Anesthetic Management of a Patient With Mast Cell Activation Syndrome: A Case Study - AANA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Anesthetic Management of a Patient With Mast
Cell Activation Syndrome: A Case Study
Sarah E. Giron, PhD, CRNA
Crystal D. Trinooson, MS, CRNA
Rana Movahedi, MD
Mast cell activation syndrome (MCAS) is a relatively its clinical presentation in the perioperative setting,
new diagnosis for a constellation of symptoms with and anesthetic considerations specific to MCAS, the
sometimes devastating results for patients. A 40-year Certified Registered Nurse Anesthetist will be better
old woman with MCAS underwent arthroscopic repair equipped to effectively manage the complex require-
of her right shoulder, with successful anesthetic man- ments of this patient population.
agement. This case report discusses the basic immu-
nologic physiology surrounding this syndrome, myr-
iad medications often used by this patient population, Keywords: Anesthesiology, cell stabilization, immune
and the anesthetic management of this patient. With hypersensitivity, mast cell activation syndrome, trigger
additional knowledge of this disorder, exposure to avoidance.
M
ast cell activation syndrome (MCAS) is tinnitus, temporomandibular joint (TMJ) stiffness and
a rare disorder involving the idiopathic pain, spontaneous pneumothoraces, and anxiety disorder.
activation of morphologically normal mast Known allergies included ranitidine, hydromorphone,
cells leading to recurrent episodic symp- acetaminophen/hydrocodone, penicillins, lamotrigine,
toms of immunologic activation or ana- trifluridine, risperidone, topiramate, latex, soy, eggplant,
phylaxis.1,2 This syndrome is characterized by a nonspecific gluten, and milk. Preoperative medical clearance had
clinical presentation involving some combination of integu- been provided by the patient’s primary medical specialist
mentary, gastrointestinal, cardiovascular, pulmonary, endo- with a detailed note of recommendations presented by
crine, hematologic, and/or neuropsychiatric symptoms that her allergist (Table 1).
often impedes early diagnosis and treatment.3 The patient’s surgical history included a septoplasty,
Patients with MCAS presenting for surgery and anes- turbinectomy, and multiple orthopedic procedures; she
thesia are at high risk of hypersensitivity reactions trig- had also received numerous sympathetic nerve blocks
gered by anesthetic agents, analgesics, neuromuscular and epidural injections for management of chronic pain.
blocking agents, anti-infective agents, environmental The patient reported no adverse effects following general
factors, surgical trauma, and psychological stress. The anesthesia aside from mild nausea and inadequate pain
primary goal of anesthetic management in such patients control, and there was no known history of familial
is to prevent mast cell degranulation.4 anesthesia-related complications.
This case report presents the successful perioperative The patient’s current home medication regimen in-
management of a patient with known MCAS presenting cluded oxycodone (15 mg every 4 hours), hydrocortisone
for orthopedic surgery. The physiology and diagnostic cri- (20 mg daily), tizanidine, erythromycin, lorazepam, lina-
teria for MCAS are briefly reviewed; the clinical summary clotide, naloxegol oxalate, ondansetron, rifaximin, and
is evaluated, and a review of available recommendations cromolyn; inhaled fluticasone and budesonide; topical
for treatment and anesthetic management is presented. 2.5% lidocaine-2.5% prilocaine cream, tretinoin cream,
and triamcinolone cream. Sumatriptan, ibuprofen, and
Case Summary albuterol were taken as needed. In accordance with her
A 40-year old woman (82 kg, 180 cm) with right shoul- allergist’s recommendations, the patient took 20 mg of
der instability presented to the preoperative holding area cetirizine, 10 mg of famotidine, 200 mg of cromolyn, 50
for a right shoulder arthroscopy with repair. Her medical mg of diphenhydramine, and 20 mg of prednisone on
history included MCAS, Ehlers-Danlos syndrome (EDS), the morning of surgery. Despite known hypersensitiv-
postural orthostatic tachycardia syndrome (POTS), gas- ity to ranitidine, famotidine was recommended by the
troparesis, esophagitis, migraine, osteopenia, cervical patient’s allergist because it had been safely adminis-
spine disk herniation (C5-6, C6-7), lumbar spine disk tered to the patient during outpatient treatment and on
herniation (L4-5), exercise- and stress-induced asthma, past admissions. (This type of combined antimediator
www.aana.com/aanajournalonline AANA Journal August 2021 Vol. 89, No. 4 307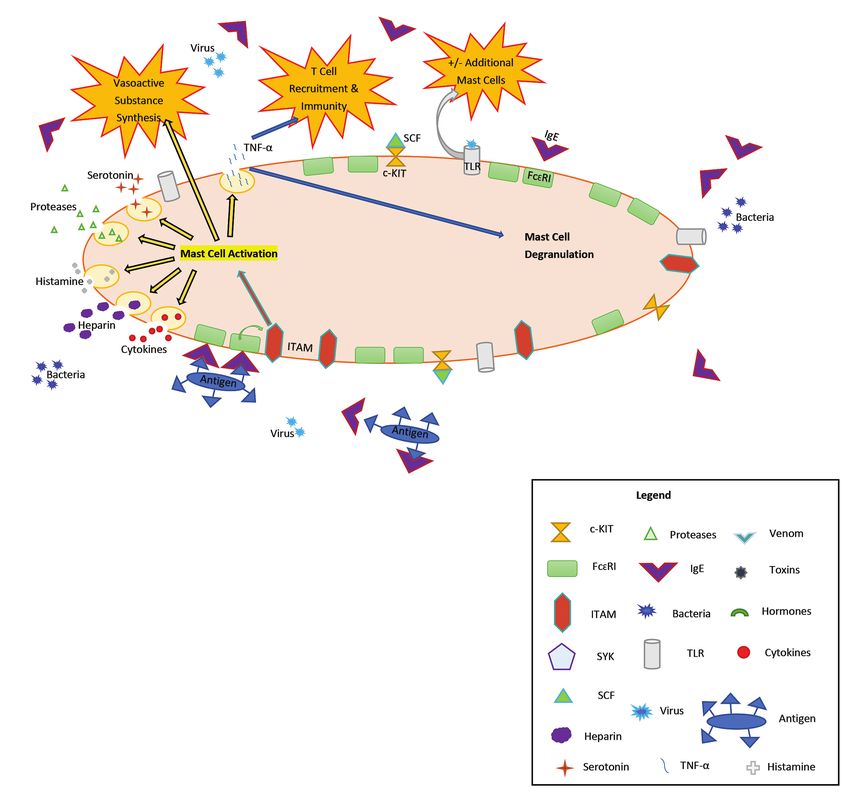
approach using H1- and H2-histamine receptor antago- Timing Intervention
nism and mast cell stabilization is a mainstay of MCAS Day before surgery •C etirizine, 20 mg in morning and 20 mg
management and will be examined in greater detail in at night
the Discussion.1,2) Preoperative laboratory results were • Famotidine, 10 mg in morning and 10
mg at night
within normal limits, and a careful review of diagnostic • Cromolyn, 200 mg 4 times a day
radiologic tests, electrocardiogram, and echocardiogram • Prednisone, 20 mg in morning and 20
revealed no abnormal findings. mg at night
On physical examination, the patient was found to be Day of surgery Two hours before surgery:
