A Prospective, Postmarket, Compassionate Clinical Evaluation of a Novel Acellular Fish-skin Graft Which Contains Omega-3 Fatty Acids for the ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ORIGINAL RESEARCH
A Prospective, Postmarket,
Compassionate Clinical Evaluation
of a Novel Acellular Fish-skin Graft
Which Contains Omega-3 Fatty Acids
for the Closure of Hard-to-heal Lower
Extremity Chronic Ulcers
Chun K.Yang, MD; Thais O. Polanco, MD; and John C. Lantis II,
MD, FACS
Wounds 2016;28(4):112-118
Abstract: Introduction. A novel piscine acellular fish-skin graft prod-
uct has 510k clearance on the US market. This product (Omega3,
From the Mount Sinai St. Luke’s Kerecis, Isafjordur, Iceland) is to be used similarly to extracellular
Hospital and Mount Sinai Roosevelt, matrices (ECMs) on the market (eg, bovine and porcine) except that
New York, NY it contains fats, including omega-3 polyunsaturated fatty acids that
have been associated with anti-inflammatory properties in many
Address correspondence to: studies. While many current ECMs are effective on open wounds,
John C. Lantis II, MD, FACS studies have largely excluded application to hard-to-heal ulcers. To
Mount Sinai St. Luke’s Hospital and test this product in a real-world environment, the authors chose to
Mount Sinai Roosevelt look specifically at hard-to-heal ulcers based on previously defined
New York, NY wound and patient factors. Methods. The primary objective was to
assess the percentage of wound closure area from baseline after
JLantis@chpnet.org
5 weekly fish-skin graft applications in 18 patients with at least 1
“hard-to-heal” criteria. Patients underwent application of the fish
Disclosure: The research product skin for 5 sequential weeks, followed by 3 weeks of standard of
was supplied free of charge by care. Wound area, skin assessments, and pain were assessed week-
Kerecis (Isafjordur, Iceland). ly. Results. A 40% decrease in wound surface area (P < 0.05) and a
48% decrease in wound depth was seen with 5 weekly applications
of the fish-skin graft and secondary dressing (P < 0.05). Complete
closure was seen in 3 of 18 patients by the end of the study phase.
Conclusion. This fish-skin product appears to provide promise as an
effective wound closing adjunctive ECM. This is true when used in
this compassionate setting, where many other products fail. This
study lacks a control arm and an aggressive application schedule,
but the investigators believe it represents real-world practice.
Key words: acellular fish-skin graft, hard-to-heal ulcers
A
cellular fish skin is increasingly being used clinically, as a readily
safe and effective alternative tissue source for wound repair in
chronic nonhealing ulcers of many etiologies.1 Current mamma-
lian acellular dermal matrices (ADM) raise concerns of the potential for
autoimmune response, risk of prion diseases, and potential cultural or
112 WOUNDS® www.woundsresearch.com
Yang et al
religious issues that may prohibit the use of porcine
Keypoints
or bovine products in many countries.1 The fish-skin
•F
ish skin material differs from other biologic ma-
material has at least 2 fundamental differences from terials on the market in 2 key areas: 1) no disease
other biologic materials on the market: 1) no disease transmission risk exists from fish to humans; and
transmission risk exists from fish to humans; and 2) the 2) the product still contains fats, which are re-
product still contains fats, which are removed during moved during processing of mammalian products.
processing of mammalian products. When grafted, the •
An in vitro study comparing fish skin to human
acellular fish skin provides a natural structure to the amnion/chorion-derived products show the fish-
wound bed that contains natural skin elements and skin graft is an ideal platform for a 3-dimensional
bioactive lipids, which not only acts as a scaffold for re- ingrowth of cells.
vascularization and repopulation of the patients’ cells, •
Antimicrobial peptides found in fish skin have
but provides anti-inflammatory and antimicrobial prop- shown to repair wounds and act effectively against
pathogenic bacteria, fungi, viruses, or parasites.
