Adverse Childhood Experiences - and their impact on health-harming behaviours in the Welsh adult population - Public Health Wales
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Welsh Adverse Childhood
Experiences (ACE) Study
Adverse Childhood
Experiences
and their impact on
health-harming behaviours
in the Welsh adult population
ALCOHOL USE, DRUG USE, VIOLENCE,
SEXUAL BEHAVIOUR, INCARCERATION,
SMOKING AND POOR DIET
Preface
This is one in a series of reports examining the prevalence of Adverse Childhood Experiences
(ACEs) in the Welsh adult population and their impact on health and well-being across the life
course. The series will include reports on:
■■ The prevalence of Adverse Childhood Experiences and their association with health-harming
behaviours in the Welsh adult population.
■■ The impact of Adverse Childhood Experiences on chronic ill health, use of health and social care
services and premature mortality in Welsh adults.
■■ The impact of Adverse Childhood Experiences on mental well-being in Welsh adults.
Over 2,000 adults aged 18-69 years participated representative of the general population in Wales.
in the ACE Study for Wales, providing anonymous Data were collected in participants’ places of
information on their exposure to ACEs before residence using an established questionnaire
the age of 18 years and their health and lifestyles incorporating the short ACE tool developed by the
as adults. The study achieved a compliance rate US Centers for Disease Control and Prevention and
of 49.1% and the sample was designed to be based on work by Felitti et al (1998) [1].
ISBN 978-1-910768-23-5
© 2015 Public Health Wales NHS Trust.
Material contained in this document may be reproduced under the terms of the Open Government Licence (OGL)
www.nationalarchives.gov.uk/doc/open-government-licence/version/3/ provided it is done so accurately and is not used
in a misleading context.
Acknowledgement to Public Health Wales NHS Trust to be stated.
Copyright in the typographical arrangement, design and layout belongs to Public Health Wales NHS Trust.
Welsh Adverse Childhood
Experiences (ACE) Study
Adverse Childhood Experiences
and their impact on health-harming
behaviours in the Welsh adult population
Alcohol Use, Drug Use, Violence, Sexual Behaviour,
Incarceration, Smoking and Poor Diet
Mark A. Bellisi, Kathryn Ashtoni, Karen Hughesii, Katharine Fordii, Julie Bishopi and Shantini Paranjothyi
Public Health Wales
i
Centre for Public Health
ii
Hadyn Ellis Building Liverpool John Moores University
Maindy Road Henry Cotton Campus
Cathays Level 2, 15-21 Webster Street
Cardiff CF24 4HQ Liverpool L3 2ET
Tel: 02921 841 933 Tel: 0151 231 4542
1
Public Health Wales
Foreword
Adverse Childhood Experiences (ACEs) are an
increasing international concern. There is a
growing body of evidence that our experiences
during childhood can affect health throughout
the life course. Children who experience stressful
and poor quality childhoods are more likely to
adopt health-harming behaviours during
adolescence which can themselves
lead to mental health illnesses and
diseases such as cancer, heart disease
and diabetes later in life. Adverse
Childhood Experiences are not just a
concern for health. Experiencing ACEs
means individuals are more likely to
perform poorly in school, more likely to
be involved in crime and ultimately less
likely to be a productive member of society.
People who experience ACEs as children often end United in Improving Health initiative and its focus
up trying to raise their own children in households on the first two years of life will be better informed
where ACEs are more common. Such a cycle of by a deeper understanding of childhood adversity in
childhood adversity can lock successive generations of Wales and therefore we welcome this first national
families into poor health and anti-social behaviour for report on ACEs. We hope that all those with an
generations. Equally however, preventing ACEs in a interest in improving the health, educational, social
single generation or reducing their impacts can benefit and economic prospects for Wales take note of what it
not only those children but also future generations in tells us about the long reach of childhood experiences
Wales. That is why Public Health Wales is leading a and that all organisations identify the steps they can
collaboration to improve early life experiences across take to give every child in Wales the best start in life.
Wales. The United in Improving Health initiative
pulls together health, social, local authority, criminal
justice, educational and other sectors to fully utilise
the expertise and assets we have in Wales to improve
the health of the Welsh population. We believe our
Dr Tracey Cooper Professor
Chief Executive Sir Mansel Aylward
Public Health Wales Chair
Public Health Wales
2
Welsh Adverse Childhood Experiences (ACE) Study
Executive Summary
An increasing body of research identifies the long-term harms
that can result from chronic stress on individuals during
childhood. Such stress arises from the abuse and neglect of
children but also from growing up in households where
children are routinely exposed to issues such as domestic
violence or individuals with alcohol and other substance
use problems.
Collectively such Liverpool John Moores University undertook the first
childhood stressors ACE study for Wales which consisted of a national
are called ACEs cross-sectional survey of adults residential in Wales.
(Adverse Childhood With an overall sample size of 2,028, Welsh adults
Experiences). were asked about their current health behaviours
Exposure to ACEs and their exposure to ACEs using an internationally
can alter how children’s validated ACE questionnaire. Initial analysis of the
brains develop as well as study has focused on identifying how health-harming
changing the development behaviours (for example, drug use and binge drinking)
of their immunological and are linked with experiencing ACEs during childhood.
hormonal systems. Subsequently, Full details of the methodology and results are
those with greater exposure to ACEs are contained in this report and a summary of the findings
more likely to go on to develop health-harming and is presented as an info-graphic.
anti-social behaviours, often during adolescence, such
as binge drinking, smoking and drug use. Ultimately, This first Welsh ACE survey identifies that substantial
such poor health and social behaviour means proportions of the Welsh population suffered abuse,
individuals progress more rapidly to develop diseases neglect and other ACEs during their childhood with
such as diabetes, cancer, cardiovascular disease and 47% reporting having experienced at least one ACE
mental illness. and 14% experiencing four or more ACEs. However,
the report also outlines a substantive range of policies
Preventing ACEs can improve health across the whole and programmes that have now been implemented in
life course, enhancing individuals’ well-being and Wales to both prevent ACEs and identify and intervene
productivity while reducing pressures and costs on where children are already experiencing such stressors.
the National Health Service (NHS). Those experiencing
more ACEs are also more likely to be involved in Findings show that ACEs have a major impact on
violence and other anti-social behaviour and perform the development of health-harming behaviours in
more poorly in schools. Thus, health, social, criminal Wales and the prevention of ACEs is likely not only to
justice and educational systems are all likely to see improve the early years experiences of children born
better results for the Welsh population if ACEs are in Wales but also reduce levels of health-harming
prevented. behaviours such as problem alcohol use, smoking,
poor diets and violent behaviour. Further reports
Tackling ACEs in Wales relies on having intelligence from this survey will detail how ACEs in Wales are
on how many individuals are exposed to ACEs, associated with chronic ill health in later life such as
the characteristics of those most at risk and the the development of cancer, heart disease, diabetes
consequences across the life course. Consequently, and ultimately premature death.
in 2015, Public Health Wales in collaboration with
3
Public Health Wales
Adverse Childhood
Experiences (ACEs) in Wales
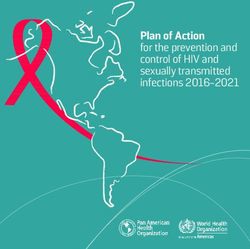
ACEs are stressful experiences occurring during childhood that directly harm a child
(e.g. sexual or physical abuse) or affect the environment in which they live
(e.g. growing up in a house with domestic violence).