agitated but alert and fully oriented; her vital signs were • Cetirizine, 20 mg
within normal limits. Palpation of peripheral pulses dem- • Famotidine, 20 mg
onstrated a regular heart rate; auscultation found all lung • Prednisone, 20 mg
fields clear with no adventitious breath sounds. Results of • One hour before: Diphenhydramine, 50
mg IV (or orally unless contraindicated)
the airway examination revealed a small mouth opening
Intraoperative (after As needed:
of 2 finger breadths, limited atlanto-occipital range of oropharyngeal • Epinephrine IV, subcutaneous
motion, Mallampati score of 3, and ability to protrude the intubation) • Albuterol, ipratropium nebulized
mandible despite a history of TMJ symptoms. Dentition • Vasoactive agents: dopamine,
was grossly intact with no loose teeth or removable dental norepinephrine, vasopressin
appliances reported. According to the patient, she had had • Diphenhydramine, 50 mg IV
nothing to eat or drink for more than 8 hours. • Methylprednisolone, 125 mg IV/IM
Following a careful review of allergist recommenda- every 6 h as needed
• Muscle relaxants, NSAIDs, morphine,
tions and a thorough discussion of anesthetic risks, and codeine should be used with caution
benefits, and options with the patient, informed consent • Avoid vancomycin
was obtained for an interscalene block with continuous Postoperative • Cetirizine, 20 mg twice daily
infusion catheter and a general anesthetic. A 20-gauge • Famotidine, 10 mg orally twice daily
peripheral intravenous (IV) line was inserted in the • Prednisone, 20 mg orally twice
daily (can discontinue after day 1 if
left antecubital vein, oxygen (O2) therapy was initiated hemodynamically stable)
through a nasal cannula, and standard noninvasive moni- • Cromolyn, 200 mg 4 times daily
tors were applied to the patient. Before the interscalene • Diphenhydramine, 50 mg orally every 6
h as needed
block and continuous infusion catheter placement, the
procedure site was confirmed to be the right side and Table 1. Sample of Patient Instructions From Allergist
procedural sedation was administered; total doses were Managing MCAS
Abbreviations: IM, intramuscular; IV, intravenous; MCAS, mast cell
4 mg IV of midazolam and 50 μg IV of fentanyl. (The
activation syndrome; NSAIDs, nonsteroidal anti-inflammatory drugs.
administration of benzodiazepines as a premedication
before general anesthesia may confer some protection
against anxiety-mediated mast cell degranulation. This ated using 8 L of O2 via face mask. A smooth IV induction
benefit must be evaluated against the risk of heavy was accomplished using 2% lidocaine, 100 mg IV; propo-
sedation, particularly in those patients receiving early- fol, 200 mg IV; and rocuronium, 70 mg IV per surgeon
generation antihistamines.5) request. (Recent studies have indicated that amides gener-
Sterile preparation of the operative side was achieved ally have a low incidence of adverse reactions in patients
with chlorhexidine topical solution, which was well with mast cell disorders. Lidocaine, in particular, is well-
tolerated. A SonoLong Echo E-Cath (Pajunk) 18-gauge tolerated and may even modulate immune responses.5)
catheter was inserted with continuous ultrasound guid- Following loss of lash reflex, the eyes were secured with
ance for nerve localization. Then 0.5% ropivacaine, 20 paper tape, and manual mask ventilation was easily
mL, was injected, with intermittent aspiration during achieved with low peak airway pressures.
administration. Ropivacaine was selected for its onset, With use of in-line cervical spine stabilization, a video-
analgesic duration, and provision of differential sensory- assisted laryngoscope (C-Mac, Karl Storz) was utilized.
motor blockade. (Like other amide local anesthetics, A 7.0-mm oral endotracheal tube was placed, with a
ropivacaine is generally well tolerated and less likely Cormack-Lehane grade 1 view; bilateral breath sounds
to contribute to mast cell activation than ester local were auscultated, end-tidal carbon dioxide was noted,
anesthetics.5,6) No blood was aspirated, and no pain or and the tube was secured at 21 cm at the teeth. General
paresthesias were reported on injection. There were no anesthesia was maintained with 60% fraction of inspired
symptoms of intraneural or IV injection and the patient oxygen (Fio2) and 1.9% to 2.2% sevoflurane, using volume
tolerated the procedure well. control ventilation. Clindamycin, 900 mg IV, was initiated
The patient was taken to the operating room and stan- as a preincision antibiotic. A 20-gauge left radial arterial
dard monitors were applied. The patient was preoxygen- line (Arrow, Teleflex) was placed with sterile technique in
308 AANA Journal August 2021 Vol. 89, No. 4 www.aana.com/aanajournalonlineone attempt, and a transparent dressing was applied. ranging from 16 to 18 cm H2O throughout the case, and
The patient was then positioned in the left lateral a grossly normal expiratory plateau of the end-tidal cap-
decubitus position with an axillary roll and vacuum- nography waveform.
packed bean bag for immobilization. Head and neck On surgical closure, ondansetron (4 mg IV) was ad-
stabilization and neutrality were maintained throughout. ministered and 3/4 train-of-four (TOF) twitches were
(Immobilization of the cervical spine during endotrache- measured with a left ulnar peripheral nerve stimulator.
