Association for Bariatric Endoscopy systematic review and meta-analysis assessing the American Society for Gastrointestinal Endoscopy Preservation ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ABE COMMITTEE SPECIAL ARTICLE
Association for Bariatric Endoscopy systematic review and
meta-analysis assessing the American Society for
Gastrointestinal Endoscopy Preservation and Incorporation of
Valuable Endoscopic Innovations thresholds for aspiration
therapy
Pichamol Jirapinyo, MD, MPH,1,* Nitin Kumar, MD, FASGE,2,* Monica Saumoy, MD, MS,3
Andrew Copland, MD,4 Shelby Sullivan, MD5
Boston, Massachusetts; Effingham, Illinois; Philadelphia, Pennsylvania; Charlottesville, Virginia; Aurora, Colorado, USA
This document was reviewed and approved by the Governing Board of the American Society for Gastrointestinal
Endoscopy.
A subcommittee of the Association for Bariatric Endoscopy, a division of the American Society for Gastrointestinal
Endoscopy (ASGE) comprising experts in the subject area, performed this systematic review and meta-analysis.
The systematic review and meta-analysis was reviewed by the ASGE Technology Committee and was ultimately
submitted to the ASGE Governing Board for approval. The systematic review and meta-analysis underwent
peer review by outside experts in statistics and meta-analysis before receiving final ASGE Governing Board
approval. The Preservation and Incorporation of Valuable Endoscopic Innovations (PIVI) initiative is an ASGE pro-
gram whose objectives are to identify important clinical questions related to endoscopy and to establish a priori
diagnostic and/or therapeutic thresholds for endoscopic technologies designed to resolve these clinical questions.
Once endoscopic technologies meet an established PIVI threshold, those technologies are appropriate to incor-
porate into clinical practice, presuming the appropriate training in that endoscopic technology has been achieved.
ASGE encourages and supports the appropriate use of technologies that meet its established PIVI thresholds.
(Gastrointest Endosc 2021;93:334-42.)
Obesity is a chronic disease associated with multiple co- interventions and pharmacologic treatment, less invasive
morbidities and has significant global impact on health, qual- than bariatric surgery, and easily performed at a lower
ity of life, and longevity.1,2 In recent decades, interventions expense than that of surgery.
such as diet and lifestyle modification, pharmacologic Endoscopic bariatric therapies (EBTs) are gaining clin-
therapy, and bariatric surgery have not been sufficiently ical acceptance as tools to address the invasiveness and ef-
effective to arrest the growth of the obesity epidemic at ficacy gap in obesity care between pharmacotherapy and
the population level.3,4 There is a need for weight loss bariatric surgery. Several EBTs have emerged, gained U.S.
therapies that are more effective and durable than lifestyle Food and Drug Administration (FDA) approval, and have
Abbreviations: : ASGE, American Society for Gastrointestinal Endoscopy; Current affiliations: Division of Gastroenterology, Hepatology and
A-tube, aspiration tube; EBT, endoscopic bariatric therapy; EWL, excess Endoscopy, Brigham and Women’s Hospital, Boston, Massachusetts, USA
weight loss; FDA, U.S. Food and Drug Administration; PIVI, Preservation (1), HSHS Medical Group, Effingham, Illinois, USA (2), Division of
.and Incorporation of Valuable Endoscopic Innovations; SAE, serious Gastroenterology, Perelman School of Medicine, University of
adverse event; TWL, total weight loss. Pennsylvania, Philadelphia, Pennsylvania, USA (3), Division of
Gastroenterology and Hepatology, Department of Medicine, University
*Drs Jirapinyo and Kumar contributed equally to this article. of Virginia, Charlottesville, Virginia, USA (4), Division of Gastroenterology
Copyright ª 2021 by the American Society for Gastrointestinal Endoscopy and Hepatology, University of Colorado School of Medicine, Aurora,
0016-5107/$36.00 Colorado, USA (5).
https://doi.org/10.1016/j.gie.2020.09.021 Reprint requests: Pichamol Jirapinyo, MD, MPH, Associate Director of
Received September 14, 2020. Accepted September 14, 2020. Bariatric Endoscopy, Brigham and Women’s Hospital, 45 Francis St, 2nd
Floor, Boston, MA 02115.