How many adults in Wales have been exposed to each ACE?
CHILD MALTREATMENT
Verbal abuse Physical abuse Sexual abuse
23% 17% 10%
CHILDHOOD HOUSEHOLD INCLUDED
Parental Domestic Mental Alcohol Drug Incarceration
separation violence illness abuse use 5%
20% 16% 14% 14% 5%
For every 100 adults in Wales 47 have suffered at least one ACE during
their childhood and 14 have suffered 4 or more.
0 ACEs 53%
1 ACE 20%
2-3 ACEs 13%
4+ ACEs 14%
Figures based on population adjusted
prevalence in adults aged 18-69 years
in Wales
4
Welsh Adverse Childhood Experiences (ACE) Study
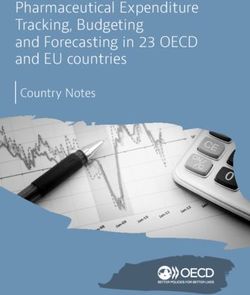
ACEs increase individuals’ risks of
developing health-harming behaviours
Compared with people with no ACEs, those with 4+ ACEs are:
4 times more likely to be a high-risk drinker
6 times more likely to have had or caused unintended teenage pregnancy
6 times more likely to smoke e-cigarettes or tobacco
6 times more likely to have had sex under the age of 16 years
11 times more likely to have smoked cannabis
14 times more likely to have been a victim of violence over the last 12 months
15 times more likely to have committed violence against another person in the last 12 months
16 times more likely to have used crack cocaine or heroin
20 times more likely to have been incarcerated at any point in their lifetime
Preventing ACEs in future generations could reduce levels of:
Heroin/crack cocaine Incarceration Violence perpetration Violence victimisation Cannabis use
use (lifetime) (lifetime) (past year) (past year) (lifetime)
by 66% by 65% by 60% by 57% by 42%
Unintended teen High-risk drinking Early sex Smoking tobacco or Poor diet
pregnancy (current) (before age 16) e-cigarettes (current;Public Health Wales
Introduction
Adverse Childhood Experiences How ACEs can affect children and
Globally there is an increasing body of evidence change their life course
examining how experiences during childhood have ACEs are known to have direct and immediate effects
long-term impacts on our health [1-2]. Chronic on a child’s health through, for instance, physical
stressful experiences in childhood, termed in this injury to a child who is abused [7]. However, recent
study Adverse Childhood Experiences (ACEs), can set evidence demonstrates that chronic traumatic stress
individuals on a health-harming life course; increasing in early life alters how a child’s brain develops and
their risks of adopting health-harming behaviours such can fundamentally alter nervous, hormonal and
as smoking, problem drinking, poor diet, low levels of immunological system development [8-10]. This can
exercise and risky sexual behaviour [2-3]. In turn, such result in individuals whose systems are ‘locked’ into
behaviours can lead to premature ill health through a higher state of alertness; permanently prepared for
increasing risks of non-communicable diseases such as further trauma. Such physiological changes increase
diabetes, heart disease and cancers [1, 3, 4]. The same the wear and tear (allostatic load) on their body;
chronic stressors in early childhood can also lead to increasing risks of premature ill health such as cancer,
individuals developing anti-social behaviours, including heart disease and mental illness [1-2; see Figure 1].
a propensity for aggressive and violent behaviour and During school years, the same individuals may display
ultimately problems with criminal justice services [5]. a heightened emotional state of anxiety (ready to fight
Individuals’ engagement in education, their ability to or always prepared to run away) and consequently
gain qualifications and ultimately their contribution to be distracted from educational pursuits, resulting in
the economy can all be affected by the combination of poor educational attainments [11]. Children raised
anti-social behaviour, difficulties with social adjustment in environments where violence, assault and abuse
and ill health [3,6]. Consequently, understanding the are common are more likely to develop such traits
prevalence and impact of ACEs across Wales and how themselves as these behaviours are seen as normal
they can inform prevention strategies is in the interest (i.e. normalised); leaving them more likely to both
of health, education and criminal justice agencies commit violent acts and/or be the victim of such acts
as well as to the long-term economic benefit of the in adulthood. Furthermore, the psychological problems
country. associated with exposure to ACEs can leave individuals
with feelings of low self-worth and a propensity for
What are ACEs? behaviours offering short-term relief at the expense of
ACEs are stressful experiences occurring during longer-term health. This combination leaves affected
childhood that directly hurt a child (e.g. maltreatment) individuals prone to adopting harmful behaviours such
or affect them through the environment in which as smoking, harmful alcohol consumption, poor diets
they live (e.g. growing up in a house with domestic and even early sexual activity [12].
violence). ACEs can continue to harm the health of
children throughout their life. A full list of ACEs used The strong associations between exposure to ACEs
in the Welsh ACE study is outlined in Table 1. and vulnerability to harms including substance use,
unintended teenage pregnancy, violence, mental
illness and physical health problems, mean the
children of those affected by ACEs are at increased
risk of exposing their own children to ACEs [13]. This
is often referred to as the ‘cycle of violence’ [14].
Consequently, preventing ACEs in a single generation
or reducing their impact on children can benefit not
only those individuals but also future generations
across Wales.
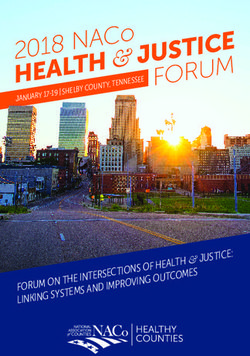
6Welsh Adverse Childhood Experiences (ACE) Study
Early
death
Disease, disability,
social problems and
low productivity
Life Course
Adoptions of high risk
behaviours and crime
Social, emotional and cognitive impairment
Disrupted neurodevelopment and allostatic load
Adverse Childhood Experiences
Figure 1: Model of ACE impacts across the life course1
ACE Survey for Wales ■■ To ensure we understand which communities and
population groups in Wales are most affected by
In 2015, Public Health Wales undertook the first Welsh
ACEs so that existing investments in child and
ACE survey to help inform its future actions and that
parent support across Wales can be effectively
of other health and well-being stakeholders in Wales.
directed.