erties as well. An in vitro study comparing fish skin to
a human amnion/chorion-derived product shows the
fish-skin graft is an ideal platform for a 3-dimensional from their harsh aquatic environment. Basic features of
(3D) ingrowth of cells. The fish skin was able to sup- fish and human skin are evolutionary conserved. The
port 3D ingrowth and proliferation of fibroblasts while main differences between human and teleost fish skin
no cell ingrowth was seen in the amnion/chorion are the presence of scales instead of hairs and a lack of
membrane-derived product.2 keratinized layer in the fish skin.3 All scales are removed
In its natural state, fish skin is metabolically active from the acellular fish-skin graft, while it still consists
and serves as a protective barrier for piscine species of 3 basic layers: epidermis, dermis, and hypodermis.
Table 1. Demographics and etiology of study participants.
Patient ID Gender Age (years) Wound Age (months) Initial Wound Size (cm2) Etiology Comorbidities
1 Male 63 126 13.0 V Tobacco
2 Male 59 34 4.2 V, DM HTN, tobacco
3 Male 31 8 1.5 DM Tobacco
4 Male 49 5 14.7 DM HIV, CKD, HTN
5 Male 59 6 1.8 DM HTN
6 Male 65 102 25.5 V CKD, HCV
7 Female 84 54 20.4 V HTN
8 Male 53 23 2.6 DM Tobacco
9 Male 70 42 2.2 V, DM, PAD HTN, tobacco
10 Male 38 38 11.4 DM CKD, DM
11 Male 49 7 6.7 DM, PAD CKD, HTN
12 Female 67 40 4.2 V, DM
13 Female 35 46 8.9 DM CKD, HTN
14 Female 64 13 7.8 DM CKD, HTN
15 Male 63 34 7.0 V HTN, HCV, tobacco
16 Male 62 43 7.8 V HTN, tobacco
17 Male 39 10 1.8 DM CKD, HTN
18 Male 47 3 6.0 DM CKD, HTN, tobacco
V: venous; PAD: peripheral artery disease; HTN: hypertension; DM: diabetes mellitus; HCV: hepatitis C virus; HIV: human immunodeficiency virus;
CKD: chronic kidney disease
Vol. 28, No. 4 April 2016 113
Yang et al
MMP inhibitors activity. There
is also a decreased proliferation
and responsiveness to growth
factor from fibroblasts, thus lead-
ing to impaired migration of
keratinocytes and impaired gap
junctions, which ultimately hin-
der the healing process. Chron-
ic, nonhealing ulcers are more
likely to occur in patients with
underlying disorders, such as
peripheral artery disease, diabe-
tes, and venous insufficiency.8-10
There is no single primary fac-
tor that contributes to impaired
wound healing, but it is well
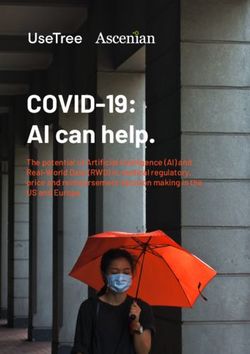
Figure 1. Wound surface area. A 40% decrease in wound surface area was seen in known that chronic wounds
week 5; *P < 0.05,
usually fail to progress through
the stages of wound healing
In the natural state, the epidermal layer consists of an and are arrested in the inflammatory stage. An exces-
outer layer rich in microfilaments and collagen; an in- sive amount of protein mediators, such as proinflam-
termediate layer, with contents such as unicellular mu- matory cytokines, play a prominent role in the mo-
cous secreting glands; and a third anchoring the basal lecular and cellular processes during the inflammatory
epithelial cells layer stage of skin healing and are known to delay wound
Following injury, mucous cells from the intermediate healing.11 Research has shown the effects of bioactive
epithelial layer margins help close wounds by secreting lipid mediators—omega-3 polyunsaturated fatty acids,
lysosomes, immunoglobulin, C-reactive peptides, and eicosapentaenoic acid (EPA) and docosahexaenoic
lymphocytes which are transported to the damaged acid (DHA)—reduce inflammatory responses and the
