UC San Diego UC San Diego Previously Published Works
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
UC San Diego
UC San Diego Previously Published Works
Title
Hepatitis C Virus Micro-elimination Among People With HIV in San Diego: Are We on Track?
Permalink
https://escholarship.org/uc/item/2jx2x52q
Journal
Open Forum Infectious Diseases, 10(4)
ISSN
2328-8957
Authors
Cheema, Jaskaran S
Mathews, William C
Wynn, Adriane
et al.
Publication Date
2023-04-04
DOI
10.1093/ofid/ofad153
Copyright Information
This work is made available under the terms of a Creative Commons Attribution-
NonCommercial-NoDerivatives License, available at https://creativecommons.org/licenses/by-
nc-nd/4.0/
Peer reviewed
eScholarship.org Powered by the California Digital Library
University of CaliforniaOpen Forum Infectious Diseases
MAJOR ARTICLE
Hepatitis C virus (HCV) micro-elimination among people
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
PT
with HIV in San Diego: Are we on track?
Jaskaran S Cheema1, William C Mathews1, Adriane Wynn1, Laura B Bamford1, Francesca
RI
J Torriani1, Lucas A Hill1, Amutha V Rajagopal1, Jeffrey Yin1, Sonia Jain2, Richard S
Garfein1, Edward R. Cachay1* and Natasha K Martin1,3*
SC
1. Division of Infectious Diseases and Global Public Health, University of California San Diego,
USA 2. Herbert Wertheim School of Public Health and Human Longevity Science, University of
U
California San Diego, USA. 3. Population Health Sciences, University of Bristol, UK
Background: Rising incidence of hepatitis C virus (HCV) among persons living with HIV
N
(PLWH) in San Diego County (SDC) was reported. In 2018, UCSD launched a micro-
A
elimination initiative among PLWH, and in 2020 SDC launched an initiative to reduce HCV
incidence by 80% across 2015-2030. We model the impact of observed treatment scale-up on
M
HCV micro-elimination among PLWH in SDC.
Methods: A model of HCV transmission among people who inject drugs (PWID) and men who
D
have sex with men (MSM) was calibrated to SDC. The model was additionally stratified by: age,
gender, and HIV status. The model was calibrated to HCV viremia prevalence among PLWH in
TE
2010, 2018, and 2021 (42.1%, 18.5%, 8.5%, respectively), and HCV seroprevalence among
PWID aged 18-39, MSM, and MSM with HIV in 2015. We simulate treatment among PLWH,
weighted by UCSD Owen Clinic (reaching 26% of HCV-infected PLWH) and non-UCSD
EP
——————————————————————————————————————————
*Denotes joint senior authors
CC
Corresponding author: Natasha Martin, 9500 Gillman Drive MC0507, La Jolla, CA, 92037, USA. 858-
822-1779, fax 1-888-539-8781. Natasha-martin@health.ucsd.edu
Alternate corresponding author: Edward Cachay, 200 West Arbor Drive, San Diego, CA 92103, USA.
Ecachay@health.ucsd.edu
A
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of
America. This is an Open Access article distributed under the terms of the Creative Commons
Attribution-NonCommercial-NoDerivs licence (https://creativecommons.org/licenses/by-nc-nd/4.0/),
which permits non-commercial reproduction and distribution of the work, in any medium, provided the
original work is not altered or transformed in any way, and that the work is properly cited. For
commercial re-use, please contact journals.permissions@oup.com
DOI: 10.1093/ofid/ofad153 1treatment, calibrated to achieve the observed HCV viremia prevalence. We simulated HCV
incidence with observed and further treatment scale-up (+/- risk reductions) among PLWH.
Results: Observed treatment scale-up from 2018-2021 will reduce HCV incidence among
PLWH in SDC from a mean 429 infections/year in 2015 to 159 infections/year in 2030. County-
wide scale-up to the maximum treatment rate achieved at UCSD Owen Clinic (in 2021) will
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
reduce incidence by 69%, missing the 80% incidence reduction target by 2030 unless
PT
accompanied by behavioral risk reductions.
Conclusions: As SDC progresses towards HCV micro-elimination among PLWH, a
RI
comprehensive treatment and risk reduction approach is necessary to reach 2030 targets.
