18-FDG PET for large-vessel vasculitis diagnosis and follow-up
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
18-
FDG PET for large-vessel vasculitis diagnosis and follow-up
F. Angelotti1, R. Capecchi1, A. Giorgetti2, P.A. Erba3, D. Genovesi2,
M. Emdin2, A. Barison2, L. Manca4, V. Rocchi1, P. Migliorini1, A. Tavoni1
1
Clinical Immunology Unit, Department ABSTRACT namely whether they represent two dis-
of Clinical and Experimental Medicine, Objective. Large-vessel vasculitis tinct nosological entities or rather be-
University of Pisa and Azienda (LVV) are chronic inflammatory dis- long to the same spectrum of disorders,
Ospedaliera Universitaria Pisana, Pisa;
eases that affect arteries. While a mere as suggested by striking similarities in
2
Cardiology and Cardiovascular Medicine
Unit, Fondazione Gabriele Monasterio clinical-serological approach does not the distribution of arterial lesions (3).
CNR/Regione Toscana, University of Pisa seem sensitive either in the initial eval- Aortitis can have extremely variable
and Azienda Ospedaliera Universitaria uation nor in long-term monitoring, and often non-specific symptoms and
Pisana, Pisa; 18-
FDG positron emission tomography signs, therefore the index of suspicion
3
Nuclear Medicine, Department of (18-FDG PET) is currently considered of the evaluating clinician must be high
Translational Research and Advanced a useful assessment tool in LVV. We to establish an accurate diagnosis in a
Technology, University of Pisa and
aimed at exploring the utility of 18-FDG, timely fashion (2, 4). Diagnosis should
Azienda Ospedaliera Universitaria
Pisana, Pisa; compared with traditional assessments, be placed as soon as possible both for
4
Department of Clinical and Experimental in the short- and long-term follow-up of the risk of potential life-threatening
Medicine, University of Pisa and patients with LVV. In addition, we com- complications, such as aortic aneurysm,
Azienda Ospedaliera Universitaria pared patterns of vascular involvement dissection, occlusion (thrombosis and
Pisana, Pisa, Italy. in patients with Takayasu’s arteritis stenosis), and for the need of an early
Francesca Angelotti, MD (TAK) and giant cell arteritis (GCA). disease-specific treatment (5, 6).
Riccardo Capecchi, MD Method. We retrospectively analysed Clinical examination, inflammatory
Assuero Giorgetti, MD 47 patients affected by LVV, evaluat- markers and imaging are all critical
Paola Anna Erba, MD
ing clinics, blood chemistry and 18-FDG components of vasculitis assessment in
Dario Genovesi, MD
Michele Emdin, MD PET results, at two time points, short- every stage of the disease, but none of
Andrea Barison, MD term (average 8 months after diagnosis) these items, used individually, is suffi-
Laura Manca, PhD and long-term (average 29 months). cient to adequately evaluate the activity
Valeria Rocchi, MD Results. 18-FDG PET uptake, expressed of LVV (7).
Paola Migliorini, MD as mean value of SUV max, decreased The gold standard for diagnosis remains
Antonio Tavoni, MD significantly during follow-up in all the the biopsy, however angiography, CT,
Please address correspondence to: patients. A low concordance between MRI and positron emission tomography
Antonio Tavoni, 18-
FDG PET and acute phase reactants with 18F-Fluorodeoxyglucose (18-FDG
Immunologia Clinica,
Dipartimento di Medicina
levels was observed, but also a good PET) are widely accepted as comple-
Clinica e Sperimentale, sensitivity in detecting the response to mentary tools to assess vascular in-
Azienda Ospedaliera treatment. volvement at first diagnosis. More con-
Universitaria Pisana, Conclusion. The results confirm the troversial, instead, is how to deal with
Via Roma 67, role of 18-FDG PET as a powerful tool disease monitoring, to detect during the
56126 Pisa, Italy. in the evaluation of LVV, both at the follow-up LVV relapses and damage.
E-mail: a.tavoni@med.unipi.it time of diagnosis and during monitor- Not every patient with systemic symp-
Received on March 22, 2020; accepted in ing. Furthermore, the data confirm that toms suggestive of exacerbations pre-
revised form on August 31, 2020. GCA and TAK are part of the same dis- sents an anatomical progression of
Clin Exp Rheumatol 2021; 39 (Suppl. 129): ease spectrum. the vascular involvement (8). On the
S76-S82. other hand, it is well known that dis-
© Copyright Clinical and Introduction ease activity is particularly difficult to
Experimental Rheumatology 2021.
