5 STRUCTURALLY RELATED MOLECULES OF HUMAN CHORIONIC GONADOTROPIN (hCG) IN GESTATIONAL TROPHOBLASTIC DISEASES
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
5
STRUCTURALLY RELATED MOLECULES OF
HUMAN CHORIONIC GONADOTROPIN (hCG) IN
GESTATIONAL TROPHOBLASTIC DISEASES
Laurence A Cole
5.1 INTRODUCTION
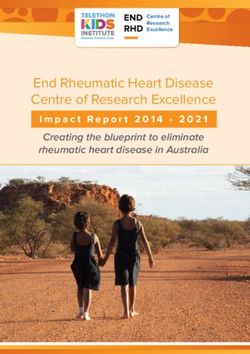
Human chorionic gonadotropin (hCG) is a glycoprotein hormone
composed of two dissimilar subunits, a- and b-subunit, held together by
charge and hydrophobic interactions. hCG comprises an a-subunit of 92
amino acids and a ß-subunit of 145 amino acids (Figs. 5.1 an 5.2). hCG
is an extraordinary glycoprotein with 8 sugar side chains (Figs. 5.1 and
5.2).
The sugar side chains account for 25% (pregnancy hCG) to 40%
(choriocarcinoma hyperglycosylated hCG) of the composition or
molecular weight of hCG (36,000 to 40,000). The combination of free
and degraded subunits and different N-linked and O-linked
oligosaccharide side chains causes significant heterogeneity in hCG
structure. hCG, free subunits, degraded molecules, molecules with
hyperglycosylated N- and O-linked oligosaccharide side chains, and
fragments are present in serum, urine and other bodily fluids. They are
detected in all pregnant women, in all women with trophoblastic
diseases, in all men with testicular germ cell malignancies and in men
and women with a proportion of non-trophoblastic neoplasms.
Figure 5.1. Amino acid sequence of hCG ß-subunit and sites of attachment of N- and
O-linked oligosaccharides.
Figure 5.2. Amino acid sequence of hCG α-subunit and sites of attachment of N-linked
oligosaccharides
148Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Figure 5.3. Principal structures of O-linked oligosaccharides attached to regular
hCG and its variants. GlcNAc is N-acetylglucosamine, GalNAc is N-
acetylgalactosamine, Man is mannose, Gal is galactose and SA is sialic acid.
In addition to regular hCG, 4 major structural variants are commonly
detected in serum samples: hCG free ß-subunit; nicked hCG; hCG
missing the b-subunit C-terminal peptide, and hyperglycosylated hCG.
Many other variants (i.e. nicked free ß-subunit, hyperglycosylated free
b-subunit, free ß-subunit missing the b-subunit C-terminal peptide,
nicked free ß-subunit missing the ß-subunit C-terminal peptide) are less
commonly detected in serum samples. The same large mixture of
molecule plus the terminal degradation product, b-core fragment, are
detected in urine samples. Table 1 summarizes the structure of the key
hCG-related molecules. These vary in size from a molecular weight of
9,500 (b-core fragment) to approximately 40,000 (hyperglycosylated
hCG).
Table 5.1. Structure of hCG-related molecules detected, to different extents, by commercial
hCG immunoassays in serum and urine samples (1-9).
hCG-related molecule Structure
Regular hCG α-subunit with 92 and β-subunit with 145 amino acid residue
(MW ~36,000) polypeptide
Mono- and biantennary N-linked oligosaccharides
Mostly trisaccharide O-linked oligosaccharides
Hyperglycosylated hCG 1 α-subunit with 92 and β-subunit with 145 amino acid residue
(MW ~40,000) polypeptide
Predominance of larger triantennary N-linked on β-subunit, and
N-linked with extra fucose on α-subunit
Mostly hexasaccharide O-linked oligosaccharides
Nicked hCG 1 α-subunit with 92 and β-subunit with 145 amino acids residues.
(MW ~36,500) β-subunit polypeptide nicked/cut at β47-48, β43-44 or β44-45
Mono- and biantennary N-linked oligosaccharides
Mostly trisaccharide O-linked oligosaccharides
hCG missing β-subunit α-subunit with 92 and β-subunit with 92-122 amino acids (C-terminal
C-terminal peptide 1 peptide determinant, β93-145 all or partly missing).
(MW ~29,000) β-subunit polypeptide also nicked at β47-48, β43-44 or β44-45
Mono- and biantennary N-linked oligosaccharides
No O-linked oligosaccharides
Free β-subunit 1 Only β-subunit present, no α-subunit
(MW ~22,000) Biantennary N-linked oligosaccharides
Mostly trisaccharide O-linked oligosaccharides
Urine β-core fragment Degraded β-subunit present (2 peptides, β6-40 and β55-92, held
(MW ~9,500) together by disulfide linkages), no α-subunit
Degraded biantennary oligosaccharide present
No O-linked oligosaccharides
1 Combinations of modification are present in serum and urine, such as hyperglycosylated nicked hCG,
hyperglycosylated hCG missing the β-subunit C-terminal peptide, nicked free β-subunit, hyperglycosylated free β-
subunit, nicked-hyperglycosylated free β-subunit and free β-subunit missing the C-terminal peptide.
149Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Over 40 different professional laboratory serum hCG tests are sold in
the USA for quantifying serum hCG. These and many other tests
may also be used to qualitatively assess urine hCG (i.e. positive test
when urine concentration >20 IU/L). Almost all of these tests work
through the contemporary multi-antibody “sandwich assay” method
permitting sensitive labeled-enzyme, isotope, fluorimetric or
chemilumenescent detection. Few if any assays are sold today using
the old competitive radioimmunoassay (RIA) method which was
developed in the nineteen fifties and has largely been displaced. Here
we review the commonly used hCG tests and their utility for
managing gestational trophoblastic disease cases.
All hCG tests use at least one antibody directed against the b-
subunit. This has led to the commonly used term “βhCG test.” Some
tests detect hCG only and are called intact hCG, or simply hCG tests.
Other tests detect hCG and invariable detect hyperglycosylated hCG,
free b-subunit and possibly the hCG degradation products. These
tests are called total hCG tests, bhCG tests, or again can just be
called hCG tests. The names are confusing. For the purpose of this
publication we will refer to them all as hCG tests.