334 GASTROINTESTINAL ENDOSCOPY Volume 93, No. 2 : 2021 www.giejournal.orgJirapinyo et al ASGE PIVI thresholds for aspiration therapy
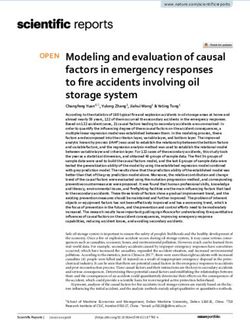
3. Connector, which counts the number of aspirations and
locks after 115 uses to allow for long-term monitoring of
compliance with therapy
4. Companion, which is a 2-way tube to allow instillation of
water into the gastric lumen and subsequent flow of
gastric contents out during aspiration
5. Reservoir (600 mL), which is used to instill water into
the stomach and then aspirate gastric contents, and a
drain tube, which attaches to the Companion to guide
gastric contents into a toilet.
Other than the A-tube and Skin-Port, the remaining ac-
cessories can be carried in a small pouch and used only
during aspiration. Patients require access to a restroom
approximately 20 minutes after eating, and the aspiration
process takes 10 to 15 minutes. The other components
of aspiration therapy include lifestyle therapy in conjunc-
tion with medical monitoring.
AspireAssist is FDA approved for individuals ages 22 and
older with a body mass index of 35 to 55 kg/m2 who have
attempted and failed nonsurgical weight loss therapy. Con-
traindications to aspiration therapy with the AspireAssist
include history of abdominal surgery, which increases the
risk of gastrostomy tube placement; esophageal or gastric
diseases, which increase the risk of adverse events (such
as esophageal stricture, gastric varices, and refractory
gastric ulcers); and eating disorders such as bulimia nerv-
osa and binge eating syndrome (Table 1).7 Patients in
whom an eating disorder is suspected should be referred
for formal psychiatric evaluation before aspiration
therapy is considered.
An EBT that meets the PIVI thresholds should be
considered appropriate for clinical practice in the setting
Figure 1. Implanted components. A, Tube and Skin-Port. B, Compo- of appropriate training and credentialing (Table 2).8 This
nents used during aspiration: connector, companion, and reservoir. systematic review and meta-analysis were performed by
(From Thompson et al.13 With permission.) the Association for Bariatric Endoscopy to specifically eval-
uate whether aspiration therapy meets these PIVI thresh-
demonstrated safety, efficacy, reversibility, and repeat- olds, based on the existing literature.
ability with clinical reproducibility.5
Aspiration therapy is an EBT that entails postprandial
aspiration of gastric contents through a gastrostomy tube METHODS
to reduce calorie absorption for weight loss and is the focus
of this Preservation and Incorporation of Valuable Endo- Data sources and search strategies
scopic Innovations (PIVI) initiative.6 AspireAssist (Aspire A comprehensive search of several English-language da-
Bariatrics, King of Prussia, Pa, USA) is an FDA-approved de- tabases was conducted for studies published between
vice for aspiration therapy that has demonstrated safety and January 1, 2000 and August 25, 2019. The databases
efficacy in the current medical literature (Fig. 1). There are included MEDLINE, EMBASE, and Web of Science. The
no comparable technologies designed for aspiration therapy search strategy was defined a priori and conducted with
or data on the use of conventional gastrostomy tubes for the assistance of a university librarian (Supplementary
performance of aspiration therapy for the treatment of Table 1, available online at www.giejournal.org). All
obesity. The device components include the following: studies assessing the efficacy and safety profile of
1. Aspiration tube (A-tube), which is a large-bore (6.0-mm in- aspiration therapy were searched with no specific
ternal diameter) fully silicone gastrostomy tube with a 15- limitations. Relevant studies were also identified from the
cm fenestrated portion extending into the gastric lumen bibliography of studies obtained through the search.