According to the Chapel Hill Consen- ascertain, and post-mortem histological
sus Conference of 2012 (1), large-ves- studies have shown a significant rate of
Key words: large-vessel vasculitis,
sel vasculitis (LVV) are defined as in- vascular inflammation even in patients
positron emission tomography,
flammatory diseases that affect arteries. with vasculitis considered inactive (9).
Takayasu’s arteritis, giant cell arteritis
Two main variants are distinguished: In fact, active vascular inflammation
Takayasu’s arteritis (TAK) and giant could be detected in the absence of
Competing interests: P.A. Erba declares
royalties from Springer, grants/research cell arteritis (GCA). Both of them are clinical or biological signs of activity
support from Gammaservizi, GE Health- the most common causes of aortitis (2). (10-17). Relying on these markers dur-
care. The other co-authors have declared Concerning the disease classification ing asymptomatic periods can poten-
no competing interests. of LVV, some issues are still debated, tially lead to the false assumption that
S-76 Clinical and Experimental Rheumatology 202118
FDG-18-FDG PET for large-vessel vasculitis / F. Angelotti et al.
the disease is in remission, while there ing a clinically active LVV from other recorded the histopathology of tempo-
is ongoing active inflammation with fi- control diseases. In this study, an uptake ral artery biopsy (TAB) when available.
brosis and progressive occlusion (18). was interpreted as an active vasculitis in Therapy was also recorded.
Traditional inflammatory markers (i.e. the majority of LVV patients considered In parallel, we took into account two
ESR and CRP) have non-optimal sen- in remission from a clinical point of consecutive 18-FDG PETs performed
sitivity (19) and low specificity (13, 18, view (41 out of 71 patients) (39). by patients during follow-up, one in the
20) and thus are not reliable for predict- Despite the high sensitivity and speci- “short-term” (T0) and the other in the
ing recurrences or disease progression ficity of 18-FDG PET for the diagnosis “long-term” (T1).
(7). This limit is particularly critical of LVV, it is still debated whether it Of each 18-FDG PET examination we
in patients treated with IL-6 inhibitors might be useful to monitor disease ac- considered the overall outcome, “ac-
(16, 21), being this cytokine implicated tivity after therapy. More specifically, tive” or “non-active” vasculitis as result-
in hepatic CRP synthesis (20). data on the correlation between 18-FDG ing from the radiologist judgement, the
Regarding the role of imaging, CT, US PET scores and inflammation markers value of SUV max, the distribution of
and angiography mostly allow to evalu- are relatively scarce. the uptake in the vascular districts (e.g.
ate the progression or the appearance of The aim of this work is to evaluate the ascending aorta, arch, descending aorta,
new arterial lesions, but poorly correlate concordance of 18F-fluorode-oxyglu- abdominal aorta, iliac arteries, lower
to the vascular inflammation (22-24). cose-positron emission tomography limbs, succlavia and carotids) and the
This latter is instead correlated with the computed tomography (18-FDG PET) target-to-background ratio (TBR) val-
progression of the disease and the de- imaging with the laboratory tests and ues in different districts: thoracic aorta
velopment of stenosis and thrombosis the clinical judgment, in order to ex- - cava (AOThorcava), abdominal aorta -
(24). On the contrary, positron emission plore the utility of 18-FDG PET with re- cava (AOAbdcava), thoracic aorta - liver
tomography with 18F-Fluorodeoxyglu- spect to traditional assessments in the (AOThorliver), abdominal aorta - liver
cose (18-FDG PET) is a very sensitive follow-up of patients with large-vessel (AOAbdliver), hot vessel - cava (Hot-
functional imaging technique for the vasculitis (LVV). vescava), hot vessel - liver (Hotvesliver).
diagnosis of inflammatory changes in The study received the local ethics
vessels with a diameter greater than 4 Patients and methods committee approval (protocol 14914)
mm (25)and thus has proved to be ex- We retrospectively evaluated a popu- and was conducted according to the
tremely useful in the management of lation of 47 patients affected by LVV Declaration of Helsinki.
large-vessel vasculitis (26-42). fulfilling the 1990 American College
18-
FDG PET can facilitate an early diag- of Rheumatology (ACR) classification Statistical analysis
nosis due to the fact that the increased criteria for GCA and TAK, referred to Data were expressed as mean values (±
metabolic activity caused by the inflam- our unit from November 2012 to June standard deviation) or median values
mation of the vascular wall precedes 2018 (total follow-up period: 15 years). (25th-75th percentiles) for continuous
the morphological changes in the arte- To assess the disease activity, clinical variables and as absolute frequencies
rial wall (28, 36, 37).Often FDG ab- condition and inflammation markers and percentages for nominal variables.