All modern professional laboratory hCG tests use a combination of
antibodies to different sites on hCG (Table 5.1). Commonly, tests
use an antibody to one site on the core of the b-subunit. A second
antibody is then directed to an alternate site on the core of the b-
subunit, on the b-subunit C-terminal peptide, on the hCG dimer or
subunit interface, on free subunits, or on the a-subunit. Because of
these variations in antibody combination, different commercial hCG
tests may measure very different mixtures of hCG-related molecules.
Some tests may detect hCG only while others may detect all major
hCG-related molecules. This may not be a problem for monitoring
pregnancy in serum samples, 7 weeks of gestation until term, since
regular hCG is consistently the principal molecule present (Table
5.2). It may, however, be a major problem in monitoring patients
with trophoblastic diseases and non-trophoblastic malignancies. In
such cases, different hCG variants may be the principal molecule
present (Table 5.2). These limitations with hCG tests are carefully
investigated in this review.
150Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Table 5.2
This article considers all aspects of hCG detection in trophoblastic
diseases. It examines the problems of false positive hCG results. It
describes how to avoid false positive hCG results. The experience of
the USA hCG Reference service is also presented: problems found
with the sensitivity of specific hCG tests; confusing hCG results due
to false positive or phantom hCG results; the complications of
“quiescent gestational trophoblastic disease” and confusing hCG
results due to pituitary hCG.” All of these issues are carefully
investigated here.
Hyperglycosylated hCG is considered here. As shown by multiple
authors, hyperglycosylated hCG is a variant of hCG with completely
independent biological functions to regular hCG. Hyperglycosylated
hCG appears to be the autocrine promoter of growth and malignancy
in gestational trophoblastic neoplasms and persistent mole. The
pathophysiology of hyperglycosylated hCG as an independent
molecule to regular hCG is carefully considered. The role
hyperglycosylated hCG has in the biology of gestational
trophoblastic diseases and the use of hyperglycosylated hCG as a test
in the management of gestational trophoblastic diseases are
considered as are the parallel evolutions of hyperglycosylated hCG
and gestational trophoblastic neoplasia.
Finally, the use of hCG free ß-subunit measurements is examined.
Use has been indicated in the differential diagnosis of placental site
trophoblastic tumor. The differential diagnosis of women presenting
with persistent low levels of hCG is considered. Examination of the
differentiation of false positive hCG, quiescent gestational
trophoblastic disease, pituitary hCG, and placental site trophoblastic
tumor are all appropriately considered.
151Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
5.2 PATHOPHYSIOLOGY OF hCG AND RELATED
MOLECULES
The hCG found through most of pregnancy, regular hCG, has 4
O-linked oligosaccharides on the ß-subunit (Fig. 5.1). These are
primarily of the trisaccharide type (Fig. 5.3). Regular hCG has 4 N-
linked oligosaccharides, 2 on the α-subunit and 2 on the ß-subunit
(Figs. 5.1 and 5.2). These are mixtures of monoantennary (8 sugar
residues) and biantennary (11 sugar residues) structures (Fig. 5.4) (1-
3). In choriocarcinoma, gestational trophoblastic neoplasm and
persistent mole cases, the principal hCG form found is
hyperglycosylated hCG (1-3). While this has the same peptide
structure as regular hCG, it has varying proportion of larger N- and
O-oligosaccharide structures (Figs. 5.3 and 5.4) (1-3). The N-linked
oligosaccharides are fucosylated triantennary structures with 15
rather than 8-11 sugar residues, and the O-linked sugars are
hexasaccharide rather than trisaccharide structures. Effectively, the
sugar structures on hyperglycosylated hCG are double size sugar
structures, comprising as much as 40% of the molecular weight of
hCG (1-3).
Table 5.3
152Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Figure 5.4. Principal structures of N-linked oligosaccharides attached to regular
hCG and its variants. hCG-H. GlcNAc is N-acetylglucosamine, Man is mannose,
Gal is galactose and Fuc is fucose, and SA is sialic acid.
As published, regular hCG is made by the differentiated
syncytotrophoblast cells, while hyperglycosylated hCG is produced
only in the stem cytotrophoblast cells, the invasive trophoblast cells
(4,5). Clearly, only the invasive trophoblast cells produce
hyperglycosylated hCG. Hyperglycosylated hCG has minimal
regular hCG-like progesterone-promoting biological activity at the
hCG/LH receptor (4,6). The possibility that hyperglycosylated hCG
may have a separate biological role to regular hCG, possibly in
promoting the growth and invasive activity in the invasive
cytotrophoblast cells is considered.
Three model systems have been used for investigating the invasive
functions of hyperglycosylated hCG with malignant cytotrophoblast
cells. The first two were JAr and JEG-3 lines of choriocarcinoma
cells. The third system was NTERA testicular germ cell cancer cell
line. All 3 cytotrophoblast models produce exclusively
hyperglycosylated hCG (7). As shown by 3 independent groups using
these models (4,8-10), hyperglycosylated hCG (also called
choriocarcinoma hCG), but not regular hCG, directly modulates
cytotrophoblast cell growth, tumor formation and cytotrophoblast
cell invasion in vitro and in vivo. This was shown by a combination
of Matrigel cell culture invasion chamber studies in vitro, cell culture
153Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
growth studies in vitro , and confirmed by examining human
xenograph malignancies, athymic nude mice with transplanted
growing human choriocarcinoma cells in vivo (4,8-10). As found in
our laboratory, addition of monoclonal antibodies to
hyperglycosylated hCG completely inhibited the cell growth,
invasion and tumor formation in all models in vivo and in vitro,
preventing cytotrophoblast cell invasion, preventing cell growth and
blocking tumor growth and progression (4,8). Addition of pure
hyperglycosylated hCG, but not pure regular hCG, promoted both
growth and invasion (4,8). Similarly, addition of antisense DNA to
either hCG α-subunit or ß-subunit prevented all hCG production in
Jar choriocarcinoma cells (hyperglycosylated hCG is the only form
of hCG made by these cells), and similarly blocked invasion, cell
growth and tumorigenesis in similar models in vitro and in vivo
(9,10). Considering our published studies with monoclonal
antibodies to hyperglycosylated hCG (4,8), and these independent
reports with antisense DNA to hCG subunits in cells solely
producing hyperglycosylated hCG (9,10), it is concluded that
hyperglycosylated hCG secreted by cytotrophoblast cells, acts on
these same cells through an autocrine receptor on the same cells to
promote growth and invasion.
