Acute Concussion Symptom Severity and Delayed Symptom Resolution
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Acute Concussion Symptom Severity and Delayed
Symptom Resolution
WHAT’S KNOWN ON THIS SUBJECT: Children are often evaluated AUTHORS: Joseph A. Grubenhoff, MD,a,b Sara J. Deakyne,
in the emergency department after a concussion. Although MPH,c Lina Brou, MPH,a,b Lalit Bajaj, MD, MPH,a,b R. Dawn
prolonged symptoms are associated with higher initial symptom Comstock, PhD,a,d and Michael W. Kirkwood, PhDe
severity when measured 2 to 3 weeks after injury, a similar Departments of aPediatrics, and ePhysical Medicine and
association with acute symptom severity has not been Rehabilitation, University of Colorado, Aurora, Colorado;
bEmergency Department, and cDepartment of Research
demonstrated.
Informatics, Children’s Hospital Colorado, Aurora, Colorado;
and dDepartment of Epidemiology, Colorado School of Public
WHAT THIS STUDY ADDS: Higher acute symptom severity is not Health, Aurora, Colorado
associated with development of persistent post-concussion KEY WORDS
symptoms 1 month after injury, but persistent post-concussive brain concussion, brain injury, acute, brain injury, traumatic,
symptoms affect a significant number of children after post-concussion symptoms, post-concussion syndrome,
concussion. Outpatient follow-up is essential to identify children emergency medicine
who develop persistent symptoms. ABBREVIATIONS
AUC—area under the curve
CI—confidence interval
DSR—delayed symptom resolution
ED—emergency department
GCS—Glasgow Coma Scale
abstract IQR—interquartile range
LOC—loss of consciousness
BACKGROUND AND OBJECTIVES: Up to 30% of children who have concus- ICD-10—International Statistical Classification of Diseases and
sion initially evaluated in the emergency department (ED) display delayed Related Health Problems, 10th revision
OR—odds ratio
symptom resolution (DSR). Greater initial symptom severity may be an
PCS—post-concussion syndrome
easily quantifiable predictor of DSR. We hypothesized that greater symp- RR—relative risk
tom severity immediately after injury increases the risk for DSR. Dr Grubenhoff conceptualized and designed the study, designed
METHODS: We conducted a prospective longitudinal cohort study of chil- the database, oversaw data collection and analysis, drafted the
initial manuscript, and reviewed and revised the manuscript; Ms
dren 8 to 18 years old presenting to the ED with concussion. Acute symp-
Deakyne performed the primary statistical analysis, assisted
tom severity was assessed using a graded symptom inventory. Presence of with study design and database design, managed study
DSR was assessed 1 month later. Graded symptom inventory scores were personnel in recruitment and data acquisition, and co-authored,
tested for association with DSR by sensitivity analysis. We conducted a sim- reviewed, and revised the manuscript; Ms Brou assisted with
the cluster analysis and drafting and reviewed and revised the
ilar analysis for post-concussion syndrome (PCS) as defined by the
manuscript; Dr Bajaj assisted with study design and study
International Statistical Classification of Diseases and Related Health personnel management, oversaw data analysis, and critically
Problems, 10th revision. Potential symptoms characteristic of DSR were reviewed and revised the manuscript; Dr Comstock assisted
explored by using hierarchical cluster analysis. with data analysis and interpretation and critically reviewed and
revised the manuscript; Dr Kirkwood conceptualized and
RESULTS: We enrolled 234 subjects; 179 (76%) completed follow-up. Thirty- designed the study, assisted with data instrument design, and
eight subjects (21%) experienced DSR. Initial symptom severity was not co-authored, reviewed, and revised the manuscript; and all
significantly associated with DSR 1 month after concussion. A total of 22 authors approved the final manuscript as submitted.