sorption correlates with the presence of were evaluated at two time points, short- Patients with missing data were ex-
increased inflammation markers (24), term (average 8 months after diagnosis) cluded from the analysis. Patients who
but moderate absorption is also present and long-term (average 29 months); the developed CV events were compared
in patients with inactive vasculitis and mean time interval between the two to those who did not, using t-test or
no sign of systemic inflammation. It is evaluations was 24 months. Mann-Whitney U-test for continuous
still unclear whether this reflects a sub- Among inflammatory markers we con- variables and Fisher’s exact test for the
clinical inflammation and predict arte- sidered erythrocyte sedimentation rate nominal valuables. Prism 4 for Win-
rial progression and vascular complica- (ESR, normal values 0–30 mm/h), C- dows (GraphPad Software Inc.) was
tions (24). reactive protein (CRP, normal values used for the analysis. Concordance was
In addition, 18-FDG PET findings of in- 0-0.5 mg/dL) and fibrinogen (normal analysed by means of the Cohen K co-
flammation normalise after treatment values 200–400 mg/dl), when measured efficient (0.21–0.40 indicates modest
with immunosuppressants, mirroring no more than 2 weeks before 18-FDG concordance; 0.41–0.60 indicates mod-
clinical improvement(29). Thus, 18- PET. erate concordance, 0.61–0.80 indicates
FDG PET can be considered a reliable Demographic and clinical data included substantial concordance). The analyses
indicator of disease activity (38). age, sex, disease signs and symptoms were performed using IBM-SPSS, v.
A prospective study was recently pub- (i.e. fever, headache, arthromyalgia, 20, package for Mac Os X.
lished in which 18-FDG PET scan was jaw claudication, abdomen claudica-
performed in patients with LVV, other tion, limbs claudication, hyposphygmia Results
pathologies mimicking LVV (i.e. hyper- of peripheral pulses, ischaemic heart Patients characteristics
lipidaemia) and in healthy controls. 18- disease, visual loss and cerebrovascular The total group of patients consists of
FDG PET showed a sensitivity of 85% manifestations), date of diagnosis and 47 subjects, 10 men and 37 women,
and a specificity of 83% in distinguish- disease duration. For GCA patients, we with a diagnosis of arteritis. The mean
Clinical and Experimental Rheumatology 2021 S-7718
FDG-18-FDG PET for large-vessel vasculitis / F. Angelotti et al.
Table I. Demographic and clinical characteristics of patients at baseline. toms, and 7 months after the diagnosis
of arteritis. The second 18-FDG PET was
Total (n=47) GCA (n=35) TAK (n=12)
performed 29 months as average after
Age (years), median (IQR) 60 (53-61) 65 (57-71) 36 (27-51) the diagnosis. The average interval be-
Sex, M/F 10/37 9/26 1/11 tween first and second 18-FDG PET was
ESR (mm/h), median (IQR) 79 (33-107.5) 69 (33-106.5) 98.5 (39.75-117.3)
CRP (mg/dl), median (IQR) 4.21 (1.3-8.36) 3.7 (1.47-8.32) 6.7 (0.43-10.43)
28 months.
Fibrinogen (mg/dl), median (IQR) 640 (471-880) 640 (471-880) 668 (397.3-890.8)
Steroid (pulse), n (%) 16 (34) 8 (23) 8 (67) Comparison of 18-FDG PET uptake
Steroid (maintenance), n (%) 34 (72) 28 (80) 6 (50) and TBR between short and long-term
MTX, n (%) 17 (36) 12 (34) 5 (42)
AZA, n (%) 1 (2) 1 (2) 0 (0)
follow-up in all patients
CFX, n (%) 20 (43) 16 (46) 4 (33) According to the radiologist’s judge-
MMF, n (%) 1 (2) 1 (2) 0 (0) ment, of the 38 positive 18-FDG PETs at
Latency before diagnosis 3 (0-8) 2 (0-8) 3 (0-13) short-term evaluation, only 15 remained
(months), median (IQR)
positive, while 23 became negative and
M: male; F: female; ESR: erythrocyte sedimentation rate; CRP: C reactive protein; MTX: methotrexate; one that was negative, became positive.