2. Skin-Port, which is a 3.5-cm diameter disc that remains An expert methodologist (P.J.) oversaw the systematic
fixed to the external portion of the aspiration tube review and meta-analysis process. Two primary authors
and contains a 1-way valve (P.J. and N.K.) independently reviewed the titles and
www.giejournal.org Volume 93, No. 2 : 2021 GASTROINTESTINAL ENDOSCOPY 335ASGE PIVI thresholds for aspiration therapy Jirapinyo et al TABLE 1. Contraindications to AspireAssist therapy Previous abdominal surgery, which increases the risk of gastrostomy tube placement Esophageal stricture, pseudo-obstruction, severe gastroparesis, gastric outlet obstruction Inflammatory bowel disease History of refractory gastric ulcer Ulcers, bleeding lesions, or tumors discovered during endoscopic examination Uncontrolled hypertension (blood pressure >160/100 mm Hg) History or evidence of serious pulmonary or cardiovascular disease (acute coronary syndrome, New York Heart Association class III or IV heart failure) Coagulation disorder (platelets 2 seconds above control, or international normalized ratio >1.5) Anemia (hemoglobin
Jirapinyo et al ASGE PIVI thresholds for aspiration therapy
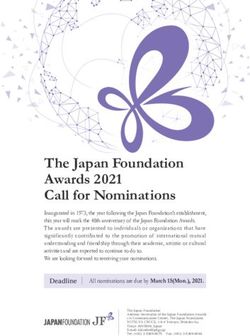
Identification
Records identified through database searching
(n = 225)
MEDLINE: 67
EMBASE: 151
Web of Science: 7
Duplicates excluded
(n = 24)
Identification
Total non-duplicate
(n = 201)
Articles excluded after title and abstract review (n = 177)
- Not related to obesity: 85
- Not original research: 79
- Not related to AspireAssist: 13
Full-text articles assessed for eligibility
(n = 24)
Eligibility
Articles excluded after full text review (n = 19)
- Same Cohort: 13
- Not original research: 4
- Full-text not available: 1
- Case report: 1
Included
Studies included in the meta-analysis
(n = 5)
- Published studies: 4
- Abstracts: 1
Figure 2. Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Statistical heterogeneity was evaluated by means of I2 statis- which were duplicates. After title and abstract review, 177
tics and Q values. An I2 value greater than 50% was considered studies were excluded, leaving 24 studies for full article
to indicate high statistical heterogeneity. A funnel plot and review. Full text review resulted in 5 studies that met
classic fail-safe test were used to assess potential publication criteria for inclusion in the systematic review and meta-
bias. Additionally, serious adverse event (SAE) rates were analysis, of which 4 were peer-reviewed published studies
analyzed as reported in the articles, regardless of the definition and 1 was an abstract.12-16 Studies included in the meta-
used in the article to define a SAE. Of note, some SAEs re- analyses are summarized in Table 3.
ported in the article may not meet the FDA criteria for SAE
as defined in accordance with 21CFR803.3.9-11 Primary outcomes
Analyses were performed by one of the primary authors Four studies with a total of 373 aspiration therapy sub-
(P.J.) using the comprehensive Meta-analysis software jects reported weight loss outcomes. Pooled intention-to-
(Comprehensive Meta Analysis, version 2.2; Biostat Inc, treat data reported 43% excess weight loss (EWL) at 12
Englewood, NJ, USA). Of note, the primary authors who months in the aspiration therapy group, which was 25.6
performed data extraction (P.J. and N.K.) and analysis percentage points greater than control subjects, with a
(P.J.) were authors on some articles included in the anal- SAE rate of 3.8% (Table 4). Both the efficacy and safety
ysis. Independent review of the data analysis and editing endpoints defined by the PIVI thresholds for an EBT
of the document was performed by authors who had not were met, because the percentage of EWL exceeded 25%
contributed to any of the included studies (M.S. and A.C.). in AspireAssist subjects with class II/III obesity and the
difference between AspireAssist and control subjects
RESULTS exceeded 15% EWL in both the intention-to-treat analysis
and the per-protocol analysis.
