A simple additive staging system for newly diagnosed multiple myeloma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Blood Cancer Journal www.nature.com/bcj
ARTICLE OPEN
A simple additive staging system for newly diagnosed multiple
myeloma
Nadine H. Abdallah 1, Moritz Binder 1, S. Vincent Rajkumar 1, Patricia T. Greipp2, Prashant Kapoor 1, Angela Dispenzieri 1,
Morie A. Gertz1, Linda B. Baughn 2, Martha Q. Lacy1, Suzanne R. Hayman1, Francis K. Buadi 1, David Dingli 1, Ronald S. Go 1,
Yi L. Hwa1, Amie L. Fonder1, Miriam A. Hobbs1, Yi Lin 1, Nelson Leung1,3, Taxiarchis Kourelis 1, Rahma Warsame1,
✉
Mustaqeem A. Siddiqui 1, Robert A. Kyle1, P. Leif Bergsagel 4, Rafael Fonseca 4, Rhett P. Ketterling1 and Shaji K. Kumar 1
© The Author(s) 2022
Risk stratification in multiple myeloma is important for prognostication, patient selection for clinical trials, and comparison of
treatment approaches. We developed and validated a staging system that incorporates additional FISH abnormalities not included
in the R-ISS and reflects the additive effects of co-occurring high-risk disease features. We first evaluated the prognostic value of
predefined cytogenetic and laboratory abnormalities in 2556 Mayo Clinic patients diagnosed between February 2004 and June
2019. We then used data from 1327 patients to develop a risk stratification model and validated this in 502 patients enrolled in the
MMRF CoMMpass study. On multivariate analysis, high-risk IgH translocations [risk ratio (RR): 1.7], 1q gain/amplification (RR: 1.4),
1234567890();,:
chromosome17 abnormalities (RR: 1.6), ISS III (RR: 1.7), and elevated LDH (RR: 1.3) were independently associated with decreased
overall survival (OS). Among 1327 evaluable patients, OS was 11.0 (95% CI: 9.2–12.6), 7.0 (95% CI: 6.3–9.2), and 4.5 (95% CI: 3.7–5.2)
years in patients with 0 (stage I), 1 (stage II), and ≥2 (stage III) high-risk factors, respectively. In the MMRF cohort, median OS was 7.8
(95% CI: NR-NR), 6.0 (95% CI: 5.7-NR), and 4.3 (95% CI: 2.7-NR) years in the 3 groups, respectively (P < 0.001). This 5-factor, 3-tier
system is easy to implement in practice and improves upon the current R-ISS.
Blood Cancer Journal (2022)12:21 ; https://doi.org/10.1038/s41408-022-00611-x
INTRODUCTION high-risk markers [11]. The R-ISS has subsequently been validated in
Multiple myeloma (MM) is the second most common hematologic several studies [12, 13] and is currently used to risk-stratify patients
malignancy and is responsible for approximately 2% of all cancer with newly diagnosed MM [11]. It is thought to perform better than
deaths in the United States [1]. With the advent of novel its predecessor in certain patient populations [8, 12, 13]. Recent
therapeutic agents and drug combinations, survival outcomes have studies have identified additional cytogenetic abnormalities not
improved considerably [2]. Despite these therapeutic advances, included in the R-ISS to be associated with adverse survival
survival outcomes remain highly variable even in uniformly treated outcomes including monosomy 13 [14, 15], gain/amplification of
clinical trial populations [3, 4]. This disparity highlights the 1q21 [16, 17], and rearrangements involving the MYC gene [18–20].