AZA: azathioprine; CFX: cyclophosphamide; MMF: mycophenolate mofetil. The mean value of SUV max at short-
term follow-up in all patients is 4.09
Table II. SUVmax and TBR values in different vascular districts in the short (T0) and long- (SD±2.13), while at long-term follow-up
term (T1) follow-up.
is 2.23 (SD±1.13). 18-FDG PET uptake,
n Mean value ± SD T0 vs. T1 expressed as mean value of SUV max,
(p-value) decreased significantly (p18
FDG-18-FDG PET for large-vessel vasculitis / F. Angelotti et al.
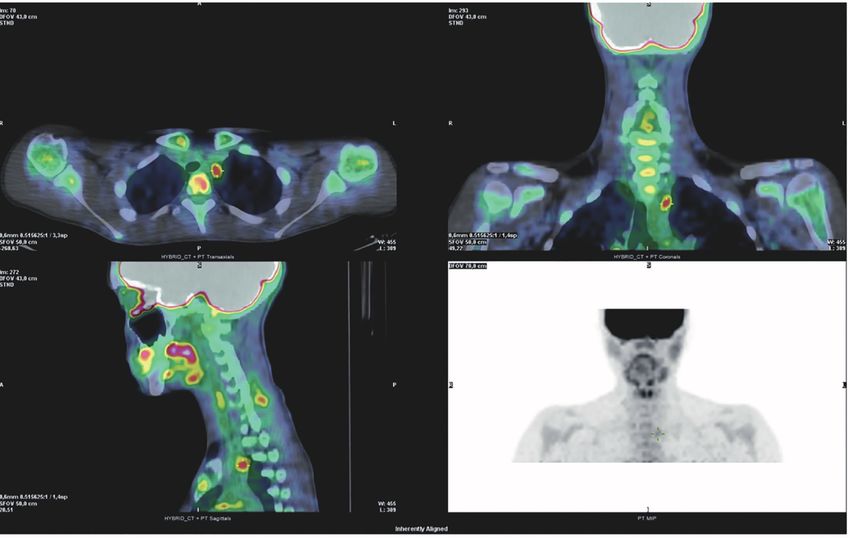
Fig. 1. 18F-FDG 18-FDG PET/CT scans of aortitis.
abdomen claudication, limbs claudica- markers (i.e. ESR, CRP, fibrinogen) clinical manifestations and inflam-
tion, hyposphygmia of peripheral puls- also at long-term follow-up. matory markers, 33 out of 42 patients
es, ischaemic heart disease, visual loss Elevated CRP (that is >0.5 mg/dl) and (78.57%) showed an active disease.
and cerebrovascular manifestations). clinical disease activity show a low con- Among these patients, 18-FDG PET ex-
Regarding the relationship between cordance since these parameters agree amination was positive in 28 subjects
clinical judgement and CRP, these pa- in only 67% of cases. In particular, CRP (66.67%). In 9 patients the disease was
rameters agree in 73% out of cases. was negative in 5% of patients with considered inactive by the clinician
Normal CRP serum levels were detect- clinical disease activity, while in 22% (21.43%), but in these ones 18-FDG PET
ed in 11% of patients with clinically ac- with no symptoms of vasculitis CRP was negative only in 1 subject (2%); 8
tive disease, while 16% of patients with was elevated (κ=0.405). of 9 patients have a positive result at 18-
no symptoms of vasculitis has elevated A fair agreement is observed between FDG PET examination (19.05%).
CRP levels. Thus, a low concordance is fibrinogen and clinical disease activ- At long-term assessment, the disease is
detected between clinical evaluation of ity, since data are concordant in 76% of considered inactive in 30 of 40 patients
disease activity and CRP (κ=0.206). cases (κ=0.521). (75%); 18-FDG PET is concordant (i.e.
Taking into account ESR, the concord- In the case of ESR, no discordant cases negative for active vasculitis) in 18 sub-
ant cases are 97%. No patient without are observed, leading to a high degree jects (45%) while 12 subjects (30%) are
symptoms has a high ESR and only 1 of agreement between the clinical ac- positive at 18-FDG PET examination.
patient with clinically active disease tivity of the disease and the ESR value On the other hand, in 10 patients the
has normal ESR. These data show a (κ=1.00). disease is considered active by the cli-
tendency of these two parameters to nician (25%) and among these 18-FDG
agree (κ=0.93). Comparison between the clinical PET is positive in 4 subjects (10%), and
evaluation of disease activity and negative in 6 (15%).