subjects (12%) had PCS. Scores .10 (possible range, 0–28) were www.pediatrics.org/cgi/doi/10.1542/peds.2013-2988
associated with an increased risk for PCS (RR, 3.1; 95% confidence doi:10.1542/peds.2013-2988
interval 1.2–8.0). Three of 6 of the most characteristic symptoms of DSR Accepted for publication Apr 10, 2014
were also most characteristic of early symptom resolution. However, Address correspondence to Joseph A. Grubenhoff, MD, 13123 East
cognitive symptoms were more characteristic of subjects reporting DSR. 16th Ave, B-251, Aurora, CO 80045. E-mail: joe.grubenhoff@
childrenscolorado.org
CONCLUSIONS: Greater symptom severity measured at ED presentation
does not predict DSR but is associated with PCS. Risk stratification there- (Continued on last page)
fore depends on how the persistent symptoms are defined. Cognitive
symptoms may warrant particular attention in future study. Follow-up is
recommended for all patients after ED evaluation of concussion to
monitor for DSR. Pediatrics 2014;134:54–62
54 GRUBENHOFF et al
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015ARTICLE
There are 630 000 emergency depart- severity of acute concussion symptoms a convenience sample of children ages
ment (ED) visits annually for mild trau- may be a useful indicator of overall se- 8 to 18 years who sustained con-
matic brain injury (concussion) among verity, and therefore may constitute an cussions no .6 hours before present-
children ages 0 to 19 years.1 The ma- easily measurable risk factor to predict ing to Children’s Hospital Colorado’s
jority of those who have concussion DSR. Recent research among youth trauma center ED, which has ∼65 000
experience symptom resolution in a few athletes who have sports-related con- annual visits. Patients identified on the
weeks.2 However, a notable minority cussion supports this concept.20 ED electronic track board presenting
experience persistent post-concussive DSR is a defining feature of post- with complaints of head injury or symp-
sequelae. concussive syndrome (PCS). However, it toms associated with concussion were
When examining post-concussive se- is important to highlight that there is no screened for enrollment 16 hours per
quelae with standardized performance- universally accepted definition of PCS. day, 7 days per week by professional
based cognitive and behavioral tests, Indeed, whether the nonspecific symp- research assistants who enrolled sub-
most prospective studies indicate that by toms typically attributed to this condition jects and administered all study proce-
2 to 3 months post-injury, deficits are no constitute a syndrome with a common dures. Subjects were contacted by
longer apparent.2–6 Fewer studies have pathophysiological explanation is contro- telephone 30 days after injury to com-
systematically examined outcomes using versial.21,22 Nonetheless, DSR affects chil- plete follow-up procedures. Subjects
dren who have concussion, and evidence were considered lost to follow-up if they
post-concussive symptom reports from
suggests that the risk for experiencing failed to respond after 3 attempts. The
children. However, available research
persistent symptoms is modifiable.23–25 study was approved by the Colorado
suggests that some pediatric patients
Identifying children at increased risk for Multiple Institutional Review Board.
display more persistent symptoms than
might be expected if examining perfor- DSR at the time of injury would allow Subjects
mance-based test results alone.7,8 The selective implementation of interventions
Children were considered to have
acute injury risk factors predictive of earlier in the recovery phase.
concussion if they had a Glasgow Coma
delayed symptom resolution (DSR) in The primary objective of this study was Scale (GCS) score of 13 or 14 or at least
children are poorly understood. to determine whether greater symptom 2 of the following symptoms occurr-
Traditionally, determining the severity of severity measured immediately after ing after a direct blow to or rapid
concussion was predicated on the pre- injury is associated with DSR. We hy- acceleration/deceleration of the head:
sence of certain signs and symptoms at pothesized that higher scores on bystander-witnessed LOC; post-traumatic
the time of injury, most notably loss of a graded symptom inventory immedi- amnesia; disorientation to person,
consciousness (LOC).9,10 However, LOC ately after injury would be associated place, or time; subjective feelings of
occurs relatively infrequently after con- with the DSR at 1 month in a pediatric ED slowed thinking; perseveration; vomiting/
cussion and is no longer used to define cohort presenting for acute evaluation nausea; headache; diplopia/blurry vision;
injury severity as it is not consistently of concussion. Given the lack of a uni- dizziness; or somnolence. This clinical
associated with neuropsychological de- versally accepted definition of PCS, we definition of concussion has been used
ficits or DSR.11,12 In contrast, research also evaluated the performance of elsewhere.28,29 Children who had open
in adults who have concussion has a graded symptom inventory for iden- head injuries, intoxication with alcohol
found that post-traumatic amnesia as tifying the risk for meeting clinical or controlled substances, receipt of
criteria for PCS laid out in the In- narcotics for pain control, injuries re-
well as higher overall symptom levels
ternational Statistical Classification of sulting from child abuse, multisystem
(ie, both number and severity of symp-
Diseases and Related Health Problems, injuries, or underlying central nervous
toms) are associated with DSR.13–17 In
10th revision (ICD-10).26 Although ICD- system abnormalities were excluded.
pediatric patients, greater symptom
10 has not yet been adopted in the
levels present a few weeks after injury
United States for coding purposes, the Measurements
are associated with a longer duration of
clinical criteria for PCS have been in-
post-concussive symptoms.18 Greater At the ED enrollment visit, the following
vestigated in concussion research.14,27
symptom levels have also been associ- demographic and injury character-
ated with objective signs of altered METHODS istics were obtained: mechanism of
mental status (eg, post-traumatic am- injury; parental report of previous
nesia) in pediatric ED patients immedi- Study Design concussion; GCS score as determined
ately after injury.19 Taken together, these We conducted a prospective cohort study by the treating provider; and presence
findings suggest that the number and from October 1, 2010 to March 31, 2013 of of abnormalities on head CT scan as
PEDIATRICS Volume 134, Number 1, July 2014 55
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015reported by a board-certified pediatric have concussion, we planned to divide were conducted by using SAS 9.3 (SAS
neuroradiologist if obtained. the cohort into low and high acute Institute, Inc, Cary, NC) and hierarchical
Self-reported concussion symptoms symptom groups based on a defined clustering was conducted by using
were quantified by using a graded cut-off score on a graded symptom in- SPSS 22.0 (IBM SPSS Statistics, IBM
concussion symptom inventory. The ventory.32 We hypothesized that DSR Corporation, Chicago, IL).