area.3-5 The fish dermis is a highly vascularized collage- transmigration of proinflammatory cytokines across the
nous matrix composed of fibroblasts, pigment cells, and endothelium.11-13 Omega-3 polyunsaturated fatty acids,
scales. Its primary function is to strengthen and protect EPA, and DHA are found predominately in fish skin, oils,
skin against tensile force. The hypodermis separates plasma, and cellular tissues.1
the inner face of the dermis from the subjacent mus- The fish-skin graft is a decellularized fish skin har-
cle cells, which is composed of loosely organized col- vested from codfish in the North Atlantic. It is a skin
lagen, chromatophores, vasculature, and adipose cells.5 substitute containing collagen, fibrin, proteoglycans, and
Neutral and acidic glycoconjugates and antimicrobial glycosaminoglycans, with the potentially added benefits
peptides (AMP) are secreted and expressed from fish of bioactive lipid mediators. It furnishes a complex scaf-
skin; examples of AMPs include hepcidin, defense-like fold that provides an optimal environment for a favor-
peptides, apolipoproteins, and piscidin. This secretion able host tissue response, a response characterized by
aids in defense against invading pathogens. Antimicro- restoration of tissue structure and function, while deliv-
bial peptides found in fish skin have shown to repair ering anti-inflammatory EPA and DHA type omega-3 fat-
wounds and act effectively against pathogenic bacteria, ty acids. The primary objective of this study is to assess
fungi, viruses, or parasites. 4 the percentage of wound closure for hard-to-heal ulcers.
Acute wounds in healthy individuals heal through
a relatively orderly, linear sequence of physiological Materials and Methods
events that include hemostasis, inflammation, epithe- All patients signed an institutional review board in-
lialization, fibroplasia, and maturation.6,7 In chronic formed consent consistent with the Helsinki Accord
wounds, there is an increase in metalloproteinases for Human Subjects. In this prospective, nonblinded,
(MMP) activity and a decrease of their counteractive noncomparative, postmarket, clinical evaluation of the
114 WOUNDS® www.woundsresearch.com
Yang et al
fish-skin graft, a total of 20 patients were enrolled in
Keypoints
the study but only 18 completed the trial. The patients
•T he 20 subjects in this study had full-thickness
were older than 18 years and recruited from an urban ulcers that were either > 20 cm2 or had been pres-
tertiary wound care program. The subjects had ulcers ent for at least 52 weeks, both factors defined as
that were of full-thickness and had either > 20 cm2 or markers of hard-to-heal wounds.
had been present for at least 52 weeks, both factors de- • Exclusion criteria consisted of patients undergoing
fined as markers of hard-to-heal wounds. If patients had chemotherapy, being treated with immunosuppres-
ulcers in bilateral extremities, the larger ulcer was un- sive drugs or corticosteroids, or were previously
dertaken for treatment enrollment. Study participants evaluated for treatment.
suffered from either a combination of venous insuffi- • Over a 5-week period, 5 weekly applications of the
ciency with an ankle-brachial index (ABI) of 0.7 to 1.3, extracellular matrices and secondary dressings re-
diabetes mellitus with an ABI ≥ 1.3 or a toe pressure sulted in a 40% decrease in wound surface area.