KEY POINTS
SC
Question: What can infectious disease modeling inform us about the impact of hepatitis C
(HCV) treatment scale-up in our progress to achieve HCV micro-elimination among PLWH in
U
San Diego County?
N
Findings: The observed DAA scale-up from 2018-2021 will reduce HCV incidence among
PLWH from a mean of 429 infections/year in 2015 to 159 infections/year in 2030 (63%
A
reduction), missing the 80% reduction target.
M
Meaning: Further county-wide treatment scale-up and behavioral interventions to reduce risk are
required to meet the 80% incidence reduction target by 2030.
D
INTRODUCTION
TE
Hepatitis C virus (HCV) and HIV share common transmission routes 1. Although the most
common HCV transmission form in the United States occurs due to sharing injection equipment
EP
among people who inject drugs (PWID) 2, sexual transmission of HCV is significant among
persons living with HIV (PLWH), especially among men who have sex with men (MSM) 3.
Hence, the co-infection of HCV among PLWH is a major public health concern. According to
CC
2009 data from the Centers for Disease Control and Prevention (CDC), 21% of all PLWH were
HCV seropositive 1. As individuals co-infected with HIV and HCV experience accelerated liver
disease progression 1, complications due to untreated HCV are a significant cause of morbidity
A
and mortality among PLWH who are otherwise well-controlled on antiretroviral therapy 1.
In 2016, the World Health Organization (WHO) adopted its Global Health Sector Strategy
(GHSS) and set the strategic goal to eliminate HCV as a public health threat 4. The WHO targets
include a 90% reduction in HCV and HBV incidence (with specific targets of 80% reduction for
HCV and 95% reduction for HBV) and a 65% reduction in HCV mortality by 2030 compared to
a 2015 baseline 4. Because screening for HCV is part of the HIV standard of care and many
PLWH already have access to health services through integrated models of care 5, many consider
DOI: 10.1093/ofid/ofad153 2that PLWH comprise a population where HCV elimination (micro-elimination) is feasible 5.
Indeed, some countries with universal healthcare systems have reported significant progress
toward HCV micro-elimination among PLWH 6,7. Similar programs exist nationally, statewide,
and county-wide in the United States. Our 2018 study on HCV burden in San Diego County
estimated that 55,354 individuals are HCV seropositive in San Diego County 8. The Eliminate
Hepatitis C San Diego County Initiative is a public-private joint endeavor between the San Diego
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
PT
County Health Department and the American Liver Foundation to support the achievement of
the WHO HCV elimination goal 9.
RI
We recently reported that the rising HCV incidence among MSM with HIV indicates an urgent
need for interventions to control the expanding HCV epidemic 10, with a projected number of
3,500 PLWH co-infected with HCV in San Diego in 2017 11. In 2018, UCSD Owen Clinic
SC
launched a micro-elimination initiative to scale-up HCV treatment among PLWH. While this
program has achieved significant progress in HCV treatment uptake among PLWH, the potential
impact of the scale-up, particularly on meeting the 2030 elimination targets, is uncertain. Further,
U
it is unclear whether San Diego is on track to achieve the HCV elimination goals among PLWH.
We aim to address that knowledge gap by using dynamic epidemic modeling of HCV
N
transmission to assess the potential impact of observed treatment scale-up on HCV micro-
A
elimination among PLWH in San Diego County by 2030.
