed of either inelastic (short-stretch) compression hosiery can be categorised:
elements, elastic (long-stretch) elements ■ British Standard Compression (Specifica-
or a combination of both. Bandaging is tion 40; BS 661210): The British Standard for
most often used to treat active venous compression hosiery has three classes that
ulceration and should be worn 24 hours a indicate the level of compression provided by
day. Bandaging can also be used for ongoing the garment. BS40 measures the compression
maintenance, for those unable to tolerate delivered by the medical compression gar-
hosiery or those with complex conditions ment at the ankle, knee and top of thigh and
such as lymphoedema, especially when the has a 3-month guarantee (Partsch, 2003).
legs are large and have skin folds. For these ■ German RAL (GZ 387/1) Standard: The Ger-
patients, full-leg bandaging may be required man standard is measured at 5cm increments
to control oedema and maintain the shape of up the garment to ensure graduation and has
the leg (Anderson and Smith, 2004). a 6-month guarantee (Földi and Földi, 1983).
■ French Standard (ASQUAL) (AFNOR NF
Compression classes: The pressure measured 30.102A): The French Standard is measured at
at the ankle is used to classify medical the ankle (Levick, 2003).
compression hosiery into compression classes
(e.g. 1, 2, 3). The stiffness of the compression Compression wraps: A type of medical
hosiery material affects the compression class. compression garment considered for the
management of lymphoedema and other
Compression hosiery: The most widely disorders of the circulatory system. Available
used form of compression in the long-term in a variety of forms, these devices consist
2 BEST PRACTICE STATEMENT: COMPRESSION HOSIERY
GLOSSARY
of fabric sheets made from one or more cellulitis, fluid leakage and ulceration (Bianchi
components with limited extensibility. The et al, 2012; Harding et al, 2015). Chronic
wraps are applied to affected limbs and oedema can be considered a surrogate marker
held in place with hook and loop fastenings for lymphoedema.
(Thomas, 2017).
Static Stiffness Index (SSI): The difference
Interface pressure: The pressure between between standing and resting pressure
the skin and the compression garment. characterises the efficacy of a specific
Measuring pressure at the interface during compression garment to narrow the venous
both lying and standing indicates how the lumen and encourage venous return (Partsch
compression garment reacts to muscular et al, 2016). The Dynamic Stiffness Index (DSI)
activity. The interface pressure was is the change in the pressure between the
previously described as the sub-bandage limb and garment (interface pressure) when
pressure. a person activates their calf muscle through
movement, such as walking or exercise. The
Lymphoedema: The accumulation of DSI demonstrates the garment’s ability to resist
fluid in the tissue spaces. It may present calf muscle expansion and to generate working
as swelling of one or more limbs and may pressure increases. The higher the SSI and DSI,
include the corresponding quadrant of the stiffer the garment.
the trunk and other areas, e.g. head, neck,
breast or genitalia. It arises from congenital Stiffness: A measure of flexibility and the
malformation of the lymphatic system ability of the bandage or hosiery to oppose
(primary lymphoedema), or damage to the muscle expansion during contraction
lymphatic vessels and/or lymph nodes (Mosti, 2012). The yarn used and the technique
(secondary lymphoedema) due to cancer employed to knit the fabric will impact the
treatment, infection, inflammation, stiffness of the fabric. The less stiff the material,
venous diseases, obesity, trauma and the lower the pressure peaks during exercise.
injury (Lymphoedema Framework, 2006). Inelastic bandage and multi-layer bandage
Lymphoedema is a progressive disease of systems generally have a higher SSI when
four stages: latency stage (stage 0), mild stage compared to compression hosiery (Vowden et
(stage 1), moderate stage (stage 2) and severe al, 2020).
stage (stage 3) (International Society of
Lymphoedema, 2016).
Oedema: Swelling caused by the accumulation
of fluid in the extra-vascular tissue. Oedema
usually affects the feet, ankles and legs,
although it can occur anywhere in the body.
The cause of oedema should be identified
before beginning treatment. Bilateral oedema
is indicative of systemic conditions such as
cardiac failure, protein reduction and venous
insufficiency, standing or sitting in the same
position for too long, eating a large amount of
salty foods, being overweight, being pregnant,
malignancy or taking certain medicines.
Unilateral oedema is more often due to local
causes, such as deep vein thrombosis or
cellulitis.
Chronic lower limb oedema is a persistent,
abnormal swelling of the leg. Chronic oedema
has an ongoing effect on the viability of the skin
leading to complications, such as infection,
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 3
PROGRESS SINCE THE SECOND EDITION
Clinicians should stay Since 2015 and the second edition of the Increasing range of medical
updated with evidence Best Practice Statement there have been compression hosiery
and guidelines on the use the following areas of progress in medical Compression hosiery has evolved
of medical compression compression therapy. considerably over the last few years and is
therapy. Clinicians now a progressive therapy that goes beyond
should be familiar with National Wound Care Strategy Class I and Class II British Standard hosiery.
the different types of Programme guidance There is now a greater variety of medical
compression systems In England, the National Wound Care compression hosiery available in terms of
and know when and how Strategy Programme (NWCSP, 2020) style, which increases the expectations of
to access and use them.
has produced recommendations for the what can be achieved for patients. However,
Failure to provide a patient
with appropriate care
immediate and necessary care of patients variations in styles can lead to inconsistency
should be seen as a harm. who have one or more wounds below in the way medical compression garments
the knee. The recommendations include are selected and prescribed (NICE, 2012).