al intubation and patient positioning is a critical tenet of Sugammadex, 180 mg (2.2 mg/kg) IV, was administered
anesthesia management for patients with known cervical to reverse neuromuscular blockade. Before tracheal
spine defects and for those whose comorbid connective extubation, 4/4 TOF twitches and sustained 5-second
tissue disease places them at high risk of atlantoaxial and tetanus at 50 Hz were exhibited, spontaneous adequate
craniocervical instabilities.7 Recent studies have found a tidal volumes and respiratory rate were present, the
possible association between connective tissue diseases, oropharynx was suctioned, and the patient was able to
particularly joint hypermobility variants, and mast cell follow commands. After extubation criteria were met, the
disorders.8 Furthermore, if cervical manipulation con- patient was extubated easily and was transported to the
tributes to the local activation of afferent neurons, the postanesthesia care unit (PACU) in stable condition with
release of inflammatory neuropeptides such as substance 6 L of O2 via face mask. Total operative time was 2 hours,
P, calcitonin gene-related peptide, vasoactive intestinal 9 minutes to complete a right shoulder hemiarthroplasty
polypeptide, and pituitary adenylate cyclase activating with arthroscopic débridement. The total estimated
polypeptide can stimulate activation and degranulation blood loss for the case was 50 mL; total IV fluid adminis-
of adjacent mast cells.9) tered was 1,000 mL of 0.9% sodium chloride.
A stress dose of methylprednisolone, 125 mg IV, On arrival to the PACU, the patient was noted to
was administered; a surgical pause was completed; and be awake and conversing clearly; bilateral lungs were
surgery commenced without issue. (The prophylactic auscultated to be clear, vital signs remained stable, and
administration of corticosteroids can help modulate the patient denied pain or nausea. Following surgical
immune responses to perioperative mast cell activation assessment of the operative arm for motor and sensory
triggers by decreasing mediator release, producing pulmo- function, a continuous infusion of 0.2% ropivacaine was
nary vasoconstriction, reducing bronchial hyperreactivity, initiated through the right interscalene catheter for post-
inhibiting inflammatory cell recruitment, and mitigating operative pain control at a rate of 4 mL/h. Early recovery
bronchial smooth muscle contraction.10 Furthermore, the was uneventful, and the patient was later discharged
administration of stress doses of corticosteroids is known home without clinical evidence of mast cell activation
to mitigate the risk of adrenal insufficiency associated during her perioperative course. However, due to subop-
with long-term corticosteroid use.5,10) timal pain control later in the hospital course, the patient
Approximately 30 minutes after incision, the patient had a longer than anticipated length of stay.
was repositioned to the supine position for surgical expo-
sure and prophylaxis against pressure-mediated mast cell Discussion
activation. Again, cervical spine stability was maintained Mast cells are a critical component of the immune
and adhesive goggles were applied over the paper tape for response, playing a major role in immunoglobulin E
additional ocular protection. (Despite the protection it (IgE)–mediated acute hypersensitivity and anaphylactic
confers against pressure-mediated injury and immune ac- reactions.8 They also help promote the expression of
tivation, intraoperative position alteration can be a criti- immunoregulatory proteins and serve a complex role in
cal event because of the risk it poses for friction-mediated delayed hypersensitivity.8,14 Mast cells originate in the
mast cell degranulation as well as orthostatic intolerance, bone marrow from the same stem cells that give rise to
particularly in patients such as this with a comorbid di- basophils; they then travel through the systemic blood
agnosis of POTS.11,12 A series of studies have examined and lymphatic circulation in a precursor form before
the role of mast cell activation in cutaneous flushing settling in the peripheral tissues and differentiating. The
during POTS episodes and have even posited a triad proliferation and maturation of mast cells are thought
relationship between POTS, EDS, and MCAS.13 Further to be influenced by a number of cytokines (small pro-
research is needed to clarify this potential relationship teins used by the immune system in cellular signaling),
and the clinical impact on diagnosis and treatment of particularly stem cell factor (SCF), which binds the
each syndrome.) The patient tolerated positioning well CD117 tyrosine kinase transmembrane receptor (c-KIT)
with no clinical evidence of tachycardia or autonomic to promote “homing” of immature mast cells from bone
dysfunction; electrocardiography showed normal sinus marrow and peripheral blood to specific tissues.8,15 The
rhythm throughout the case, vital signs were stable, and local environments of specific tissues interact with the
lung compliance was maintained as evidenced by ade- immature mast cells to promote unique phenotypical
quate measured tidal volumes, peak inspiratory pressures traits in the mature mast cells that will support various
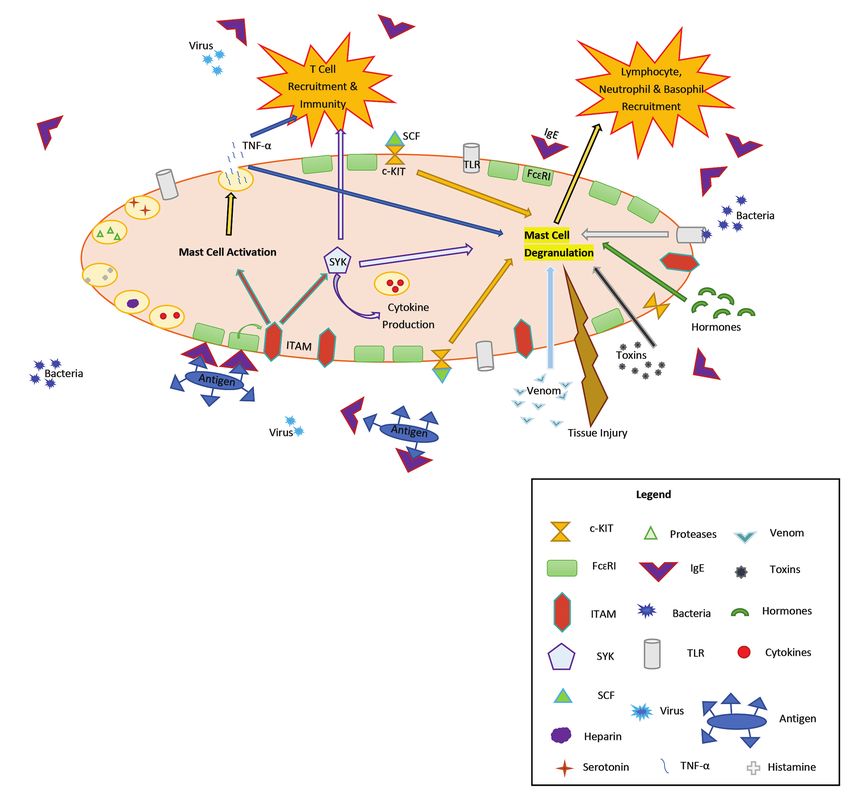
www.aana.com/aanajournalonline AANA Journal August 2021 Vol. 89, No. 4 309Figure 1. Mast Cell Activation
Abbreviations: c-KIT, CD117 tyrosine kinase transmembrane receptor; FcεRI, Fc ε-receptor; IgE, immunoglobulin E; ITAM,
immunoreceptor tyrosine-based activation motif; SCF, stem cell factor; SYK, spleen tyrosine kinase; TLR, toll-like receptor; TNF-α, tumor
necrosis factor-α.
