Acid-Base Management in Critically Ill Patients with Buffers and Renal Replacement Therapy - AKI & CRRT 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Acid-Base Management in Critically Ill Patients with Buffers and Renal Replacement Therapy AKI & CRRT 2021 Lenar Yessayan, MD, MS University of Michigan

No Disclosures

Objectives: • Understand the principles of acid-base management with buffers and RRT in critically ill patients • Understand the role and limitation of RRT in lactic acidosis • Understand the role of RRT in select cases of drug poisoning associated with metabolic acidosis
Decrease myocardial Creates coagulopathy Impairs lymphocyte contractility cytotoxicity & proliferation Decrease Response to Induces inflammatory catecholamine's mediators Acute Metabolic Acidosis Dampens WBC Vasodilation bactericidal activity Increased protein Arrhythmias Hyperkalemia degradation Pulmonary Decreased glycolysis Insulin resistance vasoconstriction

The Incidence and Prognosis of Severe Metabolic or Mixed Acidemia within The First 24 hours of ICU 155 patients admitted with Metabolic or Mixed Severe Acidosis plasma pH level lower than 7.20 Others 14% Acute renal failure 3% Septic shock 35% Acute respiratory failure 12% Multiple trauma 7% Incidence 6% Cardiac arrest Cardiogenic Hemorrhagic shock shock 12% 7% 10% ICU mortality rate of 57%. Jung et al. Critical Care 2011, 15:R238
Prevalence of specific interventions and survival in patients admitted with Metabolic or Mixed Severe Acidosis 100% 88% 90% 83% 80% 70% 60% 57% 50% 40% 37% 30% 20% 20% 10% General features of acid-base metabolism evaluated during 0% the first three days. (A) pH. (B) Bicarbonatemia. *P < 0.05, Vasopressor Renal replacement Mechanical Sodium ICU mortality administration therapy within ventilation within bicarbonate Tukey's post hoc analysis between survivors (n = 66) and upon ICU first 24 hours of first 24 hours of administration admission ICU stay ICU stay within first 24 nonsurvivors (n = 89). #P < 0.05, Tukey's post hoc analysis vs day hours of ICU stay 0. Bars represent standard deviations. NS = not significant. PaCO2 = partial pressure of carbon dioxide. Jung et al. Critical Care 2011, 15:R238

Metabolic Acidosis in Critically ill patients Normal corrected AG Corrected AG >12 mEq/L (Hyperchloremic acidosis) • Lactic acidosis • NaCl 0.9 % infusion • Ketones • Gastrointestinal losses: • End-stage renal failure/AKI • Diarrhea Drug intoxications: • Small bowel/pancreatic drainage • Salicylate intoxication • Ureteroenterostomy • Methanol intoxication • Early renal insufficiency • Ethylene glycol intoxication • Parenteral nutrition
Bases and Base Delivery Systems for Treatment of Acute Metabolic Acidosis THAM (tris- hydroxymethyl NaHCO3 aminomethane) Plasma-lyte CVVH Ringer Lactate Hemodialysis CVVHDF CVVHD
Ion/solute Lactate Plasmalyte concentration Ringers Na+ mM 130 140 K+ mM 4 5 Ca++ mM 1.5 Mg++ mM 1.5 Cl- mM 109 98 Lactate- mM 28 Acetate- mM 27 Gluconate- mM 23 Osmolarity mOsm 274 295
