A parent's guide to managing sickle cell disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

A parent’s guide to managing sickle cell disease

What’s inside?
What
Whatis is
8 Authors 15 Sickle haemoglobin with
Sickle
Hereditary Persistence of Fetal
Sickle
8 Acknowledgements
9 Foreword Haemoglobin (HbS/HPFH)
Cell
Cell
15 Sickle haemoglobin D Punjab
If you are told your child has sickle
Disease?
disease (HbSDPunjab)
Disease?
cell disease you will probably have
hat is sickle cell
W 15 Sickle haemoglobin E disease
lots of questions. In this book we disease? (HbSE)
15 Sickle haemoglobin O-Arab
disease (HbSOArab)
Management and treatment
will describe what sickle cell disease 12 What is sickle cell disease?
15 Other unusual haemoglobin
12 What causes the cells to sickle?
is, the different types, treatments 13 How did my child get sickle cell
combinations
available and offer practical advice disease? 16 Sickle haemoglobin carriers
and those carrying other
on living with and supporting a child 14 Types of sickle cell disease unusual haemoglobins
14 Sickle cell anaemia (HbSS)
with sickle cell disease. 14 Sickle haemoglobin C disease
17 Why did sickle cell first occur and
who is affected?
(HbSC)
14 Sickle beta thalassaemia disease 17 The effects of sickle cell disease
Living with Sickle Cell Disease
(HbSβ) 17 How does sickle cell affect
children?
All rights reserved. No reproduction or transmission of this publication may be made without prior
permission of the authors in accordance with the provision of the Copyright, Designs and Patent
Act 1988. Permission should be sought for the use of the content and design from the Brent Sickle
Cell & Thalassaemia Centre and the Sickle Cell Society.
© 1st Edition 1997, Brent Sickle Cell & Thalassaemia Centre, London ISBN 0 9531902 0 X
© 2nd Edition 2006, Brent Sickle Cell & Thalassaemia Centre, London ISBN 0 9531902 7 7
Other information
© 3rd Edition 2012, Brent Sickle Cell & Thalassaemia Centre, London ISBN 0 9531902 9 3
© 4th Edition 2021, Sickle Cell Society and Brent Sickle Cell
& Thalassaemia Centre, London ISBN 978 1 8383098 2 4
1st edition funded by The Department of Health, 2nd and 3rd edition funded by the NHS Sickle Cell
& Thalassaemia Screening Programme, London, 4th edition funded by Sickle Cell Society
Copies of this book and other resources can be downloaded from the Sickle Cell Society
www.sicklecellsociety.org
This book is likely to be reviewed in 2025. Picture drawn by Chakoura
3
– Anaemia 29 Other immunisations 40 The National Haemoglobinopathy – Silent stroke
– Jaundice – Pneumovax Registry 49 Eye problems
What is Sickle Cell Disease?
– Physical growth and – ACWY 50 Headaches
42 Managing an illness at home
development – Hepatitis B
42 Fever 50 Medical emergencies
– Enlarged spleen – Influenza (flu)
42 Thermometers 50 Situations when your child
– Painful episode
– How to use a digital rod needs to be seen by a doctor
– Bed wetting (Nocturnal Enuresis)
20 Will my child have all these signs
Management and thermometer straight away
– How to use a forehead tape
and symptoms? treatment thermometer 50 What to expect if your child is
admitted to hospital
21 What can I do to keep my child 43 What to do if your child has a
32 Managing your child when raised temperature 51 Getting to know the
well?
away from home children’s ward
Management and treatment
22 Diet and nutrition 44 Managing sickle cell pain at home
32 Carers, child minders and nurseries 51 Some things that may help you
23 What about giving extra vitamins – Giving painkillers (analgesics)
32 Your child in school 52 Common reasons for
or iron supplements? – Extra fluids
– Educational progress hospital admission
24 Avoiding things which may trigger – Warm baths
34 Travelling and going abroad – Pain relief
an illness – Using warm moist towels or
– Malaria prevention and – Receiving other medications
– Infection heat pads
medication – Intravenous fluids (drip)
– Adequate fluids – Massage
– Travel vaccinations – Medical investigations
– Extremes of cold and heat – Quiet play and distraction
(temperatures) – Other medications whilst abroad – Blood transfusion
45 When to seek medical and
– Stress and anxiety – Travel insurance nursing help 53 Going home after a
Living with Sickle Cell Disease
– Medical reports and other hospital admission
– Physical exertion
documents to take with you 46 Some medical problems
55 Blood transfusion
25 Common ailments – effect on – Care whilst travelling 46 Painful episodes
children with sickle cell disease 55 Types of blood transfusion
– Preventing an illness whilst 47 Sudden enlargement of the spleen
25 Coughs and colds (upper abroad (acute splenic sequestration) 55 Blood transfusion before
respiratory infections) an operation
– Checklist before you travel 47 Parvovirus B19 infection
26 Influenza (flu) and Covid-19 55 Blood safety
47 Chest infection and acute chest
26 Diarrhoea and vomiting 38 Visiting the hospital outpatient syndrome 56 Religion and blood transfusion
clinic 56 Managing iron overload
26 Urine infection 47 Painful hip (avascular necrosis of
38 Why does my child need to go the femoral head)
Other information
26 Headaches 57 Developments in the
to clinic?
27 Rashes 48 Infection in the bone management of sickle cell
– Getting information and support (osteomyelitis)
27 Asthma disease
– Having blood tests and other 48 Blood in the urine (haematuria)
investigations 57 Hydroxycarbamide (hydroxyurea)
27 Immunisations and 48 Gallstones 58 Bone marrow transplantation,
preventative medications 40 Contact between the hospital
48 Painful erection of the penis (BMT), (stem cell transplantation)
– Penicillin clinic and your child’s GP
(priapism) 59 Gene therapy
28 Routine childhood immunisations 49 Stroke
4 5
59 New drug treatments 68 How to tell your child about – Sources of further information 103 NHS England Haemoglobinopathy
sickle cell disease – Carers UK Coordinating Centre (HCC) and
60 Medical tests and what they
What is Sickle Cell Disease?