> 40 mm Hg, or peripheral artery disease with an ABI
of 0.5 to 0.7. tions were recorded. Having met the inclusion crite-
Patients had to be willing to use appropriate offload- ria, the study participants were treated with a weekly
ing and suitable compression therapy. Exclusion crite- placement of appropriately sized fish-skin graft, Allevyn
ria consisted of patients undergoing chemotherapy, (Smith & Nephew, Hull, UK) foam, secondary dressing,
being treated with immunosuppressive drugs or cor- and compression for 5 weeks. At each study visit, the
ticosteroids, or had been previously evaluated for the wound was photographed and total surface area of the
treatment. Comorbidities included hypertension, to- reference ulcers (cm2) and the area of nonviable tis-
bacco use, diabetes mellitus type 2, and hepatitis C vi- sue (cm2) were measured using planimetry. The ulcer
rus; most notably, renal failure was not an exclusion cri- and surrounding skin assessments noted were: level of
teria. There was no blinding in this study, as the sample odor (none, slight, moderate, or strong); level of exudate
size was small and the product definitively placed. This (none, slight, moderate, or heavy); condition of the sur-
was an open study with both patients and clinicians rounding skin (healthy, inflamed, macerated, dry and
aware of the products being used. flaky, or other); and any signs of erythema (no reddening,
The fish-skin graft is available in sizes 3 cm x 3.5 cm, pink, or red).Adverse events, changes in medication, and
3 cm x 7 cm, and 7 cm x 10 cm, and it is indicated for assessment of visual pain scale of 1-10 were also docu-
partial-thickness and full-thickness wounds and skin mented. For weeks 6-8, dressings were removed and sec-
loss injuries as well as superficial and second-degree ondary dressings with the foam were placed. The ulcer
burns. The fish-skin graft was moistened with normal and surrounding skin assessments were performed and
saline and applied directly to the wound. It was held photographed, pain assessment and any adverse events
in place with surgical adhesive and surgical strips. A or concomitant medications were recorded. Patients in-
secondary dressing that delivers ongoing moisture or terrupting treatment for more than 7 consecutive days
is moisture retentive was necessary. The fish-skin graft were withdrawn from the study. All adverse events re-
can be reapplied weekly and does not require the re- ported by the patient, or in response to questioning or
moval of the previously applied product since it is observation by the investigator, were recorded and ad-
gradually resorbed and remodeled in the wound. dressed properly.
Statistics. This was a pilot/feasibility study addressing
real-world effectiveness, not an efficacy study. As such Results
it was not powered to do anything other than provide The trial consisted of 20 participants representing 20
evidence of a 20% or greater wound area reduction over wounds. Two patients were withdrawn from the study
the first 5 weeks of therapy. The SPSS software (SPSS, due to loss of follow-up. Therefore, 18 participants repre-
Inc, Chicago, IL) statistical package was used, and the senting 18 ulcers successfully completed the study. The
student t test and Chi-square test were applied. study population of recruited individuals (n = 18) com-
Data collection. At the initial visit (week 1), investi- prised 14 (78%) males and 4 (22%) females.The mean age
gators verified completion of informed consent status was 55 years (range 31-84 years).The mean initial wound
and eligibility checklist. A complete history and physi- size was 8.2 cm2 (range 1.5-25.5 cm2), and the mean ulcer
cal exam were performed, and concomitant medica- age was 35 months (range 3-126 months) (Table 1).