Survey objectives ■■ To help inform a multi-agency response to ACEs
The ACE survey for Wales study had the following which includes a focus on both the prevention of
objectives: ACEs and the appropriate service response (health,
social, criminal justice and educational) to those
■■ To investigate the prevalence of ACEs during the
already affected by ACEs.
first 18 years of life in order to provide a baseline
measure of the prevalence of ACEs in Wales. Details of the methodology used to undertake the
■■ To investigate the association between ACEs and Welsh ACE Survey are outlined in Appendix 1. All
health-harming behaviours, healthcare utilisation reported differences were found to be statistically
and non-communicable diseases. significant, unless otherwise stated (see Appendix 2
for all data tables).
■■ To estimate the potential impact of preventing
ACEs on subsequent changes in ill health, anti-
social behaviour, crime and economic activity in
the Welsh population.
1 Based on the US Centers for Disease Control and Prevention ‘ACE Pyramid’: http://www.cdc.gov/violenceprevention/acestudy
7Public Health Wales
Prevalence of Adverse Childhood Experiences in Wales
Just under half of all individuals surveyed had experienced at least one ACE before the
age of 18 years (46.5%). 13.6% had experienced four or more ACEs. The prevalence of
individual ACEs ranged from 4.6% of respondents reporting living with a drug-using
household member during their childhood, to 22.8% experiencing more than one
episode of verbal abuse as a child2 (see Figure 2 and Appendix 2 Table i).
Figure 2: Prevalence of the number of ACEs and individual ACEs experienced
Verbal abuse
Parental separation
Physical abuse
Domestic violence
Alcohol abuse
Mental illness
Sexual abuse
Incarceration
Drug abuse
Experienced 0 ACEs
Experienced 1 ACE
Experienced 2-3 ACEs
Experienced 4 or more ACEs
0 10 20 30 40 50 60
Prevalence %
2 Estimates have been adjusted to mid-2013 national population estimates.
8Welsh Adverse Childhood Experiences (ACE) Study
Table 1: ACEs included in the study
All ACE questions were preceded by the statement ‘While you were growing up, before the age of 18...’
Responses listed are those categorised as an ACE.
ACE Question Qualifying
response3
Sexual abuse How often did anyone at least 5 years older than you (including adults) try Once or more than
to make you touch them sexually? once to any of the
three questions
How often did anyone at least 5 years older than you (including adults)
force you to have any type of sexual intercourse (oral, anal or vaginal)?
How often did anyone at least 5 years older than you (including adults)
ever touch you sexually?
Physical abuse How often did a parent or adult in your home ever hit, beat, kick or Once or more than
physically hurt you in any way? This does not include gentle smacking for once
punishment.
Verbal abuse How often did a parent or adult in your home ever swear at you, insult More than once
you, or put you down?
Domestic How often did your parents or adults in your home ever slap, hit, kick, Once or more than
violence punch or beat each other up? once
Parental Were your parents ever separated or divorced? Yes
separation4
Mental illness Did you live with anyone who was depressed, mentally ill or suicidal? Yes
Alcohol abuse Did you live with anyone who was a problem drinker or alcoholic? Yes
Drug abuse Did you live with anyone who used illegal street drugs or who abused Yes
prescription medications?
Incarceration Did you live with anyone who served time or was sentenced to serve time Yes
in a prison or young offender’s institution?
3 Qualifying response is the level of abuse, neglect or family problem recorded as an ACE. Levels are based on ACE studies undertaken elsewhere [3, 15].
4 The specific act of divorce or parental separation can be either harmful or beneficial to the child but in ACE studies divorce or parental separation is
often used as a marker of substantive, often long-term conflict between parents.
9Public Health Wales
Smoking Tobacco or E-Cigarettes
Smoking tobacco or e-cigarettes was defined as individuals who stated that they currently smoked either.
Figure 3: Currently Smoking Tobacco or E-Cigarettes: Percentage and Adjusted Odds Ratio (AOR)
by ACE counta
70 % AORs 9
8
60
7
50
6
AORs (95%CIs)
40 5
%
30 4
3
20
2
10
1
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
a
pWelsh Adverse Childhood Experiences (ACE) Study
0 Alcohol Use – High-Risk Drinking
High-risk drinking was calculated using the Alcohol Use Disorder Identification Test (AUDIT-C)5. Individuals with a
score of eight or over were classified as high-risk drinkers.
Figure 4: High-Risk Drinking: Percentage and Adjusted Odds Ratio (AOR) by ACE counta
30 % AORs 6
25 5
20 4
AORs (95%CIs)
% 15 3
10 2
5 1
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
a
pPublic Health Wales
Cannabis Use
A respondent was defined as having used cannabis if they reported having used this drug at any point during their
lifetime.
Figure 5: Cannabis Use: Percentage and Adjusted Odds Ratio (AOR) by ACE counta
70 18
% AORs
16
60
14
50
12
AORs (95%CIs)
40 10
%
30 8
6
20
4
10
2
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
pWelsh Adverse Childhood Experiences (ACE) Study
0 Heroin or Crack Cocaine Use
A respondent was defined as having used heroin or crack cocaine if they reported having used either of these drugs
at any point during their lifetime.
Figure 6: Heroin or Crack Cocaine Use: Percentage and Adjusted Odds Ratio (AOR) by ACE counta
22 % AORs 30
20
18 25
16
20
14
AORs (95%CIs)
12
15
% 10
8
10
6
4 5
2
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
pPublic Health Wales
Violence Victimisation
Violence victimisation accounts for anyone who reported they had been physically hit by anyone in the last 12 months.
Figure 7: Violence Victimisation: Percentage and Adjusted Odds Ratio (AOR) by ACE counta
40 % AORs 25
35
20
30
25
15
AORs (95%CIs)
20
%
10
15
10
5
5
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
a
pWelsh Adverse Childhood Experiences (ACE) Study
0 Violence Perpetration
Violence perpetration was defined as anyone who stated that they had physically hit another person in the last 12
months.
Figure 8: Violence Perpetration: Percentage and Adjusted Odds Ratio (AOR) by
ACE counta
35 % AORs 25
30
20
25
15
AORs (95%CIs)
20
%
15
10
10
5
5
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
a
pPublic Health Wales
Incarceration
Incarceration was defined as anyone who has spent one or more night(s) in prison, jail or in a police station at any
point in their lives.