guidance on wound and skin cleansing, Patients may attend appointments having
application of a simple low-adherent already looked at the options online, but
Best Practice dressing and the use of mild graduated it is important to remember that not all
Statement compression for leg wounds if there are
no red flags to contraindicate compression
medical compression hosiery are available
on every Trust’s formulary. Therefore,
(Box 1). clinicians should be familiar with the
garments that they have available in order
Medical compression Medical compression is a powerful, to select the most appropriate garment for
is an active therapy and active therapy that is part of the toolkit the patient.
will help to reduce your for the management of chronic oedema,
symptoms. You should lymphoedema and venous insufficiency. NHS Long-Term Plan
expect your clinician to be In the absence of red flags (Box 1), mild The NHS Long-Term Plan (2019) is a
confident, competent and compression (around 20mmHg at the commitment to facilitating measurable
enthusiastic about medical
ankle) should be considered the first-line improvements in population health and
compression. They should
be familiar with different
initial treatment for people who have one to reduce health inequalities. In wound
types of compression or more wounds below the knee and not on care, the NWCSP (2020) recommends
(e.g. compression hosiery, the foot (NWCSP, 2020). The patient should greater awareness of the importance
stockings, bandages and receive a full holistic assessment if clinically of early intervention of compression
wraps), so that they can required or if there is evidence of venous therapy or endovenous intervention. This
offer treatments that and/or lymphatic disease, with a view to is to be achieved through greater public
suit you. increasing the level of compression within awareness (e.g. public-facing campaigns
14 days. This is clear national guidance that such as Legs Matter https://legsmatter.org)
Patient healthcare professionals should encourage
compression uptake among patients; failure
and community, primary care, vascular,
tissue viability and lymphoedema services
expectation to provide a patient with appropriate care promoting the same prevention and early
may be seen as a harm. intervention messages.
Box 1. National Wound Care Strategy Programme (2020) guidance for people with
leg and foot wounds
If red flags are present:
People with leg and foot wounds should not be
■ Treat suspected infection in line with
treated with compression if they have any of the
following red flags: NICE (2020) antimicrobial guidelines
■ Immediately escalate to relevant
• Acute infection of leg or foot (e.g. increasing clinical specialist
unilateral redness, swelling, pain, pus, heat) ■ For people in the last few weeks of life,
• Symptoms of sepsis seek input from their other clinicians
• Acute or chronic limb-threatening ischaemia to agree an appropriate care plan.
• Suspected acute deep vein thrombosis
• Suspected skin cancer.
4 BEST PRACTICE STATEMENT: COMPRESSION HOSIERY
CHAPTER 1: PRINCIPLES OF ASSESSMENT
Selecting the correct Medical compression hosiery is the most Holistic assessment
medical compression widely used form of compression in the long- A detailed history should include past
hosiery should be based term management for a number of condi- medical and surgical history, family history
on a thorough assessment tions, including lower limb lymphoedema and history of limb or skin trauma. Current
of the patient’s presenting and oedema, and conditions associated with medications (e.g. ACE inhibitors, inmmuno-
symptoms and knowledge chronic venous insufficiency (CVI: NICE, suppressants, steroids), concurrent illnesses
of how the products work. 2012). Venous disease can be categorised us- and the patient’s limb, circulation and skin
ing the CEAP classification (Lurie et al, 2020; should also be assessed to identify the cause
Table 3, page 12) to differentiate between of venous insufficiency or chronic oedema
Best Practice mild (thread veins or telangiectasia) and and underlying disease process (Lymphoe-
Statement severe (chronic skin changes/ skin discoloura- dema Framework, 2006).
tion/ulceration). Untreated CVI can also lead
to oedema formation. There are many causes The NWCSP (2020) offers guidance on the
of chronic oedema, but they largely fall into key elements of assessment that will guide
Assessment for medical
four main categories: first-line intervention and provides red flags
compression should
■ Lymphoedema (both primary and sec- for when compression therapy should not be
include full assessment
of your limb, other ondary) initiated (Box 1, page 4).
conditions, home life, ■ Lipoedema
personal preferences, your ■ Dependency oedema Vascular assessment
willingness to be involved ■ Lymphovenous or phlebolymphoedema The ankle–brachial pressure index (ABPI)
in care, and your ability to (Green and Mason, 2006). result along with the patient’s history and
apply and remove medical other elements of the assessment process can
compression hosiery. Many of the signs and symptoms of chronic be used to rule out the presence of significant
oedema — including dermatitis, distortion peripheral arterial disease (PAD). There is a
of limb shape, episodes of cellulitis, develop- common misconception that garment selec-
Patient ment of hyperkeratosis, non-pitting when tion relies solely on the compression class or
expectation pressure is applied and hyper-pigmentation
of the skin — may be indicative of these
mmHg and the result of the ABPI.
potential venous or lymphatic conditions.
Therefore, it may be difficult to differenti-
ate between venous and lymphatic diseases,
highlighting that a full, holistic assessment is
MYTH
required for patients with chronic oedema The ABPI result will indicate the
(Wounds UK, 2015). compression class or level that the patient
requires..
An accurate assessment of the patient, their
preferences, the severity of the disease pro-
gression, and any complications or comorbid
conditions will inform the treatment pathway
TRUTH
and compression garment selection. If gar- Compression up to 20mmHg can be
ments are to be used safely, all patients need applied in the absence of red flags
to be able to report concerns they have with without any form of arterial assessment
P
their medical compression hosiery; this is (NWCSP, 2020). An ABPI assessment
is recommended before commencing
especially important where there is neuropa-
compression therapy greater than
thy or cognitive impairment. The provision 20mmHg. The role of the ABPI
of compression hosiery relies on the patient’s assessment is to screen patients to rule
protective sensation and their ability to rec- out PAD. Compression selection should
ognise problems; where this may be an issue, be based on the clinical assessment,
more regular review of the patient may be patient expectations and aim of
required. compression therapy in combination
with the ABPI result.