functions, including immune mediation, angiogenesis, vation16,18,19 (Figure 1). This sequence, immunoreceptor
tissue healing, blood-brain barrier support, and phagocy- tyrosine-based activation motif (ITAM), provides signal-
tosis.8,16,17 The influence of certain tissues on the traits ing capability for the FcεRI.19 Furthermore, the β subunit
of homed mast cells is a current topic of interest in the of FcεRI plays an important role in stabilizing the antigen-
potential relationship between EDS and MCAS.8 IgE complex to enhance the positive feedback immune
The surface of mature mast cells is heavily coated response.20 The activation of the ITAM on the β subunit
with Fc ε-receptors (FcεRI) that preferentially bind the stimulates spleen tyrosine kinase (SYK) to augment mast
crystallizable fragment regions of antibodies and have a cell degranulation, a process by which mast cells release
high affinity for IgE at their α subunit.18 When IgE binds histamine. Increased SYK then stimulates cytokine pro-
with an antigen at the α subunit of FcεRI, the β and γ duction and (via downstream second messengers) re-
subunits activate a special sequence contained in their cruits T-cell immunity19,20 (Figure 2). This leads to an
cytoplasm to trigger an immune-mediated mast cell acti- unchecked cascade of immune-mediated hypersensitivity
310 AANA Journal August 2021 Vol. 89, No. 4 www.aana.com/aanajournalonlineFigure 2. Mast Cell Degranulation Abbreviations: c-KIT, CD117 tyrosine kinase transmembrane receptor; FcεRI, Fc ε-receptor; IgE, immunoglobulin E; ITAM, immunoreceptor tyrosine-based activation motif; SCF, stem cell factor; SYK, spleen tyrosine kinase; TLR, toll-like receptor; TNF-α, tumor necrosis factor-α. responses ranging from local tissue edema, headache, attenuate the response of mature mast cells.15 Although diarrhea, urticaria, and cutaneous flushing to vascular mast cells play an integral role in immune-mediated pro- permeability, widespread vasodilation, bronchoconstric- cesses, they may also degranulate in direct response to tion, and cardiovascular collapse.11,14 toxins, venoms, hormones, and physical stimuli such as Toll-like receptors (TLRs) on the mast cell surface thermal or friction tissue injury1,22 (see Figure 2). may cause a direct immune response if bound to bacteria Mast cell activation triggers the exocytotic release of or viruses. Further investigative work on the unique role presynthesized inflammatory mediators from the cyto- of TLRs has demonstrated that they use cell signaling plasm of the cell, including proteases, heparin, cytokines, to either augment or inhibit mast cell degranulation in tumor necrosis factor-α (TNF-α), histamine, and sero- various types of peripheral mast cells.21 The binding of tonin.16,17,23 Mast cell activation also triggers synthesis SCF to c-KIT also stimulates a series of signal transduc- of platelet activating factor, prostaglandins, leukotrienes, tion pathways that activate mast cell degranulation and thromboxanes, and other vasoactive substances.16,17,24 www.aana.com/aanajournalonline AANA Journal August 2021 Vol. 89, No. 4 311
The release of TNF-α, in particular, triggers a powerful cell activation of unknown etiology despite a full diag- positive inflammatory cascade because of its stimulation nostic evaluation; these include idiopathic anaphylaxis, of T-cell immunity and its direct potentiation of addi- idiopathic angioedema, and MCAS.2,3 As with secondary tional mast cell degranulation14,16 (see Figure 1). The disorders, idiopathic syndromes are generally character- classic example of this cascade is the anaphylactic reac- ized by normal proliferation and histologic appearance tion, whereby FcεRI-IgE binding of an allergen potenti- of mast cells.2 However, idiopathic causes are associated ates massive mast cell degranulation with subsequent with markedly heightened mast cell activity; mast cells lymphocyte, neutrophil, and basophil recruitment.16 The may degranulate in response to even a mild stimulus.6,11,25 resultant release of histamines, prostaglandins, and other MCAS is a disorder of chronic mast cell degranulation that vasoactive mediators contributes to an acute array of car- has been described diagnostically only within the past diovascular, respiratory, integumentary, neuromuscular, decade.2 Diagnostic characteristics of MCAS include all of and gastrointestinal symptoms.11 the following: Mast cell disorders are often characterized as primary, • Recurrent symptoms of mast cell activation in at secondary, or idiopathic in accordance with their patho- least 2 distinct organ systems (integumentary involve- physiology. Primary disorders are associated with a defect ment is common).1,8,25 in mast cell morphology, proliferation, or signaling. • Measurably elevated immune mediator activity They generally involve c-KIT mutations (with or without within 4 hours of mast cell degranulation symptoms in at concomitant genetic mast cell alteration) and abnormal least 2 episodes,25 with elevation of serum tryptase values mast cell proliferation and activation; these conditions 20% above baseline the marker most specific for mast cell include mastocytosis, primary monoclonal MCAS, mast activation. cell sarcoma, and chronic eosinophilic leukemia. Because • Measurable reduction in symptoms in response to of the unique role of c-KIT in cellular propagation and mass cell membrane stabilizers or other immune me- migration, it is considered a proto-oncogene; any altera- diator blockade (cromolyn, antihistamines, leukotriene tion in its function may contribute to the development inhibitors).8,25 of malignancy.3,11,15,25,26 Additionally, SYK may play a Laboratory analysis of elevated immune mediator substantial role in the development of lymphomas.20 activity has been historically difficult because mast Clonal mast cell disorders may respond to cytoreduc- cells may be involved in the activation of a multitude tive therapies such as interferon-α (IFN-α), cladribine, of nonspecific mediators (eg, histamine and its urinary hydroxyurea, or tyrosine kinase inhibitors; hematopoietic metabolites are also indicative of basophil involvement).9 stem cell transplant is an additional treatment option for Furthermore, many of the serum and urine mediators patients with mast cell malignancy.25,26 Because primary that may serve as specific indexes of mast cell activa- disorders are characterized by the proliferation of clonal tion are unstable ex vivo.1,24 Unlike mastocytosis, MCAS mast cells, they may be