Vol. 28, No. 4 April 2016 115Yang et al
glycans, proteoglycans, fibronec-
tin, and growth factors, which
promote granulation and epithe-
lialization of dermal wounds.15-19
The fish-skin graft is composed
of previously mentioned compo-
nents plus the added benefits of
omega-3 lipids. Using a natural,
piscine 3D scaffold product has
early data supporting efficacy
compared to porcine ECMs and
represents a novel approach to
treat these hard-to-heal lower
extremity wounds.16,20 Baldurs-
son et al16 conducted a noninfe-
riority study that compared the
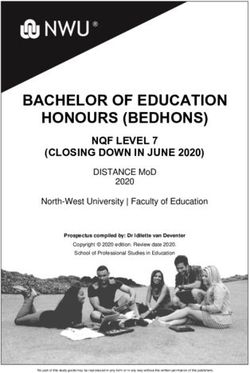
Figure 2. Wound depth. A 48% decrease in wound depth was seen in week 5; effect of fish skin ADM against
*P < 0.05. porcine small intestine submu-
cosa ECM in the healing process
Over a 5-week period, 5 weekly applications of the of 162 full-thickness, 4-mm wounds on the forearm of 81
extracellular matrix (ECM) and secondary dressing volunteers. The fish-skin product was noninferior at the
(P < 0.05) resulted in a 40% decrease in wound surface primary end point, healing at 28 days compared to por-
area (Figures 1 and 3). A 48% decrease in wound depth cine ADM. Furthermore, the wounds treated with fish-
was seen with 5 weekly applications of the ECM and skin grafts healed significantly faster and exhibited no
secondary dressing (P < 0.05) (Figure 2). No significant autoimmune reactions.16
change was seen in surface area or depth from weeks Studies on the impact of omega-3 fatty acids on heal-
5 to 8 with secondary dressing alone. A nonstatistical- ing and inflammation have found them to be mostly
ly significant reduction in reported pain and drainage beneficial.11-13,21 The most interesting quality is the an-
was seen. Three out of the 18 patients received com- ti-inflammatory effect of omega-3, EPA, and DHA. Mc-
plete wound closure by the end of the study phase. Daniel et al,11 gathered 18 individuals randomized to
28 days of either EPA + DHA supplementation (active)
Discussion or placebo. After 28 days, the active group had signifi-
It is widely accepted that healing chronic wounds cantly higher plasma levels of EPA + DHA and lower
requires moist environments, an effective antimicrobial 15-lipoxygenase. On day 28, eight 8-mm blisters were
barrier, and protection against MMP proliferation.8,14 An created on the forearms of the patients to initiate in-
ideal dressing should address all the above issues at a sig- flammation and produce wound fluid for lipid mediator
nificantly reduced cost of care. Biomedical tissue engi- and proinflammatory cytokines quantifications. The ac-
neering is a promising approach that has received great tive group had lower mean levels of myeloperoxidase
attention to restore wound-bed structure in chronic and more re-epithelialization on day 5 postwounding.12
nonhealing wounds. In Armstrong et al,15 punch biopsy While this study did not assess these properties as they
wounds in 20 subjects were treated with a collagen ma- may apply to topically applied omega-3 fatty acids, fu-
trix or Monsel’s solution. The collagen matrix produced ture in vivo studies now underway will assess such in-
less inflammation, had a lower incidence of wound in- flammatory responses.
fection, was associated with a faster re-epithelialization The purpose of this study was to evaluate the safety
rate, and healed with a better appearance at 4 weeks and effectiveness of the fish-skin graft in 20 eligible
than did Monsel’s solution.15 Many mammalian and por- patients with at least 1 ulcer meeting the “hard-to-heal”
cine collagen tissues have been widely used as ECM criteria. The etiologies of these wounds were either/or
structural protein applications for skin substitutes. Im- a combination of diabetic, venous, or arterial disease.
portant components of these ECM include glycosamino- The primary objective of this study is to assess the per-
116 WOUNDS® www.woundsresearch.comYang et al
centage of wound closure area
from baseline after 5 applica- A B
tions of fish skin. The authors
chose to apply the fish-skin graft
for 5 weeks at weekly intervals,
which in many similar studies
represents a near ideal applica-
tion cycle.17,22 They also chose,
as a primary endpoint, a well-
recognized surrogate marker of
eventual wound closure.23 The
uses of a surrogate endpoint
other than complete closure
has been well established; a sur-
rogate endpoint usually occurs
Figure 3. Ulcer at (A) week 0 and (B) week 5 following weekly extracellular matrix ap-
early in the course of therapy,
plication and secondary wound dressing.
this time frame is intended to
assess real-world outcomes of a
patient’s response to treatment. Clinicians can use valid tween fish skin and porcine or mammalian ECM are the
surrogate markers for rapid screening of potential ther- beneficial effects of bioactive lipid mediators.