Search results Excess weight loss. A meta-analysis of aspiration
Results of the search are shown in Figure 2. The therapy (intention-to-treat, including 4 studies with 373
literature search resulted in 225 potential studies, 24 of aspiration therapy patients) found 43.0% EWL at 1 year
www.giejournal.org Volume 93, No. 2 : 2021 GASTROINTESTINAL ENDOSCOPY 337ASGE PIVI thresholds for aspiration therapy Jirapinyo et al
TABLE 3. Summary of studies included in the meta-analyses
No. of subjects Female Initial body mass Total weight Excess weight
Study Design Sites (device/control) Age (y) (%) index (kg/m2) loss (%)WL loss (%)
Studies included in the analysis of primary and secondary outcomes
Sullivan 201312 Randomized 1 18 (11/7) 38.7 2.3 100 42.6 1.4 18.6 2.3 49.0 7.7
controlled trial
Thompson 201713 Randomized 10 171 (111/60) 46.1 10.2 82.9 42.4 5.0 14.2 9.8 37.2 27.5
controlled trial
Nyström 201814 Postmarket 5 201 46.1 10.9 75.1 43.6 7.4 18.2 9.4 46.3 26.3
observational
Wilson 201816 Postmarket 1 50 41.0 11.0 76.0 42.6 7.5 21.0 11.0 55.0 29.0
observational
Studies included in the analysis of secondary outcome only
Thompson 201915 Randomized 10 58 (15 at 4-year 43.7 9.7 41.6 4.5 18.7 11.7 50.8 31.9
controlled trial analysis)
Values are mean standard deviation.
(95% CI, 33.2-52.7) (P < .0001; I2 Z 88.8, P Z .001) abdominal pain secondary to prepyloric ulcer (.3%), and
(Fig. 3A). A meta-analysis of aspiration therapy (per-proto- product malfunction requiring A-tube replacement (.3%).
col, including 4 studies with 296 aspiration therapy pa- No patients in the aspiration therapy groups developed an
tients) found 46.3% EWL at 1 year (95% CI, 38.8-53.8; eating disorder, such as bulimia nervosa or binge eating dis-
P < .0001; I2 Z 77.7, P Z .038) (Fig. 3B). order, which was evaluated by both questionnaire and inter-
Total weight loss. A meta-analysis of aspiration ther- view examinations in 2 U.S. randomized controlled
apy (intention-to-treat, including 4 studies with 373 aspira- trials.12,13 No deaths have been reported.
tion therapy patients) found 16.6% total weight loss (TWL)
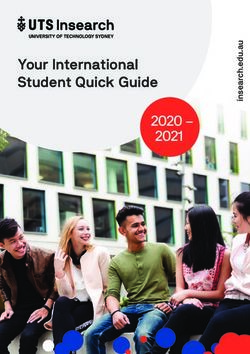
at 1 year (95% CI, 12.8-20.4; P < .0001; (I2 Z 90.3, P < Risk of bias
.0001) (Fig. 4A). A meta-analysis of aspiration therapy Risk of bias across studies that evaluated primary out-
(per-protocol, including 4 studies with 296 aspiration ther- comes was assessed using funnel plots. Visual inspection
apy patients) found 17.8% TWL at 1 year (95% CI, 15.0- demonstrated relatively symmetric funnel plots, suggesting
20.7; I2 Z 80.5, P < .0001) (Fig. 4B). minimal publication bias (Fig. 5). The classic fail-safe
method suggested that 733 and 827 studies would be
Secondary outcomes required to show no changes in EWL and TWL at 1 year af-
Longer term efficacy. Weight loss at 1 year was calcu- ter aspiration therapy, respectively (intention-to-treat
lated using published studies and abstracts. There was a analysis).
statistically significant weight loss at 1, 2, 3, and 4 years
of follow-up (Table 5). Additionally, analysis of change in
comorbidities at 1 year showed significant improvement DISCUSSION
in systolic and diastolic blood pressure, triglyceride level,
high-density lipoprotein, hemoglobin A1c, aspartate amino- Effective endoscopic therapy of obesity will require
transferase level, and alanine aminotransferase level in the tools that are broadly applicable across patient popula-
intention-to-treat analysis (Table 6). tions; safe, effective, and deliverable by an expansive range
Subgroup analysis of randomized controlled tri- of providers; and amenable to long-term clinical moni-
als. A subgroup analysis of randomized controlled tri- toring. The endoscopic treatment of obesity incorporates
als12,13 found that at 1 year the aspiration therapy group a broadening variety of devices with various mechanisms
lost more total weight (% TWL) than the lifestyle therapy of action to meet these needs.