importance of risk stratification at the time of diagnosis for Even though more powerful high-risk classifiers have been
prognostication and patient selection for clinical trials [5, 6]. Several developed based on gene expression profiles and cytogenetics,
risk stratification systems have been proposed based on clinical their acceptance in clinical practice remains poor due to the
characteristics, laboratory studies, bone marrow cytogenetics, and involved resources and need for complex modeling [21–25]. While
gene expression profiling. Among them, the International Staging the presence of high-risk laboratory and cytogenetic features has
System (ISS) and its successor, the revised ISS (R-ISS), have stood the been incorporated into the R-ISS, the additive effects of multiple co-
test of time in clinical practice. The ISS was first introduced in 2005 occurring high-risk disease features have not been accounted for
and is based on β2-microglobulin and albumin, which are thought [15, 16]. Importantly, as RISS was developed, assessment of 1q
to reflect tumor burden and host status [7]. In clinical practice, the abnormalities was not commonly employed and there was limited
ISS remains a popular choice for risk stratification due to its data to explore the value of adding this variable. Furthermore,
simplicity, although its ability to discriminate among lower-risk unlike the ISS which had a similar proportion of patients in each of
patients is limited in the era of novel therapies [8]. Interphase the three stages, R-ISS resulted in majority of patients being
fluorescence in-situ hybridization (FISH) enabled the identification classified as intermediate. In light of the identification of additional
of high-risk disease independent of ISS stage based on abnorm- cytogenetic risk factors and an improved understanding of the
alities such as t(4;14), t(14;16), and del(17p) [9, 10]. The revised ISS prognostic implications of multi-hit disease, we conducted this
(R-ISS) was introduced in 2015 and includes these cytogenetic study to evaluate a new simple additive staging system in patients
abnormalities as well as elevated lactate dehydrogenase (LDH) as with newly diagnosed MM [14, 17, 19, 20].
1
Division of Hematology, Mayo Clinic, Rochester, MN, USA. 2Department of Laboratory Medicine and Pathology, Rochester, MN, USA. 3Division of Nephrology and Hypertension,
Mayo Clinic, Rochester, MN, USA. 4Division of Hematology, Mayo Clinic, Phoenix, AZ, USA. ✉email: kumar.shaji@mayo.edu
Received: 12 August 2021 Revised: 7 December 2021 Accepted: 12 January 2022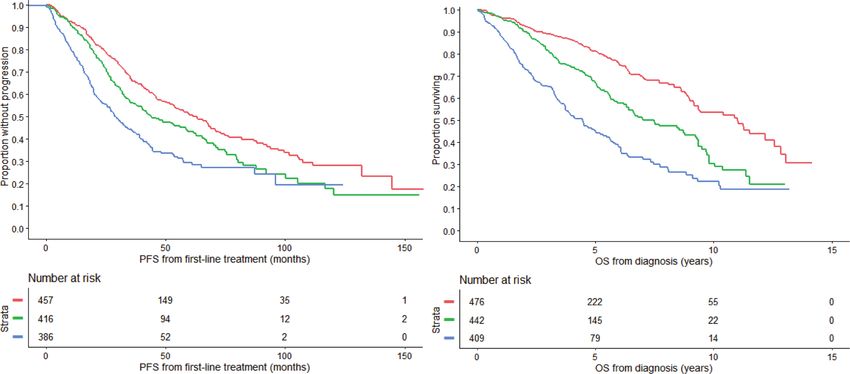
N.H. Abdallah et al.
2
PATIENTS AND METHODS multivariate model were then included in a final multivariate model with
Patients and study design ISS stage III (vs I/II) and elevated LDH. Values above the upper limit of normal
We included all patients with MM seen in Mayo Clinic in Rochester, of the reporting laboratory were considered elevated for lactate dehydro-
Minnesota between 2004 and 2019, who had cytogenetic analysis by FISH genase (above 222 U/l for the Mayo Clinic Laboratories). ISS stages were
performed within 1 year before diagnosis, or within 6 months from the defined as: β2-microglobulin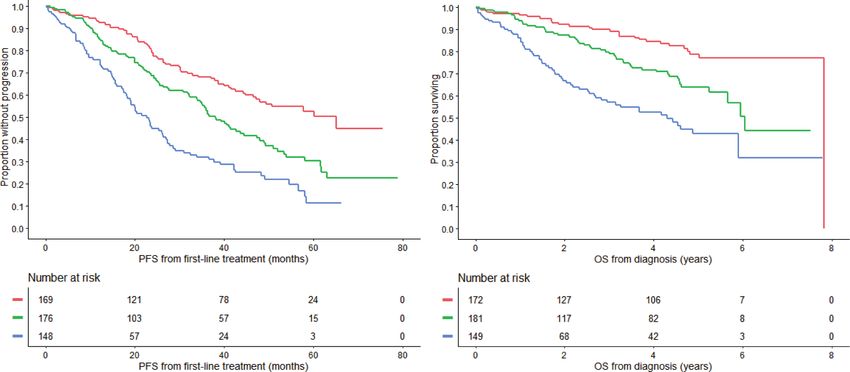
N.H. Abdallah et al.