~60%-85% of Gluconate Lactate Acetate Gluconate is excreted ? Acetate is mostly metabolized in unchanged in urine, ? Lactate Dehydrogenase tissues, lesser extent in liver some is converted to glucose Glucose Pyruvate Lactate is mostly metabolized in the Pyruvate Dehydrogenase Embden-Meyerhof liver, lesser extent in tissues Pathway Coenzyme A Acetyl-CoA Oxaloacetate 1 mol of acetate à 1 mol of bicarbonate Citrate synthase H+ 1 mol of lactate à 1 mol of bicarbonate Citrate Citric Acid Cycle CO2 H2O
All arguments against the use of LR as crystalloid in ICU LR will elevate LR is expensive the lactate level LR isn't compatible with LR is not safe in some drugs hyperkalemia
Lactated Ringers is safe in hyperkalemia • LR [K+] < patient [K+] with hyperkalemia. • Administering LR to a patient with hyperkalemia will tend to pull the patient's potassium towards 4 mEq/L • Saline causes acidosis, causing potassium to shift into the blood. H+ K+ K+ K+
What about Plasmalyte or Normosol? • Plasmalyte[K+]=5 mEq/L • Not capable of causing [K+]> 5 mEq/L) • Alkalinizing: • Shift of potassium into cells K+ K+
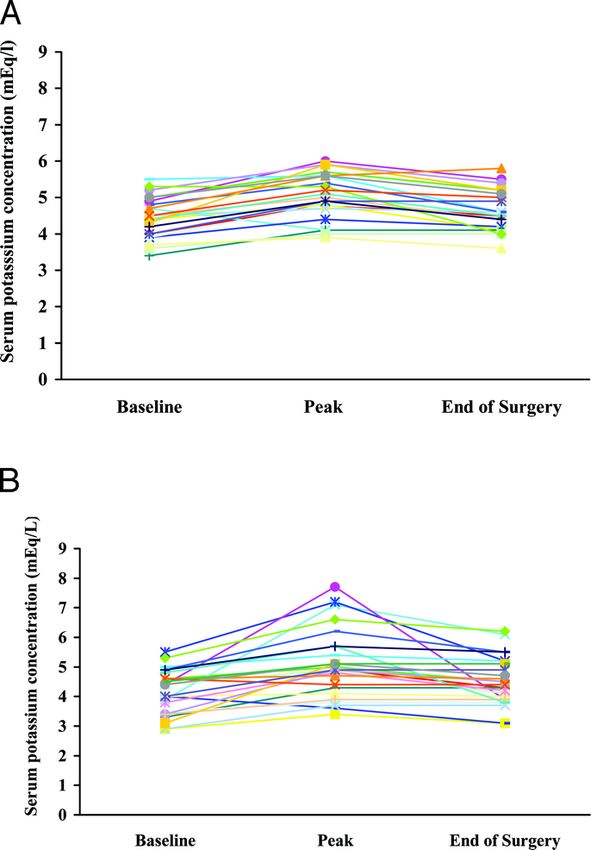
A Randomized, Double-Blind Comparison of Lactated Ringer’s Solution and 0.9% NaCl During Renal Transplantation LR: 25 patients NS: 26 patients • Peak intraoperative K+ 5.1 ± 1.1 • Peak intraoperative K+ 5.1 ± 0.6 mEq/L mEq/L • K+>6 mEq/L in 0/26 (0%) • K+>6 mEq/L in 5/26 (19%) • All required treatment Perioperative potassium concentrations in Perioperative potassium concentrations in LR- treated patients NS- treated patients O'Malley 2005
All arguments against the use of LR LR will elevate LR is expensive the lactate level LR isn't compatible with LR is not safe in some drugs hyperkalemia
DOES INTRAVENOUS LACTATED RINGER’S SOLUTION RAISE SERUM LACTATE? Δ lactate 0.93 mmol/L (95% CI 0.42–1.44 mmol/L) lactate increased in 14/15 subjects in the LR group 6/15 lactate levels >2 mmol/L Conclusion: a modest but significant rise in mean serum 30 volunteers lactate was seen after a 30 cc/kg LR bolus Raise the lactate level by ~0.5 mM higher than a bolus of NS Δ lactate 0.37 mmol/L (95% CI 0.26 mmol/L–1.00 mmol/L) Lactate increased in 7/15 in the NS group, 2/15 lactate levels >2 mmol/L Zitek et al. Journal of Emergency Medicine, Volume 55, Issue 3, 313 – 318
All arguments against the use of LR LR will elevate LR is expensive the lactate level LR isn't compatible with LR is not safe in some drugs hyperkalemia
All arguments against the use of LR LR will elevate LR is expensive the lactate level LR isn't compatible with LR is not safe in some drugs hyperkalemia
SMART SALT-ED Design Single Center, Pragmatic, Un-blinded, Interventional trial Setting 5 ICU ED/Floor Intervention Saline vs Balanced solution Number of patients 15802 13,347 Fluid Allocation Alternated monthly Outcomes Balanced Saline Balanced Saline MAKE 30 14.3% 15.4% 4.7% 5.6% (Primary Outcome SMART) ICU-free days in first 28 days 25.3 25.3 _ _ Hospital free days in first 28 days _ _ 25 25 (Primary outcome SALTED) Death 10.3% 11.1% 1.4% 1.6% RRT 2.5% 2.9% 0.3% 0.5% Persistent kidney dysfunction 6.4% 6.6% 3.8% 4.5% AKI (stage 2 or higher) 10.7% 11.5% 8.0% 8.6%