M
METHODS
D
Model description
We developed a dynamic, deterministic compartmental model of HCV transmission and
TE
progression, stratified by HIV infection, which was calibrated to San Diego County. The model
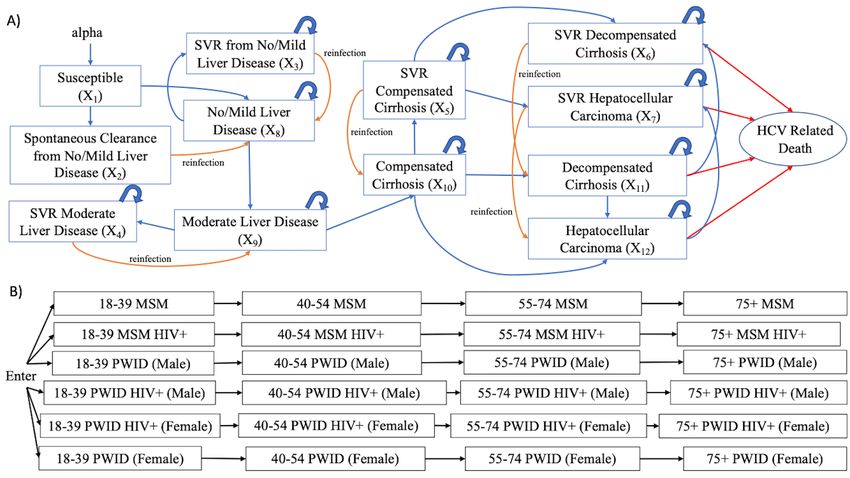
was stratified by Hepatitis C infection and disease progression status (Figure 1a), age, gender,
HIV status, and transmission risk, which included PWID or MSM (Figure 1b). The HCV
EP
infection and disease stages, represented by n are: (i) Susceptible, (ii) Spontaneous Clearance
from no/mild liver disease, (iii) SVR from no/mild liver disease, (iv) SVR Moderate Liver
CC
Disease, (v) SVR Compensated Cirrhosis, (vi) SVR Decompensated Cirrhosis, (vii) SVR
Hepatocellular Carcinoma, (viii) No/Mild Liver Disease, (ix) Moderate Liver Disease, (x)
Compensated Cirrhosis, (xi) Decompensated Cirrhosis, (xii) Hepatocellular Carcinoma. The age
stages are: 18-39, 40-54, 55-74, and 75+ years. The six population sub-types are: MSM HIV-,
A
MSM HIV+, PWID HIV- Male, PWID HIV+ Male, PWID HIV- Female, and PWID HIV+
Female. The model assumes that individuals enter the adult population at 18 years old,
susceptible to primary HCV infection, and in one of the population sub-type compartments
stratified by gender, HIV status, PWID status, and MSM (Figure 1b). PWID enter the model in
the first age stage (18-39 years), and progress through the age stages or discontinue injection
drug use. The rate of permanent cessation of injecting was sampled widely with uncertainty
using data on duration of injection among PWID from STAHR II 12. We assume HIV status is a
DOI: 10.1093/ofid/ofad153 3fixed characteristic; the model does not simulate HIV transmission dynamically due to the stable
HIV prevalence among PWID and MSM in San Diego County 13,14.
Individuals enter the model susceptible to primary HCV infection. HCV transmission is
simulated among PWID and MSM groups separately (without transmission between these
groups) because very few MSM report injecting drugs in San Diego (1% of HIV-negative and
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
3% of MSM diagnosed with acute HIV) 15,16, and based on phylogenetic analyses in other
PT
settings indicating that MSM-IDU and PWID epidemics are distinct 17. Therefore, although a
small fraction of MSM may inject drugs, we classify these individuals as MSM and assume they
RI
inject with other MSM. The model also assumes assortative mixing among MSM by HIV status.
Once acutely infected, individuals can either transition to the no/mild liver disease compartment,
SC
or they may spontaneously clear HCV infection and move to the spontaneous clearance from the
no/mild liver disease compartment. The fraction of individuals spontaneously clear infection,
which is reduced for those with HIV. From the no/mild liver disease compartment, individuals
U
continue to progress through the disease stages as if they continue to have chronic persistent
infection unless successfully treated. Individuals can be treated from all stages. Those who have
N
been successfully treated move into the equivalent SVR stage and are susceptible to HCV
reinfection. Successful treatment stops any HCV-related disease progression unless an individual
A
has already reached the compensated cirrhosis stage or beyond, where disease progression occurs
at a slower rate compared to those without SVR. HCV-related mortality occurs from the
M
decompensated cirrhosis compartments and hepatocellular carcinoma compartments. All
baseline model parameters, sampling distributions, and sources are listed in Table S1
D
(Supplement).
TE
Model Parameterization and Calibration
The model was parameterized mainly from the published literature (see Table S1, Supplement).