Concordance between clinical the result of 18-FDG PET Thus, these data show no concordance
disease activity and biomarker We compared the clinician assessment between 18-FDG PET and clinical eval-
values at long-term evaluation of the disease activity with the outcome uation of disease activity because of
We similarly assessed the concord- of 18-FDG PET at short- and long-term the 18 discordant cases (κ=-0.046 for
ance between the clinical evaluation of follow-up. short-term follow-up and κ=0.000 for
disease activity and the inflammatory At short-term assessment, based on long-term).
Clinical and Experimental Rheumatology 2021 S-79FDG-18-FDG PET for large-vessel vasculitis / F. Angelotti et al.
18
Fig. 2. 18F-FDG 18-FDG PET/CT scans of focal vasculitis of the left carotid emergence.
Concordance between 18-FDG PET to increase diagnostic sensitivity and to Recently Salvarani et al., using 18-FDG
and acute phase reactants at observe both the response to treatment PET/CT, published data that support
short- and long-term evaluation and its maintenance over time. In fact, this conclusion. These authors detected
We evaluated the concordance between 18-
FDG PET improve in all the patients: similar distribution pattern of the arte-
18-
FDG PET outcome and ESR, PCR comparing short and long-term evalua- rial lesions in GCA and TA, although
and fibrinogen at the short and long- tion, a statistically significant reduction some subtle differences were reported.
term follow-up. The results indicate a in the average value of SUVmax is ob- They also observed the tendency of
poor concordance of acute phase reac- served, as well as a reduction of TBR arterial lesions to be contiguous in the
tants and 18FDG PET, both in the short values in all the districts considered. aorta and symmetric in branch vessels,
and long term (data not shown). These conclusions are based on real as previously noted in angiographic
life data, obtained in large cohort of studies, and showed a symmetric ex-
Concordance between 18-FDG PET patients evaluated homogeneously in a tension of the lesions in paired vascular
and treatment response single centre and subjected to standard- beds at carotid, axillary, subclavian, ili-
By evaluating the result of 18-FDG PET ised screening procedures that include a ac and femoral arteries level, clustering
in patients treated with steroid pulses large number of 18-FDG PET. with the contralateral counterpart, not
and in patients treated with cyclophos- Furthermore, our data show a very simi- only in TAK but also in GCA popula-
phamide, an agreement was observed lar vascular involvement in both arteritis. tion (43-45).
between the negativity of 18-FDG PET The only significant difference that has A key issue addressed in this paper is
and therapy (κ=0.027 for CS, κ=0.152 emerged is the involvement of the aortic the reliability of evaluation of disease
for CFX). arch, more frequently affected in TAK. activity based exclusively on clinical
Comparing the values of the different symptoms and inflammatory mark-
Discussion TBRs in the two arteritis, only the TBR ers. We observed that the presence of
The data presented in this paper indi- calculated between vena cava and ab- suspicious symptoms has a low con-
cate that 18-FDG PET represents a valid dominal aorta appears to be significantly cordance with CRP both in the short
and powerful tool for the evaluation of different between GCA and TAK. Taken and long-term follow-up, while ESR
patients affected by large-vessel vascu- together, these data suggest that GCA appears to be a more reliable index.
litis, both at the time of diagnosis and and TAK are not two different conditions Due to the scarcity of data related to fi-
during monitoring. 18-FDG PET allows but part of the same disease spectrum. brinogen at short-term assessment, this
S-80 Clinical and Experimental Rheumatology 202118
FDG-18-FDG PET for large-vessel vasculitis / F. Angelotti et al.
was analysed only in the long-term, with a diameter greater than 4 mm; the References
and showed a modest correlation with use of large amounts of ionising radia- 1. AREND WP MB, BLOCH DA, HUNDER GG,
CALABRESE L: Revised International Chapel
clinical symptoms. tion (generally 15¬20 mSv per scan); Hill Consensus Conference Nomenclature of
Thus, our results are in agreement with the high costs and limited access (38, Vasculitides. Arthritis Rheum 2013; 65: 1-1.
published data that suggest the non-op- 40, 41). 2. GORNIK HL, CREAGER MA: Aortitis. Circu-
timal sensitivity (19) and the low speci- A further aspect to take into account is lation 2008; 117: 3039-51.