Further studies are ongoing regarding the selection of saline versus balanced crystalloids Study protocol for the Balanced Solution versus The Plasma-Lyte 148 v Saline (PLUS) study Saline in Intensive Care Study (BaSICS): a factorial protocol: a multicenter, randomized controlled trial randomized trial: of the effect of intensive care fluid therapy on mortality Methods: Methods: 11000 Patients will be randomized to receive Plasma- 8800 patients will be randomized to either Plasma-Lyte Lyte 148 or saline, and to rapid infusion (999 mL/h) or 148 or saline for all resuscitation fluid, maintenance fluid slow infusion (333 mL/h). and compatible drug dilution therapy while in the ICU for up to 90 days after randomization. OUTCOMES: OUTCOMES: The primary outcome: The primary outcome • 90-day all-cause mortality. • 90-day all-cause mortality Secondary outcomes: Secondary outcomes: • Incidence of renal failure requiring renal replacement • Incidence of renal replacement therapy therapy within 90 days • Incidence and duration of vasoactive drug treatment, • Incidence of acute kidney injury • Duration of mechanical ventilation • Incidence of non-renal organ dysfunction at Days 3 • ICU and hospital length of stay and 7, Number of mechanical ventilation free days • Quality of life and health services use at 6 months within the first 28 days after randomization
Do we really need any additional trials? Do you care about the pH, Hyperchloremia and Acidosis ? Use any fluid Use Balanced Crystalloids Stop checking electrolytes Stop checking ABG
Should predominantly lactic acidosis be corrected by buffer infusion? Positive Negative
Trial Year Design Patient population Intervention or Outcome comparison Cooper 1991 RCT 14 pts in septic shock with lactic NaHCO3 vs. No ≠ in CO, BP, PCWP, et al. acidosis requiring vasopressors 0.9 saline vasopressor need. ↓ iCa & ↑ETT CO2 Mathieu 1992 RCT 10 pts with lactic acidosis requiring NaHCO3 vs. No ≠ in CO, BP, PCWP or tissue et al. pressors w/o severe renal failure 0.9 saline O2 levels Mark et 1993 RCT 40 pts with CAD with Intraop ↓ in NaHCO3 vs. No ≠in total VO2, CO, lactate al. plasma HCO3 of >3mM 0.9 saline production Stacpool 1994 RCT 126 pts with lactic acidosis Dichloroacetat No improvement in acid base e et al e vs. Placebo nor hemodynamics Fang et 2008 RCT 94 pts with severe sepsis/septic 0.9 saline No ≠ in CO, MAP, HR, RR 2 or 8 al. shock with or w/o lactic acidosis. 3.5% NaCl hrs. 5% NaHCO3 No ≠ in 28 day mortality El Solh 2010 Observational 36 pts with septic shock, lactic NaHCO3 vs. ↓ ICU LOS, ↓ Vent days. No ≠ et al. acidosis and pH
Sodium bicarbonate therapy for patients with severe metabolic acidemia in the intensive care unit (BICAR-ICU): a multicenter, open-label, randomized controlled, phase 3 trial Stratified randomization according to three pre- specified factors: • Age with a cutoff of 65 years • Presence or absence of suspected sepsis • Presence or absence of moderate to severe AKI (AKIN) ≥ 2 Patient Characteristics: Maximum allowed volume of 4.2% • Patients were well matched at baseline. sodium bicarbonate • 57% were medical and 43% surgical. 1000 ml in first 24 hr after inclusion • primary diagnosis: • sepsis (53%) • hemorrhagic shock (22%) • cardiac arrest (9%) • Mechanically ventilated (83%) • Vasopressors (80%) • Baseline serum bicarbonate levels were identical, with a median of 13 mEq/L and interquartile range 4.2% sodium bicarbonate: of 10-15 mEq/L. Osmolarity is 1000 mosm. Bicarbonate 0.5 meq/mL.