Figure 9: Incarceration: Percentage and Adjusted Odds Ratio (AOR) by ACE counta
45 % AORs 35
40
30
35
25
30
AORs (95%CIs)
25 20
% 20
15
15
10
10
5
5
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
a
pWelsh Adverse Childhood Experiences (ACE) Study
0 Poor Diet
Respondents were asked how many portions of fruit and vegetables (excluding potatoes) they would eat on a normal
day. Using this data, poor diet was defined as those individuals who reported that they ate less than two portions a day.
Figure 10: Poor Diet: Percentage and Adjusted Odds Ratio (AOR) by ACE counta
35 % AORs 3.5
30 3
25 2.5
AORs (95%CIs)
20 2
%
15 1.5
10 1
5 0.5
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
a
pPublic Health Wales
Unintended Teenage Pregnancy
Unintended teenage pregnancy was defined as incidents where an individual accidently got pregnant or accidently
got someone else pregnant before the age of 18 years.
Figure 11: Unintended Teenage Pregnancy: Percentage and Adjusted Odds Ratio (AOR) by ACE
counta
35 % AORs 10
9
30
8
25 7
6
20
AORs (95%CIs)
% 5
15
4
10 3
2
5
1
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
pWelsh Adverse Childhood Experiences (ACE) Study
0 Early Sexual Initiation
Early sexual initiation was defined as someone who has had sexual intercourse before the age of 16 years.
Figure 12: Early Sexual Initiation: Percentage and Adjusted Odds Ratio (AOR) by ACE counta
60 % AORs 9
8
50
7
AORs (95%CIs)
40 6
% 5
30
4
20 3
2
10
1
0 0
0 ACEs 1 ACE 2-3 ACEs 4+ ACEs
ACE Count
a
pPublic Health Wales
Breaking the ACE Cycle in Wales
Results from the Welsh ACE survey identify both the potential harms across the
life course resulting from avoidable stress and adversity in childhood and the huge
potential health gains possible if childhood experiences are improved. As these analyses
have shown, the benefits of preventing ACEs are not limited to health, but also impact
on violent crime and social issues such as teenage pregnancy.
Wales is already pioneering a range of national policies the child’s first seven years of their life from
and programmes which aim to: conception so that families are supported to make
long-term health enhancing choices;
■■ Identify and intervene where children may already
be victims of abuse, neglect or living in adverse ■■ Promotion of bonding and attachment to support
childhood environments; positive good parent-child relationships resulting in
secure emotional attachment for children; and,
■■ Better equip parents and care-givers with the
necessary skills to avoid ACEs arising within the ■■ The promotion of positive maternal and family
home environment and encourage development emotional health and resilience.
of social and emotional well-being and resilience in
the child; Health visitors in Wales work in partnership with
families to meet these goals, assess resilience (See Box
■■ Ensure that indirect harms from for instance, 1) and provide support to meet their needs.
domestic violence, substance use and other mental
and behavioural problems in the family setting are While no communities should be considered free
identified, addressed and their impact on children from ACEs, those living in areas of deprivation are at
minimised. greater risk of experiencing multiple ACEs. In Wales
this is being addressed through Tackling Poverty
The Building a Brighter Future: Early Years and Programmes such as Flying Start; Families First and
Childcare Plan 2013-2023 [16] and The Healthy Child Communities First. These programmes are targeted at
Wales programme7 set out the policy framework and the most deprived communities in Wales. Flying Start
plan for supporting families to ensure their children is the Welsh Government’s Early Years programme for
attain their health and developmental potential and families with children less than four years of age who
aims to increase family resilience. This includes the live in some of the most deprived areas of Wales. The
following: core elements of the programme are free quality, part-
■■ Influencing Welsh national public health strategies time childcare for two-three year olds, an enhanced
to enhance healthier communities; health visiting service, access to parenting programmes
and speech, language and communication support8.
■■ Delivery of key public health messages throughout Those families assessed as experiencing substance
Box 1: ACEs and Resilience
Within the context of ACEs, resilience can be considered as an individual’s ability to avoid harmful
behavioural and physiological changes in response to chronic stress. Such individuals have the skills and
often have received the support necessary to adapt successfully to the stress, trauma and other forms of
chronic adversity [17]. Alongside the ACE questionnaire, resilience questionnaires have also been developed
to identify whether children have assets available to them (e.g. a loving parent/carer) that may help reduce
the acute and long-term impacts of ACEs on their health and behaviour. Health visitors may use resilience
tools to identify the supportive factors that need to be delivered through targeted services in order to
improve health outcomes for individuals.
7 More information on the Healthy Child Wales programme can be found here:
http://gov.wales/topics/people-and-communities/people/children-and-young-people/parenting-support-guidance/help/?lang=en
8 More information on Flying Start can be found here:
http://gov.wales/topics/people-and-communities/people/children-and-young-people/parenting-support-guidance/help/flyingstart/?lang=en
20Welsh Adverse Childhood Experiences (ACE) Study
misuse; domestic violence or abuse; a history of violent Such commitments are consistent with modern
or abusive behaviour or mental health issues can be demands on police forces. For instance, in South
referred to the Integrated Family Support Services Wales only 11% of contacts with the public are
which are funded by Welsh Government. reports of crime with the vast majority relating to
welfare, public safety and vulnerability. A public health
Public Health Wales’ Strategic Plan 2015-2018 has approach to policing means equipping and supporting
prioritised working across sectors to improve the the police to identify early indicators of adversity and
health of our children in their early years [18]. Further, using their contacts with the public to help prevent
the collective initiative United in Improving Health aims further adversity and trauma amongst those who are
to ensure co-ordinated system-based working across most vulnerable. Such measures are consistent with
public services, voluntary and private organisations both an ACE preventing and resilience promoting
at a national and local level. Through United in agenda likely to reduce crime, improve health and
Improving Health, Wales can exploit assets not just in benefit the national economy [20].
the health systems but the professionals, volunteers
and other resources that make up our schools and More broadly, the Well-being of Future Generations
workplaces, housing, police, fire and rescue services. (Wales) Act (2015)[21] aims to improve the social,
United in Improving Health is re-aligning these assets economic, environmental and cultural well-being
to accomplish a shared set of goals. The first of these of Wales, whilst ensuring the health and well-being
is improving outcomes in the early years, with a focus of future generations is secured. The Act has put
on the first two years of life. An understanding of the in place seven well-being goals (see Figure 13) and
life-time costs of ACEs, who is most affected by them this groundbreaking piece of legislation provides an
in Wales, and the most effective mechanisms for their opportunity for the reduction of ACEs across Wales
prevention, are all critical elements in advocating for through efforts to achieve its goals of both a healthier
and accomplishing this United in Improving Health and a more equal Wales.
goal.