3
Table 1. Baseline characteristics. Table 2. Cytogenetic abnormalities in multiple myeloma patients.
Baseline characteristics Median N (%) Primary abnormalities Tested N Abnormality N (%)
(interquartile range) IgH translocations
Age (years) 64 (57–71) t(4;14) 2519 248 (10)
Male 1582 (62) t(14;16) 2517 99 (4)
ECOG PS ≥ 2 (vs 0–1) 141 (20) t(11;14) 2522 519 (21)
Hemoglobin (g/dL) 11.0 (9.5–12.5) Trisomies 2491 1374 (55)
Hemoglobin ≤ 10 g/dL 720 (33) Secondary abnormalities
Platelets (×109/L) 210 (162–262) 1q gain/amplification 1896 585 (31)
Creatinine (mg/dL) 1.1 (0.9–1.5) Chromosome 17 abnormality 2499 337 (13)
Creatinine ≥ 2 mg/dL 319 (16) (17pdel/monosomy 17)
LDH > ULN (units/L) 298 (17) Monosomy 13 2513 926 (37)
B2M (µg/ml) 4.0 (2.7–6.6) MYC rearrangement 1856 160 (9)
B2M > 5.5 vs. (≤5.5) 701 (32) Prevalence of recurrent primary and secondary cytogenetic abnormalities
in patients tested by FISH at diagnosis.
Albumin (g/dL) 3.6 (3.2–3.9)
IgH immunoglobulin heavy chain gene locus, del deletion.
Albumin ≤ 3.5 (vs. >3.5) 928 (48)
Calcium (mg/dL) 9.5 (9.0–10.1)
P < 0.001), chromosome 17 abnormalities (RR: 1.6, P < 0.001), ISS III
Calcium ≥ 11 mg/dL 215 (11)
(RR: 1.7, P < 0.001), and elevated LDH (RR: 1.3, P = 0.01) were all
Serum M spike (g/dL) 2.5 (0.7–3.9) independently associated with decreased OS in the final multi-
Urine M spike (g/24 h) 0.05 (0–0.50) variate model. MYC rearrangements were associated with
Urine albumin (g/24 h) 0.05 (0.02–0.14) decreased survival, but this was not statistically significant (RR:
1.3, P = 0.06). These results are presented in Table 3.
IgA MM 464 (25)
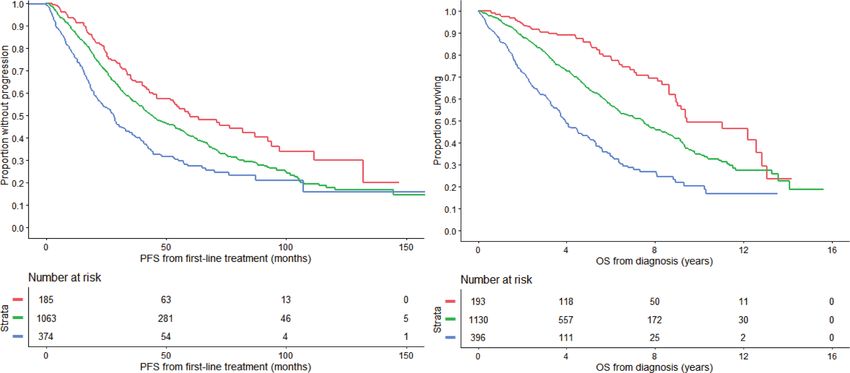
IgG MM 1177 (62) PFS and OS based on the updated R-ISS
LC MM 214 (11) The R-ISS was updated to include 1q gain/amplification in the
Involved LC definition of high-risk cytogenetic abnormalities, in addition to
high-risk IgH translocations and chromosome 17 abnormalities.