68 Your young child with sickle cell – England, Scotland and Wales National Haemoglobinopathy
mean disease Panel (NHP)
– Additional information about
60 Blood tests 69 Your teenager (adolescent) with benefits and support for carers 104 Sickle cell and thalassaemia
– Haemoglobin electrophoresis sickle cell disease
centres
– Reticulocyte count 70 Coping with sickle cell disease 77 Pregnancy and future births
– Full blood count (FBC) and pain 77 What are the chances of having 105 Local patient support groups
– Haemoglobin S (HbS) level 71 Brothers and sisters another child with sickle
– Haemoglobin F (HbF) – How to manage brothers’ and cell disease? 105 National voluntary
sisters’ feelings? 78 How do we find out which type organisations
– Blood chemistry
71 Dealing with grandparents and of haemoglobin my partner and I 105 The Sickle Cell Society
– Glucose 6 phosphate
Management and treatment
other family members have? 106 United Kingdom Thalassaemia
dehydrogenase (G6PD)
deficiency test 78 What can our child inherit? Society (UKTS)
71 Practical issues 85 Can a pregnancy be tested 106 Membership of support groups
61 Urine test
for coping before birth? and voluntary organisations
61 X-rays and scans
72 Forward planning 85 Types of prenatal diagnosis
– Chest X-ray 107 Sickle cell and thalassaemia
72 The working parent (PND) tests
– Bone X-ray all party parliamentary group
72 Questions which parents often ask – Chorionic villus sample (CVS)
– Ultrasound scan of the abdomen (APPG)
about employment issues – Amniocentesis
– Echocardiogram
85 What if the result shows that 107 Glossary of terms and
– CT scan 75 Social care and welfare rights
the foetus has sickle cell disease? abbreviations
Living with Sickle Cell Disease
– MRI scan – Universal Credit
87 What will happen after the
– MRA scan – Benefits Calculators baby’s birth? 111 Useful reading
– Transcranial Doppler scan – Links to the calculators 87 Pre-implantation genetic diagnosis 111 Useful websites
– Benefits for families
88 Questions parents often ask
Living with Sickle – Specific Benefits
– Disability Living Allowance (DLA)
112 Sickle cell and thalassaemia
centres and services
Cell Disease for children under 16
– Disability Living Allowance
Other information – Greater London
– Outside London
66 Feelings and family helpline 98 Health and social care
relationships – Disability Living Allowance (DLA) providers 115 Patient support groups and
Other information
66 How you may feel when told that for children (claim form) voluntary organisations
your child has sickle cell disease – Personal Independence Payment 103 National Health Service (NHS)
specialist provision 117 Other useful contacts
66 Public attitudes to sickle cell (PIP) for those 16 to 64 years of
disease age 103 Local Haemoglobinopathy 118 National Newborn and
– Carer’s Allowance Teams (LHT) and Specialist Children’s Standards
67 Your emotional wellbeing
Haemoglobinopathy Teams (SHT)
67 Who can help? – Disabled Students’ Allowances
(DSA) 126 Index
6 7
Authors Foreword cell disease. We hope that this handbook
will dispel some of these by giving you
Dr Lola Oni, OBE, Specialist Nurse Perhaps you have just been told that
clear, accurate information.
Consultant/ Service Director/ Lecturer, your newborn baby or older child has
Brent Sickle Cell & Thalassaemia Centre, sickle cell disease and have learnt that it We have tried to make this book easy
London Northwest University Healthcare is an inherited condition which affects to understand and to use. Some of the
NHS Trust, London. the blood. Like most parents when given scientific terms may be new to you. These
such news you may feel shock, and be are briefly explained in the glossary (page
Joan Walters, Senior Nurse Practitioner
confused, angry or afraid. Often parents 107). You may want to read the book all
Lecturer Child Health / Paediatric
cannot believe the news and may feel the way through. You can also just dip
Haematology, King’s College Hospital NHS
responsible or blame themselves for into it to find out about particular aspects
Trust and Florence Nightingale School
‘giving’ their child a disease. They may not of sickle cell disease. The book is an
of Nursing & Midwifery, King’s College,
know what to say to relatives and friends. introduction and a start of your learning
London University.
They are bewildered about how to care for about the condition. It is important to
Professor David Rees, Consultant their child and what to expect in future. get more detailed information from the
Paediatric Haematologist, King’s College people caring for your child as they will
Such feelings are natural to all parents
Hospital NHS Trust, London. be familiar with the specific ways in which
when their child has been found to have
your child experiences the disease.
Dr Olu Wilkey, Consultant Paediatrician, an inherited condition, whether it is sickle
North Middlesex Hospital NHS Trust, cell or any other inherited disease. We See page 118 for a summary of the
London. hope that this handbook will help you government’s recommended national
come to terms with some of these feelings guidelines for the care and management
Other contributors and members of and help you to learn more about sickle of children with sickle cell disease.
the project team cell disease so that you will feel confident
Sickle cell disease affects both boys and
Dr Kofi Anie, Senior Clinical Psychologist, about looking after your child and will
girls. Apart from a medical condition called
Brent Sickle Cell & Thalassaemia Centre, know how and what to tell relatives and
priapism, which only affects boys/men, all
London Northwest University Healthcare friends. You may be living in an area
the things discussed in this book relate to
Trust, London. where there are few people with sickle
both sexes. But for fluency the term ‘he’ is
cell disease and your local healthcare
Daniel Nyakutsey, Welfare Support Adviser, used in the first half of the book and ‘she’
professionals may not have cared for many
SE London Sickle Cell & Thalassaemia in the second.
people with this condition. If that is the
Centre, London.
case, it is worth mentioning this book Please remember that not all things
Iyamide Thomas, NHS Engagement Lead, and other useful materials which can be mentioned in this book will affect
The Sickle Cell Society, UK. accessed at: www.sicklecellsociety.org your child.
Illustrations by Ellen Watters. You may have been told frightening things
about sickle cell disease or may know a
friend or member of your family who has
Acknowledgements the condition. Sickle cell disease is very
variable and affects people in different
We thank Public Health England and the Sickle Cell Society for funding this fourth edition.