more readily diagnosed using lab- typically does not present with chronically heightened oratory analysis. Differential diagnosis is often confirmed baseline tryptase levels.6,25 Elevated 24-hour urinary with bone marrow aspiration or biopsy of cutaneous metabolites of mast cell mediators (histamine, prosta- lesions.9 Patients with primary disorders often present glandins, leukotrienes) are less specific indicators of mast with periodic symptomatic mast cell degranulation; trig- cell activation; they may also be measurably elevated in gering agents are typically unknown and symptoms may the setting of basophil activation, inflammatory bowel include cutaneous flushing, gastrointestinal symptoms, disease, and histamine intolerance due to exogenous his- profound hypotension, and cardiovascular collapse.3,25 tamine toxicity or reduced diamine oxidase function.11,28 Mast cell stabilization agents, leukotriene inhibitors, and Because of the nonspecific nature of presenting symp- antimediator agents (epinephrine and antihistamines) are toms and the comparatively recent introduction of diag- a mainstay of symptom management for all classifications nostic criteria, the actual incidence of MCAS is not widely of mast cell disease.27 known. A recent combined retrospective and prospective Secondary disorders are associated with extrinsic cohort study evaluated the population characteristics of activation of healthy mast cells; they often involve un- patients with MCAS. The findings indicated that MCAS is checked adaptive inflammatory responses (IgE- and most prevalent in white females whose presenting symp- non-IgE–mediated reactions, inflammation, and infec- toms commonly included fatigue, diffuse pain, presynco- tion) and include immediate hypersensitivity reactions pal or syncopal episodes, and headache. Unfortunately, and chronic autoimmune urticaria.3,25 Isolated secondary the median time from self-reported onset of symptoms to mast cell disorders generally respond to avoidance of diagnosis was 30 years.29 Diagnosis may be complicated known triggers and management of underlying infection. by the complex and nonspecific nature of the symptoms, However, secondary causes may be concomitant with the episodic nature of clinical presentation, and the lack primary or idiopathic causes.2,25 of reliable serologic indicators outside the immediate Idiopathic disorders are associated with increased mast flare.30,31 Patients may be markedly disabled during 312 AANA Journal August 2021 Vol. 89, No. 4 www.aana.com/aanajournalonline
Anesthetic
MCAS symptom Treatment considerations
Cardiovascular Emergent: Epinephrine Fluid replacement may be indicated in the setting of massive
Hypotension Prophylactic: vasodilatation and acute refractory hypotension to help
preserve circulating volume. Make emergency medications
Syncope H1-antihistamines
readily available for any anesthetic involving a patient with
Tachycardia Antileukotrienes MCAS.
Lightheadedness Omalizumab
Angina pectoris Nitrates
Calcium channel blockers
Venom immunotherapy if appropriate
Cutaneous H1- and H2-antihistamines Emergent intubation may be indicated to protect the airway
Flushing Ketotifen in patients with angioedema.
Pruritus Aspirin or NSAIDsa Have fiberoptic bronchoscopy and/or video laryngoscopy
readily available to avoid airway trauma or further edema.
Urticaria
Angioedema
Gastrointestinal Local thermal treatment Localized abdominal application of heat has been shown
Cramping H2-antihistamines to activate heat receptors that competitively interfere with
nociceptive pain.35 However, avoid systemic hyperthermia,
Diarrhea Cromolyn
which can trigger mast cell degranulation.
Nausea/vomiting Proton pump inhibitors
GERD Glucocorticoids
Colicky gastric pain Scopolamine
Biliary colic Polyethylene glycol
Respiratory Antileukotrienes When possible, use MAC anesthesia to avoid airway
Throat swelling Inhaled corticosteroids for asthma manipulation. Have advanced airway equipment and
breathing treatments readily available.
Wheezing
Shortness of breath
Musculoskeletal Calcium/vitamin D supplementation Avoid tourniquets when appropriate and possible. Treat
Bone pain Bisphosphonates pain with previously used modalities or per specialist
recommendations.
Arthralgia Aspirin or NSAIDsa
Osteoporosis Opioidsa
Muscle pain H1-antihistamines
Neuropathic pain Avoid massage
Fibromyalgia
Neurologic Acetaminophen or NSAIDs Administer adequate perioperative fluids. Start home
Migraine Triptans medications as soon as possible.
Trigeminal neuralgia Potassium supplementation
Genitourinary Scopolamine Avoid meperidine.
Renal colic
Oropharyngeal H1-antihistamines Carefully and gently manipulate oropharynx during intubation.
Sore throat Use MAC when appropriate.
Table 2. Medications Used for Treatment of MCAS
Abbreviations: GERD, gastroesophageal reflux disease; MAC, monitored anesthesia care; MCAS, mast cell activation syndrome;
NSAIDs, nonsteroidal anti-inflammatory drugs.
aAssess for tolerability before administering.
episodes, leading to a delay in seeking treatment; by the which must be continued perioperatively and incorpo-
time they present for care, their baseline tryptase values rated into the anesthetic plan (Table 2). With a dearth of
are often within normal limits. Furthermore, emergency randomized controlled studies on which to base clinical
medical treatment during acute anaphylaxis may focus decisions, the anesthetist is forced to rely on case reports
on symptom management and identification of triggering and observational studies in the MCAS population. To
agents without focus on a global diagnosis.4,32 date, no therapeutic trials exist and no guidelines are
The anesthetic management of the patient with MCAS available on the anesthetic management of patients with
spans a vast range of clinical symptoms and incorporates MCAS.26,27,32,33
the basic therapeutic considerations of this disease: (1) The avoidance of known mast cell activation triggers
highly individualized care to avoid known triggers and is one of the primary considerations in the perioperative
(2) prevention of mast cell mediator proliferation.9,33 care of the patient with MCAS. A detailed history is para-
Patients typically are receiving a plethora of medications, mount to safe anesthetic management, as well as close
www.aana.com/aanajournalonline AANA Journal August 2021 Vol. 89, No. 4 313Drugs with patient in the past, with no unfavorable sequelae.
Drug class high risk Alternativesa Pain is also a known trigger of mast cell activation.