Kappa 1252 (65)
Based on this definition, 193 (11%), 1130 (66%), and 396 (23%)
Lambda 674 (35) patients had stage I, II, and III disease, respectively. The median
ISS Stage III (vs. I&II) 710 (33) PFS was 60.0 (95% CI: 46.1–87.1), 44.0 (95% CI: 40.5–48.8), and 28.1
BMPCs (%) 50 (30–70) (95% CI: 23.0–31.4) months in the 3 groups, respectively (P < 0.001)
(Fig. 1a). Median OS was 9.4 (95% CI: 8.9–12.8), 7.5 (95% CI:
PCLI (%) 0.8 (0.3–1.5)
6.4–8.0), and 3.9 (95% CI: 3.6–4.6) years in patients with stage I, II,
First-line treatment and III disease, respectively (P < 0.001) (Fig. 1b).
PI 727 (31)
IMiD 720 (31) Developing a simpler approach for risk stratification – The
MASS
PI + IMiD 804 (34)
Among all patients included in the study, 1327 had simultaneous
Other 107 (5) data available for: high-risk IgH translocations, 1q gain/amplifica-
Transplant 1399 (55) tion, chromosome 17 abnormalities, ISS stage, and LDH. There
Early (≤1 year from 1184 (85) were no significant differences in baseline characteristics
diagnosis) between evaluable patients and the rest of the cohort (Supple-
Late (>1 year from 215 (15) mental Table 1). Among evaluable patients, 476 (36%) had no
diagnosis) high-risk factors (stage I), 442 (33%) had 1 high-risk factor (stage
Clinical and laboratory characteristics at diagnosis of patients diagnosed
II), and 409 (31%) had ≥2 high-risk factors (stage III). Median PFS
with multiple myeloma included in the study. The median (range) are was 63.1 (95% CI: 53.0–70.8), 44.0 (95% CI: 37.8–58.7), and 28.6
presented for continuous variables and number (percentage) for catego- (95% CI: 25.4–34.7) months in the 3 groups, respectively (Fig. 2a).
rical variables. OS was 11.0 (95% CI: 9.2–12.6), 7.0 (95% CI: 6.3–9.2), and 4.5 (95%
B2M beta2microglobulin, BMPCs bone marrow plasma cells, IMiD immuno- CI: 3.7–5.2) years in patients with stage I, II, and III disease,
modulatory drug, ISS international staging system, LC light chain, LDH respectively (Fig. 2b) (Table 4).
lactate dehydrogenase, MM multiple myeloma, PCLI plasma cell labeling
index, PI proteasome inhibitor, PS performance status, ULN upper limit of Subgroup analysis by age and transplant status
normal. The prognostic ability of this staging system was evaluated based
on age group and transplant status. Among patients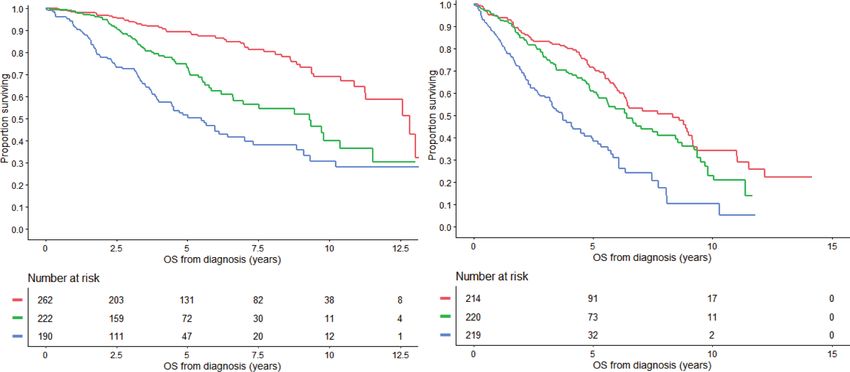
N.H. Abdallah et al.
4
Table 3. Univariate and multivariate survival models.
Variable Univariate Multivariate (FISH Multivariate (all)
abnormalities only)
OS RR (95% CI) P value OS RR (95% CI) P value OS RR (95% CI) P value
HR IgH translocations 2.0 (1.7–2.3)
N.H. Abdallah et al.
5
a) b)
PN.H. Abdallah et al.
6
a) b)
PN.H. Abdallah et al.