symptom inventory included the 12 would be more prevalent in the high
items from the Concussion Symptom symptom group. Therefore, we esti- RESULTS
Inventory30 plus 2 additional items re- mated that a sample size of 202 subjects
Research assistants screened 1253
garding feeling irritable and sad. Sub- would be necessary to demonstrate
patients for participation; 273 met in-
jects verbally rated to what degree they a 15% absolute difference in prevalence clusion criteria and 234 subjects con-
were experiencing 14 symptoms com- of DSR between the low and high sented to participate in the study. Of
mon to concussion. We modified the symptom group, using 90% power and those enrolled, 179 subjects (76%)
instrument for our pediatric popula- 2-tailed a of 0.05. completed the 30-day follow-up call and
tion from a 0 to 6 point scale to a 0 to 2 Pre-injury scores for individual symp- comprised the study cohort (Fig 1).
point scale to ensure understanding toms were subtracted from both the Subjects who did not complete follow-
(range, 0–28). Parents rated their initial and 30-day follow-up scores to up were similar to those who did in
child’s symptom severity in the week account for the presence of these non- age, gender, initial GCS, mechanism of
before injury using the same in- specific symptoms before injury. Symp- injury, and history of previous concus-
strument to provide a pre-injury base- toms present before injury but absent sion. Subjects lost to follow-up had
line for these nonspecific symptoms. post-injury were scored as 0 (ie, a neg- significantly lower initial graded symp-
The primary outcome, DSR, was de- ative score was not assigned). De- tom inventory scores (median score, 7;
fined as the presence of 3 or more scriptive statistics for demographic and interquartile range [IQR], 4–12) com-
symptoms 1 month after injury that acute injury data were calculated as pared with subjects completing the
were absent or less severe in the week proportions or medians with inter- study (median score, 10; IQR, 7–13;
before injury reflective of findings in quartile ranges and compared by using P = .01).
similar cohorts.18 a x 2 test and Wilcoxon rank sum as Thirty-eight children (21%) from the
ICD-10 criteria for PCS require the appropriate. Because there is no de- study cohort met the study definition for
presence of 3 or more of the following 8 fined point separating low from high DSR. The pre-injury baseline symptom
symptoms 1 month after injury: head- symptoms, a sensitivity analysis was score differed significantly in both
ache, dizziness, fatigue, irritability, dif- performed by using the x2 statistic to groups, but the scores were low for both
ficulty in concentration or performing determine the best cut-point for initial groups (Table 1). Two subjects in the
mental tasks, impairment of memory, symptom severity scores to divide the early symptom resolution (ESR) group
insomnia, and reduced tolerance to low and high groups using DSR as the and 1 in the DSR group experienced
stress, emotional excitement, or alco- outcome. After sensitivity analysis, the a subsequent concussion in the follow-
hol.31 The criteria do not adjust for best cut-point score was used for mul- up period. Forty subjects underwent
symptoms present before injury as our tiple logistic regression, adjusting for head CT scan with only 5 abnormal
clinical definition did. Patients were gender and age, as symptom report findings, all found in the ESR group
considered to have PCS if they reported may vary by both age and gender.32–34 (Table 2).
3 or more symptoms on the Concussion The same methods were used The results of sensitivity analysis of
Symptom Inventory that aligned with substituting our clinical definition of initial symptom inventory scores rang-
PCS diagnostic criteria. There is no DSR with the PCS criteria. Results of x 2 ing from 8 to 14 are shown in Table 3.
corollary for “reduced tolerance to
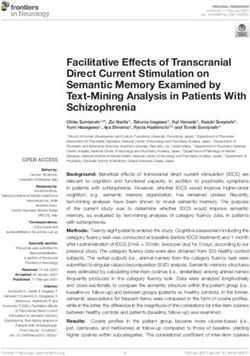
analysis were considered significant if P The receiver-operator characteristic
stress, emotional excitement, or alco-
, .05. Relative risk and odds ratios (OR) curve is shown in Fig 2 (area under the
hol” on the Concussion Symptom In-
were considered significant if the 95% curve [AUC], 0.508; 95% CI, 0.475–0.683;
ventory, so that symptom was excluded
confidence interval (CI) did not include P = .14, rounded). The best cut point
during analysis.
1. Lastly, we conducted hierarchical was a score of 11 with a sensitivity of
clustering with average linkage analysis 63% and a specificity of 50% for DSR.