While syncytiotrophoblast regular hCG functions as an endocrine,
promoting progesterone production at a distant corpus luteal LH/hCG
receptor, hyperglycosylated hCG seemingly acts as an autocrine,
rather than endocrine, produced by cytotrophoblast cells and
attenuating cytotrophoblast cell growth and implantation.
Hyperglycosylated hCG is in multiple ways a distinct molecule from
regular hCG, it has a different molecular weight to regular hCG
(40,000 vs. 36,000), it is produced by separate cells (cytotrophoblast
vs. syncytotrophoblast), it is has an autocrine rather than an
endocrine action, and has a separate functions, promoting growth and
invasion and tumor formation. This is a unique situation, specific
genes coding for the α- the ß-subunit of regular hCG and
hyperglycosylated hCG (the polypeptide sequences are identical (4))
yielding two independent molecules. The same polypeptides forming
the common backbone of two very separate molecules, regular hCG
and hyperglycosylated hCG. It is concluded that secreted
hyperglycosylated hCG modulates the invasion and growth of
cytotrophoblast cells in choriocarcinoma and testicular germ cell
malignancies.
Multiple publications show that tumor growth factor beta (TGFß) is
the promoter of apoptosis in trophoblast cells (11,12). As shown,
TGFß directly inhibits invasiveness and proliferation in
choriocarcinoma cells and testicular germ cells. Absence of TGFß
and smad 3 consistently occurs in cytotrophoblast cells in
choriocarcinoma permitting growth and invasion. These findings
154Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
suggest that invasiveness and growth in choriocarcinoma malignancy
may be controlled through blockage to TGFß activity and apoptosis
(13,14). As reported, choriocarcinoma hCG or hyperglycosylated
hCG work by promoting cell invasion and growth, by blocking the
normally TGFß modulated apoptosis (10).
TGFß promotes apoptosis in all tissues. In promoting apoptosis it
blocks tissue invasion and proliferation. TGFß activity is limited or
absent in most cancers permitting growth and invasion. Malignancy
may be modulated by blockage of TGFß activity and apoptosis (over
4000 citations, references limited to recent reviews: 15,16). As
published, hyperglycosylated hCG also promotes cell invasion and
proliferation through blocking apoptosis in trophoblast cells (10), or
works by a TGFß receptor-like controlled apoptosis mechanism.
The ß-subunit of hCG has structural homology with TGFß. Both
the ß-subunit of hCG and TGFß (and platelet derived growth factor
and nerve growth factor) contain a exclusive cystine knot structure in
which multiple disulfide bridges uniquely link anti-parallel peptides
in the center of the molecule (17). A molecule the exact molecular
size of hyperglycosylated hCG, has been shown to bind the TGFß
receptor on choriocarcinoma cytotrophoblast cells (18). The binding
of hyperglycosylated hCG to the TGFß receptor is inferred by both
these molecular size studies and by obviousness (hyperglycosylated
hCG functions by blocking apoptosis in choriocarcinoma, TGFß-
regulates apoptosis and is absent in choriocarcinoma). It is inferred
that hyperglycosylated hCG acts in an autocrine manner on the TGFß
receptor, to antagonize TGFß action. In so doing it blocks apoptosis,
as demonstrated (10), permitting cell growth and invasion. Through
this pathway, cytotrophoblast hyperglycosylated hCG promotes
invasion and growth in choriocarcinoma.
As described above, blockage of hyperglycosylated hCG with a
monoclonal antibody to hyperglycosylated hCG in nude mice
xenograph cancer models, completely blocks human
choriocarcinoma growth and invasion or induces oncostasis (4,8). It
is inferred, that administration of human antibodies to
hyperglycosylated hCG or administration of a vaccine to
hyperglycosylated hCG to humans would perform similarly in
humans, blocking gestational trophoblastic neoplasm,
choriocarcinoma and testicular germ cell malignancy growth,
inducing oncostasis or effectively curing disease. Efforts have been
made to license this technology and manufacturers to produce human
antibodies for this purpose. There has been no interest because the
diseases are rare and they would not make enough money. A
company called CG Therapeutics Inc. in Seattle WA, is, however,
producing a vaccine, that should be very useful for treatment of
gestational trophoblastic disease and testicular germ cell
malignancies in the future.
155Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
5.3 PARALLEL EVOLUTION OF hCG AND GESTATIONAL
TROPHOBLASTIC NEOPLASIA
Humans are unique in that over 60% of the energy intake in utero
is used to support the developing brain’s nutritional needs, compared
with just 20% used by 4300 other mammalian species (19,20). For a
human to evolve there was a need for gestational mechanisms to
support such a nutritionally demanding nervous system (19, 20). An
ultra-deep hemochorial placental implantation mechanism evolved
with humans to accommodate this human fetal nutritional need.
Examining the evolution of hyperglycosylated CG, reveals that this
molecule is the signal for placental invasion in humans, whether as in
choriocarcinoma or at implantation as in pregnancy (4, 8). It also
reveals the parallelism between the molecular evolution of this
molecule and its biological activity and the evolution of the advanced
systems in primates and humans. The evolution of hyperglycosylated
CG appears to be at the root of the evolution of placental
implantation to accommodate nutritional needs for human brain
development.
It appears that the amount of nutritional support or supply of
energy in a species limits brain size and the development of the brain
throughout gestation (19,20). Brain size is therefore related to the
combination of body mass and the metabolic support of the
developing progeny (21). How then did humans evolve an
exceptionally large brain relative to body mass? They appear to have
evolved a unique very deeply implanted placental mechanism to
support the nutritional demands of the embryonic brain (Table 5.3).
Primates have a two-fold greater brain to body mass than other
mammals (22). At embryo implantation, cytotrophoblast cells of the
placenta invade more deeply into the endometrium permitting greater
vascular contact than occurs in other species (19-22). Uniquely in
humans, under influence of high acidity hyperglycosylated hCG,
cytotrophoblast cells invasion is deepest going to the inner third of
the myometrium and permitting hemochorial bleeding of spiral
arteries directly onto placental cells (19, 20, 23). This nutritionally
supports supports development a cranial capacity relative to body
mass that is three-fold greater than those of the most advanced
primates. Evolution of primates and, to a greater extent, humans is
marked by hemochorial placentation, deeper placental invasion,
which thus provides the nutrients for brain development (Table 5.3).