For model calibration and parameterization, we used data from our 2018 HCV burden estimation
EP
(population sizes and HCV seroprevalence) among adults over age 18 in San Diego County 8 and
three time-points of HCV viremia prevalence among PLWH from UCSD Owen Clinic 18. By
varying seven pre-determined parameters (transmission rate among MSM, transmission rate
CC
among PWID, degree of assortative mixing among MSM by HIV status, county-wide annual
treatment rates among HIV/HCV co-infected individuals treated from 1996-2010 and 2011-
2017, non-UCSD treatment rates among HIV/HCV co-infected individuals from 2018-2021, and
A
number of PWID at model initialization in 1955) the model was calibrated to: HCV
seroprevalence estimates in 2015 among MSM (4.6% among all MSM, 16.5% among MSM with
HIV) and PWID aged 18-39 years (49.5%) 8,12, HCV viremia prevalence among HCV
seropositive PLWH of 42.1% (2010), 18.5% (2018) and 8.5% (2021) 18, and number of PWID
in 2007 19. Calibrated parameters are listed in Table S2 (Supplement). The calibrated model was
then validated against HCV seroprevalence among PWID aged 40-54 (68%) and 55-74 (88%) in
2015 (age stratified data unpublished, but overall prevalence published in 12).
DOI: 10.1093/ofid/ofad153 4Historic (pre-2017) HCV treatment rates among PLWH were unknown in San Diego County and
calibrated to observed HCV viremia prevalence trends among PLWH. To obtain the observed
declines in viremic prevalence among PLWH, we simulated a piece-wise treatment function
from 1996-2010, 2011-2017, and 2018-2021. The time period of 1996-2010 represents the
pegylated interferon (IFN) plus ribavirin era. 2011-2017 represents the era of the first generation
of direct-acting antiviral (DAA) therapy, such as Telaprevir (which still required IFN and was
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
PT
available in Feb 2011 at UCSD through compassionate access programs), along with the DAA
era. The UCSD Owen Clinic cares for approximately 3,200 PLWH every year. As we had data
from UCSD Owen Clinic on treatment rates from 2018 onwards, we simulated a weighted
RI
treatment rate during this period between UCSD and other (non-UCSD) clinics, with UCSD
Owen Clinic providing care for an estimated 26% of PLWH in San Diego County in the last five
years 11,20 and our model assumed a conservative estimate of a similar proportion of PLWH co-
SC
infected with HCV. At Owen clinic, a rapid scale-up of HCV treatment among PLWH occurred
from 2018 onwards, achieving an average rate of 54% HCV-infected PLWH treated per year
between 2018-2021, reaching a maximum treatment rate of 71% in 2021. HCV treatment rates
U
among patients without HIV were obtained from studies in San Francisco and nationally 21,22. As
N
the model does not explicitly model diagnosis, the data informing our treatment rates are based
on treatment among the entire population, and calibrated treatment rates among PLWH outside
A
Owen Clinic implicitly incorporate undiagnosed individuals.
M
To capture uncertainty in input parameters, a sample of 500 parameter sets was drawn from
uncertainty distributions for each parameter. These sampled parameter sets were then used to
generate 500 model fits to the observed data. Calibration was achieved using a least-squares
D
minimization solver, lsqnonlin, in MATLAB (Optimization Toolbox). The lsqnonlin function
uses the Levenberg-Marquardt minimization algorithm, and we use the function MultiStart to
TE
start from multiple initial guess points within the parameter priors to ensure a global minimum is
found. We assign wide prior bounds to the unknown parameters and assess our posterior
estimates to ensure our priors were sufficiently wide (Table S2 shows priors and posteriors).
EP
Calibrated model runs were then excluded if the fits fell outside the 95% CI of the calibration
data for HCV seroprevalence in 2015 among (i) all MSM, (ii) PWID aged 18-39 years, (iii)
CC
MSM with HIV 8,12, generating a total of 182 model fits to the data.