Sodium bicarbonate therapy for patients with severe metabolic acidemia in the intensive care unit (BICAR-ICU): a multicenter, open-label, randomized controlled, phase 3 trial Primary outcome: A composite of all-cause mortality at day 28 or the presence of ≥1 organ failure at day 7: • Entire cohort • In patients with AKIN scores of 2-3 (pre-specified subgroup) Secondary Outcomes: Maximum allowed • The use, duration and the number of days alive volume of 4.2% free from specific life saving interventions (RRT, sodium bicarbonate 1000 ml in first 24 hr Mechanical ventilation, vasopressors) after inclusion 4.2% sodium bicarbonate: Osmolarity is 1000 mosm. Bicarbonate 0.5 meq/mL.
Sodium bicarbonate therapy for patients with severe metabolic acidemia in the intensive care unit (BICAR-ICU): a multicenter, open-label, randomized controlled, phase 3 trial RCT N=400 Inclusion: pH ≤ 7.20 Blood bicarbonate ≤ 20 mmol/L PaCO2 ≤ 45 mmHg Blood lactate > 2 mmol/L or SOFA score > 4) Bicarbonate arm Control arm Composite endpoint (day-28 mortality and/or 66% 71% p = 0.24 presence of at least one organ failure at day 7) 28 day survival 55% 46% p = 0.09 At least one organ 62% 69% p = 0.15 failure at day 7
Sodium bicarbonate therapy for patients with severe metabolic acidemia in the intensive care unit (BICAR-ICU): a multicenter, open-label, randomized controlled, phase 3 trial RCT N=400 Inclusion: pH ≤ 7.20 Blood bicarbonate ≤ 20 mmol/L PaCO2 ≤ 45 mmHg Blood lactate > 2 mmol/L or SOFA score > 4) Bicarbonate arm Control arm Use of renal replacement p= 0·0009 35% 52% therapy during ICU stay Time from enrolment to 19 (7–82) 7 (3–18) p
Sodium bicarbonate therapy for patients with severe metabolic acidemia in the intensive care unit (BICAR-ICU): a multicenter, open-label, randomized controlled, phase 3 trial AKI stratum Inclusion: pH ≤ 7.20 Blood bicarbonate ≤ 20 mmol/L PaCO2 ≤ 45 mmHg n=92 n=90 Blood lactate > 2 mmol/L or SOFA score > 4) Among AKIN 2 or 3 Bicarbonate arm Control arm Composite endpoint (day-28 mortality and/or 70% 82% p = 0.04 presence of at least one organ failure at day 7) 28 day survival 63% 46% p = 0.02 At least one organ failure at day 7 66% 82% p = 0.01
AKI stratum Inclusion: pH ≤ 7.20 Blood bicarbonate ≤ 20 mmol/L PaCO2 ≤ 45 mmHg n=92 n=90 Blood lactate > 2 mmol/L or SOFA score > 4) Bicarbonate arm Control arm Among AKIN 2 or 3 Use of renal replacement 47/92 (51%) 66/90 (73%) p=0·0020 therapy during ICU stay Time from enrollment to 20 (8–82) 7 (3–17) p
In the setting of AKI, when should RRT be used in severe metabolic acidosis? AKI Initiate RRT Ø No RCTs with mortality as endpoint Ø pH ≤ 7.15 Ø Recommendation are based on Ø No respiratory acidosis retrospective studies/case reports Ø Cut off 7.15 used in RCTs comparing early versus late RRT pH as a criteria for RRT Elaine AKIKI IDEAL ICU pH Not used ≤ 7.15 ≤ 7.15
In the setting of septic shock with lactic acidosis would CRRT cause meaningful changes in serum lactate levels?