We ask, what are the mechanisms that have evolved in primates and
humans that initiated this sequentially deeper invasion at
implantation?
CG is part of a family of hormones that includes luteinizing
hormone (LH). These hormones are the glycoproteins hormones that
share a common α-subunit coded by a single gene, and a separate ß-
156Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
subunit which dictates hormone function (24,25). Fiddes et al., 1980
(24) examined the DNA sequence for the ß-subunits of CG and LH
and showed evolution of CG from LH in primates by a single
deletion mutation in LH DNA and read-through into the 3’-
untranslated region. Maston et al., 2002 (25) examined the DNA
sequences of the ß-subunit of 14 primates and showed that CG was
not present in prosimians the more primitive primates, but evolved
with anthropoid primates. Frequent gene and sequence changes have
occurred in the sequence of the CG ß-subunit with the evolution of
anthropoid primates to catarrhine primates (orangutan and baboon)
and hominids (25).
The acidity of CG and LH in species affects their circulating half
times and thus their serum concentrations and therefore their
biopotency. Human CG has 4 O-linked oligosaccharides, all on its ß-
subunit. These acidify it resulting in a molecule with a mean
isoelectric point (pI) of 3.5, and a circulating half time of 2400
minutes (26). Human LH, by comparison, has no O-linked
oligosaccharides, a pI of 8.0 and circulating half time of just 25
minutes. As such, CG circulates for approximately 100 times longer
than hLH and is therefore approximately 100-fold more biologically
active than LH.
LH was the only progesterone promoting gonadotropin produced
by early primates and other species (25). The rapid circulating half-
time of LH very much limited its serum circulating concentration or
biological activity.
The earliest CG in anthropoid primates had 2 O-linked
oligosaccharides on the ß-subunit at serine residues 121 and 132
(25). This had a mean isoelectric point of 6.25 (Table 3). As a result
of a point mutation at residue 127 (Asn→Ser), the more advanced
catarrhine primates evolved further with 3 O-linked oligosaccharides
(25,27). Then with the evolution of the hominoid ancestor, a point
mutation occurred at residue 138 (Ala→Ser) and molecules were
developed with 4 O-linked oligosaccharides (25). The 4 O-linked
oligosaccharide molecule was the most acidic CG (26). The
sequentially increasing circulating half-time of LH and then CG with
0, 2, 3 and 4 O-linked oligosaccharides (pI 8, pI 6.3, pI 4.9 and pI
3,5, respectively) with primitive species, anthropoid primates,
catarrhine primates and then hominoid ancestors was associated with
sequentially increasing serum concentrations or biological activities
over the 100-fold range. As discussed in this article,
hyperglycosylated CG is the cytotrophoblast cell or the stem placenta
cell glycosylation variant of CG. The hyperglycosylated CG made by
cytotrophoblast cells and regular CG made by syncytiotrophoblast
cells status seemingly occurred with all primates. As such
hyperglycosylated hCG evolved with increasing numbers of O-linked
oligosaccharides parallel to the evolution of regular hCG.
157Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Hyperglycosylated CG therefore evolved with anthropoid primates
and exponentially increasing serum concentrations of
hyperglycosylated CG with the evolution of species with molecules
containing 2, 3 and 4 O-linked oligosaccharides respectively, leading
to greater and greater acidity or biological activity which correlated
with deeper and deeper implantation (Table 5.3).
As discussed in this article, CG-H has separate biological functions
to CG in cytotrophoblast invasion. It is associated with
cytotrophoblast growth and invasion through a TGFß - apoptosis
mechanism. Hyperglycosylated CG with 2 O-linked oligosaccharides
seemingly was expressed initially in anthropoid primates, this led to
minimal invasion at implantation. Hyperglycosylated CG was then
raised in concentration and biological activity with addition of a
further O-linked oligosaccharides with the evolution of advanced
catarrhine primates leading to deeper implantation (Table 5.3). It was
raised further in activity with the addition of a one more O-linked
oligosaccharide with the evolution of hominoid ancestors leading to
the ultra deep implantation seen in humans.
The hyperglycosylated hCG-associated evolution model may be
optimal for nutrition and brain development in human but clearly
comes with complications. As published, hyperglycosylated hCG is
critical for appropriate implantation in humans, insufficient
hyperglycosylated hCG leads to miscarriages (28). The incidence of
pregnancy failures (miscarriages and early pregnancy losses) is much
higher in humans (40%) than in rodents (10%) and all other species
(10%). Furthermore, human placentas harbor hyperglycosylated
hCG, an invasion-promoter critical for the super-implantation needed
for human placentation to support the nutrition for brain
development. As a complication of humans having this invasion
promoting molecule, humans uniquely develop persistent mole,
gestational trophoblastic neoplasm or choriocarcinoma.
It is hypothesised that there is an evolutionary connection between
the nutritional requirements for brain development in humans,
placental invasion and implantation, advances in the development
and glycosylation of hyperglycosylated CG, and the development of
neoplastic gestational trophoblastic disease in humans.
5.4 SELECTING AN APPROPRIATE HCG TEST FOR
TUMOR MARKER APPLICATIONS AND FOR
MONITORING PATIENTS WITH GESTATIONAL
TROPHOBLASTIC DISEASES
In the USA, all professional laboratory and point of care hCG tests
are approved by the Food and Drug Administration for serum
pregnancy testing only. All tests provide assistance in their
158Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
information leaflet and guidance values for pregnancy testing only.
Most test manufacturers recommend that the use of the test be
confined to pregnancy testing. Currently, however, only about 65%
of laboratory hCG testing is for pregnancy detection, approximately
20% is for Down syndrome screening (triple and quadruple screen
protocols) and 15% is for trophoblastic diseases and cancer
applications. The proportion of tests for trophoblastic diseases and
cancer applications is quite high because the average pregnant
women has only two hCG tests, one to confirm pregnancy and one
for Down syndrome screening. In contrast, the person with
trophoblastic disease has as many as 80 or more hCG tests during
multi-year monitoring. There is clearly a need for manufacturer’s to
consider these “off label” applications, and to verify and certify use
for serum and urine trophoblast disease management and other
common applications.
