ADDRESSING IMPROVED PATIENT SERVICE DELIVERY WDHB GASTROENTEROLOGY DEPARTMENT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

A D D R E S S I N G I M P ROV E D
PA T I E N T S E RV I C E D E L I V E RY
W D H B G A S T RO E N T E RO L O G Y
D E PA RT M E N T
A New Model of Mortality and Morbidity Meetings
Co-Authors: Alison Bowman CNM, Dr Zoe Raos Gen Med/Gastroenterologist &
Sue French Operations Manager i3 – WDHB
WAITEMATA DHB Auckland, North Shore & Waitakere Hospital
Thurs 22nd Nov 2018
INTRODUC TION Mortality and Morbidity Meetings (M&M) are internationally established method of providing a dedicated, track-able and safe multidisciplinary forum for broad quality improvements. Opportunity for EVERYONE involved – collaboratively fostering improved patient care and quality service delivery. Data obtained, assessed and evaluated – presents dynamic quality outcomes achieved through a united team approach.

OBJEC TIVES To enhance the quality of clinical care, patient safety and patient experience To support the growth of an INCLUSIVE team culture/model with an open and transparent learning process in a no-blame environment

METHOD OF CONSTRUC TION

MORE BRICKS & MORTAR
9 C O R E S TA N D A R D S
( C O R R E C T TO O L K I T )
ToR – Terms Of Reference: Written Guidelines -Improving Quality, Outcomes and
Experiences
C G F – Intergration of the WDHB Clinical Governance Frameworks
Frequency/Scheduled Meetings – 2nd Friday of every month (45mins)
Participation (Medical & Non-Medical) – Everyone Matters
Case Selection process – Selected deaths, serious morbidity & aspects covering
clinical practice
Collection & Presentation of Data – Use of evaluation check sheet
Documentation – ISBAR approach; concise, factual, brief (5-8min) x3-4 cases
Follow up/Feedback – Meeting minutes, Actions to implement based on recommendations – ‘Your Voice Matters’ ,
Accountability in follow through on actions
Confidentiality – PQAA Protected Quality Assurance Act ActivitySTA N DA R D AGE N DA Review of previous minutes Review of process of outstanding recommendations/actions Review of IIMS – (Incident Information Management Systems) incidents Review of deaths (SAC 1) Review of serious adverse events Review of complaints Review of cases requiring open disclosure Review of risk register
R ES U LTS Average of 19 attend from five disciplines per meeting Post M&M presentation – recommended standards discussed, solutions determined/agreed on SAC Cases reviewed Captured responsibilities and timelines recorded – by Secretary Followed up at the next M & M – by Chairperson ALL STAFF – Feel included, encouraged to share, open to challenge each other (feeling safe to do so – each voice is important) Confident toward making change
M&M PRESENTERS APPROACH ISBAR method for presentation style Introduction Situation Background (As many slides as required – 1,2 &3) Assessment and Analysis (As many slides as required…) Review of Literature Recommendations
EXAMPLE OF M&M SLIDE
EXAMPLE OF M&M SLIDE
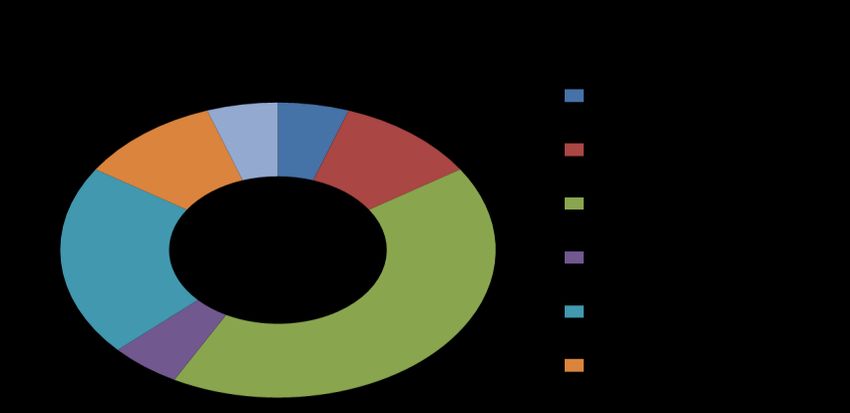
Role Number attended
SMO 3
RMO 3
Breakdown of staff attending Nov 2017
HCA 1
SMO
RN 11 12 RMO
Pathologist 0
Student Dr 1 10 HCA
Student Nurse 1 8 RN
Clerical 0 Pathologist
6
Quality Lead 1
Student Dr
Business Manager 0 4
Allied Health 2 Student Nurse
2
Technician 1 Clerical
0
Total 24 Quality Lead
1
SMO included Zoe, RN incl Ali
How participants felt about the M&M meeting - Nov 2017
Evaluation forms total completed/total number attended 16/24 66% 18 Pace of
16 16 16 16 pesentations
Yes 16 15
First M&M(total) 9 7
14
Felt encouraged and had opportunity to speak 16
Presentation easy to follow 16 12
Learning achieved 16
Will recommend to colleagues 16 10
Too fast 0
A bit Fast 1 8
Just Right 15
6
A bit Slow 0
Too slow 0
4
2 1
0 0 0
Comments on Evaluation Sheets 4 comments from 3 evaluations sheets 0