7
193 193
51
250 250
114
30
373 156
81
168 154
234 291
25% 39% 35%
17% 66% 17%
36% 33% 31%
Fig. 5 Stage migration between R-ISS and MASS and ISS and MASS. The distribution and migration of patients between disease stages
using ISS, R-ISS, and MASS risk stratification systems. ISS International Staging System, R-ISS Revised International Staging System, MASS Mayo
Additive Staging System.
a) b)
P=0.003
PN.H. Abdallah et al.
8
have prevailed in clinical practice and research alike due to their CONCLUSION
simplicity and reliance on readily available baseline characteristics In summary, we developed and validated a simple, additive
[7, 11]. The recognition of additional risk factors motivated the 5-factor 3-tier risk model for newly diagnosed MM in two diverse
revision of the ISS and resulted in a more powerful predictive patient populations that is easy to implement in clinical practice
model [11]. Since the introduction of the R-ISS, data on additional and can play an important role in patient selection for clinical
risk factors including chromosome 13 abnormalities, 1q gains, and trials.
MYC rearrangements have come to light [15–17, 20]. Furthermore,
it has become evident that the co-occurrence of multiple high-risk
disease features compounds the risk for adverse outcomes, REFERENCES
leading to the concept of double- and triple-hit myeloma 1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin.
[15, 16]. This insight led us to propose a refined additive risk 2020;70:7–30.
stratification system. 2. Kumar SK, Dispenzieri A, Lacy MQ, Gertz MA, Buadi FK, Pandey S, et al. Continued
improvement in survival in multiple myeloma: changes in early mortality and
We first evaluated the prognostic impact of known cytogenetic
outcomes in older patients. Leukemia 2014;28:1122–8.
abnormalities in MM. In addition to the high-risk abnormalities 3. Durie BGM, Hoering A, Sexton R, Abidi MH, Epstein J, Rajkumar SV, et al. Longer
included in the R-ISS, 1q gain demonstrated independent term follow-up of the randomized phase III trial SWOG S0777: bortezomib,
prognostic value in our final multivariate model, while the lenalidomide and dexamethasone vs. lenalidomide and dexamethasone in
prognostic impact of MYC rearrangements did not reach statistical patients (Pts) with previously untreated multiple myeloma without an intent for
significance. Trisomies and monosomy 13 were not independently immediate autologous stem cell transplant (ASCT). Blood Cancer J. 2020;10:53.
associated with OS when adjusting for other cytogenetic 4. Srivastava G, Rana V, Lacy MQ, Buadi FK, Hayman SR, Dispenzieri A, et al. Long-
abnormalities, and thus the poor prognostic impact of non- term outcome with lenalidomide and dexamethasone therapy for newly diag-
hyperdiploidy [33] and chromosome 13 abnormalities [34–36] nosed multiple myeloma. Leukemia 2013;27:2062–6.
5. Chng WJ, Dispenzieri A, Chim CS, Fonseca R, Goldschmidt H, Lentzsch S, et al.
may be due to their association with other HR cytogenetic
IMWG consensus on risk stratification in multiple myeloma. Leukemia
abnormalities. When we used an updated version of the R-ISS, 2014;28:269–77.
where 1q gain/amplification was included in the definition of 6. Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, Dispenzieri A, et al. Review of
high-risk disease, we discriminated 3 groups of patients with 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc.
significantly different outcomes. However, as with the original R- 2003;78:21–33.
ISS, most patients had intermediate risk disease (stage II) using this 7. Greipp PR, San Miguel J, Durie BG, Crowley JJ, Barlogie B, Blade J, et al. Inter-
classification (66%). In addition, the R-ISS as originally designed national staging system for multiple myeloma. J Clin Oncol. 2005;23:3412–20.
did not consider the compounding effects of co-occurring high- 8. Cho H, Yoon DH, Lee JB, Kim SY, Moon JH, Do YR, et al. Comprehensive evaluation
risk disease features. Thus, we proposed a system that stratifies of the revised international staging system in multiple myeloma patients treated
with novel agents as a primary therapy. Am J Hematol. 2017;92:1280–6.
patients based on the number of high-risk factors present at
9. Fonseca R, Bergsagel PL, Drach J, Shaughnessy J, Gutierrez N, Stewart AK, et al.
diagnosis: HR IgH translocations, 1q gain/amplification, chromo- International Myeloma Working Group molecular classification of multiple mye-
some 17 abnormalities, ISS III, and/or elevated LDH. Using this loma: spotlight review. Leukemia 2009;23:2210–21.