Special thanks to the children, parents and families for inspiring the team to write the original
ways, even people in the same family,
and later editions. This book has become a crucial resource for parents and all those looking born of the same parents, so do not
after children with sickle cell disease. We also thank all the children who participated in the assume that how it affected the person
Children’s drawing competition. you know or knew is how it will affect
We hope the information contained in this book will continue to encourage and empower you
your child. There are quite a lot of myths
as you continue to make efforts to look after a child with sickle cell disease. and popular misconceptions about sickle
8 9
What is
What is Sickle Cell Disease?
Sickle Cell
Disease?
Sickle cell disease is a term
covering a number of
different but similar conditions
which affects haemoglobin.
Haemoglobin gives blood its What is sickle cell disease?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Types of sickle cell disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
red colour and is responsible for Sickle haemoglobin carriers and those carrying other unusual haemoglobins. . . . . . . . . . . . . . . . . . . . . . . . . 16
carrying oxygen from the lungs The effects of sickle cell disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
to all parts of the body. What can I do to keep my child well?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Common ailments – effect on children with sickle cell disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Immunisations and preventative medications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
10
What is Sickle Cell Disease?
What is sickle cell These conditions are called ‘sickle’ cell Getting very cold or dehydrated tends How did my child get sickle cell
disease because the red blood cells, which to make red cells lose oxygen and can disease?
disease? are normally round and very flexible, increase sickling. The things that can cause Sickle cell disease is inherited. This means
Sickle cell disease is a term covering become rigid and shaped like a crescent sickling of red cells and obstruction to that your child inherited an unusual type
a number of different but similar moon or farmer’s sickle. Red blood cells blood flow include: of haemoglobin from both you and your
conditions which affects haemoglobin. in sickle cell disease do not last as long in partner. (See illustrations from page 77).
• Dehydration (lack of water in the body)
Haemoglobin gives blood its red colour the body as normal red blood cells and this
and is responsible for carrying oxygen leads to anaemia. Sickled red blood cells • Infections and fevers The normal and most common
from the lungs to all parts of the body. are also not as flexible as normal red blood haemoglobin type is haemoglobin A.
• Sudden changes in body temperature, There are over 1000 different types of
The types of sickle cell disease commonly cells and cannot always pass through very
particularly skin cooling unusual haemoglobin but the ones that
seen in the United Kingdom are sickle cell small blood vessels. If the sickled cells get
anaemia (HbSS), Sickle Haemoglobin C trapped in the blood vessels, this reduces • Excessive physical exertion are commonly seen in the United Kingdom
disease (HbSC) and various forms of sickle the blood supply to that part of the body are haemoglobin S (sickle haemoglobin),
• Stress haemoglobin C, haemoglobin D and
beta thalassemia, such as, sickle beta and causes pain and sometimes damage.
plus thalassemia (HbS/β+ThaIassaemia) This is sometimes called a ‘painful crisis’. beta thalassemia. All babies are also born
See page 24 for more information on with baby or fetal haemoglobin called
and sickle beta zero thalassemia (HbS/ It often comes on suddenly, and typically
how to avoid some of the causes listed haemoglobin F, regardless of which adult
β0Thalassemia). These are described lasts several hours or days. Usually it does
above. haemoglobin gene they have inherited
further on page 14. not cause any permanent damage.
from their parents. Haemoglobin F
accounts for 90% of the newborn baby’s
What causes the cells to sickle? haemoglobin at birth but this amount
A normal red blood cell is round, soft, decreases gradually over the first few
spongy and very flexible. It carries oxygen
very well and is able to travel through the
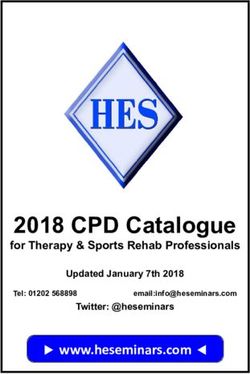
Sickled red blood cells are body without getting stuck in the blood Figure 1 Normal and Sickle cell blood flow
vessels. The sickle red blood cell on the
not as flexible as normal other hand is hard, rigid, breaks easily and
red blood cells and cannot is not able to keep its round shape.
always pass through very Red blood cells change to a sickle shape
small blood vessels. when oxygen levels in the body are low.
They usually return to their original round Normal red blood cell
shape when they get more oxygen, often
when they have passed through the
lungs, but after a while they lose their
ability to make this change and cease
to carry oxygen.
Sickle red blood cell Normal blood flow Sickle blood flow (blockage)
12 13
What is Sickle Cell Disease?
years of life to reach adult levels of about The aim is that all children with sickle Sickle haemoglobin with hereditary health problems. Penicillin and transcranial
1%. Some children with sickle cell disease cell anaemia will live happy and normal persistence of fetal haemoglobin doppler scans are usually recommended.
carry on producing small amounts of lives, although medical problems will (HbS/HPFH)
haemoglobin F, which may be beneficial. occur sometimes. This occurs if your child has inherited sickle Sickle haemoglobin O-Arab disease
An inherited condition like sickle cell On average, people have about one haemoglobin from one parent and high (HbSOArab)
disease remains with a person all their life. significant health problem per year that is fetal (baby) haemoglobin levels (HbF) from This is a rare form of sickle cell disease,
related to this form of sickle cell disease. the other parent. Your child will continue occurring when haemoglobin S is inherited
Sickle cell disease varies in severity from to make significant amounts of fetal from one parent and haemoglobin O-Arab
one person to the next for reasons that are haemoglobin (approximately 30%) and
Sickle haemoglobin C disease from the other. Haemoglobin O-Arab
not clear. It is known that inheriting alpha should have very mild sickle cell disease
(HbSC) occurs in the Middle East, but is also found
thalassaemia trait (also known as being an with no significant problems. Penicillin and in populations across the world. This
alpha thalassaemia carrier) or having the This occurs if your child has inherited transcranial doppler scans are not usually combination usually causes a disease like
ability to make lots of haemoglobin F tend sickle haemoglobin from one parent recommended for those with S/HPFH. sickle cell anaemia (HbSS), and is similarly
to make sickle cell disease less severe. and haemoglobin C from the other. In
variable, with some people getting more
general, HbSC disease is less severe than
There are many things that you can do to
sickle cell anaemia but the same health
Sickle haemoglobin D Punjab problems and others very few. Regular
keep your child healthy and it is important
problems can occur.