apies, therefore aiding in the discovery of novel treat- The limitations of this pilot study include a small
ments that correlate with true clinical outcomes.23-25 sample size, lack of a control arm, and an aggressive ap-
Gelfand et al23 assessed the surrogate endpoints for plication schedule. Investigational studies are needed
the treatment of venous leg ulcers in which 56,488 with larger sample sizes to assess further efficacy of
wounds from 29,189 patients were analyzed. The study the acellular fish-skin graft and to compare its effective-
demonstrated in a large, diverse patient population that ness to other ECM-derived scaffolds. Studies designed
the percent change in area, log healing rate, and log area in a similar fashion to other studies using mammalian
ratio at the fourth week of care can serve as important ECM would be interesting.17,22
surrogate markers of complete wound healing at 12 or
24 weeks of care. The authors recommend using the Conclusion
time frame of approximately 4 weeks of treatment for This product appears to provide promise as an ef-
studies being conducted to screen initial wound heal- fective wound closing adjunctive ECM. This is espe-
ing agents in diseases in which the true outcome is cially true when used in this compassionate setting,
delayed.23 Sheehan et al26 showed that in diabetic foot where many other products fail. However, clearly a bet-
ulcers there was an absolute wound area reduction at ter body of evidence is necessary in regards to its best
4 weeks (82% reduction vs. 25% reduction; P < 0.001), application.
which correlated with the absolute closure rate at 12
weeks (58% reduction vs. 9% reduction; P < 0.01).26 References
The authors’ data indicates that the fish-skin graft 1. Krishnan S, Sekar S, Katheem MF, Krishnakumar S, Sas-
exceeded their expectations, with > 20% surface area try TP. Fish scale collagen—a novel material for corneal
of the patients’ wounds closing between weeks 0 to 5 tissue engineering. Artif Organs. 2012;36(9):829-835.
with 5 weekly fish-skin graft applications and second- 2. Kjartansson H, Magnusson S, Baldursson BT, Sigurjons-
ary dressings. Given the increased rate of closure, no son GF. Fish skin acellular dermal graft facilitates cel-
threat of known disease transmission or immune reac- lular ingrowth. Paper presented at: 7th Joint Meeting
tivity, benefits of bioactive lipid mediators, and ease of of the European Tissue Repair Society with the Wound
use, the fish-skin graft appears to be at least noninferior Healing Society 25th Annual Meeting of ETRS Scandic
to ADMs derived from mammalian tissue. This product Copenhagen; October 21-23, 2015; Copenhagen, Den-
can be used as a suitable, safe, alternative for skin sub- mark.
stitute. Possibly, the most fundamental difference be- 3. Rakers S, Niklasson L, Steinhagen D, et al. Antimicro-
Vol. 28, No. 4 April 2016 117Yang et al
bial peptides (AMPs) from fish epidermis: perspec- 17. Mostow EN, Haraway GD, Dalsing M, Hodde JP, King D;
tives for investigative dermatology. J Invest Dermatol. OASIS Venus Ulcer Study Group. Effectiveness of an ex-
2013;133(5):1140-1149. tracellular matrix graft (OASIS Wound Matrix) in the
4. Rakers S, Gebert M, Uppalapati S, et al. ‘Fish matters’: treatment of chronic leg ulcers: a randomized clinical
the relevance of fish skin biology to investigative der- trial. J Vasc Surg. 2005;41(5):837-843.
matology. Exp Dermatol. 2010;19(4):313-324. 18. Turner NJ, Badylak SF. The use of biologic scaffolds
5. Le Guellec D, Morvan-Dubois G, Sire JY. Skin develop- in the treatment of chronic nonhealing wounds. Adv
ment in bony fish with particular emphasis on collagen Wound Care (New Rochelle). 2015;4(8):490-500.