system, we discriminated 3 groups of patients with significantly 10. Avet-Loiseau H, Durie BG, Cavo M, Attal M, Gutierrez N, Haessler J, et al. Com-
different progression-free and overall survival with nearly a third bining fluorescent in situ hybridization data with ISS staging improves risk
of the patients distributed between the 3 stages. assessment in myeloma: an International Myeloma Working Group collaborative
The prognostic utility of this system was demonstrated in both project. Leukemia 2013;27:711–7.
age groups: ≥65 years andN.H. Abdallah et al.
9
20. Abdallah N, Baughn LB, Rajkumar SV, Kapoor P, Gertz MA, Dispenzieri A, et al. Research Foundation Personalized Medicine Initiatives (https://research.themmrf.org
Implications of MYC rearrangements in newly diagnosed multiple myeloma. Clin and www.themmrf.org).
Cancer Res. 2020;26:6581–8.
21. Kuiper R, Broyl A, de Knegt Y, van Vliet MH, van Beers EH, van der Holt B, et al. A
gene expression signature for high-risk multiple myeloma. Leukemia AUTHOR CONTRIBUTIONS
2012;26:2406–13. NA and SKK designed the study, collected, and analyzed the data, and wrote the first
22. Kuiper R, van Duin M, van Vliet MH, Broijl A, van der Holt B, El Jarari L, et al. draft of the manuscript. MB contributed to data analysis, provided critical revision
Prediction of high- and low-risk multiple myeloma based on gene expression and and final approval of the manuscript version for publication. SVR, PTG, PK, AD, MAG,
the international staging system. Blood. 2015;126:1996–2004. LBB, MQL, SRH, FKB, DD, RSG, YLH, ALF, MAH, YL, NL, TK, RW, MAS, RAK, PLB, RF, RPK
23. Mason MJ, Schinke C, Eng CLP, Towfic F, Gruber F, Dervan A, et al. Multiple provided critical revision and final approval of the manuscript version for publication.
myeloma DREAM challenge reveals epigenetic regulator PHF19 as marker of
aggressive disease. Leukemia 2020;34:1866–74.
24. Perrot A, Lauwers-Cances V, Tournay E, Hulin C, Chretien ML, Royer B, et al.
Development and validation of a cytogenetic prognostic index predicting sur- COMPETING INTERESTS
vival in multiple myeloma. J Clin Oncol. 2019;37:1657–65. PK received research funding from Takeda Pharmaceuticals, Celgene, and Amgen. AD
25. Shaughnessy JD Jr, Zhan F, Burington BE, Huang Y, Colla S, Hanamura I, et al. A received research funding from Celgene, Millennium Pharmaceuticals, Pfizer, and
validated gene expression model of high-risk multiple myeloma is defined by Janssen and received a travel grant from Pfizer. MAG served as a consultant for
deregulated expression of genes mapping to chromosome 1. Blood Millennium Pharmaceuticals and received honoraria from Celgene, Millennium
2007;109:2276–84. Pharmaceuticals, Onyx Pharmaceuticals, Novartis, GlaxoSmithKline, Prothena, Ionis
26. Fonseca R, Blood E, Rue M, Harrington D, Oken MM, Kyle RA, et al. Clinical and Pharmaceuticals, and Amgen. MQL received research funding from Celgene. NL
biologic implications of recurrent genomic aberrations in myeloma. Blood serves on an advisory board for Takeda Pharmaceuticals. RF served as a consultant for
2003;101:4569–75. Amgen, BMS, Celgene, Takeda, Bayer, Janssen, Novartis, Pharmacyclics, Sanofi,
27. Goldsmith SR, Fiala MA, Dukeman J, Ghobadi A, Stockerl-Goldstein K, Schroeder Karyopharm, Merck, Juno, Kite, Aduro, OncoTracker, Oncopeptides, GSK, and AbbVie,
MA, et al. Next generation sequencing-based validation of the revised interna- and is on the scientific Advisory Board for Adaptive Biotechnologies, Caris Life
tional staging system for multiple myeloma: an analysis of the MMRF CoMMpass Sciences and OncoTracker. SKK served as a consultant for Celgene, Millennium
study. Clin Lymphoma Myeloma Leuk. 2019;19:285–9. Pharmaceuticals, Onyx Pharmaceuticals, Janssen, and Bristol-Myers Squibb and
28. Miller C, Yesil J, Derome M, Donnelly A, Marrian J, McBride K, et al. A comparison received research funding from Celgene, Millennium Pharmaceuticals, Novartis, Onyx
of clinical FISH and sequencing based FISH estimates in multiple myeloma: an Pharmaceuticals, AbbVie, Janssen, and Bristol-Myers Squibb. The remaining authors
Mmrf CoMMpass analysis. Blood 2016;128:374. declare no competing financial interests.