Simulation scenarios
A
We simulated three scenarios of HCV treatment. For all of them, we assumed a treatment rate of
2%/year from 1996 to the end of 2012. It increased to 5%/year from 2013 onwards for all non-
PLWH populations 21,22. Among PLWH, our calibrated model fits generated estimates of mean
treatment rates of 25.4%/year from 1996-2010 and 28.8%/year from 2011-2017. From 2018
onwards, the following scale-up among PLWH was simulated:
DOI: 10.1093/ofid/ofad153 5• Scenario 1 (counterfactual, no scale-up from 2018 onwards): continuation of pre-2018
treatment rates [mean 28.8% of chronically infected PLWH treated/year]
• Scenario 2 (observed): UCSD [53.7%/year], other sites [calibrated 60.6%/year]
• Scenario 3 (enhanced scale-up from 2021): As in scenario 2, then all scale-up to
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
maximum UCSD treatment rate [in 2021, 71% chronically infected PWH treated/year]
PT
starting in 2021
• Scenario 4 (enhanced scale up plus halved transmission risk from 2021 onwards):
RI
As in scenario 3, with the addition of a halving of transmission risk starting in 2021.
We outputted the incidence of HCV infections among PLWH, HCV viremia prevalence among
SC
PLWH, and the percent reduction in HCV incidence among PLWH from 2015 to 2030.
Sensitivity analyses
U
We performed a partial rank coefficient correlation (PRCC) analysis to understand how sensitive
N
the model prediction of HCV incidence reductions (2015-2030) was to uncertainty in the
underlying parameters.
A
We perform several one-way sensitivity analyses to test the importance of model assumptions.
M
First, we examine variations in assumptions of treatment among people without HIV. For our
baseline analysis, we assume historic treatment rates, but we perform two additional sensitivity
analyses assuming: (i) treatment scale-up at the same relative percent increase as HCV-infected
D
PLWH compartments and (ii) 2-fold relative percent increase as compared to HCV infected
PLWH compartments.
TE
Second, there is uncertainty regarding the effect of the COVID-19 pandemic on treatment rates
in San Diego County, but national analyses showed a drop in treatment by 20% during 2020,
EP
which rebounded through the end of 2020 but did not achieve pre-COVID levels . We performed
two sensitivity analyses where treatment rates were reduced by a relative 20% from (iii) 2020 to
2021 (then returning to pre-COVID levels in 2022), and (iv) 2020 to 2024 (returning to pre-
CC
COVID levels in 2025).
Lastly, our baseline analysis assumes similar SVR rates by risk, as a recent meta-analysis found
SVR rates among PWID or people on opiate substation therapy are high (90%) and were not
A
significantly different to patients without a history of injecting drugs 23. However, we
additionally performed a sensitivity analysis, where SVR rates among PWID are reduced by a
relative 10% (re-calibrated parameters listed in Table S3, Supplement).
Statistical analysis
The model was created using MATLAB (version R2022b).
DOI: 10.1093/ofid/ofad153 6RESULTS
The model calibration resulted in 182 runs that fit the data. The calibrated model accurately
matched 2015 HCV seroprevalence estimates for MSM and PWID aged 18-39 years and HCV
viremia prevalence among PLWH for 2010, 2018, and 2021 (Table 1). The model was validated
against HCV seroprevalence estimates among PWID aged 40-54 (model estimate 71.5% [95%
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
CI: 61.9%, 77.9%] compared to 68% target) and PWID aged 55-74 (84.3% [95% CI: 75.7%,
PT
89.4%] compared to 88% target) in 2015. In 2015, the model projects 429 [95% CI: 238, 777]
incident HCV infections among PLWH (Figure 2), with an HCV incidence rate of 2.6 per 100
RI
person-years (/100py) [95% CI: 1.4, 4.6]. HCV viremia prevalence among HCV seropositive
PLWH was estimated at 27.2% [95% CI: 21.7%, 32.3%] (Figure 3). Details on HCV incident
infections (total) among PLWH in San Diego County are provided in Table S4 (Supplement).