3. MAKSIMOWICZ-MCKINNON K, CLARK TM,
ficity (13, 18, 20) of traditional inflam- that the presence of atherosclerosis and HOFFMAN GS: Takayasu arteritis and giant
matory markers. the increase in the rate of vascular up- cell arteritis: a spectrum within the same dis-
Similarly, comparing the disease activ- take with age, that might overestimate ease? Medicine (Baltimore) 2009; 88: 221-6.
ity evaluated on a clinical basis with the the degree of vascular inflammation in 4. LORICERA J, BLANCO R, HERNANDEZ JL et
al.: Tocilizumab in giant cell arteritis: Multi-
outcome of 18-FDG PET, we did not ob- older patients (42), even if the distribu- center open-label study of 22 patients. Semin
serve any concordance between these tion of FDG uptake is usually different Arthritis Rheum 2015; 44: 717-23.
parameters, either in the short-term or (i.e. circumferential in LVV, limited in 5. KERR LD, CHANG YJ, SPIERA H, FALLON JT:
Occult active giant cell aortitis necessitating
in the long-term follow-up. atherosclerotic lesion)(42).
surgical repair. J Thorac Cardiovasc Surg
Thus, our data confirm the low sensi- Nevertheless, 18-FDG PET has enabled 2000; 120: 813-5.
tivity and specificity of clinical mani- in our cohort the identification of a great 6. SCHMIDT J, SUNESEN K, KORNUM JB,
festations, and even more of inflam- number of patients with active disease, DUHAUT P, THOMSEN RW: Predictors for
pathologically confirmed aortitis after resec-
matory markers, in monitoring disease that the mere clinical-serological as- tion of the ascending aorta: a 12-year Danish
activity, in particular the possible mini- sessment had not recognised. Thus, 18- nationwide population-based cross-sectional
mal residual disease in vessel walls that FDG PET was a key tool for the assess- study. Arthritis Res Ther 2011; 13: R87.
could be the cause of damage progres- ment of disease activity, allowing also 7. KESER G, DIRESKENELI H, AKSU K:
Management of Takayasu arteritis: a system-
sion. a better evaluation of the response to atic review. Rheumatology 2014; 53: 793-
Besides being useful for the diagnosis therapy, that possibly leads to a lower 801.
and monitoring of LVV, 18-FDG PET incidence of complications. 8. TOMBETTI E, MANFREDI A, SABBADINI MG,
allows the differential diagnosis from In conclusion, we suggest that a multi- BALDISSERA E: Management options for Ta-
kayasu arteritis. Expert Opin Orphan Drugs
other possible causes of increase in in- parametric evaluation, based on clinical 2013; 1: 685-93.
flammatory markers and non-specific symptoms, inflammatory markers and 9. HOFFMAN GS, AHMED AE: Surrogate mark-
or non-typical symptoms. A negative imaging, is necessary to obtain a better ers of disease activity in patients with Ta-
temporal artery biopsy, an ultrasonog- diagnosis and monitoring of LVV. At kayasu arteritis. A preliminary report from
The International Network for the Study of
raphy without an arterial halo, or an present, 18-FDG PET is the most reliable the Systemic Vasculitides (INSSYS). Int J
MRI without aortic wall thickening or method for diagnosis and monitoring of Cardiol 1998; 66 (Suppl. 1): S191-4.
oedema do not exclude the presence of vascular inflammation in patients with 10. O’CONNOR TE, CARPENTER HE, BIDARI S,
WATERS MF, HEDNA VS: Role of inflamma-
LVV, that should be explored by 18-FDG LVV, and is a useful tool in the diag- tory markers in Takayasu arteritis disease
PET/CT when clinical data are sugges- nosis of uncertain forms and in thera- monitoring. BMC Neurol 2014; 14: 62.
tive of LVV(33). peutic monitoring. This critical role of 11. YU-WAI-MAN P, DAYAN MR: Giant cell arte-
Another advantage of obtaining a base- 18-
FDG PET will be strengthened by ritis with normal inflammatory markers. Acta
Ophthalmol Scand 2007; 85: 460.
line 18-FDG PET is to get an initial an increase in its resolution, as will be 12. MAHLMANN A, PFLUECKE C, OUDA A,
semi-quantitative parameter (SUV), probably obtained by 18-FDG PET-MRI SIMONIS G, WEISS N, KAPPERT U: Com-
useful for the diagnosis of aortitis and that should allow the precise identifica- bined immunosuppressive therapy including
also in follow up for monitoring the re- tion of the arterial wall inflammation, a TNF-alpha blocker induces remission in a
difficult to treat patient with Takayasu arteri-
sponse to therapy; according to some combined with a sensitive demonstra- tis and coronary involvement. Vasa 2012; 41:
studies, it may also have a prognostic tion of response to treatment (23). 451-7.