Statistical Analysis to determine if certain symptoms were However, a score of 11 was not signif-
Based on a previous study examining more characteristic of delayed versus icantly associated with DSR (P = .46). In
symptom severity in ED patients who early symptom resolution.35 Analyses multivariate analysis, adjusting for age
56 GRUBENHOFF et al
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015ARTICLE
PCS in the high symptom versus low
symptom group was 3.7 (95% CI, 1.3–
10.6).
Figures 3 and 4 show the results of
cluster analysis. Three of the 6 most
characteristic initial symptoms in the
DSR and ESR groups (those in which
the relative linkage distance on the
x-axis are shortest) were similar (pho-
nophobia, photophobia, blurred, or dou-
ble vision). However, cognitive symptoms
(difficulty remembering, difficulty con-
centrating, or “feeling foggy”) were more
characteristic of the DSR group.
DISCUSSION
Our study of children 8 to 18 years old
presenting to an ED ,6 hours after
FIGURE 1 concussion demonstrated that initial
Study Participant Flow Diagram. symptom severity is not associated with
DSR. This is an important finding given
and gender, a score of 11 was still not in Fig 2 (AUC, 0.629; 95% CI, 0.509–0.748; evolving knowledge of concussion symp-
associated with DSR (OR, 1.4; 95% CI, P = .03). The best cut point was 10 with tom resolution. In 1988, Lishman pro-
0.7–2.8). a sensitivity of 77% and specificity of posed that symptoms appearing shortly
Twenty-two subjects (12%) met criteria 51% for PCS (P = .02). The relative risk after a concussion were primarily the
for PCS. Sensitivity analysis for initial for PCS in subjects who had an initial result of physiologic derangements di-
graded symptom scores ranging from 8 symptom score .10 was 3.1 (95% CI, rectly related to the injury, whereas
to 14 is shown in Table 4. The receiver- 1.2–8.0). In multivariate analysis, ad- protracted symptoms were more likely
operator characteristic curve is shown justing for age and gender, the OR for related to latent psychological factors.36
Two decades later, accumulated research
suggests that “physiogenic” and “psy-
TABLE 1 Demographic and Injury Characteristics for Early and Delayed Symptom Resolution chogenic” factors contribute to the con-
Groups
stellation of symptoms present both
ESR (n = 141) DSR (n = 38) Pa immediately after injury as well as
Demographics throughout recovery.37
Mean age, years (SD) 12.6 (2.5) 13.4 (2.2) .79
Male, % 70 66 .69 Intuitively, it is reasonable to assume
History of previous concussion, % 24 29 .53 that more severe acute physiologic in-
Injury characteristics
jury will manifest as more severe
Mechanism, % — — .79
Sport 48 53 — symptomatology and likely require
Fall 43 34 — a longer recovery period. Recent re-
Assault 3 5 — search supports this assumption. A
Motor vehicle collision 1 3 —
Other 5 5 — prospective cohort study of youth ath-
LOC, % 26 29 0.68 letes evaluated in sports concussion
Post-traumatic amnesia, % 26 34 0.42 clinics in the first 3 weeks after a con-
Received head CT scan in ED, % 21 26 0.52
Abnormal head CT scan results, % 4 0 0.02
cussion demonstrated that increasing
Initial GCS, medianb 15 15 0.99 initial graded symptom inventory
Preinjury graded symptom score, median (IQR) 1 (0–2) 2 (1–4) 0.002 scores were associated with increased
Initial ED graded symptom score, median (IQR) 9 (6–13) 10.5 (7–15) 0.14
odds of symptom resolution occurring
a x 2 was used to compare proportions and Wilcoxon rank sum to compare medians. x2 analysis compared the overall
difference among mechanism for the ESR and DSR groups and only this single p-value is provided.
beyond 28 days.20 Similarly, pediatric
b IQR for GCS was 15–15 for both groups. ED patients who had high symptom
PEDIATRICS Volume 134, Number 1, July 2014 57
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015TABLE 2 Characteristics of Subjects Who Had Abnormal Head CT Scans but our results differed from these