Anesthetics Methohexital Propofol Therefore, an adequate analgesic plan must be discussed
Phenobarbital Ketamine with the patient and surgical service preoperatively and
Thiopental Etomidate implemented during planned procedures. Remifentanil,
Midazolam
alfentanil, fentanyl, oxycodone and ketamine are rec-
TIVA/sevoflurane26
ommended analgesics; morphine and codeine should
Muscle relaxants Atracurium Cisatracurium
be avoided if possible due to their impact on me-
Mivacurium Vecuronium
diator release.9,26,32,34 The anesthetist should be aware
Rocuroniumb Pancuronium
that opioids and nonsteroidal anti-inflammatory drugs
Antibiotics Cefuroxime Agents administered
in previous therapies (NSAIDs) can also trigger MCAS events, so a thorough
Fluoroquinolones
Vancomycin with no reaction preoperative assessment and plan for pain control are
Anticonvulsants Carbamazepine Clonazepam
essential.9,26 In this case report, the patient underwent a
Topiramate regional nerve block with catheter placement for periop-
Opioids Meperidine Remifentanil erative pain control to limit the administration of narcotic
Morphine Alfentanil analgesics. The intraoperative and immediate postop-
Fentanyl erative periods were successfully managed with a mul-
Codeine
Oxycodone
timodal analgesic plan and continuous infusion through
Other analgesics Acidic NSAIDs (eg, Acetaminophenb
acetaminophen and the regional block catheter. However, due to suboptimal
ibuprofen)b pain control later in the hospital course, the patient had
Local anesthetics Articaine Amides such as a longer than anticipated length of stay.
Tetracaine bupivacaine5 Highly attentive hemodynamic management is foun-
Procaine dational to anesthetic management of all patients. There
Plasma Hydroxyethyl starch Albumin are currently no consensus data for specific perioperative
substitutes 0.9% Normal saline
Lactated Ringer’s monitoring in patients with MCAS, but the use of arterial
solution blood pressure monitoring or noninvasive continuous he-
Cardiovascular ACE inhibitors Angiotensin II blockers modynamic devices may provide early awareness of hypo-
drugs β-Blockers Calcium channel tension due to mast cell degranulation or other intraopera-
blockers
Ivabradine tive factors. Hemodynamic instability should be managed
aggressively with vasoactive support; epinephrine is the
Table 3. Drugs Associated With High Risk of Release
of Mediators From Mast Cells and Their Alternatives agent of choice if mast cell involvement is suspected.11
Abbreviations: ACE, angiotensin-converting enzyme; NSAIDs, Because of the risk of mast cell degranulation with ex-
nonsteroidal anti-inflammatory drugs; TIVA, total intravenous tremes of temperature, normothermia should be carefully
anesthetic. maintained.1 Core temperature monitoring at the distal
a Any injectables containing ethanol should be avoided.4
b Assess for tolerability before administering. esophagus, nasopharynx (at appropriate depth) or pulmo-
(Adapted from: Molderings et al.33)
nary artery (if pulmonary artery access is warranted) may
provide the most reliable data to assist in maintaining nor-
mothermia.36,37 If nasopharyngeal monitoring is employed,
collaboration with any allergist or immunology specialist it should be used with great care to mitigate the risk of local
involved in the patient’s care. Continuation of baseline trauma and potential mast cell activation. Alternatively, a
therapy of antimediators, mast cell stabilizing agents, core approximate site such as the bladder may be used.36
and leukotriene inhibitors is critical for safe anesthetic Skin temperature monitoring should be used with caution
management.1 Premedication with histamine antagonists because of the potential for unreliable data.
and corticosteroids may be warranted; close consultation The nature of symptoms of mast cell activation episodes
with the patient’s immunologist will help provide clini- often precludes early identification in the perioperative
cal guidance for preoperative optimization and manage- setting. Headache, loss of concentration, peripheral vasodi-
ment.1,5 Unless there is a known history of hypersensitiv- lation and cutaneous flushing, urticaria, and gastrointesti-
ity reaction during a prior anesthetic, prescreening with nal symptoms are often present in mild mast cell degranu-
a skin test is not recommended, but obtaining a baseline lation events.1,2 These events may be difficult to identify
tryptase level may be helpful.32 The patient in this case when the patient is under general anesthesia. However,
reported a constellation of food allergies, which were ongoing cutaneous assessment may help promote early
easily avoided; latex and penicillin use was avoided peri- identification of urticaria, flushing, and rashes if surgical
operatively, and 900 mg of clindamycin was administered positioning and draping allows. Attentive monitoring of
before the incision. Of note, patient records indicated peak airway pressure and lung compliance measures is also
that clindamycin had been safely administered to the essential for early identification and treatment of airway
314 AANA Journal August 2021 Vol. 89, No. 4 www.aana.com/aanajournalonlineinvolvement, as is chest auscultation, if feasible.2 in treatment if the event is triggered before IV access
Many aspects of surgery induce mast cell medi- has been established.11 Placement of a secure airway is
ator release, as do common anesthetic medications. paramount if not already in place at the time of the ana-
Anesthesia, extreme temperatures, psychological stress phylactoid reaction; inhaled β2-agonists may confer some
or anxiety, pain, mechanical trauma (including applica- benefit as a secondary approach.5,11,33 Fluid administra-
tion of tourniquets), friction injury (often associated tion is also a critical aspect of anaphylaxis management.
with positioning or adhesive placement and removal), When hemodynamic stability has been achieved, mea-
ischemia-reperfusion injury, and excessive skin pressure surement of serum tryptase level is of diagnostic benefit if
can all activate mast cell mediators.9,27,32 A summary of collected within 30 to 120 minutes after the event.5
common anesthetic drugs that activate mast cell media- This case exemplifies the careful history taking, com-
tors are listed in Table 3. Because many of the agents as- prehensive physical evaluation, interdisciplinary commu-
sociated with anesthetic management can induce mast nication, and multimodal anesthetic management needed
cell activation, current literature recommends premedi- to avoid mast cell activation in a patient with MCAS.
cating with an antihistamine and a corticosteroid.9,26,32 Further study is indicated to identify additional serologic
Both a forced warm air blanket and fluid warmer were markers of mast cell activation, as the limited diagnostic
utilized to maintain a stable normothermic state and to window and nonspecific nature of tryptase and urine me-
prevent rapid patient cooling intraoperatively. In this diators impede their diagnostic value. The development
case report, coordination with the surgical team allowed of additional treatment options is also paramount for pro-
for the intraoperative repositioning of the patient to avoid viding ongoing mast cell stabilization, reduction in the
excessive skin pressure and to maximize surgical site ex- scope of mast cell degranulation, and interference with
posure. Positioning changes should always be conducted the physiological activity of released mediators. Global
with careful ongoing attention to hemodynamic status awareness of this disorder and its diagnostic criteria may
due to the risk for friction-mediated mast cell activation aid in earlier diagnosis and treatment.25 Of particular in-
or profound hypotension (possibly immune-mediated in terest to the anesthetist is the development of published
these patients, but orthostatic intolerance may also be guidelines for the anesthetic management of MCAS and
present in those with certain comorbid conditions).13,28 other mast cell disorders.