disease (HbSDPunjab) penicillin and transcranial doppler scans
to recognise early signs of illness which This is a rare form of sickle cell disease are usually recommended.
can then be treated promptly. and occurs if your child has inherited
Sickle beta thalassaemia disease
sickle haemoglobin from one parent and Other unusual haemoglobin
(HbSβthal)
Types of sickle cell haemoglobin D Punjab from the other combinations
This occurs if your child has inherited parent. This is usually similar to sickle cell There are several other combinations of
disease sickle haemoglobin from one parent anaemia, causing similar health problems. unusual haemoglobin which can cause
and beta thalassaemia from the other. Penicillin and transcranial doppler scans
All babies are now tested for sickle disease sickle cell disease but these are rare.
There are many different types of beta are usually recommended.
in their first week of life using a spot of
thalassaemia mutation. A mild beta In this book we write about sickle cell
blood taken from a heel prick. It usually
thalassaemia mutation in combination disease as if it is one condition although
takes a few weeks to get the results, Sickle haemoglobin E disease
with sickle haemoglobin causes sickle the different types are not all the same,
and if the baby seems to have sickle (HbSE)
beta plus thalassaemia, commonly written and everyone’s experience of an illness
cell disease a repeat test is necessary to
HbS/β+thaIassaemia; this combination Haemoglobin E (HbE) is very common differs. Some experience milder symptoms
confirm this and find out exactly which
usually causes less severe disease. A severe in Southeast Asian countries, like than others and children with the same
type of sickle cell disease he has inherited.
form of the beta thalassaemia mutation Thailand and Vietnam, and also in parts sort of sickle cell disease, even children
in combination with sickle haemoglobin of India and Bangladesh; it is a type of with the same parents, may have different
Sickle cell anaemia (HbSS) results in sickle beta zero thalassaemia, thalassaemia. Sickle haemoglobin E occurs experiences and medical problems.
This is the commonest form of sickle commonly written HbS/β0thaIassaemia, if your child inherits sickle (HbS) from one
cell disease and occurs if your child has which is often more like HbSS. parent and haemoglobin E from the other.
inherited sickle haemoglobin (HbS) from It causes a mild form of sickle cell disease
For more information about beta sometimes with problems such as acute
both parents. Sickle cell anaemia is very
thalassaemia contact the UK Thalassaemia pain, but does not usually cause major
variable and it is not possible to predict
Society (details on page 106) or one of the
what sort of problems might occur.
specialist centres listed on page 112.
14 15
What is Sickle Cell Disease?
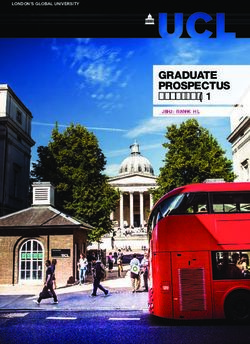
Sickle haemoglobin a carrier of the sickle cell gene may have other parent (HbAβthalassaemia). These • 1 in 20-50 Asians
some health problems, such as pain in do not cause health problems, but might
carriers and those the spleen. There is also evidence that make some of the person’s blood/results
• 1 in 100 Northern Greeks
carrying other unusual kidney problems are a bit more common slightly abnormal. For example, people For information about malaria and the
especially as people get older, and very who carry beta thalassaemia tend to have need for protection see page 35. All the
haemoglobins rarely, extreme exercise may cause severe small, pale red cells and might be very other unusual haemoglobin types that
Being a ’carrier’ of sickle haemoglobin dehydration, heat exhaustion and severe slightly anaemic which can be mistaken have been described here probably also
is sometimes known as having sickle cell illness. for a condition called iron deficiency and offer some protection against malaria.
trait, and does not usually cause significant treated with iron tablets unnecessarily.
illness. It is not a form of sickle cell disease People who are sickle cell carriers (HbAS)
and will never change into sickle cell may need to train differently if they The importance of knowing if you The effects of sickle cell
join the armed forces or take up sport carry sickle cell or any other unusual
disease. If a person is born a carrier they
professionally. haemoglobin is that it can be passed on to
disease
are healthy and will always be a carrier.
your children. How this inheritance works
Being a carrier of sickle haemoglobin Other common haemoglobin carrier states How does sickle cell affect children?
is explained further on pages 78-84.
means that you have inherited normal seen in the UK include haemoglobin C During the first few months of life, your
haemoglobin A from one parent and sickle carrier, where a person has inherited child may not show signs of having
normal haemoglobin A from one parent Why did sickle cell first occur and
haemoglobin S from the other; this is who is affected? sickle cell disease, because at birth
sometimes commonly written HbAS. and haemoglobin C from the other there is a high (about 90%) level of
parent (HbAC). Beta thalassaemia carrier It is thought that the sickle cell baby haemoglobin which is called Fetal
In extreme conditions where there is a is when a person has inherited normal haemoglobin first occurred thousands of haemoglobin (HbF), and usually a very
lack of oxygen, such as when deep sea haemoglobin A from one parent and beta years ago, probably in Africa and other low level of sickle haemoglobin S (HbSS)
diving or being on top of a high mountain, thalassaemia (βthalassaemia) from the tropical countries. Being a carrier for (about 5-10%) or any other unusual
sickle haemoglobin seems to offer some haemoglobin that your child has inherited.
protection against malaria, which is often For example in the combination of HbSC,
fatal in young children. Over thousands the child will make about 5-10% of S and
Figure 2 Worldwide distribution of the Sickle Cell Gene of years, sickle cell trait has become C combined. Over the first year of life the
increasingly common in areas of the world haemoglobin F begins to reduce as your
where malaria occurs, and more children child starts making more haemoglobin S.
are therefore born in these areas with The rate at which haemoglobin F drops
sickle cell. can be linked to when the symptoms of
This is why we find haemoglobin S in sickle cell disease start. Some children
people whose ancestors come from Africa, have higher than usual amounts of
Asia, the Middle and Far East and the haemoglobin even till adult hood, and this
Mediterranean. Sickle cell trait is found in may be beneficial. The longer your child
approximately: goes on making haemoglobin F the better,
because it means he will be making less
• 1 in 4 West Africans
haemoglobin S and is less likely to have
• 1 in 10 Afro-Caribbeans serious sickle cell complications or crises.