29. Harrell FE Jr, Lee KL, Califf RM, Pryor DB, Rosati RA. Regression modelling stra-
tegies for improved prognostic prediction. Stat Med. 1984;3:143–52.
30. Newson RB. Comparing the predictive powers of survival models using Harrell’s C ADDITIONAL INFORMATION
or Somers’ D. Stata J. 2010;10:339–58. Supplementary information The online version contains supplementary material
31. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J available at https://doi.org/10.1038/s41408-022-00611-x.
Am Stat Assoc. 1958;53:457–81.
32. Munshi NC, Avet-Loiseau H, Anderson KC, Neri P, Paiva B, Samur M, et al. A large Correspondence and requests for materials should be addressed to Shaji K. Kumar.
meta-analysis establishes the role of MRD negativity in long-term survival out-
comes in patients with multiple myeloma. Blood Adv. 2020;4:5988–99. Reprints and permission information is available at http://www.nature.com/
33. Smadja NV, Bastard C, Brigaudeau C, Leroux D, Fruchart C, Groupe Francais de reprints
Cytogenetique H. Hypodiploidy is a major prognostic factor in multiple myeloma.
Blood 2001;98:2229–38. Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims
34. Fonseca R, Oken MM, Greipp PR, Eastern Cooperative Oncology Group Myeloma in published maps and institutional affiliations.
G. The t(4;14)(p16.3;q32) is strongly associated with chromosome 13 abnormal-
ities in both multiple myeloma and monoclonal gammopathy of undetermined
significance. Blood 2001;98:1271–2.
35. Chiecchio L, Protheroe RK, Ibrahim AH, Cheung KL, Rudduck C, Dagrada GP, et al.
Deletion of chromosome 13 detected by conventional cytogenetics is a critical Open Access This article is licensed under a Creative Commons
prognostic factor in myeloma. Leukemia 2006;20:1610–7. Attribution 4.0 International License, which permits use, sharing,
36. Chng WJ, Santana-Davila R, Van Wier SA, Ahmann GJ, Jalal SM, Bergsagel PL, et al. adaptation, distribution and reproduction in any medium or format, as long as you give
Prognostic factors for hyperdiploid-myeloma: effects of chromosome 13 dele- appropriate credit to the original author(s) and the source, provide a link to the Creative
tions and IgH translocations. Leukemia 2006;20:807–13. Commons license, and indicate if changes were made. The images or other third party
37. Hebraud B, Leleu X, Lauwers-Cances V, Roussel M, Caillot D, Marit G, et al. material in this article are included in the article’s Creative Commons license, unless
Deletion of the 1p32 region is a major independent prognostic factor in young indicated otherwise in a credit line to the material. If material is not included in the
patients with myeloma: the IFM experience on 1195 patients. Leukemia article’s Creative Commons license and your intended use is not permitted by statutory
2014;28:675–9. regulation or exceeds the permitted use, you will need to obtain permission directly
from the copyright holder. To view a copy of this license, visit http://creativecommons.
org/licenses/by/4.0/.
ACKNOWLEDGEMENTS
The MMRF kindly provided the data from the CoMMpass study for the purpose of
© The Author(s) 2022
scientific research. These data were generated as part of the Multiple Myeloma
Blood Cancer Journal (2022)12:21You can also read

















