group by 11.6 percentage points (95% CI, 6.5-16.7; P < The body of published evidence for aspiration therapy
.0001). At 1 year the aspiration therapy group lost more demonstrates that aspiration therapy does meet American
excess weight (% EWL) than the lifestyle therapy group Society for Gastrointestinal Endoscopy (ASGE) PIVI
by 25.6 percentage points (95% CI, 16.0-35.3; P < .0001). criteria. Additionally, aspiration therapy induced significant
Adverse events. All four studies (with a total of 373 improvement in multiple comorbidities of obesity,
aspiration therapy subjects) reported SAEs. The pooled including diabetes mellitus, markers of steatohepatitis, hy-
SAE rate was 3.8% (14/373). These included buried bumper pertension, and hyperlipidemia. The AspireAssist device
(2.2%), peritonitis treated with intravenous antibiotics (.5%), for performing aspiration therapy has proven safe across
severe abdominal pain treated with pain medication (.5%), studies, with a low adverse event rate and no reported
338 GASTROINTESTINAL ENDOSCOPY Volume 93, No. 2 : 2021 www.giejournal.orgJirapinyo et al ASGE PIVI thresholds for aspiration therapy
TABLE 4. Aspiration therapy meets PIVI thresholds
Absolute efficacy Relative efficacy Serious adverse events (%)
PIVI threshold 25% EWL at 12 mo 15% EWL greater than control subjects 5
Statistically significant difference
compared with control subjects
Aspiration therapy (pooled 43% EWL at 12 mo 25.6% EWL greater than control subjects 3.8
intention-to-treat data) P < .0001
PIVI, Preservation and Incorporation of Valuable Endoscopic Innovations; EWL, excess weight loss.
after A-tube removal can be treated with a variety of
techniques, including proton pump inhibitor therapy
with argon plasma coagulation of the fistula tract and
gastric os, endoscopic clip placement, and endoscopic
suturing. The risk appears to increase after the A-tube
has been in place for 2 years or longer, which is consis-
tent with PEG tube placement as well.14,20 Notably, no
deaths have been reported, underscoring the safety of
the therapy.
Attention has been given to the effect of aspiration
therapy on the risk of developing eating disorders. How-
ever, no patients in the aspiration therapy group devel-
oped an eating disorder, such as bulimia nervosa or
binge eating disorder. Both randomized controlled trials
included 2 eating disorder evaluations (Questionnaire on
Eating and Weight Patterns Revised and Eating Disorder
Examination) administered before enrollment and again
Figure 3. Percent excess weight loss at 1 year after aspiration therapy. A,
at approximately 4, 6, and 12 months into therapy.
Intention-to-treat analysis. B, Per-protocol analysis. CI, Confidence
interval. One patient in the control group of the PATHWAY study
developed binge eating disorder. The prevalence of
deaths. Although not included in this meta-analysis, Aspir- binge eating disorder in patients with obesity is 3.3%
eAssist has also demonstrated significant and durable effi- to 3.5% and 14% to 56% in patients seeking bariatric sur-
cacy in 11 superobese patients at 3 centers with a mean gery, so it is not unexpected that a patient would
body mass index of 66.5 kg/m2, with 14.5% TWL (28.5% develop binge eating in a trial.21 However, the fact that
EWL) at 6 months, 21.4% TWL (33.9% EWL) at 1 year (8/
11 patients), and 25.5% TWL (38.8% EWL) at 2 years.17
There were no SAEs.
The SAEs reported for aspiration therapy are similar
to those reported for PEG tube placement, including
buried bumper, peritonitis, severe abdominal pain
treated with pain medication, and persistent fistula after
removal.18 The multicenter PATHWAY study included
multiple sites and extensive characterization of adverse
events. In the Pivotal Aspiration Therapy with Adjusted
Lifestyle Therapy (PATHWAY) study, the SAEs included
a case of mild peritonitis treated with intravenous
antibiotics, a case of severe perioperative pain treated
with intravenous analgesics, a case of abdominal pain
from a prepyloric ulcer at 53 weeks, and a case of skin-
port malfunction requiring A-tube replacement.19 Late-
onset buried bumper can be treated with temporary
placement of a 20F gastrostomy tube and then replace-
ment of the A-tube. Peristomal granulation tissue has Figure 4. Percent total weight loss at 1 year after aspiration therapy. A,
been frequently reported and can be addressed during Intention-to-treat analysis. B, Per-protocol analysis. CI, Confidence
clinical follow-up with topical therapy. Persistent fistula interval.