Age (y) Gender GCS LOC (+/2) Injuries previous reports. This suggests that
10.8 F 15 – Cerebral contusion acute symptom report alone is not an
10.0 M 14 – Subarachnoid and epidural hematoma, skull fracture accurate reflection of the physiologic
14.0 M 15 + Subdural hematoma
9.4 M 14 – Subarachnoid hematoma, skull fracture
and psychological factors that ulti-
10.1 M 15 + Subarachnoid hematoma mately lead to DSR.
We defined DSR in terms relevant to
TABLE 3 Sensitivity Analysis of Graded Symptom Inventory Scores for Identifying Delayed
clinical practice. Specifically, we de-
Symptom Resolution veloped a definition that would likely
Cut Point Sensitivity, % Specificity, % NPV, % PPV, % P prompt a primary care provider to refer
8 73 33 79 26 .66 a child for specialist evaluation (at least
9 71 33 81 22 .45 3 symptoms that are worse 1 month
10 71 35 82 23 .14 after injury than they were before in-
11 63 50 84 26 .46
12 53 55 81 24 .13
jury). Although the clinical criteria for
13 47 66 82 27 .19 PCS also require the presence of at least
14 37 74 81 27 .10 3 symptoms 1 month after concussion,
the diagnostic accuracy of this defini-
levels measured in the early weeks tation of concussion symptoms, there is tion is a topic of scientific debate as it is
after a concussion had significantly some evidence that the acute injury both subjective and imprecise.39–41
higher odds of symptoms persisting factors are stronger determinants of There is also significant controversy as
for up to 1 year.18 In both studies, initial symptom reports early in recovery, to whether the term “syndrome” is
symptom inventories were obtained an whereas non-injury factors contribute appropriate, given that common con-
average of 11 days after concussion. more to persistent symptoms.38 A cussion symptoms are also found in
Although both physiologic and psycho- strength of our study is that we en- patients who do not have concussion.42
logical factors contribute to manifes- rolled subjects within 6 hours of injury, Regardless of these shortcomings, PCS
FIGURE 2
ROC curves displaying sensitivity analysis of concussion symptom inventory scores for identifying delayed symptom resolution or post-concussive syndrome.
Optimal scores (closest to upper left of graph) for each outcome are shown along with the AUC and associated P value for each curve.
58 GRUBENHOFF et al
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015ARTICLE
TABLE 4 Sensitivity Analysis of Graded Symptom Inventory Scores for Identifying ICD-10 Post- different criteria for PCS showed that
Concussion Syndrome
a subset of 6 symptoms common to all 3
Cut Point Sensitivity, % Specificity, % NPV, % PPV, % P criteria was specific to PCS owing to
8 77 33 91 14 .46 concussion among adults.44 In contrast,
9 77 36 92 14 .34
10 77 51 94 18 .02
other work calls into question whether
11 64 55 92 17 .11 the symptoms included in various di-
12 55 66 91 18 .10 agnostic criteria are specific to con-
13 41 73 90 18 .21
cussion. Our results resemble those of
14 36 80 90 21 .10
McCauley, Boake, and colleagues, who
found wide variations in the prevalence
has been studied as an outcome mea- .10 was associated with a threefold of PCS, depending on the criteria
sure in studies of persistent symp- increased risk for PCS in our cohort, employed as well as a lack of specificity,
toms.27,43,44 Therefore, we repeated our whereas there was no association with because many adult patients who did
analysis using PCS as the outcome our clinical definition. not have head trauma also met PCS
rather than our clinical definition of One may conclude from these findings criteria.45,46 Additionally, although the
DSR. We noted 2 important findings. that the smaller subset of symptoms PCS ROC curve showed a statistically
First, we found a 43% relative decrease that meet criteria for PCS are more significant association (P = .034) be-
in prevalence in the outcome (9% ab- representative of a specific clinical entity tween an initial symptom severity score
solute difference) when applying this characterized by persistent symptoms of 10 and PCS, the absolute AUC of 0.629
alternate definition. Second, we showed than those found on broader symptom suggests no more than a modest re-
that a graded symptom inventory score inventories. An analysis comparing 3 lationship. Therefore, concluding that
FIGURE 3
Hierarchical cluster analysis for participants who had early symptom resolution. Shorter relative cluster linkage distances on the x-axis indicate symptoms
(y-axis) that are more characteristic of the group, whereas longer distances indicate symptoms that are less characteristic.
PEDIATRICS Volume 134, Number 1, July 2014 59
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015FIGURE 4
Hierarchical cluster analysis for participants who had delayed symptom resolution. Shorter relative cluster linkage distances on the x-axis indicate symptoms
(y-axis) that are more characteristic of the group, whereas longer distances indicate symptoms that are less characteristic.
PCS criteria are more representative of specific symptoms are more closely fying children who, at the time of their
a unique clinical syndrome is difficult to associated.14,48 The exploratory na- concussion, are at risk for DSR. We did
justify and suggests that accurate risk ture of cluster analysis prevents not perform serial assessments to
stratification is heavily dependent on drawing firm conclusions regarding determine the precise day of symptom
how the outcome is defined. the ability of these symptoms to pre- resolution or the range of symptom
Hierarchical cluster analysis is an ex- dict DSR. However, cognitive symp- duration. It is possible that some sub-
ploratory method that aims to dem- toms may warrant particular scrutiny jects in the DSR group had resolution of
onstrate which features are most when present. symptoms shortly after their 30-day
characteristic of a group. Three of the 6 We experienced a lost-to-follow-up rate follow-up call and were misclassified.