• 1 in 12 Turks
16 17
Children with sickle cell
disease may be smaller
than those who do not
have the condition but
What is Sickle Cell Disease?
they generally grow at
a steady rate. the body uses folic acid when making new in such cases your child needs to see a your child’s spleen is big and can be felt
red blood cells. However, in the United doctor. (See page 48.) just below the rib cage. The spleen may
Kingdom most children get enough folic continue to be enlarged for some time but
However, your child will still be at risk of acid from their normal diet and extra folic Physical growth and development then reduces in size and may stop working
serious infection and will need to be on acid is not necessary. There is no evidence It is usual for children with sickle cell altogether. This is because it becomes
penicillin (oral antibiotics) by 3 months to suggest that giving folic acid will disease to be thinner and slightly shorter filled with the sickled red blood cells that
of age. (See page 27.) One of the first improve your child’s health, but it does no than children who do not have the it is trying to clear from the body. If the
signs of sickle cell complications, which harm. Only give folic acids if directed to do condition but they generally grow at a spleen gets filled with sickle cells it cannot
may occur after the age of about 6 -18 so by your child’s specialist doctor. steady rate. They tend to go through clear the body of infection. This is why we
months, is swelling of one or more fingers puberty later than average but they go on recommend that your child takes penicillin
There are some rare additional
or other parts of the hand, or one or more growing for a little bit longer to eventually twice daily. (See page 27 for further
complications of sickle cell disease which
toes or other parts of the foot. This is reach their normal adult height. information on penicillin). Sometimes a
can lead to a worsening of the anaemia,
known as hand-foot syndrome, also called lot of blood gets trapped in the spleen
such as acute splenic sequestration. Enlarged spleen
dactylitis. Although this may be distressing and it gets very big worsening the
(See page 47.)
at the time it does not mean the child will The spleen is an organ that lies on the child’s anaemia. This is an acute splenic
necessarily have more problems in the Jaundice left side of the stomach under the rib sequestration. (See page 47.)
future. This symptom of crisis is usually cage. The spleen helps to clear infection
When the red blood cells come to the Depending on the type of sickle cell
treated with simple pain medicine and from the body and also clears up old or
end of their useful life, they are broken disease your child has, you may be shown
the child is encouraged to drink extra oral damaged blood cells. One of the first
down in the body; one of the substances how to feel your child’s spleen when he
fluids. things that your doctor may notice is that
produced during this process is a yellow
Anaemia pigment called bilirubin.
When a child is making a lot more The liver clears the bilirubin from the
haemoglobin S, these red blood cells have body, but if there is a lot of bilirubin being Figure 3 Spleen being examined
a much briefer life span than the cells produced the liver may not be able to clear
that contain the usual haemoglobin A. it all away and the yellow pigment may
The body tries to compensate by making appear in the eyes, a condition known as
more red blood cells but it usually cannot jaundice. Some children may always have
compensate completely hence your child slightly yellowish eyes, even when they are
becomes anaemic. Your child may look well. Others may only become jaundiced You may be shown how to
when they are unwell, for example with feel your child’s spleen when
pale and the palm of his hand and his
he is well, so that when he
lips will be paler than your own. This sort coughs and colds or when they are in pain
is unwell you can tell. If it is
of anaemia is known as a haemolytic or have other ailments. bigger than usual he should
anaemia and is not the same as the sort be seen by a doctor.
It can be a useful sign that your child is
of anaemia caused by lack of iron. For this
not as well as usual. There is no specific
reason, iron tonics or medicines should not
treatment for this sort of jaundice and the
be given unless prescribed by your child’s
common practice of giving your child lots
doctor. (See page 23.)
to drink will not make much difference.
Folic acid tablets or other vitamin If they have very significant jaundice this
medications may be prescribed because may be associated with gallstones, and
18 19What is Sickle Cell Disease?
is well, so that you can tell if it is getting Bed wetting (Nocturnal Enuresis) beta zero thalassaemia (HbSβ°Thal) are What can I do to keep my
bigger and could need medical attention. Bedwetting is normal in all children up usually anaemic and may get jaundiced
We recommend that you feel your child’s until the age of about 7 years. It may when they unwell. Some children are child well?
spleen once daily, especially when your take longer for a child with sickle cell mildly jaundiced all the time. Not all In the first few months of life, your child
child is unwell. disease to become dry at night. Because of children with sickle cell disease have will grow and develop like any other baby
tiredness from the anaemia the child may an enlarged spleen or dactylitis (hand- and should not be affected by sickle cell
Painful episode foot-syndrome). Some children rarely disease. This is because he will still be
sleep very deeply at night and not wake
Pain is a known and sometimes common up in time to go to the toilet. In addition, experience pain although this is the producing a lot of baby haemoglobin
symptom of sickle cell disease. The classic in sickle cell disease the kidneys are not commonest symptom of sickle cell disease. F and not so much haemoglobin S.
pain episode seen in sickle cell disease is able to produce concentrated urine. However, one of the main risks is serious
Children who have sickle – haemoglobin
often called a ‘painful crisis’, which occurs Urine in the bladder is very dilute. The infection due to ‘pneumococci’. Even in
C disease (HbSC) or some types of sickle
when the very small blood vessels become bladder becomes very full and the child the first few months the spleen may not
beta plus thalassaemia (HbSβ+Thal) – tend
blocked by ’sickled’ red blood cells. Usually has to get up at night, sometimes several be able to clear the body of this infection.