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 5
1. PRINCIPLES OF ASSESSMENT
Instead, the results of the ABPI may influence The BLS (2019) Position Document offers
compression selection, and, it is important to further guidance on how to assess limbs in the
remember that, in the presence of significant presence of oedema.
PAD, compression therapy can be dangerous
and should only be used at the recommenda- Treatment plan
tion of a vascular specialist. For more infor- Results from the mediven® observational study
mation on the role of ABPI, see Best Practice found that patients’ individual factors were
Statement: Ankle–brachial pressure index rarely taken into account when prescribing
(ABPI) in practice (Wounds UK, 2019a). medical compression garments (Schwahn-
Schreiber et al, 2016). Just as medication
If an ABPI cannot be obtained, for instance, dosage is prescribed according to the needs
the patient is unable to lie flat, or has oedema- and characteristics of the individual, selection
tous legs, pain, fragile skin or calcified vessels, of compression therapy should be based on
the arterial supply needs to be assessed in careful assessment of the patient’s individual
other ways, for example toe pressure, pulse needs and condition identified in the holistic
auscultation and pulse palpation. If it is not assessment, taking into consideration patient
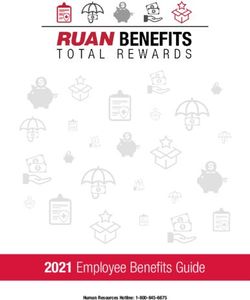
possible to obtain an ABPI initially due to choice (Figure 1).
oedema, then it may be helpful to apply
compression therapy at 20mmHg to manage
the oedema and attempt to obtain an ABPI the
following week.
Arterial
assessment
e.g. ABPI, toe
pressure, pulse
palpation
Holistic Patient
assessment choice
identifies level of Medical compression e.g. style, colour,
compression needed hosiery selection ability and willingness
to treat underlying to self-manage
cause/symptoms
Individual
patient factors
identified
during holistic
assessment, e.g. BMI,
mobility,
limb shape
Figure 1. Factors that influence medical compression hosiery selection.
6 BEST PRACTICE STATEMENT: COMPRESSION HOSIERY
CHAPTER 2: MEDICAL COMPRESSION HOSIERY
CONSTRUCTION
Medical compression hosiery must be se- Elasticity and stiffness –
Practitioners should lected based on the outcomes of the holistic How compression works
understand the range assessment, patient preferences and the goals Inelastic compression systems generally
of medical compression
of treatment. Product selection should also have a higher Static Stiffness Index (SSI)
hosiery garments available
and understand how
take into account limb size and shape, skin compared to elastic compression systems.
the construction of the condition, allergies and sensitivities, patient Stiffer compression systems have higher
garment affects clinical considerations (e.g. dexterity, psychosocial working pressure peaks and can be more
efficacy. issues) and the garment itself. comfortable than more elastic garments
with a lower SSI as they support the leg
Construction of compression hosiery and provide ‘strong wall stability’.
Best Practice The type of yarns and knitting techniques
Statement used to manufacture medical compression
hosiery affects the stiffness or elasticity of the
Conversely, the leg muscles contract and
change shape during walking and exer-
garment. The material used to make compres- cising, so compression garments have to
sion garments is produced by knitting two provide some elasticity to allow this move-
Using language you
understand, the clinician types of yarn together: ment while still supporting calf action and
should be able to explain to ■ Inlay yarn – produces the compression counteracting the gravitational effect of
you the different medical ■ Body yarn – delivers the thickness and standing.
compression hosiery stiffness of the knitted fabric (Clark and
garments available and help
to find the best garment to
suit your individual needs.
Krimmel, 2006).
MYTH
The arrangement of the inlay and body yarn
will produce either flat-knit or round-knit Stiffer medical compression hosiery is
Patient fabric, which impacts on the material’s prop-
erties and indications for use (Table 1, page 8).
sometimes perceived as uncomfortable.
expectation
TRUTH
Flat-knit fabric tends to be relatively thick,
stiff and inelastic, which lets it lie across skin
folds without cutting into the skin. Flat-knit is
usually used for ‘made-to measure’ garments Stiff or inelastic medical compression
because it can be more readily adapted to hosiery provides higher working pressure
peaks while the patient is walking or
limb shape distortion. ‘Off-the-shelf’ medical
exercising but is comfortable at rest.
compression hosiery is available in standard
sizes and tends to be manufactured from
round-knit fabric. Compression standards
Medical compression hosiery is a medical
device, so it is measured against set cri-
MYTH teria to describe the support or compres-
sion applied to the lower leg. Standards
provide confidence about the quality and
Flat-knit medical compression hosiery should life span of a product. It is important to
be used as a ‘last resort’ for patients as they
know how long a product is able to give
are difficult to measure patients for and
mistakes are expensive and wasteful. therapeutic levels of compression to avoid
putting patients at risk of sub-standard
care (Lymphoedema Framework, 2006).