SC
Without treatment scale-up in 2018 (scenario 1), incident HCV infections among PLWH were
expected to decrease to 342 [95% CI: 183, 633] incident infections by 2018, with an HCV
U
incidence rate of 2.0/100py [95% CI: 1.1, 3.7]. By 2030, incident infections decline to 347 [95%
CI: 185, 636] but the HCV elimination target is not reached – with an estimated 43% [95% CI:
N
33%, 52%] reduction in HCV incidence from 2015-2030 (Figure 2). By 2030, HCV incidence
rate declines to 1.4/100py [95% CI: 0.7, 3.0]. HCV viremia prevalence among PLWH declines to
A
18.8% [95% CI: 13.2%, 25.1%] in 2018 and 11.2% [95% CI: 8.1%, 17.4%] in 2030.
M
With observed treatment scale-up from 2018 onwards (scenario 2), the model projects a sharp
decline in incident HCV infections and HCV viremia prevalence among PLWH that slowly
tapers off as the model approaches 2030. By 2021, the number of incident infections drops to
D
211 [95% CI: 109, 421], HCV incidence rate drops to 1.2/100py [95% CI: 0.6, 2.4], and viremia
TE
prevalence among HCV seropositive PLWH drops to 8.6% [95% CI: 8.6%, 8.6%]. By 2030, the
number of incident infections drops to 159 [95% CI: 78, 331], HCV incidence rate drops to
0.9/100py [95% CI: 0.4, 1.9], and viremia prevalence drops to 6.3% [95% CI: 5.2%, 7.3%].
EP
Between 2015 and 2030, this would achieve a reduction in HCV incidence among PLWH of
63% [95% CI: 57%, 67%].
If non-UCSD sites scale-up to the maximum levels achieved at UCSD from 2021 onwards
CC
(scenario 3), the model predicts 132 [95% CI: 59, 309] incident HCV infections among PLWH
in 2030, with an HCV incidence rate of 0.7/100py [95% CI: 0.3, 1.8], just falling short of the
HCV elimination goal (achieving a decrease in HCV incidence among PLWH of 69% [95% CI:
A
60%, 75%]). If in addition to treatment scale-up to the maximum level, there is a reduction in the
behavioral risk starting in 2021 (Scenario 4), the model predicts 28 [95% CI: 13, 68] incident
infections among PLWH in 2030, with an HCV incidence rate of 0.002/100py [95% CI: 0,
0.004], meeting the HCV elimination goal (achieving a decrease in HCV incidence among
PLWH of 94% [95% CI: 91%, 95%].
DOI: 10.1093/ofid/ofad153 7Reductions in incidence can be tracked through corresponding reductions in HCV viremia
prevalence among HCV seropositive PLWH (Figure 3) to monitor elimination progress, with
scenarios 2 and 3 projecting between a 4% to 7% viremia prevalence among PLWH by 2030.
The HCV reinfection rate among previously treated PLWH is projected to remain steady at
around 4%, with treatment scale-up scenarios 2 and 3 projecting a slight increase from 3.4% in
2015 to above 4.5% by 2030. Only the scenario with behavioral risk reductions results in
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
PT
reduced reinfection incidence in 2030. Results on HCV reinfection rate among previously treated
PLWH and HCV-infected PLWH under treatment in San Diego County are presented in Figure 4
and Figure S1 (Supplement), respectively.
RI
Sensitivity and Uncertainty Analysis
SC
There is uncertainty in treatment rates among HCV-infected persons without HIV, which
we explored through sensitivity analysis (see Figures S2, S3, and S4, Supplement). Assuming an
increase in background treatment among those without HIV, the model projects greater
U
reductions in HCV incidence among PLWH (see Figure S5, Supplement, which looks at
sensitivity analyses on relative reduction in HCV incidence among PLWH from 2015-2030 (%)).
N
However, our models still predict that status quo treatment rates will not be able to achieve
elimination with this level of scale-up, unless there was a two-fold relative increase in treatment
A
rates among non-PLWH populations compared to PLWH populations (mean 82% reduction). In
contrast, if treatment rates for PLWH were scaled-up among non-UCSD providers, and treatment
M
rates for people infected with HCV mono-infection also increased (at the same relative rate or
above), the HCV elimination targets could be met and even achieve a 90% reduction in incidence
D
(see Figure S5, Supplement).
TE
In additional scenario analyses assuming a 20% reduction in HCV treatment rates during
the COVID-19 pandemic (from 2020-2021 or 2020-2025), the model projects more HCV
incident cases during the reduced treatment rate period (see Figures S2, S3, and S4, Supplement).