value (in particular in TAK) (29, 33). 13. ISHIHARA T, HARAGUCHI G, TEZUKA D,
KAMIISHI T, INAGAKI H, ISOBE M: Diagno-
18-
FDG PET currently has the limita- Acknowledgements
sis and assessment of Takayasu arteritis by
tion of not being able to discriminate We wish to thank Prof. Chiara Baldini multiple biomarkers. Circ J 2013; 77: 477-
vascular remodelling from inflamma- for reviewing the paper and for her 83.
tory involvement of the arterial wall very useful suggestions. 14. TOMBETTI E, FRANCHINI S, PAPA M, SAB-
BADINI MG, BALDISSERA E: Treatment of
as cause of persistent low-grade ab- refractory Takayasu arteritis with tocilizum-
sorption of vascular FDG in treated Take home messages ab: 7 Italian patients from a single referral
patients considered in remission. Well • 18-
FDG PET scan is the most re- center. J Rheumatol 2013; 40: 2047-51.
known drawbacks of 18-FDG PET are liable method for diagnosing and 15. XENITIDIS T, HORGER M, ZEH G, KANZ L,
HENES JC: Sustained inflammation of the
represented by the lack of a uniform monitoring LVVtherapies; aortic wall despite tocilizumab treatment in
definition of vascular inflammation • A multi-parametric evaluation, two cases of Takayasu arteritis. Rheumatol-
based on the absorption of FDG; the based on clinical symptoms, in- ogy (Oxford) 2013; 52: 1729-31.
inability to provide information on flammatory markers and imaging, 16. TOMBETTI E, DI CHIO MC, SARTORELLI S et
al.: Anti-cytokine treatment for Takayasu ar-
the wall structure or luminal flow; the is necessary for a correct diagnosis teritis: State of the art. Intractable Rare Dis
power of resolution limited to vessels and follow-up of LVV. Res 2014; 3: 29-33.
Clinical and Experimental Rheumatology 2021 S-81FDG-18-FDG PET for large-vessel vasculitis / F. Angelotti et al.
18
17. FERFAR Y, MIRAULT T, DESBOIS AC et al.: al.: The role of 18F-FDG 18-FDG PET in char- MONCAYO R, SCHIRMER M: Do we need 18F-
Biotherapies in large vessel vasculitis. Auto- acterising disease activity in Takayasu arteri- FDG-positron emission tomography as a func-
immun Rev 2016; 15: 544-51. tis. Eur J Nucl Med Mol Imaging 2004; 31: tional imaging technique for diagnosing large
18. KERR GS, HALLAHAN CW, GIORDANO J et 627-34. vessel arteritis? Clin Exp Rheumatol 2003; 21
al.: Takayasu arteritis. Ann Intern Med 1994; 29. KOBAYASHI Y, ISHII K, ODA K et al.: Aortic (Suppl. 32): S1-2.
120: 919-29. wall inflammation due to Takayasu arteritis 38. PIPITONE N, VERSARI A, SALVARANI C:
19. RAHMAN W, RAHMAN FZ: Giant cell (tem- imaged with 18F-FDG 18-FDG PET coregis- Role of imaging studies in the diagnosis and
poral) arteritis: an overview and update. Surv tered with enhanced CT. J Nucl Med 2005; follow-up of large-vessel vasculitis: an up-
Ophthalmol 2005; 50: 415-28. 46: 917-22. date. Rheumatology (Oxford) 2008; 47: 403-
20. DAGNA L, SALVO F, TIRABOSCHI M et al.: 30. WALTER MA, MELZER RA, SCHINDLER C, 8.
Pentraxin-3 as a marker of disease activity MULLER-BRAND J, TYNDALL A, NITZSCHE 39. GRAYSON PC, MAKSIMOWICZ-McKINNON
in Takayasu arteritis. Ann Intern Med 2011; EU: The value of (18F)FDG-18-FDG PET in the K, CLARK TM et al.: Distribution of arterial
155: 425-33. diagnosis of large-vessel vasculitis and the as- lesions in Takayasu’s arteritis and giant cell
21. UNIZONY S, ARIAS-URDANETA L, MILO- sessment of activity and extent of disease. Eur arteritis. Ann Rheum Dis 2012; 71: 1329-34.
SLAVSKY E et al.: Tocilizumab for the treat- J Nucl Med Mol Imaging 2005; 32: 674-81. 40. MAVROGENI S, DIMITROULAS T, CHATZIIO-
ment of large-vessel vasculitis (giant cell 31. ARNAUD L, HAROCHE J, MALEK Z et al.: ANNOU SN, KITAS G: The role of multimo-
arteritis, Takayasu arteritis) and polymyalgia Is (18)F-fluorodeoxyglucose positron emis- dality imaging in the evaluation of Takayasu
rheumatica. Arthritis Care Res (Hoboken) sion tomography scanning a reliable way to arteritis. Semin Arthritis Rheum 2013; 42:
2012; 64: 1720-9. assess disease activity in Takayasu arteritis? 401-12.