TRUTH For medical compression hosiery, there
are three internationally recognised qual-
ity compression standards – British Stan-
Flat-knit medical compression hosiery dard, German RAL Standard and French
often requires a few more measurements,
Standard (Table 2, page 9).
but, for patients with chronic oedema/
lymphoedema, it is the optimal therapy
and should be considered once the initial There is no independent quality European
reducible oedema has been decreased. standard, but the German RAL Standard is
widely accepted as the basic requirement
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 7
2. MEDICAL COMPRESSION HOSIERY
Table 1. Features of round-knit and flat-knit medical compression hosiery
Feature Round-knit compression hosiery Flat-knit compression hosiery
Seam Seamless With seam
Manufacturing
Knit Knitted on a round cylinder Knitted in flat rows
Stitches per row Constant Variable
Shape Shaped by variable mesh size and pretension of the inlaid Shaped by variable number of stitches with the elastic thread
elastic thread laid in
Stretch High Low
Thread structure
Elastic thread Not covered Covered
Working pressure Low High
Effect Effect on veins to improve venous return Primary effect is to increase tissue pressure
Secondary effect is on the veins to improve venous return
Measurement When measuring the patient’s limb, measure the surface When measuring the patient’s limb, there is a degree of
circumferences interpretation required as the garment is designed to sculpt the
limb rather than necessarily match the size and shape presented
Uses Generally used for off-the-shelf hosiery, although it can be used Commonly used for made-to-measure hosiery
for made-to-measure hosiery
Indications Typically for patients who have venous insufficiency or mild Typically for patients who have chronic oedema/lymphoedema
lymphoedema due to the action on the limb, and its ability to be knitted to fit
any limb shape
Most suitable where there is no or minimal limb distortion due
to oedema (Anderson and Smith, 2014) If round-knit is causing problems for the patient, consider flat-
knit, which can be more comfortable and easier to apply
Images used with permission of medi UK©.
8 BEST PRACTICE STATEMENT: COMPRESSION HOSIERY2. MEDICAL COMPRESSION HOSIERY
for certifying medical compression stock- when selecting medical compression
ings (BSI Standards Publication, 2018). hosiery, more emphasis should be given to
Clinicians should check that the medical the compression dosage (mmHg) required
compression hosiery they are using has for the patient’s individual needs rather
a quality standard as this will guarantee than the compression class of the garment.
the stocking offers the correct ‘dosage’
of mmHg and that it delivers consistent
graduation of pressure levels, i.e. higher
at the ankle, and reducing throughout the
length of the stocking.
MYTH
When choosing a medical compression
Compression class garment, the compression class and
The elasticity and stiffness of the textile compression dosage (mmHg) are the most
has a great impact on the haemodynamic important aspect to consider.
efficacy of a garment (Bjork and Ehmann,
2019). The stiffness of the compression ho-
siery material affects the compression lev- TRUTH
els exerted by different types and classes of
hosiery. The compression measured at the In most clinical situations, it is important
ankle is used to classify the hosiery into to consider a holistic approach (e.g. BMI,
compression classes; however, the pres- limb shape, disease severity, patient
sure range used to define each class varies preference and ability) before deciding
between the different standards, and what medical compression hosiery
different techniques are used to measure garment will provide the right compression
dosage (mmHg) for the patient.
the levels of compression (Lymphoedema
Framework, 2006) (Table 2). As a result,
Table 2. Classes and standards of medical compression hosiery
Compression standards
Compression class British standard 40 French Standard German Standard
(BS 661210) 3-month guarantee (AFNOR NF 30.102A) (RAL GZ 387/1) 6-month guarantee
(Partsch, 2003) (Levick, 2003) (Földi and Földi, 1983)
Class 1 mild 14–17mmHg 10–15mmHg 18–21mmHg
compression
Class 2 moderate 18–24mmHg 15–20mmHg 23–32mmHg
compression
Class 3 strong 25–35mmHg 20–36mmHg 34–46mmHg
compression
Class 4 extra strong Not available >36mmHg >49mmHg
compression
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 9CHAPTER 3: PATIENT CONSIDERATIONS DURING
MEDICAL COMPRESSION HOSIERY SELECTION
The patient’s clinical Different types of hosiery should be used Medical compression hosiery is available
presentation and at different stages of disease progression, as open-toe or closed-toe garments. In the
preferences should be depending on the conditions and symptoms close-toe option, the toe compartment of the
assessed during hosiery present, and whether or not oedema is pres- hosiery does not provide sufficient compres-
selection (e.g. presence ent. Compression garments are not a ‘one- sion at the tip, but it does provide contain-
of oedema, venous size-fits-all’ prescription. ment. It is important to protect the toes;
insufficiency and their this can be achieved through the use of toe
body size, limb shape, Role of compression in oedema gloves or caps, depending on the extent of the
size and shape of foot and Any form of oedema (i.e. oedema, chronic oedema, patient choice and ability to apply
manual dexterity).
oedema or lymphoedema) is a cause of con- (Elwell, 2014). Toe gloves can be used with
cern, and patients with oedema should seek open-toe or closed-toe hosiery.
Best Practice help as soon as possible and not wait until
Statement issues have developed. Patients with signs and
symptoms of lymphatic insufficiency should
Open-toe hosiery is frequently considered
easier to apply due to the fact they are often
be prescribed appropriate hosiery as early as supplied with a `silk-like slipper` device to aid
possible to manage the underlying condition application. A patient may require open-toe
Your clinician should and prevent disease progression (Anderson hosiery because:
identify the medical and Smith, 2014). Without appropriate treat- ■ The patient has arthritic or clawed toes
compression hosiery that ment to reduce the oedema, the affected tis- ■ The patient has a fungal infection
is best for your clinical sues become progressively hard, fibrosed and ■ The patient prefers to wear a sock over
individual needs. Your non-pitting, and the oedema fails to reduce the compression hosiery
compression garment on elevation. Patients with oedema will have ■ The patient has a long foot size compared
should be comfortable to
an altered leg shape, which may include large with calf size (hosiery with longer foot-
wear. If it is uncomfortable,
an alternative garment
skin folds especially around the ankle and size options are available, if necessary)
should be chosen. knee making it difficult to ascertain where the ■ The patient requires regular podiatry/
knee joint is. This can be exacerbated if the chiropody appointments
individual is overweight. ■ There is no oedema present in the toes,
Patient and the patient prefers open-toe hosiery
expectation In patients with chronic oedema, the key (NICE, 2012).