deposition in the dermis of the zebrafish (Danio rerio). 19. Badylak SF, Freytes DO, Gilbert TW. Reprint of: Extracel-
Int J Dev Biol. 2004;48(2-3):217-231. lular matrix as a biological scaffold material: structure
6. Diegelmann RF, Evans MC. Wound healing: an overview and function. Acta Biomater. 2015;23(Suppl):S17-S26.
of acute, fibrotic and delayed healing. Front Biosci. 20. Richardson R, Slanchev K, Kraus C, Knyphausen P, Em-
2004;9:283-289. ing S, Hammerschmidt M. Adult zebrafish as a model
7. Clark RA. Fibrin and wound healing. Ann N Y Acad Sci. system for cutaneous wound-healing research. J Inves
2001;936:355-367. Dermatol. 2013;133(6):1655-1665.
8. Lev-Tov H, Li CS, Dahle S, Isseroff RR. Cellular versus 21. Serhan CN. Pro-resolving lipid mediators are leads for
acellular matrix devices in treatment of diabetic foot resolution physiology. Nature. 2014;510(7503):92-101.
ulcers: study protocol for a comparative efficacy ran- 22. Niezgoda JA, Van Gils CC, Frykberg RG, Hodde JP. Ran-
domized controlled trial. Trials. 2013;14:8. domized clinical trial comparing OASIS Wound Matrix
9. Chalimidi KR, Kumar Y, Kini UA. Efficacy of collagen to Regranex Gel for diabetic ulcers. Adv Skin Wound
particles in chronic non healing ulcers. J Clin Diagn Care. 2005;18(5 Pt 1):258-266.
Res. 2015;9(6):PC01-3. 23. Gelfand JM, Hoffstad O, Margolis DJ. Surrogate end-
10. Lipscomb, GH, Ling, FG. Wound healing, suture material, points for the treatment of venous leg ulcers. J Invest
and surgical instrumentation. In: Rock JA, Jones HA III, Dermatol. 2002;119(6):1420-1425.
eds. TeLinde’s Operative Gynecology, 9th ed. Philadel- 24. Temple R. Are surrogate markers adequate to assess
phia, PA: Lippincott Williams & Wilkins;2003:233. cardiovascular disease drugs? JAMA. 1999;282(8):790-
11. McDaniel JC, Belury M, Ahijevych K, Blakely W. Omega-3 795.
fatty acids effect on wound healing. Wound Repair Re- 25. Prentice RL. Surrogate endpoints in clinical trials: defi-
gen. 2008;16(3):337-345. nition and operational criteria. Stat Med. 1989;8(4):431-
12. McDaniel JC, Massey K, Nicolaou A. Fish oil supplemen- 440.
tation alters levels of lipid mediators of inflammation 26. Sheehan P, Jones P, Giurini JM, Caselli A, Veves A. Percent
in microenvironment of acute human wounds. Wound change in wound area of diabetic foot ulcers over a
Repair Regen. 2011;19(2):189-200. 4-week period is a robust predictor of complete heal-
13. Alexander JW, Supp DM. Role of arginine and omega-3 ing in a 12-week prospective trial. Plast Reconstr Surg.
fatty acids in wound healing and infection. Adv Wound 2006;117(7 Suppl):239S-244S.
Care (New Rochelle). 2014;3(11):682-690.
14. Sood A, Granick MS, Tomaselli NL. Wound dressings and
comparative effectiveness data. Adv Wound Care (New
Rochelle). 2014;3(8):511–529.
15. Armstrong RB, Nichols J, Pachance J. Punch biopsy
wounds treated with Monsel’s solution or a colla-
gen matrix. A comparison of healing. Arch Dermatol.
1986;122:546-549.
16. Baldursson BT, Kjartansson H, Konrádsdóttir F, Gudna-
son P, Sigurjonsson GF, Lund SH. Healing rate and auto-
immune safety of full-thickness wounds treated with
fish skin acellular dermal matrix versus porcine small-
intestine submucosa: a noninferiority study. Int J Low
Extrem Wounds. 2015;14(1):37-43.
118 WOUNDS® www.woundsresearch.comYou can also read