Preoperative consultation with the surgical team revealed
that anticipated blood loss would be minimal, so no ad- REFERENCES
1. Frieri M, Patel R, Celestin J. Mast cell activation syndrome: a review.
ditional IV access was obtained. Curr Allergy Asthma Rep. 2013;13(1):27-32. doi:10.1007/s11882-
Anaphylaxis can be common in the MCAS population, 012-0322-z
with reactions ranging from cutaneous findings to cardio- 2. Hamilton MJ, Hornick JL, Akin C, Castells MC, Greenberger NJ. Mast
vascular collapse.32 Intravenous or intramuscular (IM) cell activation syndrome: a newly recognized disorder with systemic
clinical manifestations. J Allergy Clin Immunol. 2011;128(1):147-152.
epinephrine, antihistamines, and corticosteroids should doi:10.1016/j.jaci.2011.04.037
be readily available to administer during any anesthetic 3. Akin C, Valent P, Metcalfe DD. Mast cell activation syndrome: pro-
management of the patient with MCAS.26,32 Omalizumab, posed diagnostic criteria. J Allergy Clin Immunol. 2010;126(6):1099-
1104. doi:10.1016/j.jaci.2010.08.035
an IgE antagonist, may also benefit the patient with
4. Afrin LB, Molderings GJ. A concise, practical guide to diagnos-
MCAS in anaphylaxis by preventing IgE-mediated mast tic assessment for mast cell activation disease. World J Hematol.
cell degranulation.26 The anesthetist should also keep in 2014;3(1):1-17.
mind that agents with an increased propensity to cause 5. Carter MC, Metcalfe DD, Matito A, et al. Adverse reactions to drugs
anaphylaxis in the general population (latex, muscle and biologics in patients with clonal mast cell disorders: A work
group report of the Mast Cells Disorder Committee, American
relaxants and antibiotics) need not be avoided in the Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol.
patient with MCAS unless a previously documented reac- 2019;143(3):880-893. doi:10.1016/j.jaci.2018.10.063
tion has occurred.32 6. Ilfeld BM. Continuous peripheral nerve blocks: an update of the
published evidence and comparison with novel, alternative anal-
Furthermore, some antihistamines can cause QT pro- gesic modalities. Anesth Analg. 2017;124(1):308-335. doi:10.1213/
longation, so caution is warranted when administering ANE.0000000000001581
other medications or agents that prolong the QT interval. 7. Henderson FC, Austin C, Benzel E, et al. Neurological and spinal
If anaphylaxis does occur in the patient with MCAS, the manifestations of the Ehlers-Danlos syndromes. Am J Med Genet C
Semin Med Genet. 2017;175(1):195-211. doi:10.1002/ajmg.c.31549
causative agent should immediately be stopped in ac-
8. Seneviratne SL, Maitland A, Afrin L. Mast cell disorders in Ehlers-Dan-
cordance with current recommendations. Antihistamines los syndrome. Am J Med Genet C Semin Med Genet. 2017;175(1):226-
(preferably IV diphenhydramine) and corticosteroids 236. doi:10.1002/ajmg.c.31555
such as methylprednisolone should be administered for 9. Wirz S, Molderings GJ. A practical guide for treatment of pain in
patients with systemic mast cell activation disease. Pain Physician.
the treatment of both mild and severe hypersensitivity re- 2017;20(6): E849-E861.
actions.32-34 Epinephrine is the mainstay of management 10. Bonini M, Usmani OS. Drugs for airway disease. Medicine. 2020;
for anaphylaxis; IV administration is preferred in most 48(5):314-322. doi:10.1016/j.mpmed.2020.02.007
cases, but intramuscular injection may mitigate delays 11. Picard M, Giavina-Bianchi P, Mezzano V, Castells M. Expanding
www.aana.com/aanajournalonline AANA Journal August 2021 Vol. 89, No. 4 315spectrum of mast cell activation disorders: monoclonal and idiopathic 31. Perales Chordá C, Fabregat Nebot S, Moral Moral P, Jarque Ramos
mast cell activation syndromes. Clin Ther. 2013;35(5):548-562. I, Hernández Fernandez de Rojas D. Syncope as a manifesta-
doi:10.1016/j.clinthera.2013.04.001 tion of mast cell activation disorder. Ann Allergy Asthma Immunol.
12. Shibao C, Arzubiaga C, Roberts L, et al. Hyperadrenergic postural 2015;114(2):153-154. doi:10.1016/j.anai.2014.11.019
tachycardia syndrome in mast cell activation disorders. Hypertension. 32. Richter EW, Hsu KL, Moll V. Successful management of a patient
2005;45(3):385-390. doi:10.1161/01.HYP.0000158259.68614.40 with possible mast cell activation syndrome undergoing pulmonary
13. Kohn A, Chang C. The relationship between hypermobile Ehlers- embolectomy: a case report. A A Case Rep. 2017;8(9):232-234.