to be only slightly anaemic and usually do
the pain will last several days, although times, to go to the toilet. In addition The national standard for medical care
not get jaundiced unless they have a sickle
sometimes it lessens more quickly. When he is encouraged to drink lots of water of children with sickle cell disease is
cell complication. An enlarged spleen in
this occurs your child will need to be given during the day so his kidneys will produce that your baby should take twice-daily
these forms of sickle cell disease is more
regular painkillers and plenty of fluids more urine. Wetting the bed is outside penicillin (an antibiotic) from the age of
common and does not usually cause any
and occasionally may need admission to your child’s control and he should never 3 months so as to prevent this infection.
serious problems.
hospital, depending on what is causing be punished. This will be recommended strongly by
the painful episode. If the pain gets better For information on medical your doctor. This and other standards
quickly in a few hours, it may not be Bedwetting is therefore not uncommon complications of sickle cell disease see of care can be found in the ‘Sickle Cell
caused by sickle cell disease, and might be in children with sickle cell disease. Most pages 46-50. Disease in Childhood: Standards and
a simple headache or tummy pain which achieve dryness eventually and there are Recommendations for Clinical Care’
everybody gets sometimes. certain techniques that can help. We publication available on the Sickle Cell
suggest you talk to your specialist nurse or
Dactylitis, also known as ’hand-foot doctor if you are concerned.
syndrome’ may be the first painful episode
that you see and usually occurs between
Will my child have all these signs
the ages of 6 and 18 months when a
and symptoms?
finger or other parts of the hand, or a toe
or other parts of the foot, become swollen Not necessarily. The aim of this book is to
and painful. After this age, pain may occur provide you with advice and guidance.
more commonly in the arms, legs or back. Every child may not encounter the exact
For further information about pain same experiences or complications. The
and how to manage sickle cell pain at advice provided is designed to guide you
home see pages 44-45. It is worthwhile with the information on what to do,
remembering that not all pain is due should you encounter some of the issues
to sickle cell crisis or related to sickle or complications outlined.
cell disease. Children especially those who have sickle
cell anaemia (HbSS) or those with sickle
20 21What is Sickle Cell Disease?
Society website at: www.sicklecellsociety. For how to manage sickle cell pain and are cooked according to the maker’s What about giving extra vitamins
org/paediatricstandards. other complications see page 44. instructions. Extra care needs to be or iron supplements?
taken if re-heating previously cooked On the whole extra vitamins are not
After about 3 to 6 months of age it is
Diet and nutrition food. Make sure the food is heated right needed as your child will get sufficient
possible that sickle cell problems may start
through, especially if you are using a from a normal balanced diet. The one
to occur. There are basic precautions that All growing children need protein,
microwave oven. vitamin that children do not get enough of
you can take to help keep your child well carbohydrates, fat, vitamins and minerals.
and these are outlined below. These they will get from a diet containing Parents often worry that their child with from their diet is vitamin D. We make this
fish, meat, fresh fruit and vegetables. It is sickle cell disease is not eating enough and vitamin from sunlight so it is important
Please remember that it is not always that your child gets enough sun on his
recommended that we should all eat five is not putting on weight. This is very rarely
possible to prevent a sickle cell skin. One of the symptoms of vitamin D
portions of fruit and vegetables every day. the case. Children with sickle cell disease
pain episode. deficiency is bone pain and this could get
tend to be thinner than others because
Children with sickle cell disease do not confused with sickle cell pain. If you are
most of the energy provided by the food
need special food. They should eat the concerned about this your specialist doctor
goes towards making new red blood cells
same foods as the rest of the family. If can do a blood test to check if your child
but they usually grow at a steady rate.
your family is vegetarian, it would be best is vitamin D deficient and may recommend
to talk to your health visitor to check that Your child will be routinely weighed and taking supplements.
your child is getting enough protein and measured at the outpatient clinic. Should
fat from his diet as well as vitamins and there be a problem with growth, this will All babies are advised to take Abidec
minerals needed for healthy growth. be identified early and discussed with you. (multivitamins). It is important that your
Your child needs to be encouraged to child continues to take this after the first
Sometimes children with sickle cell disease 2 years of life.
develop feeding skills at the appropriate
eat things which are not nutritious, such
age and eat food at regular mealtimes Your child does not need other vitamins
as chalk, paper, coal and furniture foam.
with the rest of the family. unless your family eats a special diet.
This is known as ’pica’ and the cause is
not known. It is usually not harmful but it If fasting is part of your family’s religious If your child becomes more anaemic than
is worth mentioning to your child’s doctor practice, you need to consider the special usual, and he is not already taking it,
if this occurs. needs of your child with sickle cell disease. folic acid supplements may be prescribed
Although he should not be brought up any by your doctor. This helps the body to
Children with sickle cell disease are
differently from his brothers and sisters, make more red blood cells. Some clinics
more at risk from certain infections,
fasting for long periods of time may cause prescribe folic acid, 1—5 mg once a day,
which include food poisoning caused
him health problems. Modifying your routinely, but a normal balanced diet
by salmonella infection. Chicken and
cultural and religious practice is a part of will contain sufficient folic acid and daily
eggs can be infected with salmonella.
staying healthy. supplements are generally not required
It is important to cook these and other
foods thoroughly. Before your child reaches the age when in the UK.
he is expected to start fasting, it may Tonics containing iron or iron tablets
Salmonella can lead to a bone infection
be helpful to arrange a meeting with should not be given. Your child is anaemic
called osteomyelitis (see page 48).
your religious leader and nurse specialist because the sickle red blood cells are more
It is important to thoroughly defrost or doctor so that you can discuss fragile and do not live as long as the usual
frozen food before cooking and to make together your child’s specific health and red blood cells. He does not have the sort
sure chilled foods from the supermarket religious needs. of anaemia caused by insufficient iron in
22 23What is Sickle Cell Disease?
the diet. If he does need iron the doctor that eggs and chicken are properly cooked. Extremes of cold and heat own level of tolerance and to take part in
will tell you and will prescribe the right All children should take advantage of (temperatures) normal activities with other children.