most characteristic symptoms for both of 24%. The subjects lost to follow-up However, the prevalence of DSR in this
the DSR and ESR groups were identical in had a significantly lower median ini- study was 21% compared with studies
our cohort, suggesting that these symp- tial symptom score than the final study in other US pediatric ED cohorts 3
toms (phonophobia, photophobia, blur- cohort. It is plausible that most of these months after concussion, which ranged
red or double vision) may not be useful in subjects would have fallen into the ESR from 15% to 29%, so this limitation is
identifying those at risk for DSR. However, group but did not complete the study unlikely to have had a significant impact
we found it interesting that cognitive owing to resolution of symptoms.49 If on our results.50,51
symptoms were more characteristic of true, the absence of these patients Finally, we did not include a control
subjects who had DSR. Although some from analysis would tend to bias our group who had injuries to body regions
authorshavefoundastrongerassociation results toward the null hypothesis. other than the head. Although children
between the number of initial symptoms Our follow-up period was limited to 30 who have concussion tend to report
and DSR,17,47 others have shown that days, as we were interested in identi- more post-concussive symptoms than
60 GRUBENHOFF et al
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015ARTICLE
children with orthopedic injuries, there specificity further emphasizes the need sequelae and that accounts for the
is considerable overlap in symptom re- for more accurate definitions related to contribution of both physiologic and
port, highlighting the non-specific na- sequelae after concussion. psychological processes. Given the in-
ture of post-concussive symptoms.29 We ability to predict the resolution of post-
are therefore unable to evaluate what CONCLUSIONS concussive symptoms at the time of
proportion of symptoms is simply at- Greater symptom severity at the time of injury, outpatient follow-up and serial
tributable to injury in general and what injury does not predict DSR among symptom assessment should be a cor-
proportion is attributable to concus- children presenting to the ED for eval- nerstone of concussion management
sion specifically. Our objective, how- uation of concussion, but it is a risk for all children after ED discharge.
ever, was to determine whether acute factor for meeting criteria for PCS as
symptom severity could be used for defined by ICD-10. These findings un- ACKNOWLEDGMENTS
risk-stratification among head-injured derscore the need to refine the defini- We thank Kendra Kocher, BS, who pro-
children rather than as a diagnostic tion of post-concussive syndrome to one vided study coordination and database
tool. Nonetheless, the issue of symptom that is truly representative of concussion management.
REFERENCES
1. Faul MXL, Wald MM, Coronado VG. Trau- 9. Leclerc S, Lassonde M, Delaney JS, Lacroix 18. Yeates KO, Taylor HG, Rusin J, et al. Longi-
matic Brain Injury in the United States: VJ, Johnston KM. Recommendations for tudinal trajectories of postconcussive
Emergency Department Visits. Hospital- grading of concussion in athletes. Sports symptoms in children with mild traumatic
izations and Deaths 2002–2006. Atlanta, GA: Med. 2001;31(8):629–636 brain injuries and their relationship to
Centers for Disease Control and Pre- 10. Kelly JP, Rosenberg JH. The development of acute clinical status. Pediatrics. 2009;123
vention, National Center for Injury Pre- guidelines for the management of concus- (3):735–743
vention and Control; 2010 sion in sports. J Head Trauma Rehabil. 19. Grubenhoff JA, Kirkwood MW, Deakyne S,
2. Carroll LJ, Cassidy JD, Peloso PM, et al; 1998;13(2):53–65 Wathen J. Detailed concussion symptom
WHO Collaborating Centre Task Force on 11. Lovell MR, Iverson GL, Collins MW, McKeag analysis in a paediatric ED population.
Mild Traumatic Brain Injury. Prognosis for D, Maroon JC. Does loss of consciousness Brain Inj. 2011;25(10):943–949
mild traumatic brain injury: results of the predict neuropsychological decrements af- 20. Meehan WP III, Mannix RC, Stracciolini A,
WHO Collaborating Centre Task Force on ter concussion? Clin J Sport Med. 1999;9 Elbin RJ, Collins MW. Symptom severity
Mild Traumatic Brain Injury. J Rehabil Med. (4):193–198 predicts prolonged recovery after sport-
2004; (43, suppl)84–105 12. Erlanger D, Kaushik T, Cantu R, et al. Symptom- related concussion, but age and amnesia
3. Satz P, Zaucha K, McCleary C, Light R, based assessment of the severity of a con- do not. J Pediatr. 2013;163(3):721–725
Asarnow R, Becker D. Mild head injury in cussion. J Neurosurg. 2003;98(3):477–484 21. Iverson GL. Misdiagnosis of the persistent
children and adolescents: a review of 13. King NS, Crawford S, Wenden FJ, Caldwell postconcussion syndrome in patients with
studies (1970-1995). Psychol Bull. 1997;122 FE, Wade DT. Early prediction of persisting depression. Arch Clin Neuropsychol. 2006;
(2):107–131 post-concussion symptoms following mild 21(4):303–310
4. Satz P. Mild head injury in children and and moderate head injuries. Br J Clin 22. Garden N, Sullivan KA. An examination of
adolescents. Curr Dir Psychol Sci. 2001;10: Psychol. 1999;38(pt 1):15–25 the base rates of post-concussion symp-
106–109 14. Yang CC, Hua MS, Tu YK, Huang SJ. Early toms: the influence of demographics and
5. Babikian T, Asarnow R. Neurocognitive clinical characteristics of patients with depression. Appl Neuropsychol. 2010;17(1):
outcomes and recovery after pediatric TBI: persistent post-concussion symptoms: 1–7
meta-analytic review of the literature. a prospective study. Brain Inj. 2009;23(4): 23. Ponsford J, Willmott C, Rothwell A, et al.