function of hosiery is ongoing maintenance
(Wounds UK, 2015). Compression com- Role of medical hosiery for patients with
bined with exercise increases lymph flow and venous insufficiency
venous return, thus reducing the volume of The therapeutic aim of compression for venous
oedema. In addition, compression increases insufficiency is to provide the highest level of
the blood flow into the microcirculation, compression possible that is tolerated by the
which may improve wound healing and help patient. National guidelines (NWCSP, 2020)
soften thickened or ‘woody’ tissues (Elwell, suggest the use of 2-layer compression kits that
2014). A made-to-measure medical compres- offer a minimum of 40mmHg as first-line, cost-
sion hosiery garment may be more practical effective treatment of venous leg ulceration.
for people with oedema as it can be measured
to the patient’s limb size and shape. Compression hosiery is most commonly
used by patients with venous insufficiency
Toe oedema for either primary prevention or post-ulcer
Toe oedema can be a natural occurrence in healing to control oedema and reduce venous
chronic oedema, but it can also be induced by hypertension.
incorrectly applied compression bandaging
that leaves the toes, and often the forefoot, People with healed venous leg ulcers and no
vulnerable without compression (Elwell, symptoms of arterial insufficiency should
2014). Oedema management requires ongo- be prescribed medical compression hosiery
ing maintenance, so if toe oedema is initially and reviewed 6-monthly for replacement
resolved with bandaging, the patient will need compression garments and ongoing advice
to be monitored and compression continued about prevention of recurrence (SIGN, 2010;
with compression hosiery. NWCSP, 2020).
10 BEST PRACTICE STATEMENT: COMPRESSION HOSIERY3. CLINICAL CONSIDERATIONS
Patient-related factors account when deciding which medical
Ultimately, the hosiery selected should be compression hosiery to use.
the patient’s choice. The practitioner’s job is
to explain the available options and direct Table 3 (page 12) offers suggestions for
the patient towards the clinically optimal medical compression hosiery and additional
choice. One of the most important factors treatment to manage the symptoms of venous
with regard to hosiery selection, partnership- insufficiency and oedema/lymphoedema.
working and concordance is understanding There are tools available that can help guide
the patient’s motivations and what is hosiery prescribing, for example, The Hosiery
important to the patient in their life. Hunter® tool focuses on the patient’s disease
progression and clinical symptoms, BMI and
The practitioner should listen to the patient limb shape (Wounds UK, 2019b).
and identify and understand the issues that
may result in non-concordance (Wounds
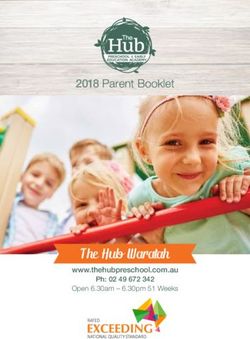
UK, 2015). Figure 2 summarises the patient-
specific factors that should be taken into
Patient preference
e.g. style,
appearance, colour.
Obesity
Consider wrap systems
Skin condition or stiffer flat-knit hosiery
See tips for skin care that has a higher SSI and
under compression ‘strong wall stability’
hosiery to hold the tissue.
(page 19). Also consider hosiery
application aids
(page 17).
Low dexterity or Consider limb shape
mobility Bandaging, wrap
Consider supplying systems or a stiffer flat-
patients with an aid knit compression hosiery
to ease application to reshape distorted limb
(page 17). shape and skin folds.
Patient motivation
Ask the patient what
is important to them
and what impact
treatment has on
their daily life.
Figure 2. Patient factors to
consider during garment selection.
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 113. PATIENT CONSIDERATIONS
Table 3. Suggestions for medical compression hosiery and additional treatment for venous insufficiency and oedema
Clinical indications Medical compression hosiery suggestion Additional treatment suggestions
C0 No visible or palpable signs of No treatment required No treatment required
venous disease
C1 Telangiectasias or reticular veins
C2 Varicose veins ■ Round-knit, off-the-shelf, RAL Standard ■ Daily skin care and emollient regimen to main-
Venous insufficiency: CEAP classification (Lurie et al, 2020)
C2r Recurrent varicose veins compression tain skin integrity
C3 Oedema ■ CCl 1 (18–21mmHg) or CCl 2 (23–25mmHg) ■ Simple ankle/calf exercises to enhance the calf
may be most appropriate muscle pump function
■ For patients who do not fit in standard sizes, ■ Increased activity/mobility, such as short walks
made-to-measure round-knit RAL Standard or water exercises (e.g. walking in shoulder-
options should be considered. If there is high water, aqua-aerobics or aqua-cycling, but
significant shape distortion, flat-knit, made- not swimming). A GP gym referral scheme
to-measure hosiery in CCl 1–3 should be may be available in some areas
considered. ■ Limb elevation on resting
C4 Changes in skin and subcutaneous ■ Round-knit, off-the-shelf, RAL Standard ■ Weight loss/maintenance (referral to dietitian
tissue secondary to CVD compression or bariatric services)
C4a Pigmentation or eczema ■ CCl 2 (23–25mmHg) may be most appropriate ■ If oedema is venous related and is persistent or
C4b Lipodermatosclerosis or atrophie ■ For patients not fitting in to standard sizes, worsening, patients should be seen by a vascu-
blanche round-knit, made-to-measure, RAL Standard lar specialist to explore venous intervention to
C4c Corona phlebectatica hosiery should be considered. aid symptoms (NICE, 2021).