The aspirations for a healthier Wales includes the
As part of a united approach, Public Health Wales creation of a society in which people’s physical
recognises the Police as a fundamental in preventing and mental well-being are maximised from the
ACEs; not just as a service which responds to crises, beginning of the life course and in which choices and
but as part of the ACE prevention process. The South behaviours which benefit future health outcomes
Wales Police and Crime Commissioner has adopted are understood and supported. Preventing ACEs and
early intervention as a key principle and has signed a building resilience in children will directly support
memorandum of understanding with Public Health the achievement of this goal. A more equal Wales
Wales [19] that commits both organisations to: envisages a society that enables people to fulfill their
potential, reducing inequality and placing a greater
■■ Wherever possible focus efforts on ensuring that,
value on diversity. This goal relies on every child
from the earliest possible age, individuals are
growing up free from ACEs and on understanding that
supported to follow a health benefiting and crime
ACEs do not arise in isolation but are associated with
free life course that allows them to realise their full
environments that tolerate inequalities. Whilst life
potential.
expectancy and health outcomes are often poorer for
■■ Promote the positive impact that parents can have men, domestic abuse, sexual violence and other forms
in the early years by encouraging early intervention of gender-based discrimination are more likely to be
initiatives and promotion of positive lifestyle and experienced by women and girls. Tackling gender
well-being choices within the family. inequalities is part of creating households free from
ACEs [22]. The Violence Against Women, Domestic
Abuse and Sexual Violence Act (Wales) 2015 provides
another important policy framework in the prevention
and protection against gender-based violence [23].
21Public Health Wales
Figure 13: The seven well-being goals taken from the Well-being of Future Generations (Wales)
Act (2015)
A globally A prosperous
responsible Wales
Wales
A Wales of
vibrant culture
and thriving A resilient
Welsh language Wales
A Wales of
cohesive A healthier
communities Wales
A more equal
Wales
International support directs health systems globally to play a central role in
addressing violence, in particular against women and
As well as policy in Wales, international developments
children [26]. Public Health Wales is already an active
are requiring nations to provide safe, secure and
member of an international network working with
supportive childhoods and are providing access to
the World Health Organization and other regions and
international evidence about the best ways to achieve
nations to develop and share evidence on what works
this goal. With an estimated 9.6% of all children
in the prevention of ACEs.
suffering sexual abuse across Europe and as many as
22.9% suffering physical abuse, the World Health
Organization has launched Investing in Children:
Research
the European child maltreatment prevention action Whilst this first ACE report for Wales has begun
plan 2015–2020 [24]. The plan aims to reduce the to identify the scale and impact of ACEs in Wales,
prevalence of child maltreatment by implementing a better understanding of their impact on the life
preventive programmes that reduce risk and increase course is required along with an ability to monitor the
protective factors. In addition the United Nations in effectiveness of efforts to prevent ACEs. Systems such
2015 launched the Sustainability Goals (SDGs). With as the Secure Anonymised Information Linkage (SAIL)
much in common with the Well-being of Future databank already enable information on individuals to
Generations (Wales) Act 2015, the SDGs include the be anonymously linked both across organisations and
aim of ending abuse, exploitation, trafficking and all over time. Consequently, longitudinal studies on ACEs
forms of violence against and torture of children [25]. and their on-going impact on the Welsh population
Such ambitions are also consistent with the recent are already in development. New research initiatives
World Health Assembly resolution on violence which across Wales, such as HealthWise Wales, will create
even greater opportunities to understand and address
ACEs9.
9 HealthWise Wales is a Health and Care Research Wales initiative for a Welsh National Population cohort study, which will engage with the
population of Wales and encourage them to become actively involved in research to improve health and well-being, and provide a platform for
research, policy and service development and evaluation. For more information, see http://www.healthwisewales.gov.wales/
22Welsh Adverse Childhood Experiences (ACE) Study
Conclusion
This report is primarily aimed at identifying the extent support in parenting and child development. Again,
of exposure to ACEs across the adult population of such services are already in place across some parts of
Wales and their impact on health-harming behaviours. Wales. However, what is actually delivered, how well
This first ACE survey found that adults resident needs are met and how well interventions match the
in Wales experience ACEs at levels comparable evidence for ACE prevention is sometimes unclear.
(Wales; 47% experienced at least one ACE and 14%
experienced four or more ACEs) to other parts of ACEs may be prevented through enhanced public
the UK (England; 48% experienced at least one ACE and professional awareness, evidence-informed
and 9% experienced four or more ACEs [3]) as well universal service specifications, effective pathways
as further afield (for example, Eastern Europe; 53% into additional support, monitoring of intervention
experienced at least one ACE and 7% experienced coverage and content and, routine audit of fidelity to
four or more ACEs [12])10. The impact of such ACEs intervention specifications. While Public Health may
may include being responsible for nearly a quarter have a leadership role in these developments they
of current adult smoking, over a third of teenage require partnerships and investment from healthcare
pregnancy and more than half of the violence, services, local authorities and more widely across the
heroin/crack use and incarceration reported by study whole public sector. Policies including the Well-being
participants. Reflected in population terms, eradicating of Future Generations (Wales) Act 2015 provide the
ACEs could ultimately result in over 125,000 less legitimacy for such activity, and structures such as
smokers or e-cigarette users across Wales and over United in Improving Health provide the opportunity
55,000 fewer people who have ever used heroin or for the essential co-ordination of assets, investments
crack cocaine. and activity in order to make it happen. The results
from this ACE survey will help inform and enhance
The existing international evidence on ACEs has developments in this area to increase the focus on
informed the priority given to the early years in preventing ACEs in the future.
Wales. However despite significant investment, the
overall impact of these programmes on preventing
ACEs is often unclear. In order to effectively reduce
ACEs in Wales and improve individuals’ life course
prospects, a number of issues should be addressed.
Firstly, improved awareness is needed of the
importance of early life experiences on the long-term
health, social and economic prospects of children.
Information should be available to a wide range
of professionals (health, education, social, criminal
justice and others) on ACEs, their consequences
and how they can be prevented. Information should
also be disseminated to the public and especially
those planning or having children. All parents and
their children in Wales should already have access to
support services – especially in early years. However,
a better understanding is needed of specifically what
support every individual should and ultimately does
receive. Support must conform to established and
emerging evidence of what works in the prevention
of ACEs and the successful development of resilience
in children. Finally, some families (often but not
exclusively in deprived communities) require enhanced
10 There are difficulties with direct comparison of results from different ACE studies due to differences in sampling techniques used and variations
in the age groups and communities included.