www.giejournal.org Volume 93, No. 2 : 2021 GASTROINTESTINAL ENDOSCOPY 339ASGE PIVI thresholds for aspiration therapy Jirapinyo et al
TABLE 5. Weight loss and analysis of subjects who completed study protocols (published studies D abstracts)
Duration of aspiration therapy No. of studies (no. of subjects) Amount of weight loss (%) P value I2 (P value)
Total weight loss
1y 3 (296) 17.8 [15.0-20.7]Jirapinyo et al ASGE PIVI thresholds for aspiration therapy
0
2
Standard Error
4
6
8
10
-100 -80 -60 -40 -20 0 20 40 60 80 100
A
Mean
0
1
Standard Error
2
3
-50 -40 -30 -20 -10 0 10 20 30 40 50
B Mean
Figure 5. Funnel plots for the primary outcomes (intention-to-treat analysis). A, Percent excess weight loss at 1 year after aspiration therapy. B, Percent
total weight loss at 1 year after aspiration therapy.
(reaching >55 kg/m2 in case series outside the United obesity and comorbidities of obesity an attractive, less-
States), a high level of efficacy, and durability extend- invasive treatment option.
ing beyond 4 years. The technical skill for placement Limitations of this meta-analysis include risk of bias in
of AspireAssist does not require proctoring or other nonrandomized studies. Additionally, 1 study16 was an
extensive training, because the device can be placed abstract but was included because the principal
by endoscopists familiar with PEG tube placement. investigator died, and it is not certain that a full article
The conventional mechanism of device placement will be published. The analysis found a high degree of
means that adverse events involving the aspiration heterogeneity among included studies, which is
tube are familiar and easily manageable by practi- consistent with the limited number of published studies.
tioners familiar with the management of traditional Nevertheless, each study demonstrated significant weight
gastrostomy tubes. Furthermore, the integration of a loss in its study population, and the findings were
counter into the device, which locks and prevents consistent with the results of both randomized trials.
usage after 115 aspirations, allows physicians to monitor pa- AspireAssist meets PIVI thresholds based on currently
tients for underuse and/or overuse and to encourage available medical literature. The Association for Bariatric
compliance with follow-up. Long-term compliance is also Endoscopy and ASGE will continue to work with their
enhanced by the dietary flexibility AspireAssist allows, members and other medical societies to promote and facil-
because occasional high-volume meals are not precluded itate widespread adoption and implementation of safe and
by the device. In total, AspireAssist offers patients with effective EBTs in clinical practice.
www.giejournal.org Volume 93, No. 2 : 2021 GASTROINTESTINAL ENDOSCOPY 341ASGE PIVI thresholds for aspiration therapy Jirapinyo et al
DISCLOSURE 7. Aspire Bariatrics, Inc. AspireAssist instructions for use. Available at:
https://www.accessdata.fda.gov/cdrh_docs/pdf15/p150024d.pdf. Ac-
cessed November 10, 2019.
The following authors disclosed financial relation- 8. Ginsberg GG, Chand B, Cote GA, et al. A pathway to endoscopic bar-
ships: P. Jirapinyo: Research support from Apollo Endo- iatric therapies. Gastrointest Endosc 2011;74:943-53.
surgery, Aspire Bariatrics, Fractyl, and GI Dynamics; 9. U.S. FDA. CFR - Code of Federal Regulations Title 21. Available at:
consultant for Endogastric Solutions and GI Dynamics; https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.
cfm?frZ312.32. Accessed July 5, 2020.
honorarium from Obalon Therapeutics; in-kind support
10. U.S. FDA. What is a serious adverse event? Available at: https://www.
from USGI Medical. N. Kumar: Consultant for Aspire Bari- fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-
atrics, GI Dynamics, Obalon Therapeutics, and USGI event. Accessed July 5, 2020.