C5 Healed ulcer
C6 Active venous ulcer ■ 2-layer compression hosiery kit or compression
C6r Recurrent active venous ulcer bandaging providing a combined 40mmHg
should be used.
Chronic oedema/lymphoedema ■ Round-knit, off-the-shelf, RAL Standard ■ Daily skin care and emollient regimen to main-
stage 0–2 (latency, mild or moderate) compression may be suitable in early stages tain skin integrity
■ Flat-knit, made-to-measure, RAL Standard ■ Simple ankle/calf exercises
Oedema classification (International Society of Lymphology, 2016)
hosiery should be considered in most cases ■ Avoid sitting with leg dependant/sleeping in
■ CCl 1–4 may be most appropriate according the chair at night-time; this may undermine all
to the holistic assessment of the individual and compression treatment/management
their circumstances. ■ Increasing activity/mobility, such as short
walks or water exercises (e.g. walking in
shoulder-high water, aqua-aerobics or aqua
cycling, but not swimming). A GP gym referral
scheme may be available in some areas
■ Limb elevation on resting
■ Consider simple/manual lymphatic drainage.
Chronic oedema/lymphoedema ■ Flat-knit, made-to-measure, RAL Standard ■ As above for chronic oedema/lymphoedema
stage 3 compression hosiery with a high SSI is often stage 0–2
the most suitable ■ Weight loss/maintenance (referral to dieti-
■ CCl 3 (35–45mmHg) or CCl 4 (>49mmHg) tian or bariatric services).
may be most appropriate; however, CCl 2
(23–35mmHg) may be considered according
to the holistic assessment of the individual and
their circumstances.
CCl: Compression class, CVD: Cardiovascular disease.
12 BEST PRACTICE STATEMENT: COMPRESSION HOSIERYCHAPTER 4: ENCOURAGING SHARED DECISION-
MAKING
Patient adherence to compression therapy The focus of compression treatment is to
The clinician should is often poor, but it is unhelpful to label slow disease progression, but it can be dif-
be confident in their patients as intentionally non-adherent ficult for the patient to imagine what will
own knowledge of
(Green and Jester, 2019). Rather than happen if they do not wear compression.
medical compression to
dismissing the patient as non-adherent to A way of promoting concordance with
confidently explain the
impact of compression treatment, instead listen to the patient’s compression therapy is to ask the patient
hosiery. During concerns and motivations with regard to to consider the future with regard to their
consultations, explore the the presenting condition. To help to facili- lower limbs and to discuss the possible
patient’s individual ideas, tate shared decision-making, use language consequences of not wearing compres-
concerns and expectations that is appropriate for the patient and cre- sion therapy, i.e. What might occur if they
of compression therapy. ate an open, accepting environment that choose not to wear it? What could life be
allows the patient to share their own story. like in a few years’ time?
Best Practice It is acceptable to discuss compromise, as During appointments, explore with the
Statement this may keep the patient engaged and can patient other avenues that will aid treat-
help ease patients into accepting long- ment and make compression more toler-
term treatments, such as medical com- able, such as skin care, elevation, activity,
pression hosiery. Patients also need to be weight loss, access to support groups. Ask
You should expect to be
aware that their choice cannot always be questions that might not be directly relat-
involved in making joint
decisions about your care,
fully accommodated, and that there may ed to compression therapy itself, but might
feel able to voice your have to be some balance between clinical help to identify areas where the patient
concerns and be reassured need and patient preference. Treatment could be supported. Box 2 includes areas
that changes can be made can be modified to use a lower compres- of discussion for clinician and patient to
to your care if required. sion if high compression is not tolerated help inform compression selection.
Your clinician may ask at first, but discussions should include
whether you have family/ the fact that as tolerance builds over time, ‘Best’ garment for the patient
carers who would like to compression levels may also be increased. The ‘best’ garment for the patient is the
take part in the care plan if Practitioners and patients alike should garment that they will use and wear cor-
you need extra support. understand that compression is an on- rectly. To identify the best garment for the
going treatment that needs to be worn patient:
Patient long-term, just as long-term medication 1. Listen and explore: Explore the pa-
expectation regimens should be adhered to. tient’s understanding, concerns and
hopes related to medical compression
hosiery (Box 2).
MYTH 2. Assess: Assess the limb and patient to
determine the most appropriate medi-
cal compression hosiery clinically (see
Wearing compression is always for life.
Chapter 2).
3. Consider patient ability: Consider the
TRUTH patient’s ability to apply compression ho-
siery, for example their manual dexterity
and their body size and shape.
Some conditions such as lymphoedema 4. Check fit: Check how the medical com-
require compression therapy for life, others,
pression hosiery fits on the leg(s).
such as varicose veins, may be surgically
treated and may not require life-long
5. Patient preference: Ask the patient if
therapy. For patients with chronic oedema they are happy with the appearance and
and venous insufficiency where intervention fit of the medical compression hosiery.
is not suitable, medical compression therapy
is a life-long therapy.
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 134. SHARED DECISION-MAKING
Box 2. Questions to ask the patient during medical compression hosiery selection:
gathering information and encouraging adherence
■ What do you understand about the condition in your leg(s)?
■ Have you used medical compression garments before?
■ If yes, how did they affect your day-to-day lifestyle?
■ What are your priorities for treatment?
■ Do you feel confident in applying and removing your hosiery?
■ Is there someone who can help you apply/remove your medical compression garments?