23Public Health Wales
References
1 Felitti VJ, Anda RF, Nordenberg D et al. 1998. ‘Relationship of child- 14 World Health Organization. 2013. European report on preventing
hood abuse and household dysfunction to many of the leading child maltreatment. http://www.euro.who.int/en/publications/abstracts/
causes of death in adults: the Adverse Childhood Experiences (ACE) european-report-on-preventing-child-maltreatment-2013 (accessed 4 Sep
Study.’ American Journal of Preventive Medicine 14:245–258. 2015).
2 Anda RF, Felitti VJ and Bremner JD. 2006. ‘The enduring effects 15 Bynum L, Griffin T, Ridings DL, Wynkoop KS, Anda RF, Edwards VJ
of abuse and related adverse experiences in childhood. A conver- and Croft JB. 2010. Adverse childhood experiences reported by
gence of evidence from neurobiology and epidemiology’ European adults—five states, 2009. MMWR:Morbidity & Mortality Weekly
Archives of Psychiatry and Clinical Neuroscience 256(3):174-186. Report, 59(49), 1609–1613.
3 Bellis MA, Hughes K, Leckenby N, Perkins C and Lowey H. 2014a. 16 Welsh Government (2013) Building a Brighter Future: The
‘National Household Survey of adverse childhood experiences and Early Years and Childcare Plan 2013-2023: http://gov.wales/topics/
their relationship with resilience to health-harming behaviours in educationandskills/earlyyearshome/building-a-brighter-future-early-years-and-
England’. BMC Medicine 12:72. childcare-plan/?lang=en (accessed 4 Sep 2015).
4 Lozano R, Naghavi M, Foreman K et al. 2012. ‘Global and regional 17 National Scientific Council on the Developing Child. 2015.
mortality from 235 causes of death for 20 age groups in 1990 and Supportive Relationships and Active Skill-Building Strengthen
2010: a systematic analysis for the Global Burden of Disease Study the Foundations of Resilience: Working Paper 13. http://www.
2010’. Lancet 380(9859):2095-2128. developingchild.harvard.edu (accessed 4 Sep 2015).
5 Dregan A, Gulliford MC. 2012. ‘Foster care, residential care and 18 Public Health Wales. 2015. Creating a Healthier, Happier, Fairer
public care placement patterns are associated with adult life Wales for everyone. Introducing the Public Health Wales Strategic
trajectories; population-based cohort study. Social Psychiatry and Plan for 2015-2018. http://www.wales.nhs.uk/sitesplus/888/page/82750
Psychiatric Epidemiology 47(9):1517-1526. (accessed 4 Sep 2015).
6 Hillis SD, Anda RF, Dube SR, Felitti VJ, Marchbanks PA, Marks JS. 19 The Chief Constable for South Wales Police and Public Health
2004. ‘The association between adverse childhood experiences and Wales. 2015. Memorandum of Understanding between the Police
adolescent pregnancy, long-term psychosocial outcomes, and fetal and Crime Commissioner for South Wales.
death.’ Pediatrics 113(2):320–327. 20 Heckman J. 2012. The case for investing in disadvantaged
7 Flaherty EG et al. 2006. ‘Effect of early childhood adversity on child young children. http://hanswernersinn.de/de/dms/EENEE/Policy_Briefs/
health’ Archives of Paediatrics and Medicine 160(12) 1232-1238. PolicyBrief1-2012.pdf (accessed 20th Oct 2015).
8 Anda RF, Butchart A, Felitti VJ and Brown DW. 2010. ‘Building a 21 Welsh Government. 2015. Well-being of Future Generations
framework for global surveillance of the public health implications (Wales) Act. http://gov.wales/topics/people-and-communities/people/future-
of adverse childhood experiences.’ American Journal of Preventive generations-bill/?lang=en (accessed 4 Sep 2015).
Medicine 39 (1): 93-98. 22 Equality and Human Rights Commission. 2011. How Fair is Wales?
9 Danese A and McEwen B. 2012. ‘Adverse childhood experiences, http://www.equalityhumanrights.com/sites/default/files/publication_pdf/how_
allostasis, allostatic load, and age-related disease’ Physiology and fair_is_wales.pdf (accessed 14th Oct 2015).
Behavior 106(1):29-39. 23 Welsh Government. 2015. Violence Against Women, Domestic
10 Broyles ST, Staiano AE, Drazba KT, Gupta AK, Sothern M and Abuse and Sexual Violence (Wales) Act. http://www.legislation.gov.uk/
Katzmarzyk PT. 2012. ‘Elevated C-reactive protein in children from anaw/2015/3/contents/enacted (accessed 14 Oct 2015).
risky neighborhoods: evidence for a stress pathway linking neigh- 24 World Health Organisation. 2014. Investing in children: the
borhoods and inflammation in children.’ PLoS One 7(9):e45419. European child maltreatment prevention action plan 2015-2020.
11 Currie J and Widom CS. 2010. ‘Long-term consequences of http://www.euro.who.int/__data/assets/pdf_file/0011/282863/Investing-in-
child abuse and neglect on adult economic well-being’ Child children-European-child-maltreatment-prevention-action-plan-2015-2020.pdf
Maltreatment 15(2) 111-120. (accessed 26 Oct 2015).
12 Bellis M, Hughes K, Leckenby N, et al. 2014b. ‘Adverse childhood 25 United Nations Division for Sustainable Health. 2015. Transforming
experiences and associations with health-harming behaviours in our world: the 2030 Agenda for Sustainable Development. https://
young adults: surveys in the European region’. Bulletin of the World sustainabledevelopment.un.org/post2015/transformingourworld (accessed 26
Health Organisation 92(9):621-696. Oct 2015).
13 Renner, L and Slack, K. 2006. ‘Intimate partner violence and child 26 Sixty-Seventh World Health Assembly. 2014. Strengthening the role
maltreatment: Understanding intra- and intergenerational connec- of the health system in addressing violence, in particular against
tions’ Child Abuse and Neglect 30(6):599-617. women and girls, and against children. http://apps.who.int/gb/ebwha/
pdf_files/WHA67/A67_ACONF1Rev1-en.pdf (accessed 26 Oct 2015).
We would like to thank Dinesh Sethi, Helen Lowey, Janine Roderick and staff in Welsh Government for their
comments on drafts of this document. Many people were involved in the development and delivery of the ACE
survey. We thank them for helping make this survey possible and also thank all those respondents who freely
gave up their time so that we can better understand and respond to the long reach of childhood adversity in
Wales.