Danlos syndrome (hEDS), postural orthostatic tachycardia syndrome doi:10.1213/XAA.0000000000000476
(POTS), and mast cell activation syndrome (MCAS). Clin Rev Allergy 33. Molderings GJ, Haenisch B, Brettner S, et al. Pharmacological treatment
Immunol. 2020;58:273-297. doi:10.1007/s12016-019-08755-8 options for mast cell activation disease. Naunyn Schmiedebergs Arch
14. Biedermann T, Kneilling M, Mailhammer R, et al. Mast cells con- Pharmacol. 2016;389(7):671-694. doi:10.1007/s00210-016-1247-1
trol neutrophil recruitment during T cell-mediated delayed-type 34. Konrad FM, Schroeder TH. Anaesthesia in patients with mastocytosis.
hypersensitivity reactions through tumor necrosis factor and macro- Acta Anaesthesiol Scand. 2009;53(2):270-271. doi:10.1111/j.1399-
phage inflammatory protein 2. J Exp Med. 2000;192(10):1441-1452. 6576.2008.01780.x
doi:10.1084/jem.192.10.1441 35. King BF, Liu M, Townsend-Nicholson A, Burnstock G. Oral Com-
15. Esposito I, Kleeff J, Bischoff SC, et al. The stem cell factor-c-kit munications: Inhibitory interaction between activated TRPV1 and
system and mast cells in human pancreatic cancer. Lab Invest. P2X3 receptors. Paper presented at: Physiological Society Annual
2002;82(11):1481-1492. doi:10.1097/01.lab.0000036875.21209.f9 Conference University College London; July 5, 2006; London, UK.
16. Benoist C, Mathis D. Mast cells in autoimmune disease. Nature. Proc Physiol Soc. 2006;3:C35. 1 Accessed September 1, 2019. https://
2002;420(6917):875-878. doi:10.1038/nature01324 www.physoc.org/abstracts/inhibitory-interaction-between-activated-
17. Theoharides TC, Valent P, Akin C. Mast cells, mastocytosis, and trpv1-and-p2x3-receptors/
related disorders. N Engl J Med. 2015;373(2):163-172. doi:10.1056/ 36. Sessler DI, Warner DS, Warner MA. Temperature monitoring and
NEJMra1409760 perioperative thermoregulation. Anesthesiology. 2008;109(2):318-
18. von Bubnoff D, Novak N, Kraft S, Bieber T. The central role of FcεRI 338. doi:10.1097/ALN.0b013e31817f6d76
in allergy. Clin Exp Dermatol. 2003;28(2):184-187. doi:10.1046/ 37. Wang M, Singh A, Qureshi H, Leone A, Mascha EJ, Sessler DI. Optimal
j.1365-2230.2003.01209.x depth for nasopharyngeal temperature probe positioning. Anesth Analg.
19. Nunomura S, Gon Y, Yoshimaru T, et al. Role of the FcεRI β-chain 2016;122(5):1434-1438. doi:10.1213/ANE.0000000000001213
ITAM as a signal regulator for mast cell activation with monomeric
IgE. Int Immunol. 2005;17(6):685-694. doi:10.1093/intimm/dxh248
AUTHORS
20. Mócsai A, Ruland J, Tybulewicz VL. The SYK tyrosine kinase: a Sarah E. Giron, PhD, CRNA, has been a clinical and didactic educator in
crucial player in diverse biological functions. Nat Rev Immunol. nurse anesthesia since 2005. She is currently a full-time faculty member
2010;10(6):387-402. doi:10.1038/nri2765 of the Kaiser Permanente School of Anesthesia in Pasadena, California,
21. Novak N, Bieber T, Peng WM. The immunoglobulin E-Toll- and practices at the South Bay Kaiser Permanente facility in Harbor City,
like receptor network. Int Arch Allergy Immunol. 2010;151(1):1-7. California.
doi:10.1159/000232565
Crystal D. Trinooson, MS, CRNA, is a staff nurse anesthetist at Keck
22. Arinobu Y, Iwasaki H, Akashi K. Origin of basophils and mast cells. Medical Center of the University of Southern California.
Allergol Int. 2009;58(1):21-28. doi:10.2332/allergolint.08-RAI-0067
Rana Movahedi, MD, is an associate clinical professor at the University
23. Theoharides TC, Alysandratos KD, Angelidou A, et al. Mast cells
of California, Los Angeles, where she teaches clinical and didactic regional
and inflammation. Biochim Biophys Acta. 2012;1822(1):21-33.
anesthesia. She completed her residency at Cedars-Sinai Medical Center,
doi:10.1016/j.bbadis.2010.12.014
Los Angeles, California, and her fellowship at the Hospital for Special
24. Kovarova M, Koller B. Differentiation of mast cells from embry- Surgery, New York, New York.
onic stem cells. Curr Protoc Immunol. 2012;97:22F.10.1-16.
doi:10.1002/0471142735.im22f10s97
25. Akin C. Mast cell activation syndromes presenting as anaphylaxis. DISCLOSURES
Immunol Allergy Clin North Am. 2015;35(2):277-285. doi:10.1016/j. Name: Sarah E. Giron, PhD, CRNA
iac.2015.01.010 Contribution: This author made significant contributions to the concep-
26. Onnes MC, Tanno LK, Elberink JN. Mast cell clonal disorders: clas- tion, synthesis, writing, and final editing and approval of the manuscript
sification, diagnosis, and management. Curr Treat Options Allergy. to justify inclusion as an author.
2016;3(4):453-464. doi:10.1007/s40521-016-0103-3 Disclosures: None.
Name: Crystal D. Trinooson, MS, CRNA
27. Gülen T, Akin C. Pharmacotherapy of mast cell disorders. Curr
Contribution: This author made significant contributions to the concep-
Opin Allergy Clin Immunol. 2017;17(4):295-303. doi:10.1097/
tion, synthesis, writing, and final editing and approval of the manuscript
ACI.0000000000000377
to justify inclusion as an author.
28. Akin C. Mast cell activation syndromes. J Allergy Clin Immunol. Disclosures: None.
2017;140(2):349-355. doi:10.1016/j.jaci.2017.06.007 Name: Rana Movahedi, MD
29. Afrin LB, Self S, Menk J, Lazarchick J. Characterization of mast Contribution: This author made significant contributions to the concep-
cell activation syndrome. Am J Med Sci. 2017;353(3):207-215. tion, synthesis, writing, and final editing and approval of the manuscript
doi:10.1016/j.amjms.2016.12.013 to justify inclusion as an author.
30. Rechenauer T, Raithel M, Götze T, et al. Idiopathic mast cell activa- Disclosures: None.
tion syndrome with associated salicylate intolerance. Front Pediatr. The authors did discuss off-label use within the article. Disclosure state-
2018;6:73. doi:10.3389/fped.2018.00073 ments are available for viewing upon request.
316 AANA Journal August 2021 Vol. 89, No. 4 www.aana.com/aanajournalonlineYou can also read

















