Medical. S. Sullivan: Consultant for Aspire Bariatrics, 11. U.S. FDA. 21CFR803dmedical device reporting. Available at: https://
USGI Medical, GI Dynamics, Spatz FGIA, Allurion Tech- www.govinfo.gov/content/pkg/CFR-2012-title21-vol8/pdf/CFR-2012-
title21-vol8-part803.pdf. Accessed July 5, 2020.
nologies, Elira Therapeutics, Endo Tools Therapeutics, Ni-
12. Sullivan S, Stein R, Jonnalagadda S, et al. Aspiration therapy leads to
tinotes Surgical, Obalon Therapeutics, and Phenomix weight loss in obese subjects: a pilot study. Gastroenterology
Sciences; researcher for Aspire Bariatrics, Obalon Thera- 2013;145:1245-52.
peutics, Allurion Technologies, Elira Therapeutics, Finch 13. Thompson CC, Abu Dayyeh BK, Kushner R, et al. Percutaneous gas-
Therapeutics, and ReBiotix; stock warrants from Elira trostomy device for the treatment of class II and class III obesity: re-
sults of a randomized controlled trial. Am J Gastroenterol 2017;112:
Therapeutics; food and beverage compensation from Bos-
447-57.
ton Scientific and Novo Nordisc. All other authors dis- 14. Nyström M, Machytka E, Norén E, et al. Aspiration therapy as a
closed no financial relationships. tool to treat obesity: 1-to 4-year results in a 201-patient multi-
center post-market European registry study. Obes Surg 2018;28:
1860-8.
REFERENCES 15. Thompson CC, Abu Dayyeh BK, Kushnir V, et al. Aspiration therapy for
the treatment of obesity: 4-year results of a multicenter randomized
1. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prev- controlled trial. Surg Obes Relat Dis 2019;15:1348-54.
alence of overweight and obesity in children and adults during 1980- 16. Wilson EB, Noren E, Gruvaeus J, et al. A comparative 100-participant 5-
2013: a systematic analysis for the Global Burden of Disease Study year study of aspiration therapy versus Roux-en-Y gastric bypass: 2nd
2013. Lancet 2014;384:766-81. and 3rd year results. Surg Obes Relat Dis 2018;14:S15.
2. Heymsfield SB, Wadden TA. Mechanisms, pathophysiology, and man- 17. Machytka E, Turro R, Huberty V, et al. Aspiration therapy in super obese
agement of obesity. N Engl J Med 2017;376:254-326. patientsdpilot trial. Gastroenterology 2016;150(Suppl 1):S822-3.
3. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a sys- 18. ASGE Training Committee 2013-2014; Enestvedt BK, Jorgensen J, Sed-
tematic and clinical review. JAMA 2014;311:74-86. lack RE, et al. Endoscopic approaches to enteral feeding and nutrition
4. Bray GA, Fruhbeck G, Ryan DH, et al. Management of obesity. Lancet core curriculum. Gastrointest Endosc 2014;80:34-41.
2016;387:1947-56. 19. Singh A, Gelrud A. Adverse events associated with percutaneous
5. ASGE Bariatric Endoscopy Task Force and ASGE Technology Commit- enteral access. Gastrointest Endosc Clin North Am 2015;25:71-82.
tee; Abu Dayyeh BK, Kumar N, Edmundowitz SA, et al. ASGE Bariatric 20. Alshafei A, Deacy D, Antao B. Risk factors for a persistent gastrocutane-
Endoscopy Task Force systematic review and meta-analysis assessing ous fistula following gastrostomy device removal: a tertiary center
the ASGE PIVI thresholds for adopting endoscopic bariatric therapies. experience. J Indian Assoc Pediatr Surg 2017;22:220-5.
Gastrointest Endosc 2015;82:425-38. 21. Mitchell JE, King WC, Pories W, et al. Binge eating disorder and medical
6. Sullivan S. Aspiration therapy for obesity. Gastrointest Endosc Clin comorbidities in bariatric surgery candidates. Int J Eat Disord 2015;48:
North Am 2017;27:277-88. 471-6.
342 GASTROINTESTINAL ENDOSCOPY Volume 93, No. 2 : 2021 www.giejournal.orgJirapinyo et al ASGE PIVI thresholds for aspiration therapy SUPPLEMENTARY TABLE 1. Search strategy Database Search strategy MEDLINE (AspireAssist[tiab] OR “aspiration therapy”) EMBASE Aspireassist OR “Aspiration Therapy” Web of Science (AspireAssist) or (“Aspiration Therapy”) www.giejournal.org Volume 93, No. 2 : 2021 GASTROINTESTINAL ENDOSCOPY 342.e1
You can also read