Funding
This report was funded by Public Health Wales as part of its strategic focus on evidence based approaches to
improving early years outcomes across Wales.
24Welsh Adverse Childhood Experiences (ACE) Study
Appendix 1 Methodology
A national cross-sectional survey of adults resident in Wales was undertaken between
February and May 2015. The study was coordinated jointly by Public Health Wales NHS
Trust and Liverpool John Moores University. The fieldwork element was commissioned
from a private market research company, Future Focus Research . Ethical approval 11
was obtained from Liverpool John Moores University and Research and Development
approval was obtained from the Public Health Wales Research and Development Office.
All interviewers followed the Market Research Society (MRS) Code of Conduct 12
Sample frame and sample selection quota of respondents (based on age and gender) for
Adults aged 18-69 years and resident in Wales were each LSOA. Household visits were made on all days of
recruited to participate in the study using a method the week and between the hours of 9:00 am and 8:00
of quota sampling. In order to allow adequate pm during weekdays; at weekends visit times were
representation of residents of Wales by age, sex and limited to between the hours of 10:00 am to 6:00 pm.
deprivation, a target sample size of 2,000 individuals Only one individual from each household was eligible
was set. The achieved sample size was 2,028 (1,009 to participate in the study. On contact with a member
males and 1,019 females). Sample selection was of the household, interviewers presented individuals
stratified using Local Health Boards (LHBs), the Welsh with a letter of authority from Public Health Wales
Index of Multiple Deprivation (WIMD) and Lower NHS Trust. This letter outlined the purpose of the study
Super Output Areas (LSOAs). LSOAs are geographic and provided information regarding the utility of the
areas generated by the Office for National Statistics results, confidentiality and anonymity, and informed
(ONS) to define areas in Wales with relatively similar consent for participation. This made it clear to
population sizes (between 400-1,200 households)13. individuals that participation in the study was entirely
Each LSOA was assigned to a deprivation quintile voluntary and that they were free to withdraw at any
based on the WIMD. In order to get an equal range of point during the interview. No personal identifiable
lower deprivation and higher deprivation areas across details were collected from the individual at any
Wales, the study randomly selected a proportionate stage during the recruitment process or interview. If
number of LSOAs across each deprivation quintile no one was at the address, or an individual refused
within each LHB in Wales. This approach ensured that to participate, or were ineligible to participate in the
the LSOAs selected were broadly representative of the study, the interviewer recorded the outcome of the
geo-demographic diversity of each LHB. contact then moved on to the next household on their
random route. Potential participants were also given
Recruitment the option for the interviewers to call back at a date or
Face-to-face interviews were undertaken on the time more suitable to them. All individuals were given
doorstep of participants’ homes using a validated the option to complete the interview in Welsh, and
questionnaire. Households were visited by trained where possible translators for other languages were
interviewers from the market research company with arranged.
a sub set of visits being accompanied by researchers
from Liverpool John Moores University and Public The study inclusion criteria were:
Health Wales (for quality assurance purposes). Within ■■ Resident in selected LSOA
each LSOA, a random starting address was selected
for each interviewer shift. Each interviewer then ■■ Aged 18-69 years
followed a random route until they had met their ■■ Cognitively able to participate.
11 More information about Future Focus Research can be found on their web pages: http://www.futurefocusresearch.co.uk/
12 https://www.mrs.org.uk/standards/code_of_conduct/
13 http://www.ons.gov.uk/ons/guide-method/geography/beginner-s-guide/census/super-output-areas--soas-/index.html
25Public Health Wales
Questionnaire
The study used an established survey tool developed by the US Center for Disease Control and Prevention to
measure the prevalence of ACEs14. Alongside basic demographics, such as age, sex, ethnicity and marital status,
data was collected on the following categories outlined in Table i.
Table i: Topics included in questionnaire
Child abuse and neglect ■■ Physical abuse and neglect
■■ Psychological abuse and neglect
■■ Sexual abuse
Household dysfunction ■■ Parental separation
■■ Substance misuse within household
■■ Incarceration
■■ Domestic violence
■■ Mental illness
Health-harming behaviours ■■ Smoking
■■ Alcohol consumption
■■ Illicit drug use
■■ Sexual risk behaviours
■■ Short Warwick-Edinburgh Mental Well-being Scale (SWEMWBS)
■■ Importance of physical activity
■■ Healthy eating
■■ Height and weight (to allow for calculation of Body Mass Index)
Health complaints and ■■ Non-communicable diseases
healthcare utilisation ■■ Allergies
■■ How often visited GP and dentist
■■ Number of hospital stays in last 12 months
The interview utilised methods of Computer Assisted Personal Interviewing (CAPI), and also Computer Assisted
Self Interviewing (CASI) for the more sensitive sections of the questionnaire. Respondents were also given the
option to complete the survey on paper. On completion of interview, individuals were issued with a thank-you
leaflet which included information on the survey, contact details for help-lines in Wales and contact details for
the research team if they required further information regarding the study.
Response rate and compliance
A total of 14,893 households were visited during the study period. Contact was made with 6,293 households,
of which 4,127 included individuals conforming to the inclusion criteria. Thus, of the known eligible households,
2,099 (50.86%) opted out of completing the survey, leaving a compliance rate of 49.14% (n=2028).
Sample characteristics
Table ii illustrates the sample demographics of the survey participants in comparison to the Welsh population15.
Overall, 49.8% of respondents were male and 50.2% were female, which did not differ significantly from the
Welsh population estimates in mid-2013 for gender (p=0.901). However, the final ACE sample had a slight but
significant over-representation of individuals aged 18 to 29 years and 60-69 years, and an under-representation
of those aged 30-59 years. There was also an over-representation of individuals within the least deprived
deprivation quintile in Wales and significant differences in ethnicity.
14 www.cdc.gov/nccdphp/ace
15 For ethnicity, data was obtained from the 2011 Census: http://www.ons.gov.uk/ons/rel/census/2011-census/key-statistics-for-local-authorities-
in-england-and-wales/rpt-ethnicity.html . All other population estimates were obtained from the Office for National Statistics’ mid-2013
population estimates: http://www.ons.gov.uk/ons/rel/sape/small-area-population-estimates/mid-2013/mid-2013-small-area-population-
estimates-statistical-bulletin.html
26Welsh Adverse Childhood Experiences (ACE) Study
Table ii: Sample demographics and comparison with the Welsh national populationa (aged 18-69
years)
Sample Population X2 P
n % n %
Age 18-29 617 30.4 487,274 23.9
Years 30-39 287 14.2 349,286 17.1
40-49 360 17.8 423,900 20.8
50-59 355 17.5 401,040 19.7
60-69 409 20.2 379,068 18.6 63.17Public Health Wales
Calculation of Health-Harming Behaviours (HHBs)
The methodology used for calculating whether an individual recorded any health-harming behaviours is outlined
in Table iii.