Acute Bicarbonate Administration in Lactic Acidosis Daily production of lactic acid • 1,000 -2000 mmol/day Gluconeogenesis Lactate • 15–20 mmol/kg BW NADH/NAD+ Lactate Dehydrogenase Glucose Pyruvate Pyruvate Dehydrogenase Glycolysis Tissues with high rate of glycolysis: Acetate Skeletal muscle, gut, brain, skin, Coenzyme A and red blood cells Acetyl-CoA Oxaloacetate Citrate synthase blood lactate levels are maintained less than 1 mM. H+ Citrate Citric Acid Cycle CO2 H2O
Under Normal Conditions What is the magnitude of
small solute clearance
during hemodialysis and
&'(')*+,-( )*+' (00-1/0,()
CRRT ?
= 4-56 71'*)(*7' (8/0,()
?.@ 00-1/0,(
1 .5 / = 4-56 71'*)(*7' (8/0,()
=1
= 1000 ml/min
Lactate clearance with hemodialysis and CRRT (ml/min) and how does it compare to body lactate clearance ? = 1 / CRRT clearance is ~20-40 ml/min for Hemodialysis clearance is 250 ml/min body weight of 50 to 100 kg Hemodialysis clearance 25% of body clearance CRRT clearance 2-4% of body clearance
Under Conditions of High Generation (i.e. Septic Shock)
&'(')*+,-( )*+' (00-1/0,()
= 4-56 71'*)*(7' (8/0,()
CRRT High
?.@ 00-1/0,( ×15 Clearance
= 4-56 71'*)*(7' (6L/hr)
8/0,(
QR 00-1/0,(
23 / = S
?
TUV
QR 00-1/0,(
= S
? WXYYZ 1*7+*+' 71'*)*(7'
TUV
QR 00-1/0,(
= ? 8/0,( = 21 /
W[.? 8/0,(Should minute ventilation be increased in mechanically ventilated patients with metabolic acidosis? Management of Metabolic Acidosis in Mechanically Ventilated patients ? • No specific data Treat metabolic acidosis and its • Increase RR ≤35, TV≤ 8 ml/kg cause • Goals: • pH >7.15 • Avoid intrinsic PEEP, high plateau pressures
What is the role of bicarbonate in respiratory acidosis? What is aa safe What is safepH pHrange rangeinin What What isis aa safe safepCO2 pCO2range range in respiratory acidosis? respiratory acidosis? respiratory in respiratoryacidosis? acidosis? Are there scenarios where bicarbonate therapy could be detrimental?
What is a safe pH range in respiratory acidosis? pH management from the protocol of the ARDSnet trial of low tidal ventilation • Optimal pH? • No well-defined pH cutoff below which Arterial pH GOAL: 7.30 – 7.45 patients obviously deteriorate A. Acidosis Management: • Balancing the potential harm from more • If pH 7.15 – 7.30: aggressive mechanical ventilation Ø Increase set RR until pH > 7.30 or PaC02 versus the potential harm from acidemia < 25 (Maximum Set RR = 35) Ø If set RR = 35 and pH < 7.30, NaHC03 • What is a reasonable target pH for most may be given (not required) patients? • No high-quality data. • If pH < 7.15: • Modern study protocols pH >7.2 (seems Ø Increase set RR to 35. to be a largely arbitrary choice). Ø If set RR = 35 and pH 7.15 and NaHC03 has been considered or infused, tidal volume may be increased in 1 ml/kg PBW steps until pH > 7.15 (Pplat target may be exceeded).