amount for your child’s specific needs. the routine childhood immunisation Excessive chilling of the skin may trigger
programme, which will protect them from
If you are giving your child any traditional,
whooping cough, meningitis, haemophilus
a painful episode, for example swimming Common ailments –
herbal or complementary medicines do in very cold water or getting wet from
remember to tell his hospital doctor
influenza, mumps, measles and German rain water. When in the house your child effect on children with
because it may be important to consider
measles as well as the less common ones:
polio, diphtheria and tetanus.
should not be overdressed and the heating sickle cell disease
this when prescribing other treatments should not be too high as there is then
Most of the health problems affecting your
for your child. It is also advisable for your child to be the risk that your child may get too hot
child with sickle cell disease will probably
immunised against influenza (flu) every and sweaty causing him to lose fluid and
be common things which can affect
year. If he is travelling, it is important to his skin become chilled. Make sure he
any child, including those who do not
consider whether he needs any special has sufficient outer layers when he goes
Children should be medications, for example, anti-malaria outside if it is cold or windy. Chilling quite
have sickle cell disease. These problems
will usually get better quickly without
encouraged to find drugs (see page 35). commonly occurs after swimming, and
any complications, but occasionally
their own level of your child should dry off and get dressed
sickle cell disease can make things a
Adequate fluids as quickly as possible. If the swimming
tolerance and to take It is important that your child drinks pool water is cold, he should be advised
bit more complicated. These common
illnesses include:
part in normal activities enough to maintain a steady fluid balance. not to swim. It is important to discuss this
with other children. In sickle cell disease the kidneys are not with your child’s school so that they are
Coughs and colds (upper
able to concentrate urine and so he will aware of the importance of this advice and
the reason behind it. respiratory infections)
pass large quantities of dilute urine.
Avoiding things which may trigger All children get lots of coughs and colds,
When your child is well, he will probably Stress and anxiety particularly in winter and when they first
an illness
drink enough to make up for this loss in Stress and anxiety can affect the body. go to nursery or school. In general these
Infection the urine but if he becomes unwell, for A certain amount of anxiety can be helpful should not cause complications related to
Infection is an important trigger of sickle example with a fever or with diarrhoea because it motivates us to perform, but too sickle cell disease, and your child should
illness, but it may be difficult to avoid some and vomiting, he needs to drink more to much can trigger a sickle cell pain episode recover in a week or so. It is important
of the common viral infections such as avoid dehydration (see page 42 for how and this should be avoided. If your child is your child is kept warm and that he is
coughs and colds. Children with sickle cell to manage fever). Insufficient water in the feeling stressed by school, or if his illness or given plenty to drink. Paracetamol is
disease are more prone to certain bacterial body (dehydration) can trigger a sickle cell something else is worrying him, it may be helpful if your child has a fever or feels
infections because their spleen does not pain episode. Plain water or diluted juice worth discussing this with your specialist unwell. He should continue to take his
work properly. One of the most common should be encouraged and fizzy drinks nurse, doctor, social worker or psychologist. penicillin as usual, but extra antibiotics are
is pneumococcal infection which can avoided because these may cause stomach not usually needed because most coughs
be avoided by taking the recommended pain in some children. It is not necessary Physical exertion and colds are caused by viral infections
penicillin twice daily and having regular to force your child to drink more than he Physical activity can reduce stress, so and antibiotics do not help. Occasionally,
pneumococcal immunisations (see page wants when he is well and there is no on the whole it should be encouraged. a cough or cold might lead on to acute
29). Salmonella infection can be avoided by evidence that it makes the yellowness Children with sickle cell disease may find pain from sickle cell disease, and giving
re-heating food thoroughly and ensuring in his eyes (jaundice) any better. competitive sports more difficult because of paracetamol and ibuprofen should help.
their anaemia, which may lead to fatigue. If the pain becomes very severe, admission
Children should be encouraged to find their to hospital may be needed.
24 25What is Sickle Cell Disease?
Influenza (flu) and Covid-19 Vaccination will become very important to Very rarely, sickle cell disease can damage Immunisations and
prevent and control the virus long-term. the blood vessels in the head and cause
Influenza is a severe viral infection which is
commonest in winter and sometimes occurs severe headaches. Most normal headaches preventative medications
in big outbreaks across the world, called Diarrhoea and vomiting should be managed at home with Penicillin
pandemics. Symptoms include high fevers, paracetamol, plenty of fluids and rest. Try
Children often get gastroenteritis, which Making sure your child has penicillin twice
muscle aches and pains, shaking (‘rigors’), to identify if there is an underlying cause
is usually due to viral infections such a day is one of the most important things
coughing and sickness. It is sometimes hard such as constipation or problems in school.
as norovirus and rotavirus. This usually that you can do for your child. Children
to know whether symptoms are due to flu improves in a few days and antibiotics do If headaches occur once a week or more, with sickle cell disease are 600 times more
or a different viral infection, but initially not help, but your child should continue you should discuss this with your GP or likely to get pneumococcal infection than
children should stay at home, drink plenty the recommended daily penicillin. It is sickle cell doctor. If your child has a very other children. This is because the spleen
of fluid and continue their penicillin. In important for your child to drink plenty sudden or severe headache or has any does not work properly in a person with
up to half of cases of actual influenza a of fluids and oral rehydration fluids difficulty speaking or moving, you should sickle cell disease.
significant sickle complication may develop, may be helpful (Dioralyte, Electrolade, seek urgent medical advice from your
including acute chest complications, severe The spleen is an important part of the
World Health Organisation (WHO) Oral nearest hospital Accident & Emergency
pain and anaemia. body’s defense against infection.
Rehydration Salts). If the vomiting is very (A&E) department.