As described earlier in this review, hyperglycosylated hCG is the
principal form of hCG produced in active
choriocarcinoma/gestational trophoblastic neoplasm cases, hCG free
ß-subunit is the principal hCG variant made in PSTT and non-
trophoblastic neoplasms. Yet very few manufacturers, however, have
calibrated their so called “total hCG” tests for equally detecting
regular hCG, hyperglycosylated hCG and free ß-subunit (76). This is
in part due to a lack of availability from WHO of a
hyperglycosylated hCG standard. The FDA in the USA only requires
calibration against the molecule called hCG or regular hCG (41, 76).
Hyperglycosylated hCG is the predominant form of hCG produced
in the three weeks following implantation in pregnancy (Table 5.1.
During the first, second, third and subsequent weeks after
implantation, hyperglycosylated hCG is gradually replaced with
hCG; hyperglycosylated hCG accounting for >80%, 63%, 50% and
25 toStructurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Table 5.4
Circulating hCG (from hydatidiform mole) and hyperglycosylated
hCG (from invasive trophoblast disease or choriocarcinoma)
commonly becomes nicked as levels diminish after therapy (Table
5.2) (5,6). hCG and hyperglycosylated hCG are nicked or cleaved at
ß43-44, ß44-45 or ß47-48. This is a major a-subunit:ß-subunit
hydrophobic and charge interaction or linkage point. As such,
nicking leads to rapid dissociation of molecules (1), releasing the
nicked free ß-subunit (34). In trophoblastic disease cases, when hCG
values fall below 100 mIU/ml, nicked hCG and free ß-subunit often
become the major or even sole sources of hCG immunoreactivity in
serum (Table 5.2) (35,36). Cases have been reported in which a
recurrence of invasive disease has been completely missed by use of
an assay that does not detect nicked hCG (Table 5.4) (35). False
negative results have also been observed using assays that do not
detect free ß-subunit or nicked hCG. It appears that measurement of
these molecules is essential for accurately monitoring hCG levels
until they become undetectable, or reach background (Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
In two independent studies we have observed nicked hCG missing
the ß-subunit C-terminal peptide in trophoblast disease patient serum
(32, 37). As shown in Table 5.4, only one of 11 tests appropriately
detects nicked hCG missing the ß-subunit C-terminal peptide. In a
recent study, 5 of 76 cases of complete mole and choriocarcinoma
were shown to have significantly lower hCG values when tested with
any one of 9 tests requiring the ß-subunit C-terminal peptide to be
present (32). As found, 6 of 86 gestational trophoblastic disease cases
(about 1 in 14) required detection of hCG missing ß-subunit C-
terminal for meaningful management of trophoblastic disease.
Multiple blind studies with no financial or commercial bias have
been completed by the USA hCG Reference Service to investigate
abilities of common commercial immunoassays to detect the
different hCG-related molecules associated with trophoblastic
diseases and cancers (32,41,76). As found, the Siemens Immulite
hCG test is the only one that efficiently detects all of the hCG variant
antigens in serum samples on an equimolar basis (Table 5.4). This is
clearly the only appropriate test for management of cases with
gestational trophoblastic disease and non-trophoblastic malignancies.
All other tests either inappropriately failed to detect molecules
missing the ß-subunit CTP, or failed to appropriately detect
hyperglycosylated hCG, free ß-subunit or other molecules critical to
gestational trophoblastic disease and cancer detection (Table 5.4).
Centers managing gestational trophoblastic disease cases need to
change to the Siemens Immulite test. We also blindly investigated
the Charing Cross RIA (Table 5.4). This is the test used by the
Charing Cross Gestational Trophoblastic Disease Center. This center
has been at the root of many discoveries regarding gestational
trophoblastic disease management and they have claimed that their
RIA is the best assay alternative for them. As found in blind studies
(Table 5.4), this RIA test inappropriately detects hCG free ß-subunit,
nicked hCG missing the ß-subunit C-terminal peptide and urine ß-
core fragment (32,41). Furthermore, as described later in this review,
this type of assay has clear problems with false positive hCG results
(41).
Blind studies were also carried out examining the abilities of
different assay to appropriately detect 76 cases of gestational
trophoblastic disease. As shown in Table 5.5, the Siemens Immulite
assay once again proved to be the best test, with only 6 of 76 results
varying from the median test result for 8 assays by more than 25%.
By far the poorest results (72 of 76 values varying from the median
result by more than 25%) were observed with the Charing Cross RIA
(Table 5.5).
161Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Table 5.5
It is concluded that hCG-related molecules may vary greatly in
structure and size. In cases of trophoblast disease or non-
trophoblastic malignancies, any one of the variants may constitute
the sole form of hCG in serum or urine samples. It is important to
talk with your laboratory and make sure that they are using an
appropriate test which detects all the pertinent hCG-related
molecules, before submitting samples for monitoring patients with
trophoblastic diseases or other malignancies, or before making
important decisions from the results. Based on blind and non-biased
studies the Siemens Immulite is seemingly the only appropriate test
for this purpose.
5.4.1 THE EXPERIENCE OF THE USA HCG REFERENCE
SERVICE
The USA hCG Reference Service was started in January 1998 in
response to repeated requests from physicians for help with
confusing or inconsistent hCG results (28, 33, 42). It is a consulting
service that investigates patient medical history, laboratory hCG
records, and brands and versions of hCG tests used. It also
independently measures in a single test concentrations of all common
hCG-related molecules listed in Table 5.1 (Siemens Immulite hCG
test), and regular hCG only, nicked hCG only, hyperglycosylated
hCG only, free b-subunit only, and b-core fragment only in parallel
serum and urine samples provided by patients (28, 33, 42). Dilution
parallelism is investigated (1X value in undiluted sample and 1/3rd
and 1/10th of the value in 3-fold and 10-fold diluted sample), as is the
affect of HBT (Scantibodies Inc.), a heterophilic antibody/interfering
substance blocking agent on all assay results (28,33, 42). A clinical
records report is prepared for the physician on the nature of the hCG
detected by the clinical laboratory, on the most likely source of the
immunoreactivity (malignant gestational trophoblastic neoplasm,
placental site trophoblastic disease, pituitary hCG, non-trophoblastic
neoplasm, or false positive hCG) and on the suggested management
of the case.
162Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
The USA hCG Reference Service is United States Department of
Health and Human Services CLIA certified for preparing data/reports
for inclusion in patient records (CLIA ID# 32D0972561). The USA
hCG Reference Service is monitored for consistency in results by the
College of American pathologist. While called the USA Service,
they consult on approximately 70 cases from throughout the USA
and 20 cases from around the world (from Europe, Middle East,
South America, South-east Asia) each year. In seven years there have
been over 500 patient referrals to the USA hCG Reference Service
for various reasons. Commonly the USA hCG Reference Service
data confirms physician’s diagnoses of gestational trophoblastic
diseases, persistent mole, ectopic pregnancy, placental site
trophoblastic disease, testicular choriocarcinoma, or ovarian germ
cell or other non-trophoblastic neoplasms. The USA hCG Reference
Service also discusses and advises on a large number of cases of
gestational trophoblastic disease on the telephone (over 500 further
cases), making recommendations or suggesting tests that can be
carried out in the patient’s locality. In addition the web site
(www.hcglab.com) attracts approximately 200 e-mails from patients
each year. Questions about hCG results, pregnancy, trophoblast
disease and the soundness of the hCG test are addressed. Often
patient inquiries by e-mail lead to home urine hCG testing, and
sometimes to further outside hCG testing, physician involvement and
USA hCG Reference Service testing to determine the validity of hCG
results.
Of particular interest has been the observation of numerous cases
peri-menopause, post-menopause or following oophorectomy with
pituitary hCG. This is very commonly mistaken for gestational
trophoblastic neoplasm, or persistent malignancy if patient has no
history (42). A very large number of false positive or phantom hCG
cases have been identified, in which the patient received unnecessary
therapy for the diagnosis of gestational trophoblastic disease
(invasive/malignant disease or choriocarcinoma not confirmed by
pathology). Also of interest has been the observation of a significant
number of women producing low levels of normal pregnancy hCG
with no clear physical evidence of tumor or new or recurrent
trophoblastic disease, this is quiescent gestational trophoblastic
disease. The USA hCG Reference Service now uses the
hyperglycosylated hCG test to identify quiescent gestational
trophoblastic disease, and an hCG free ß-subunit test to identify
patients with placental site trophoblastic disease. Here we will
describe each one of these common findings of the USA hCG
Reference Service, false positive hCG, pituitary hCG, quiescent
gestational trophoblastic disease, placental site trophoblastic tumor.
We also describe how the USA hCG Reference Service distinguishes
each diagnosis.
163Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
5.4.2 FALSE POSITIVE hCG
In the first few months of operation of the USA hCG Reference
Service, 3 unusual cases were investigated for gestational
trophoblastic disease or choriocarcinoma (40). In all 3 cases the
woman had an incidental pregnancy test prior to surgery which was
positive. The positive hCG value persisted with small rises and
reductions in reported hCG results. Ultrasound, dilation and curettage
and laparoscopy ruled out pregnancy or ectopic pregnancy. The
diagnosis of gestational trophoblastic disease or choriocarcinoma
was made, even though there was no previous history of
trophoblastic disease or physical evidence of tumor. In two of the 3
cases chemotherapy was started, and in 1 case a hysterectomy was
carried out. All 3 cases were then referred to the emerging USA
hCG Reference Service (the need for the Service emerged from cases
like this). At that time the reported hCG concentrations were 17, 53,
110 IU/L, respectively. It was a surprise when false positive hCG
results were demonstrated in these individuals. The findings
indicated that the hCG test used by the physicians was detecting
interfering antibodies rather than hCG (40).
Now, after eight years of operation, and multiple publications on
the false positive hCG problem (37-40,42-44), over 400 women have
been referred to the USA hCG Reference Service for investigating
potential false positive hCG results. To date (October 2007) 91
women were shown to have had false positive hCG result. False
positive results are due to interfering antibodies in the patient’s
serum, whether human anti-animal antibodies gained from exposure
to animals or human heterophilic antibodies. Human heterophilic
antibodies are gained from immunoglobulin A deficiency disorder or
history of mononucleosis (42-45). The interfering antibodies, just
like hCG, can bridge the capture and tracer animal anti-hCG
antibodies used in the hCG assay. In our experience, false positive
hCG results can range from 2 to 1100 mIU/ml. We have never
observed a false positive case with erroneous levels exceeding 1100
mIU/ml (42-44).
False positive results were identified by the following criteria (42-
44):
1. The finding of more than 5-fold differences in serum hCG
results with alternative immunoassays.
2. The presence of hCG in serum and absence of detectable hCG
or hCG related molecule immunoreactivity in a parallel urine
sample (interfering antibodies are large glycoproteins. The do
not cross the glomerular basement membrane so do not
interfere with urine measurements).
3. The observation of false positive results in other tests for
164Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
molecules not normally present in serum, such as urine b-core
fragment.
4. The finding that a heterophilic antibody blocking agent
(Scantibodies Inc. HBR) prevented or limited false detection
(confirmatory criterion).
5. The finding that hCG results differ greatly when tested
undiluted, and diluted with serum.
Other laboratories around the world have also identified cases
having needless therapy due to false positive hCG results in modern
hCG tests (45-50). Many false positive hCG results were reported in
the nineteen eighties using the older RIA technology, and more
recently false positive results coming from very few testing by
centers still using the RIA technology today (41,51-53).
The USA hCG Reference Service has also investigated cases with
proven history of hydatidiform mole or choriocarcinoma with
recurrence of disease. In 6 cases the recurrence was all or in part due
to false positive hCG results. In 3 of these 6 cases chemotherapy or
surgery was needlessly carried out to treat a phantom or false
positive recurrence.
In the remaining 85 false positive cases observed by the USA hCG
Reference Service there was no history of trophoblastic disease and
no direct physical evidence of a tumor. Patients were investigated
and then treated according to protocol for a diagnosis of gestational
trophoblastic disease or choriocarcinoma. The history of each of the
85 false positive cases started with a positive incidental pregnancy
test. Seventy of the cases had dilation and curettage and/or
laparoscopy to exclude ectopic pregnancy. Fifty three received
needless single agent chemotherapy or underwent high risk
etoposide-based multi-agent chemotherapy. Nine had needless
hysterectomy and/or bilateral salpingo-oophorectomy; in addition
some had further major surgical procedures. Among the cases, false
hCG immunoreactivity (at the time of USA hCG Reference Service
consultation) ranged from 9 to 900 mIU/ml. Earlier false positive
values of up to 1,100 IU/L were recorded. It is our understanding that
in all cases after false positive hCG demonstration all treatment was
halted, even though physician’s laboratory test remained positive. It
is our experience that false positive results in a specific hCG assay
may remain false positive for 3 or more years. Women having false
positive hCG results can also have falsely elevated results in other
immunoassays. The history of a representative false positive hCG
case is outlined in Table 5.6.
165Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Table 5.6
In the experience of the USA hCG Reference Service, most false
positive hCG results have occurred in patients monitored by their
medical center’s laboratory using the Abbott AxSym hCG test, the
Siemens ACS180 and Siemens Centaur tests, by the Beckman
Access and Dade Dimension tests, and the Ortho Vitro test. No cases
referred to us were being monitored by their medical center using the
Siemens Immulite or Roche Elecsys tests, indicating that these tests
are less prone to false positive hCG test problems.
False positive hCG results in the USA hCG Reference Service
assay were prevented by pre-treatment of serum with the heterophilic
antibodies blocking agent HBR (54). Heterophilic antibodies are
bivalent human antibodies against other human antibodies, or against
animal-like antibodies. Human antibodies can cross species and bind
animal antibodies, like the mouse, rabbit, sheep and goat antibodies
used in hCG tests. These cross species, bivalent, antibodies are able
to act like hCG linking the capture and tracer antibodies. Their
presence in blood can cause persistent false positive hCG results. The
USA hCG Reference Service experience with HBR indicates that
circulating heterophilic antibodies in patient blood are the cause of
false positive results. The problem of human heterophilic antibodies
and human anti-animal immunoglobulins is well known by
commercial test manufacturers. Commonly, manufacturers add an
excess of non-specific antibodies or animal serum to samples to
avoid false positive results.
Many of the medical doctors that managed the 91 cases referred to
the USA hCG Reference Service, in which hCG was shown later to
be due to false positive hCG results, observed a transient decrease in
the hCG values in the time following chemotherapy or surgery. This
166Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
misled physicians by wrongly indicating presence of disease and
successful therapy of disease. The transient decrease may be due to
an interim weakening of the immune system as a result of
chemotherapy or surgery. This could reduce circulating antibody
concentration, leading to decreased false hCG results.
5.4.3 QUIESCENT GESTATIONAL TROPHOBLASTIC
DISEASE
Among other unexpected results recorded by the USA hCG
Reference Service are the finding of persistent low real (not false
positive) hCG values in women, lacking evidence for tumor, rising
hCG or any evidence of clinically active disease. These inactive
gestational trophoblastic disease cases are called quiescent
gestational trophoblastic disease cases (quiescent GTD). Quiescent
GTD was diagnosed in these cases by the observation of persistent
low levels of hCG (alwaysStructurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Table 5.7
Table 5.8
Quiescent GTD, in our experience, always follows a history of
choriocarcinoma/gestational trophoblastic disease, hydatidiform
mole or occasionally an ectopic pregnancy or spontaneous abortion.
A recent study by Sebire et al (54). indicates that all cases of
gestational trophoblastic neoplasm following an ectopic pregnancy or
spontaneous abortion are likely following an aborted or ectopic
hydatidiform mole, though confirmatory pathology is often lacking.
As such, the study by Sebire et al (54) confirms our observation that
all cases of quiescent GTD are limited to cases with gestational
trophoblastic disease.
168Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Hyperglycosylated hCG (hCG-H) testing aids in the diagnosis of
quiescent GTD and the early detection of active GTN or
choriocarcinoma. As discussed in a previous section of this review,
hyperglycosylated hCG is the promoter or driving force of
trophoblast cell growth and invasiveness or malignant disease. As
such it is no surprise that absence of hyperglycosylated hCG
production marks non-invasive non-propagating disease or quiescent
GTD. Choriocarcinoma and choriocarcinoma cell lines comprise
mainly invasive cytotrophoblast cells producing primarily the
hyperglycosylated form of hCG (1,4,8-10). hCG-H is the
predominant form of hCG in the circulation in invasive cases, GTN,
and choriocarcinoma (1, 33, 42), but is not prominent or is absent in
benign cases of hydatidiform mole or quiescent GTD. It is therefore
likely to be a useful marker of invasive trophoblast behavior. Here
we review the most recent publications on this possibility and
compare findings with other reports.
The recent papers by Cole, et al. demonstrates the usefulness of
total hCG and hyperglycosylated hCG in detecting active GTN and
quiescent GTD (33, 42). In these studies 83 women or histologically
proven choriocarcinoma were compared with 95 benign disease
controls, 26 patients with self resolving hydatidiform mole and 69
with quiescent GTD. In addition, serial samples were collected from
23 women with recurring disease. All were tested for total hCG and
hyperglycosylated hCG. Hyperglycosylated hCG was calculated as
the percentage of total hCG (percent hyperglycosylated hCG). There
was no significant difference in the spread of hCG values between
choriocarcinoma and gestational trophoblastic neoplasm, and no
difference between quiescent GTD and self-resolving hydatidiform
mole cases. In contrast, the percent hyperglycosylated hCG was very
significantly higher in choriocarcinoma/GTN cases than in quiescent
GTD (PStructurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
hyperglycosylated hCG in identifying quiescent disease (55, 56).
Follow-up data indicated that most cases of quiescent GTD lead to
the diminution of hCG, or loss of hCG producing trophoblast cells.
In the majority of cases this occurred within 6 months of the
identification of quiescent gestational trophoblastic disease. In one
rare case it persisted for 9 years (33,42-44). To date, in 23 cases,
active disease followed the diagnosis of quiescent GTN (24% of
cases). While the majority of cases that led to active disease were
those with history of gestational trophoblastic
neoplasm/choriocarcinoma, a few were patients with history of non-
invasive hydatidiform mole. We estimate an approximate 40%
incidence of recurrent disease in patients with history of gestational
trophoblastic neoplasm/choriocarcinoma and 10% incidence in those
without history of invasive disease. Data suggests that quiescent
GTD is a transient condition or pre-malignant disease.
Repeat consultations were performed in 23 of 23 cases in which
active disease was subsequently demonstrated. In 12 of 23 cases,
proportion hyperglycosylated hCG results were able to first identify
active disease 0.5 to 11 months prior to rapidly rising hCG or
detection of clinically active neoplasia. In the remaining 11 cases
proportion hyperglycosylated hCG showed active disease (needing
chemotherapy) at the same time as rising hCG or demonstrable
clinical tumor.