Neuropsychology. 2009;23(3):283–296 299–306 Impact of early intervention on outcome
6. Belanger HG, Vanderploeg RD. The neuro- 15. Sheedy J, Geffen G, Donnelly J, Faux S. following mild head injury in adults.
psychological impact of sports-related Emergency department assessment of mild J Neurol Neurosurg Psychiatry. 2002;73(3):
concussion: a meta-analysis. J Int Neuro- traumatic brain injury and prediction of 330–332
psychol Soc. 2005;11(4):345–357 post-concussion symptoms at one month 24. Wade DT, King NS, Wenden FJ, Crawford S,
7. Barlow KM, Crawford S, Stevenson A, post injury. J Clin Exp Neuropsychol. 2006; Caldwell FE. Routine follow up after head
Sandhu SS, Belanger F, Dewey D. Epide- 28(5):755–772 injury: a second randomised controlled
miology of postconcussion syndrome in 16. Drake AI, McDonald EC, Magnus NE, Gray N, trial. J Neurol Neurosurg Psychiatry. 1998;
pediatric mild traumatic brain injury. Pe- Gottshall K. Utility of Glasgow Coma Scale- 65(2):177–183
diatrics. 2010;126(2). Available at: www. Extended in symptom prediction following 25. Mittenberg W, Tremont G, Zielinski RE,
pediatrics.org/cgi/content/full/126/2/e374 mild traumatic brain injury. Brain Inj. 2006; Fichera S, Rayls KR. Cognitive-behavioral
8. Yeates KO. Mild traumatic brain injury and 20(5):469–475 prevention of postconcussion syndrome.
postconcussive symptoms in children and 17. Lundin A, de Boussard C, Edman G, Borg J. Arch Clin Neuropsychol. 1996;11(2):139–145
adolescents. J Int Neuropsychol Soc. 2010; Symptoms and disability until 3 months 26. Boake C, McCauley SR, Levin HS, et al.
16(6):953–960 after mild TBI. Brain Inj. 2006;20(8):799–806 Limited agreement between criteria-based
PEDIATRICS Volume 134, Number 1, July 2014 61
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015diagnoses of postconcussional syndrome. J 35. Beckstead JW. Using hierarchical cluster 44. Laborey M, Masson F, Ribéreau-Gayon R,
Neuropsychiatry Clin Neurosci. 2004;16(4): analysis in nursing research. West J Nurs Zongo D, Salmi LR, Lagarde E. Specificity of
493–499 Res. 2002;24(3):307–319 postconcussion symptoms at 3 months af-
27. Iverson GL, Lange RT. Examination of “post- 36. Lishman WA. Physiogenesis and psycho- ter mild traumatic brain injury: results
concussion-like” symptoms in a healthy genesis in the ’post-concussional syn- from a comparative cohort study. J Head
sample. Appl Neuropsychol. 2003;10(3):137– drome’. Br J Psychol. 1988;153(10):460–469 Trauma Rehabil. 2014;29(1):E28–E36
144 37. Silverberg ND, Iverson GL. Etiology of the 45. McCauley SR, Boake C, Pedroza C, et al.
28. Taylor HG, Dietrich A, Nuss K, et al. Post- post-concussion syndrome: physiogenesis Postconcussional disorder: Are the DSM-IV
concussive symptoms in children with and psychogenesis revisited. Neuro- criteria an improvement over the ICD-10? J
mild traumatic brain injury. Neuropsychol- Rehabilitation. 2011;29(4):317–329 Nerv Ment Dis. 2005;193(8):540–550
ogy. 2010;24(2):148–159 38. McNally KA, Bangert B, Dietrich A, et al. 46. Boake C, McCauley SR, Levin HS, et al. Di-
29. Moran LM, Taylor HG, Rusin J, et al. Do Injury versus noninjury factors as pre- agnostic criteria for postconcussional
postconcussive symptoms discriminate in- dictors of postconcussive symptoms fol- syndrome after mild to moderate trau-
jury severity in pediatric mild traumatic lowing mild traumatic brain injury in matic brain injury. J Neuropsychiatry Clin
brain injury? J Head Trauma Rehabil. 2011; children. Neuropsychology. 2013;27(1):1–12 Neurosci. 2005;17(3):350–356
26(5):348–354 39. Frances A. The new crisis in confidence in 47. Chrisman SP, Rivara FP, Schiff MA, Zhou C,
30. Randolph C, Millis S, Barr WB, et al. Concus- psychiatric diagnosis. Ann Intern Med. Comstock RD. Risk factors for concussive
sion symptom inventory: an empirically de- 2013;159(3):221–222 symptoms 1 week or longer in high school
rived scale for monitoring resolution of 40. Kendell R, Jablensky A. Distinguishing be- athletes. Brain Inj. 2013;27(1):1–9
symptoms following sport-related concussion. tween the validity and utility of psychiatric 48. De Kruijk JR, Leffers P, Menheere PP,
Arch Clin Neuropsychol. 2009;24(3):219–229 diagnoses. Am J Psychiatry. 2003;160(1):4– Meerhoff S, Rutten J, Twijnstra A. Prediction
31. World Health Organization. The ICD-10 12 of post-traumatic complaints after mild