22. AL-HOMOOD IA: Tocilizumab: a new thera- Arthritis Rheum 2009; 60: 1193-200. 41. PONTE C, RODRIGUES AF, O’NEILL L, LUQM-
py for large vessel vasculitis. Clin Exp Med 32. LEE SG, RYU JS, KIM HO et al.: Evaluation of ANI RA: Giant cell arteritis: Current treat-
2014; 14: 355-60. disease activity using F-18 FDG 18-FDG PET- ment and management. World J Clin Cases
23. TOMBETTI E, MASON J: Large vessel vas- CT in patients with Takayasu arteritis. Clin 2015; 3: 484-94.
culitis: the search for response biomarkers. Nucl Med 2009; 34: 749-52. 42. TATSUMI M, COHADE C, NAKAMOTO Y,
Expert Rev Clin Immunol 2016; 12: 1011-3. 33. BALINK H, BENNINK RJ, van ECK-SMIT BLF, WAHL RL: Fluorodeoxyglucose uptake in
24. SOUSSAN M, NICOLAS P, SCHRAMM C et al.: VERBERNE HJ: The Role of 18F-FDG 18-FDG the aortic wall at 18-FDG PET/CT: possible
Management of large-vessel vasculitis with PET/CT in Large-Vessel Vasculitis: Appro- finding for active atherosclerosis. Radiology
FDG-18-FDG PET: a systematic literature priateness of Current Classification Criteria? 2003; 229: 831-7.
review and meta-analysis. Medicine (Balti- Biomed Res Int 2014; 2014: 687608. 43. SORIANO A, PAZZOLA G, BOIARDI L et al.:
more) 2015; 94: e622. 34. LEHMANN P, BUCHTALA S, ACHAJEW N et Distribution patterns of 18F-fluorodeoxyglu-
25. BLOCKMANS D, BLEY T, SCHMIDT W: al.: 18F-FDG 18-FDG PET as a diagnostic pro- cose in large vessels of Takayasu’s and giant
Imaging for large-vessel vasculitis. Curr cedure in large vessel vasculitis-a controlled, cell arteritis using positron emission tomog-
Opin Rheumatol 2009; 21: 19-28. blinded re-examination of routine 18-FDG raphy. Clin Exp Rheumatol 2018; 36 (Suppl.
26. BLEEKER-ROVERS CP, BREDIE SJ, van der PET scans. Clin Rheumatol 2011; 30: 37-42. 111): S99-106.
MEER JW, CORSTENS FH, OYEN WJ: F18-fluoro- 35. JANSSEN SP, COMANS EH, VOSKUYL AE, 44. BARDI M, DIAMANTOPOULOS AP: EULAR
deoxyglucose positron emission tomography WISSELINK W, SMULDERS YM: Giant cell recommendations for the use of imaging in
in diagnosis and follow-up of patients with arteritis: heterogeneity in clinical presenta- large vessel vasculitis in clinical practice
different types of vasculitis. Neth J Med tion and imaging results. J Vasc Surg 2008; summary. Radiol Med 2019; 124: 965-72.
2003; 61: 323-9. 48: 1025-31. 45. QUINN KA, ROSENBLUM JS, RIMLAND CA,
27. MELLER J, GRABBE E, BECKER W, VOSS- 36. MELLER J, STRUTZ F, SIEFKER U et al.: GRIBBONS KB, AHLMAN MA, GRAYSON PC:
HENRICH R: Value of F-18 FDG hybrid camera Early diagnosis and follow-up of aortitis Imaging acquisition technique influences in-
18-
FDG PET and MRI in early takayasu aorti- with ((18)F) FDG 18-FDG PET and MRI. Eur terpretation of positron emission tomography
tis. Eur Radiol 2003; 13: 400-5. J Nucl Med Mol Imaging 2003; 30: 730-6. vascular activity in large-vessel vasculitis.
28. WEBB M, CHAMBERS A, AL-NAHHAS A et 37. WENGER M, CALAMIA KT, SALVARANI C, Semin Arthritis Rheum 2020; 50: 71-6.
S-82 Clinical and Experimental Rheumatology 2021You can also read

















