What is a desirable pCO2 level in respiratory acidosis? • There is no reliable data regarding what the optimal pCO2 level is • Difficult to distinguish clinical consequences of hypercapnia from those of respiratory acidemia • Elevated pCO2 levels are generally well tolerated: • Severe COPD • Obesity hypoventilation Syndrome • Elevated pCO2: • Increase intracranial pressure • Pulmonary vascular resistance • TAME RCT is currently underway to evaluate whether mild hypercapnia (PaCO2 50-55mm) may be beneficial following cardiac arrest.
Permissive hypercapnia: Is there any upper limit? • Case reports of patients with extreme respiratory acidosis who Timeline pH pC02 PO2 survived Presentation 7.01 100 38 Protective TV 150 to 180 ml, RR 35 ventilation 24 hours 6.96 219 54 36 hours 6.88 230 68 12 h of sodium bicarbonate infusion at 36 hours the rate of 50 mL/h 48 hours 7.09 373 62 48 hours TV increased to 230 from 180 53 hours 7.29 141 92 Indian J Crit Care Med. 2014 Sep;18(9):612-4.
What is a safe pH range in respiratory acidosis? • Case reports of patients with extreme respiratory acidosis who survived Indian J Crit Care Med. 2014 Sep;18(9):612-4.
Toxic Core clinical Core laboratory General principles of Indications for RRT alcohol features features treatment Methanol CNS depression AGMA Supportive care pH < 7.3 Seizures High osmolal gap Fomepizole Methanol level > 50 mg/dL Retinal toxicity Elevated lactic acid (formic Ethanol (if fomepizole is End organ damage Hemodynamic acid mediated inhibition of unavailable) Hemodynamic instability instability mitochondrial electron Folic acid or folinic acid and progression despite transport chain) appropriate care Ethylene CNS depression AGMA Supportive care pH < 7.3 glycol Seizures High osmolal gap Fomepizole Ethylene glycol > 50 mg/dL? AKI Falsely elevated lactic acid Ethanol (if fomepizole is End organ damage Calcium oxaluria (glycolic acid can be unavailable) Hemodynamic instability Hemodynamic mistaken for lactic acid) Thiamine and progression despite instability Pyridoxine appropriate care Calcium oxalate crystals in urine Roberts et al; Crit Care Med. 2015; Feb;43(2):461-72.
Increasing pH immediately decreases effective toxicity Core laboratory features ^ • Respiratory alkalosis • AGMA: Ketoacid OH OH salicylic acid lactic acid H + + Treatment: • Induce alkalemia Salicylic acid • ± Dialysis Salicylate Lower pH favors non ionized form: Higher pH favors ionized form: • It diffuses into tissues (more toxic) • Less tissue penetration (less toxic): • Cannot be concentrated in urine (it will • trapped and excreted in the urine. diffuse out of tubules)
General Principles of Treatment that Pertain to Salicylate Poisoning Avoid or delay intubation if possible. Indication for RRT If performed: EXTRIP (Extra Corporeal Treatment in Poisoning • Intubation rapidly Workgroup) Recommendations • After intubation, adjust settings to (1) Altered mental status or noncardiogenic pulmonary maximize minute ventilation (e.g. TV 8-10 edema cc/kg, RR as high as possible without (2) Noncardiogenic pulmonary edema requiring causing autoPEEP). supplemental oxygen (3) Salicylate level >100 mg/dL (7.2 mM) >90 mg/dL (6.5 mM) with renal dysfunction >90 mg/dL (6.5 mM) despite supportive care (e.g. fluid resuscitation) Alkalization: > 80 mg/dL (5.8 mM) despite supportive care and in Indications: context of renal dysfunction • level >40 mg/dL (>2.9 mM) (4) pH < 7.2 despite supportive care (e.g. bicarbonate) • All symptomatic patients (5) Volume overload which prevents adequate Target pH ~7.5-7.55. alkalization is a potential indication for dialysis Target urine pH of at least 7.5 https://www.annemergmed.com/article/S0196-0644(15)00285-1/pdf
THANK YOU Questions? Email: lenar@med.umich.edu
You can also read

















