Classification of Mental and Behavioral 41. Carroll CP, Cochran JA, Guse CE, Wang MC. traumatic brain injury: early symptoms and
Disorders: Clinical Description and Di- Are we underestimating the burden of biochemical markers. J Neurol Neurosurg
agnostic Guidelines. Geneva: World Health traumatic brain injury? Surveillance of se- Psychiatry. 2002;73(6):727–732
Organization; 1992 vere traumatic brain injury using Centers 49. Blinman TA, Houseknecht E, Snyder C, Wiebe
32. Grubenhoff JA, Kirkwood M, Gao D, Deakyne for Disease Control International Classifi- DJ, Nance ML. Postconcussive symptoms in
S, Wathen J. Evaluation of the standardized cation of Disease, 9th revision, Clinical hospitalized pediatric patients after mild
assessment of concussion in a pediatric Modification, Traumatic Brain Injury Codes. traumatic brain injury. J Pediatr Surg. 2009;
emergency department. Pediatrics. 2010; Neurosurg. 2012;71(6):1064–1070; discus- 44(6):1223–1228
126(4):688–695 sion 1070 50. Eisenberg MA, Andrea J, Meehan W, Mannix
33. Frommer LJ, Gurka KK, Cross KM, Ingersoll 42. Meares S, Shores EA, Taylor AJ, et al. Mild R. Time interval between concussions and
CD, Comstock RD, Saliba SA. Sex differences traumatic brain injury does not predict symptom duration. Pediatrics. 2013;132(1):
in concussion symptoms of high school acute postconcussion syndrome. J Neurol 8–17
athletes. J Athl Train. 2011;46(1):76–84 Neurosurg Psychiatry. 2008;79(3):300–306 51. Babcock L, Byczkowski T, Wade SL, Ho M,
34. Berz K, Divine J, Foss KB, Heyl R, Ford KR, 43. Yang CC, Tu YK, Hua MS, Huang SJ. The Mookerjee S, Bazarian JJ. Predicting post-
Myer GD. Sex-specific differences in the se- association between the postconcussion concussion syndrome after mild traumatic
verity of symptoms and recovery rate fol- symptoms and clinical outcomes for brain injury in children and adolescents
lowing sports-related concussion in young patients with mild traumatic brain injury. J who present to the emergency department.
athletes. Phys Sportsmed. 2013;41(2):58–63 Trauma. 2007;62(3):657–663 JAMA Pediatr. 2013;167(2):156–161
(Continued from first page)
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Funding for the conduct of this study was provided by a Thrasher Research Fund Early Career Award to Dr Grubenhoff. Use of REDCap Database was
supported by NIH/NCATS Colorado CTSI grant UL1 TR000154. Contents are the authors’ sole responsibility and do not necessarily represent official NIH or Thrasher
Research Fund views.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
62 GRUBENHOFF et al
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015Acute Concussion Symptom Severity and Delayed Symptom Resolution
Joseph A. Grubenhoff, Sara J. Deakyne, Lina Brou, Lalit Bajaj, R. Dawn Comstock
and Michael W. Kirkwood
Pediatrics 2014;134;54; originally published online June 23, 2014;
DOI: 10.1542/peds.2013-2988
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/134/1/54.full.ht
ml
References This article cites 48 articles, 13 of which can be accessed free
at:
http://pediatrics.aappublications.org/content/134/1/54.full.ht
ml#ref-list-1
Citations This article has been cited by 2 HighWire-hosted articles:
http://pediatrics.aappublications.org/content/134/1/54.full.ht
ml#related-urls
Permissions & Licensing Information about reproducing this article in parts (figures,
tables) or in its entirety can be found online at:
http://pediatrics.aappublications.org/site/misc/Permissions.xh
tml
Reprints Information about ordering reprints can be found online:
http://pediatrics.aappublications.org/site/misc/reprints.xhtml
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned, published,
and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk
Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015Acute Concussion Symptom Severity and Delayed Symptom Resolution
Joseph A. Grubenhoff, Sara J. Deakyne, Lina Brou, Lalit Bajaj, R. Dawn Comstock
and Michael W. Kirkwood
Pediatrics 2014;134;54; originally published online June 23, 2014;
DOI: 10.1542/peds.2013-2988
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/134/1/54.full.html
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned,
published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point
Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org by guest on May 23, 2015You can also read