■ Are you happy with the medical compression hosiery’s colour? Pattern? Texture? Softness? (This is
especially important to ask as summer approaches, so patients have medical compression they are
comfortable with when wearing lighter/shorter clothing).
■ Would you prefer open- or closed-toe medical compression hosiery?
■ Do you have at least two pairs of medical compression hosiery? (Patients must wash and wear pairs
alternately, and not keep one pair ‘in good shape’ for later).
Supporting patients at home
MYTH To successfully support your patient to care at
home, they need to have understanding of:
If the patient refuses to wear medical ■ The reasons why hosiery has been pre-
compression hosiery, there is nothing more scribed
that can be done for the patient. ■ A well-fitting garment, skin care and how
to apply and remove the garment
TRUTH
■ The expectations of care
■ When they should contact the clinician
and the ‘red flags’
If the patient refuses to wear medical ■ The emergency contact details of who to
compression hosiery, listen to the patient’s contact if issues arise
concerns and why they feel they cannot ■ When and how to re-order hosiery
wear compression hosiery. Consider with
the patient whether the expectations of care
need to be modified. The expectations of
Patients may also benefit from keeping a self-
care should be agreed between the clinician care journal and being provided with where to
and patient before treatment begins and access online patient resources (e.g. Legs Mat-
revisited during treatment. ter campaign: www.legsmatter.org/help-infor-
mation/resources) or advice leaflets designed
for patients (e.g. www.lymphoedema.org).
MYTH
Wearing medical compression hosiery is
uncomfortable.
TRUTH
Patients with venous and lymphatic
disorders should always feel more
comfortable when wearing medical
compression hosiery than when they are not.
14 BEST PRACTICE STATEMENT: COMPRESSION HOSIERYCHAPTER 5: MEASURING AND SIZING
Medical compression hosiery is only effective pressure to control their limb on an ongoing
Limbs should be if the patient’s limbs are measured accurately basis. After measurement, it is important to
measured and medical and the garment is applied correctly. Medical continue with compression bandaging until
compression hosiery compression measured and prescribed inac- the patient’s compression hosiery garment
prescribed according
curately can lead to tissue trauma/pressure is available. Box 3 includes tips for hosiery
to the manufacturer’s
damage particularly if the fabric rolls during measurement.
own measuring guide, as
sizes vary according to wear or is too tight and digs into the skin
manufacturer. There are (Robertson et al, 2014). These experiences If a patient does not fit the measurements on
tools available to support may stop the patients wanting – or being able the manufacturer’s sizing chart for standard,
clinicians to measure – to continue with treatment. off-the-shelf sizes, ‘made-to-measure’ medical
and identify the correct compression hosiery should be prescribed.
compression garment for Limbs should be measured and hosiery pre- Made-to-measure can be considered first line
the patient. scribed according to each manufacturer’s own for chronic oedema and larger limbs with a
measuring guide, as sizes vary according to uniform shape, i.e smaller at the ankle, in-
manufacturer. Every effort should be made to creasing in size up the leg. Where skins folds
Best Practice reduce oedema before hosiery is measured. In are present compression bandaging will be re-
Statement some cases, bandaging may be required dur-
ing the intensive management phase to help
quired first to achieve reduction and reshap-
ing. If fitting is not accurate, hosiery will fail
reshape the limb, reduce limb volume and/ to prevent oedema, maximise ulcer healing or
or treat the ulcer. Once oedema has reduced, prevent recurrence, and will increase the risk
patients can be measured for medical com- of skin damage complications (Wounds UK,
You should expect your pression hosiery that will deliver sufficient 2015).
clinician to measure both
of your legs so that you can
be prescribed appropriately Box 3. Tips for hosiery measurement (Wounds UK, 2015)
sized medical compression
hosiery. ■ Use the correct measuring guide for the brand of medical compression hosiery to be pre-
scribed, as each manufacturer will vary
Patient ■ Take measurements as early in the morning as possible, when oedema is at a minimum
expectation (see below for common measurement points for A] off-the-shelf; and B] made-to-measure
compression hosiery)
A. B.
Images used with permission of medi UK©.
■ Take measurements directly against the skin to ensure accuracy (use a skin marker to ensure
accuracy and reproducability)
■ Take measurements for both leg, as they may differ in size
■ Take measurements when the patient is sitting down, with feet flat on the floor
■ If the patient has skin folds due to oedema or the limb is particularly misshapen, a specialist
flat-knit garment may be required. This will require specialist assessment.
■ Ask the patient to wear their medical compression hosiery to the next appointment so that the
fit can be re-evaluated.
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 155. MEASUREMENT AND SIZING
The practitioner should prescribe a minimum colour and options on prescription, which
of two, but preferably three pairs of medi- may support concordance. Patients may be
cal compression hosiery (one to wash, one given details of websites where they can re-
air drying and one to wear) every 6 months search the hosiery products further online.
(3 months for British Standard compres-
sion hosiery), to ensure the effectiveness of
compression. This is regardless of the type of
compression or class. Prescriptions should
be clearly and thoroughly specified to ensure
MYTH
accurate dispensing. The patient only ever needs two pairs of
medical compression hosiery.
When a new prescription is required, the pa-
tient must be re-measured. If the patient has
a current medical compression prescription, TRUTH
it should be continued until the new prescrip-
It would be beneficial to the patient if
tion is ready. If the weight of the patient re- clinicians prescribed a minimum of two
duces or increases, this is likely to change the pairs of medical compression hosiery every
size of the limb. Old, worn hosiery should be 6 months (3 months for British Standard).
handed back to the clinician when the patient Some patients may be able to purchase more
receives a new prescription to prevent the pairs privately if they are given the full details
patient wearing old ‘comfy’ medical hosiery. of the garment.