If your child seems very unwell, then severe and your child is unable to keep Pneumococcal infection may cause
they may need admitting to hospital and fluids down, admission to hospital will be Rashes pneumonia or meningitis. The symptoms
treating with anti-viral medicines (such as needed for intravenous fluids (a drip) to be can develop rapidly, making your child very
Rashes are not usually due to sickle
Tamiflu), strong antibiotics and sometimes given to prevent dehydration. ill very quickly, even before you have time
cell disease. Common causes of rashes
blood transfusion. to get medical help, and this can be fatal.
in children include viral infections and
Urine infection You can reduce the risk of pneumococcus
Vaccination against influenza is allergies. In general you should see your
recommended each year (see page 29), Urine infections are more common in GP if you are concerned.
and you should normally be contacted by children with sickle cell disease, particularly
in girls. Symptoms include burning and Asthma
your GP about this in autumn. If your child
stinging on passing urine and needing to
Making sure your child
does not get invited for the vaccination
contact your GP surgery. go frequently. It is important to see your
Asthma is common among all children
and it is not caused by sickle cell disease.
has penicillin twice a
doctor, who can test the urine and give
It is important to treat asthma in the usual day is one of the most
Covid-19 is a severe viral infection which antibiotics to treat the infection. If your
emerged in late 2019 and caused a global child gets several urine infections, further
way, with inhalers and sometimes with important things you can
pandemic. At the time of writing this tests may be useful to check the kidneys
oral medicines. Sometimes asthma attacks do for your child.
book we are still learning more about how cause acute problems in sickle cell disease
and bladder.
Covid-19 affects people with sickle cell and asthma may increase the risk of sickle
disease, but it seems that children usually complications, so it is important to see your
Headaches GP or practice nurse for advice about the best by ensuring you child takes penicillin syrup
have mild symptoms and complications
are no more common than for influenza. Headaches are common in children possible treatment for your child’s asthma. or tablets twice daily as recommended.
It is important to follow official advice and are often caused by tiredness, If your child is allergic to penicillin then
whilst the pandemic continues, particularly stress, dehydration, constipation or viral another antibiotic, usually erythromycin,
regarding the need to wash hands infections. Sickle cell disease can also cause may be prescribed instead.
carefully and to stay at home as necessary. headaches due to sickling in the skull but
this is uncommon.
26 27What is Sickle Cell Disease?
For the penicillin to be effective it must lt is strongly recommended that penicillin sure about the timing, check the book Hepatitis B
be taken twice every day at around the is given throughout childhood and carried and ask your health visitor. There is no Your child will probably have a blood test
same time. Make sure you do not run out on into adulthood. It is probably better reason why a child with sickle cell should in the outpatient department to check
of supplies. If your child is unwell and has to use penicillin in tablets rather than not have any of the routine childhood whether he has been in contact with
been put on another antibiotic by your syrup. This is because tablets can be kept immunisations. In fact it is perhaps even hepatitis. Hepatitis B is occasionally passed
GP or the hospital, check whether you at home for a longer time and because more important that your child should from mother to baby in the womb. In the
need to stop the penicillin and remember most syrup medications contain sugar, be fully protected because children with UK babies are now offered this vaccination
to start it again once the other prescribed which is harmful to teeth. However it is sickle cell disease are more susceptible to as part of the national routine childhood
antibiotic is finished. Penicillin should now possible to obtain sugar free penicillin infections and infections can trigger sickle immunisation programme. However it
be continued if your child is admitted from your pharmacist. Whilst your child is cell complications. may need to be given to children who
to hospital unless other antibiotics have still young you can give tablets by crushing have recently moved to the UK and were
been prescribed, as mentioned above. them with a spoon and mixing the powder Other immunisations not given it in their country of origin. Very
Taking regular penicillin does not weaken with a little unsweetened fruit juice to occasionally hepatitis B can be passed on
the body in any way. Resistance of the make it pleasant to take. Pneumovax
through a blood transfusion, but the blood
pneumococcus to penicillin is not a Pneumovax gives protection against more transfusion services in the UK are extremely
problem in the UK, although it has been Routine childhood immunisations of the pneumococcal types that cause careful and screen all blood donors for
reported in other countries. Penicillin infection than the routine PCV vaccine. hepatitis B (see page 55). If your child
Your child should receive all the same
taken regularly has been shown to protect This vaccine is given at around two years should need regular blood transfusions for
childhood immunisations recommended
against pneumococcal infection. The dose of age and then every 5 years thereafter any reason and has not already received a
for every child in the UK. These
of penicillin is as follows even throughout adulthood; it is given course of immunisations, his doctor may
immunisations include: diphtheria,
routinely to all children with sickle cell advise that a course should be given.
The dose of penicillin is as follows: whooping cough, tetanus (DPT), polio,
disease and your GP surgery or hospital
- 62.5mg twice a day until 1 year of age; haemophilus influenza (Hib), PCV
specialist doctor will prescribe and give it. Influenza (flu)
(conjugate pneumococcal vaccine),
- 125mg twice a day from 1 until meningitis C and measles, mumps and PCV and Pneumovax give protection The flu virus causes an infection which
5 years of age; rubella (MMR) and Hepatitis B. These against pneumococcal infection but it is may lead to respiratory problems that
are fully explained in the parent-held important that your child continues to take can be serious in children with sickle cell
- 250mg twice a day from
record (or baby book). If you are not penicillin as well. disease. Your specialist doctor will advise
5 years onwards.
and recommend that your child should be
ACWY given the flu vaccine by your GP, from the
This gives protection against first autumn after your child is 6 months
Figure 4 Medicine being poured
Follow the instructions for giving any meningococcus types A and C, which old and then once a year thereafter.
medication, you can ask your doctor, cause meningitis. Even if your child has
nurse or pharmacist for advice. had the Men C vaccine, which protects
against meningococcus type C, if you
Your child should have
are travelling to some parts the world, the same immunisations
e.g. Africa and Asia, he should also as other children. It is also
have ACWY as it will protect against advisable to ask your GP
meningitis type A.
to give your child the flu
vaccine each autumn.
28 29Management
and
treatment
Management and treatment
As you learn more about
sickle cell disease you will
find that you become more Managing your child when away from home.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Visiting the hospital outpatient clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
knowledgeable on how to Managing an illness at home.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
manage many aspects of the Some medical problems.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
illness at home and when to Medical emergencies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
seek medical help. What to expect if your child is admitted to hospital. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Blood transfusion.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
Developments in the management of sickle cell disease.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Medical tests and what they mean. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
30 31You can also read