Table iii: Health-Harming Behaviours
Outcome Question (text in brackets is the response indicating behaviour)
Smoking either e-cigarettes or Derived outcome:
tobacco In terms of smoking tobacco, which of the following best describes you? (I
smoke daily) or Do you smoke e-cigarettes? (Yes)
Higher risk drinkers Derived outcome : includes all individuals who had an AUDIT-C score of 8 or
morea
Cannabis use How often, if ever, have you taken the following illegal drugs...cannabis?
(any level of use)
Heroin/crack cocaine use How often, if ever, have you taken the following illegal drugs...heroin/crack
cocaine? (any level of use)
Violence victimisation How many times have you been physically hit in the past 12 months? (any
frequency)
Violence perpetration How many times have you physically hit someone in the past 12 months?
(any frequency)
Incarceration How many nights have you ever spent in prison, in jail or in a police station?
(Any number of nights)
Poor diet On a normal day, how many portions of fruit and vegetables (excluding
potatoes) would you usually eat (one portion is roughly one handful or a full
piece of fruit such as an apple)? (Appendix 2 Data Tables
Table i: Bivariate relationship between participant demographics, individual ACEs and ACE Counta
Individual ACEs ACE Count
Child abuse Household dysfunction 0 1 2-3 4+
Parental
separation Verbal Physical Sexual Mental Domestic Alcohol Incarceration Drug
illness violence abuse abuse
Prevalence % 20.12 22.53 17.06 9.67 13.76 16.07 14.00 4.78 4.54 54.39 18.98 13.02 13.61
n (total sample
size) 2028 2028 2028 2028 2028 2028 2028 2028 2028 2028 2028 2028 2028
Age 18-29 27.39 25.45 17.02 8.10 14.59 18.48 18.64 5.83 7.78 53.48 17.67 11.18 17.67
Years 30-39 33.45 27.53 20.20 12.89 18.47 19.16 16.73 8.71 7.67 42.16 25.44 11.50 20.91
40-49 21.39 25.56 20.56 10.56 16.67 17.22 17.22 5.28 3.89 48.61 17.78 19.17 14.44
50-59 9.58 16.90 13.52 11.83 11.83 12.68 7.89 3.38 1.97 61.41 17.46 13.24 7.89
60-69 7.82 16.87 14.91 7.09 8.31 12.22 7.58 1.22 0.24 63.33 18.83 11.25 6.60
2
X 115.415 22.944 5.953 10.486 19.619 12.552 40.911 24.333 44.611 32.639
PTable ii: Bivariate associations between health-harming behaviours and demographicsa
30
Outcome Smoking Alcohol Illicit drugs Violence and criminal justice Diet Sexual behaviour
High-risk Heroin Violence Unintended
Tobacco or drinkers Cannabis or crack victimiza- Violence Incarcera- teenage Early sexual
e-cigarettes (AUDIT-C = 8 use cocaine use tion (past perpetration tion (life- Poor diet pregnancy initiation
(current) or over) (lifetime) (lifetime) year) (past year) time) (current) (Table iii: Bivariate association between health-harming behaviours and ACE count
0
Outcome All ACE Count, % X2trend P
% n 0 1 2-3 4+
Text
Smoking
Tobacco or E-cigarettes (current) 26.45 1932 19.59 23.06 24.59 60.15 183.581Table iv: Modelled impact of preventing ACEs at sample and national population levels on health-harming behaviours
32
Sample Adjusted to national population estimates
Current Estimates % Number Current Estimates % Number
Outcome
prevalence with 0 ACEs change saved prevalence with 0 ACEs change saved
% n % n % n % n
Public Health Wales
Smoking
Either tobacco or e-cigarettes (current) 26.45 511 20.30 412 - 23.24 99 25.88 528084 19.66 401147 - 24.04 126937
Alcohol
High-risk drinking (AUDIT-C = 8 or overa) 12.92 261 8.45 172 - 34.59 89 12.52 255500 8.16 166496 - 34.84 89004
Illicit drugs
Cannabis use (lifetime) 25.04 507 14.88 302 - 40.59 205 24.23 494517 14.15 288713 - 41.62 205804
Heroin or crack cocaine use (lifetime) 4.44 90 1.48 30 - 66.63 60 4.27 87132 1.44 29344 - 66.32 57788
Violence and criminal justice
Violence victimization (past year) 9.09 184 3.95 80 - 56.51 104 8.39 171105 3.61 73676 - 56.94 97429
Violence perpetration (past year) 7.79 157 3.13 64 - 59.84 93 7.43 151678 3.01 61425 - 59.50 90253
Incarceration (lifetime) 10.09 220 3.86 78 - 61.76 142 10.48 213771 3.71 75717 - 64.58 138054
Diet and weight
Poor diet (current) 20.47 414 17.22 350 - 15.89 64 19.55 399030 16.38 334158 - 16.26 64872
Sexual behaviour
Unintended teenage pregnancy (Welsh Adverse Childhood Experiences (ACE) Study
About us
Public Health Wales exists to protect and improve health and wellbeing and
reduce health inequalities for people in Wales.
We are part of the NHS and report to the Minister for Health and Social
Services in the Welsh Government.
Our vision is for a healthier, happier and fairer Wales. We work locally,
nationally and, with partners, across communities in the following areas:
Health protection – providing information Primary, community and integrated
and advice and taking action to protect people care – strengthening its public health impact
from communicable disease and environmental through policy, commissioning, planning and
hazards. service delivery.
Microbiology – providing a network of
Safeguarding – providing expertise and
microbiology services which support the
strategic advice to help safeguard children and
diagnosis and management of infectious
vulnerable adults.
diseases.
Screening – providing screening programmes Health intelligence – providing public
which assist the early detection, prevention and health data analysis, evidence finding and
treatment of disease. knowledge management.
NHS quality improvement and patient Policy, research and international
safety – providing the NHS with information, development – influencing policy,
advice and support to improve patient supporting research and contributing to
outcomes. international health development.
Health improvement – working across
agencies and providing population services to
improve health and reduce health inequalities.
Further information
Web: www.publichealthwales.org
Email: generalenquiries@wales.nhs.uk
Twitter: @PublichealthW
Facebook: www.facebook.com/#!/PublicHealthWales
33You can also read