Some hosiery manufacturers a wide range of
Fitting FAQs
The patient has previously found compression uncomfortable and placement are correct, it may be beneficial to suggest
and doesn’t want to try again – what do I do? using a garment with a different style or a stiffer fabric. If the
If the patient did not tolerate compression in the past, it does hosiery are thigh-length garments and the hosiery fit has
not mean that they will not be able to tolerate compression been checked, consider using an adhesive designed to adhere
ever again. If the hosiery is not comfortable, it is not the right compression garments to the limb.
choice for this patient right now. Talk to the patient again and
listen to their concerns. How will I know that the compression garment is working?
Compression therapy will help with limb volume reduction
What if the hosiery digs in at the top around the knee? and leg comfort. If the leg was initially swollen and the medi-
Check that the garment is not overstretched and that place- cal compression hosiery starts to loosen and fall down after
ment is correct (the top band should sit two fingers’ width a few weeks, this could be a positive sign that treatment is
from the crease of the knee). If the size and the placement are working. You might have to order a smaller-sized stocking
correct, it may be beneficial to change the fabric. Contact your initially, depending on the condition you are treating and until
local TVN/lymphoedema specialist if unsure. the limb is stable. The patient should know who to contact if
the garment is getting loose quickly, and that this is not a sign
What if the compression hosiery is too tight? that the compression therapy has worked and is no longer
Ensure patients understand that a larger garment size will not required.
make the garment feel less tight, and that this will reduce the
effectiveness of the treatment. Less elastic garments may be What if the garment starts to fall down?
useful if this feeling persists. Garments that continue to fall down cannot provide thera-
peutic compression. If the garment fits and the fabric is the
What if the top of the compression hosiery is rolling? correct type for the condition being treated, the use of a body
Check that the garment is the correct size/measurement glue, or addition of a top band, may help to keep the garment
and ensure placement is correct (with the top band sitting in place.
two fingers’ width from the crease of the knee). If the size
16 BEST PRACTICE STATEMENT: COMPRESSION HOSIERYCHAPTER 6: KEY ELEMENTS TO SUPPORTED SELF-
MANAGEMENT: HOSIERY APPLICATION, REMOVAL
AND CARE, AND SKIN CARE
Hosiery application (donning) and sion stocking aid is usually made from a
The practitioner who removal (doffing) slippery fabric, which is designed to make
measured, selected and Even if the patient is experienced with it easier to slide compression hosiery over
prescribed the medical the foot and leg. Patients will still need
compression hosiery, they should not
compression hosiery
independently apply compression hosiery to be able to bend to reach their feet with
should guide the patient
through first application, for the first time or if the prescription has fabric aids. Rigid aids typically provide a
and discuss how to apply changed. The practitioner should demon- frame that lets the patient step into hosiery
and remove the hosiery, strate donning and doffing, then help the or pull up garments without bending to
how to manage skin patient practise until they are competent at reach the floor (Dilks and Green, 2005).
care under compression applying and taking off compression hosiery There are many different aids available,
and how to take care of on their own. Showing how to apply and which should be chosen according to each
compression hosiery. remove the hosiery and what constitutes a patient’s physical needs (Table 4, page 19).
If this is not possible, good fit when a carer is present is beneficial
another qualified, skilled (Box 4). Other aid options include non-slip mats,
practitioner should guide roll-on adhesives and roll-on membranes.
the patient. Box 4. Quick guide for good medical Wearing rubber gloves with soft interior
compression hosiery fit
linings can aid grip during application
Best Practice ■ Hosiery should fit well and not feel loose and removal of all types of compression
Statement ■ Hosiery should not be twisted, rolled or
folded down
stockings.
■ Hosiery should sit two fingers’ width below
the knee crease, or four fingers’ width MYTH
below the gluteal fold in thigh-length gar-
The clinician who
ments Hosiery application and removal aids are not
measured and prescribed
■ The fabric should be evenly distributed available on the NHS.
your medical compression
hosiery should show you over the length of the garment
how to apply (don) and ■ Hosiery should not pinch the skin or cause
remove (doff) the hosiery,
and provide you with ■
pain
If numbness or pain occurs while wear- TRUTH
advice on how to care ing medical compression, it should be
for your limb, skin and Clinicians who prescribe compression
removed and reported to the clinician who
garments. If you do not hosiery should ensure that they are familiar
prescribed the compression hosiery with the aids that are available on FP10
understand any part of
■ Hosiery should not cause shortness of locally and advise patients accordingly.
what has been said, you
breath.
should ask for further
explanation.
It is important to explain that compression
Patient hosiery application is a new skill, which
expectation may require patience and practice in the Application & removal FAQs
early phase of treatment. Patients should
ensure they set aside time in their daily Can the patient wear compression while
routine and their environment is suit- they sleep at night?
able to apply/don and remove/doff their It is preferable that the patient wears medi-
hosiery. Instructions to apply thigh-length cal compression hosiery throughout the day
hosiery without a fabric or rigid aid are and removes them at night, allowing for the
shown in Figure 3, page 18. skin to be routinely checked for compression
damage and to be moisturised. However,
If a patient finds it difficult to don their if the patient sleeps in a chair, they should
hosiery, a hosiery application aid can help. wear medical hosiery throughout the night
Application and removal aids are typically to prevent the legs from swelling. Patients
either fabric or rigid. A fabric compres- with complex lymphoedema may be advised
to wear a garment overnight.
BEST PRACTICE STATEMENT: COMPRESSION HOSIERY 17You can also read