Cant think of anything to improve. Appears very well organised 1 Felt Presentation Learning Will Too fast A bit Fast Just Right A bit Slow Too slow
encouraged easy to follow achieved recommend
Very informative - relevant to recovery of patients with dilatations 1
and had to colleagues
Nothing a good meeting 1 opportunity to
Appreciated the anatomical teaching for nurses from Zoe 1 speakTHEMES FOR IMPROVEMENT
10
9
Number of cases
8
7
6
5
4
3
2
1
0
OutcomesM&M MEETING MINUTES
Waitemata DHB Mortality and Morbidity
Meeting Report
Department: Endoscopy Chair: Dr Zoe Raos
Secretary:Alison Bowman (CNM)
Division: NSH – Specialist Medicine
Date: 09/02/18 Time:0915-1000 Venue: Radiology
Conference Room
LGF
Attendees:
Nurses: 3
Doctors: 14
OP Managers: 1
Clerical Staff: 1 Other: HCA: 1
Number of cases to date: 7
Reviewed: 15 Morbidity cases: 3
Open: 2 Complaint cases: 0
Closed:13 Cases of significant learning: 9
Mortality cases:2 Cases presenting today: 3
1. Actions from previous meetings:
Case Review Recommendation Action Perso
Resp
1. Mortality Case Inappropriate Referral Advocate to
73 yr old Female – Morbid Obesity due to unstable pt. support
– Upper GI bleed System failure – Gastro Service Zoe
NFR gastroenterologist Cover weekly Raos
review service. to D Wong
Hx: Diabetic, Gout, Asthma Pt care changing
Pelvic Mass - +Comorbidities multiple times. Ali J Systemic Fail
2/7 Diarrhoea/Vomiting – Malena – Reg hndovr
Query ICU not to Reg,
Tx: Pre Gastro Work Up accepting the pt when unrecognised
Restrictive-Limited Full presenting so acutely depth of acute
Assessment unwell – WHY? unwellness.
Delayed IVF commencement Scoping, required SMO perhaps
X1 N/Saline overnight need from ICU not supprtve
X2 units RBC prior to Gastroscope intensivetist. John P enough – ed
No handover on Hyperkalaemia training
on referral SMO communication requrd!
Hypotensive/Hypovolemic/ poor. No phone call
Hyperkalaemic – Renal Failure direct to gastro Case presentM&M OUTCOMES
• 32 cases reviewed over one year (previously 3 – 4per annum)
• 6 deaths, 26 harm, 3 near-miss
• broad range of case-types
• 38 recommendations generated
• 17 actions agreed from recommendations
5% completed,
71% partially completed
24% not yet started
• 59% of actions do not involve direct expenditure e.g. improve communication & care pathwaysCONCLUSION
M&M Gastroenterology at WDHB has exceeded
expectations, including recordable improvements for
patient safety.
Multidisciplinary Staff engagement – Collegial
communication with a shared understanding of
respective pressures – All improved, aimed to
serve Risk Management and Quality Service Delivery
in a timely manner.
Supporting the growth of an inclusive team culture
model with an open and transparent learning
process in a No Blame Environment – Your Voice
Matters!
REFERENCES
Conducting & Reporting Clinical Review/Morbidity & Mortality
Meetings – Clinical Excellence Commission. Oct 2016 Sydney NSW
The American Journal of Surgery (2012) 203, 26–31
The Association for Surgical Education, SBAR M&M: a feasible, reliable, and valid tool to
assess the quality of, surgical morbidity and mortality conference presentations
Erica L. Mitchell, M.D.a, Dae Y. Lee, M.D.a, Sonal Arora, M.D., Ph.D.b,
Karen L. Kwong, M.D.a, Timothy K. Liem, M.D.a, Gregory L. Landry, M.D., M.R.C.a,
Gregory L. Moneta, M.D.a, Nick Sevdalis, Ph.D.b
ANAESTHESIA MORBIDITY & MORTALITY MEETINGS
A Practical Toolkit For Improvement - Oct 2013
(REPRINTED) ARCH SURG/VOL 144 (NO. 4), APR 2009 WWW.ARCHSURG.COM
development of an Online Morbidity, Mortality, and Near-Miss Reporting System to Identify
patterns of Adverse Events in Surgical Patients
Karl Y. Bilimoria, MD, MS; Thomas E. Kmiecik, PhD; Debra A. DaRosa, PhD; Amy Halverson, MD;
Mark K. Eskandari, MD; Richard H. Bell Jr, MD; Nathaniel J. Soper, MD; Jeffrey D. Wayne, MDYou can also read