Hyperglycosylated hCG is made by only cytotrophoblast cells, the
invasive trophoblast cells (5,6). Since regular hCG is produced by
syncytiotrophoblast and hyperglycosylated hCG by cytotrophoblast
we conclude that the absence of detectable hyperglycosylated hCG in
patients with quiescent GTD must be associated with conversion of
cytotrophoblast to syncytiotrophoblast or by the total loss of all
cytotrophoblast cells in patients. Clearly, when quiescent GTD
transforms to active disease the number of cytotrophoblast cells must
increase sufficiently to produce detectable hyperglycosylated hCG .
Currently, multiple measurements of rising hCG results are
required to identify new or recurrent choriocarcinoma/GTN. As
shown by this data, a single measurement showing the presence of
hCG-H is sufficient to demonstrate the presence of active disease and
to initiate chemotherapy. This data presented on hyperglycosylated
hCG in identifying quiescent GTD and in the early detection of
recurrent active disease is seemingly sufficient to encourage the
immediate adoption of hhcg as a marker for gestational trophoblastic
diseases.
With the availability of such an accurate diagnostic tool, physicians
can avoid two pitfalls inherent in current hCG testing regimens.
First, the use of an hyperglycosylated hCG assay allows physicians
to determine the presence or absence of invasive disease, to treat
those with active GTD or choriocarcinoma, and avoid unnecessary
170Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
treatment in those with quiescent GTD. Second, the use of an hCG-
H test would allow the physician to diagnose active disease in the
timeliest fashion (without waiting for serial increases in hCG or
physical observance of tumor) and thus initiate treatment at the
earliest sign of actual invasive disease
Physicians treating gestational trophoblastic disease are encouraged
to use the hyperglycosylated hCG test to avoid unnecessary
chemotherapy and surgery, and to initiate treatment of neoplastic
disease as early as possible.
5.4.4 PITUITARY hCG
It is now 30 years since human chorionic gonadotropin (hCG)
production was first demonstrated in healthy non-pregnant women
(57). This hCG was shown in 1980 to be coming from the pituitary
gland (59). As described in numerous publications, low level hCG
production accompanies luteinizing hormone (LH) production at the
time of the mid-cycle pre-ovulatory surge, as a normal part of human
physiology (42, 57-64). Furthermore, significant pituitary derived
hCG is normally present alongside LH due to the lack of suppression
by estrogen and progesterone, and is measurable in serum and urine
samples of postmenopausal women (59-63). In medical practice, a
positive hCG test prior to menopause suggests a gestational event;
either pregnancy or gestational trophoblastic disease (42,61,64). In
practice, a positive hCG in menopausal women represents a
quagmire, and a malignancy is commonly considered. The detection
of hCG in blood after menopause often creates confusion in
physicians unaware of the normal pituitary production of hCG which
can lead to the erroneous assumption of malignant disease
(42,61,64). When this assumption is made, necessary treatments may
be delayed, expensive invasive testing initiated or toxic treatments
given resulting in poor patient outcomes.
In this past year, the USA hCG Reference Service has consulted on
120 cases of peri-menopausal and postmenopausal women with
measurable hCG. Nearly all cases had analogous histories and
conclusions. In most of these, we informed the referring physicians
about the normal physiology of pituitary hCG and suggested how to
clinically confirm it. In almost every history, hCG was detected as
part of pre-operative or pretreatment evaluation. Surgery, therapy or
renal transplants were then postponed pending these consultations
investigating the positive hCG result. In multiple cases needless
hysterectomy was performed or chemotherapy given for assumed
gestational trophoblastic neoplasm or assumed other malignant
disease.
171Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
In cases evaluated by the USA hCG Reference Service, the age
range was 29-69 year, (median age 52), 9 women were menopausal
following oophorectomy (ages 29 to 40) and the balance were
naturally menopausal due to age (age 45 to 69). The average hCG
results at the time of consultation were 9.5 ± 6.5 mIU/ml and the
range was 2.1 to 32 mIU/ml. In all cases low positive serum hCG
results persisted from 3 months to 10 years. In the majority of cases
attending physicians had inferred the presence of gestational
trophoblastic disease or cancer.
In all cases serum was tested for hyperglycosylated hCG (indicates
active gestational trophoblastic disease, see previous section). No
significant hyperglycosylated hCG was detected in any case
(hyperglycosylated hCG 15 mIU/ml and >20 mIU/ml).
It was concluded in all cases that the source of the persistent low
levels of hCG were menopause and normal pituitary gland function.
In all cases it was recommended that the source of hCG be confirmed
by treatment of these women for 3 weeks or longer with a high
estrogen contraceptive pill. If the hCG was of pituitary origin this
should suppress production. To the best of USA hCG Reference
Service knowledge, from feedback received, a high estrogen pill
suppressed hCG production in all cases, confirming the pituitary
origin.
This information about normal pituitary production of hCG peri-
menopause (approximate age 40-55, and post-menopause
approximate age 55>) is of great importance to physicians managing
cases with persistent low levels of hCG and those managing cases
with gestational trophoblastic disease (42-44). These findings show
that persistent low levels of hCG (Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
5.4.5 FREE ß-SUBUNIT AND PLACENTAL SITE
TROPHOBLASTIC TUMORS
Placental site trophoblastic tumors (PSTT) usually presents with
amenorrhea or irregular vaginal bleeding commonly following a
normal pregnancy, spontaneous abortion or occasionally after a
hydatidiform mole (65-68). PSTT is generally associated with
significantly lower hCG levels than choriocarcinoma (Structurally related molecules of human chorionic gonadotrophin (hCG) in gestational trophoblastic diseases
Table 5.9
Two types of PSTT patients were referred to the USA hCG
Reference Service. Firstly, those with history of PSTT to determine
whether a new elevation of hCG was real (hCG was confirmed as
real and not false positive). Secondly, those with persistent low levels
of hCG of unknown source, in all these cases PSTT was later
identified by histology. At total of 7 cases were referred between
2001 and 2004 (Table 9). When examined collectively, persistent
low hCG ranged from 0.77 to 236 mIU/ml, and no significant
hyperglycosylated hCG was identified (You can also read