EP
However, the relative reduction in HCV incidence among PLWH from 2015-2030 is similar to
the baseline analysis (see Figure S5, Supplement).
The model findings were additionally insensitive to analyses assuming PWID have
CC
reduced SVR rates of a relative 10% lower than non-PWID (see Figures S2, S3, S4, and S5,
Supplement).
A
The outcomes from the partial rank correlation coefficient uncertainty analysis found that
the predicted relative reductions in HCV incidence among PLWH from 2015-2030 are most
sensitive to the relative HCV susceptibility for PLWH compared to individuals without HIV,
with greater susceptibility among PLWH resulting in lower incidence reductions (see Figure S6,
Supplement)
DOI: 10.1093/ofid/ofad153 8DISCUSSION
Our analyses used epidemic modeling with available surveillance data from an HCV micro-
elimination initiative among PLWH in San Diego County to determine whether we are on track
to achieve 2030 HCV elimination targets. Our analysis indicates that despite a substantial
increase in HCV treatment provided to PLWH at UCSD Owen Clinic, current levels of treatment
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
are unlikely to achieve the HCV incidence elimination target of 80% reduction between 2015
PT
and 2030 among PLWH in San Diego County. We found that achieving HCV micro-elimination
among PLWH will likely require a scale-up of HCV treatment among both PLWH and
RI
reductions in transmission risk. In response to this observation, the Owen Clinic expanded
services in 2022 to treat HCV in people who use drugs without HIV in conjunction with
integrated substance use treatment and HIV prevention services. The expansion of evidence-
SC
based harm reduction interventions such as medications for opioid use disorder and syringe
service programs (which together have been shown to reduce risk by 75% among PWID) 24, and
the development of interventions to reduce HCV risk among MSM are both needed. Yet, there is
U
insufficient evidence on effective interventions to mitigate the risk of sexual HCV transmission
among MSM. Our Clinic protocol includes periodic STI testing during and after DAA treatment
N
as a surrogate marker of ongoing condomless behaviors. This strategy provides us with
A
opportunities for reinforcement counseling on sexual behaviors associated with HCV infection
(such as condomless anal sex, fisting, and multiple partners) 25-27 to prevent HCV reacquisition
M
and forwards transmission 28. Additionally, our findings highlight that reinfection may be an
important consideration among PLWH, with both modeling and observational studies showing a
potential rise in reinfection rates with expanded treatment 28.
D
Strengths and Limitations
TE
The Lancet Gastroenterology & Hepatology Commission on Accelerating the Elimination of
Viral Hepatitis point out that HCV elimination data are limited 29. Traditional surveillance data
EP
on new diagnoses is hampered by under-ascertainment and late diagnoses, so longitudinal data
from at-risk populations may provide better insights regarding changes in reinfection incidence
and chronic prevalence and treatment scale-up impacts 29. This is one of the strengths of our
CC
analysis because it uses recent data on HCV treatment and chronic prevalence from a large
cohort of PLWH at the UCSD Owen Clinic in San Diego.
However, the model does have several limitations. First, we lacked recent and robust data on
A
HCV treatment rates among the population without HIV in San Diego. We explored the
implications through sensitivity analyses, but this warrants further exploration. The COVID-19
pandemic led to reduced HCV testing and treatment, nationally 30 and it is possible that HCV
treatment rates declined both among PLWH and overall in San Diego County, even though at the
UCSD Owen Clinic, treatment rates increased in 2021. Nevertheless, even in our simulations
with more pronounced disruptions until 2025, our key results were unchanged that scaled-up
treatment is required to achieve HCV elimination. Although our modeling focuses on a single
DOI: 10.1093/ofid/ofad153 9county, to our knowledge, there are few funded projects explicitly aimed to facilitate larger-scale
data accrual tracking HCV elimination among PLWH with a similar level of detail in the US.
Investing in better surveillance systems for PLWH that track and routinely report data such as
HCV diagnoses, treatment numbers, outcomes, and reinfections would facilitate more robust
modeling, validation, and analytics to determine whether communities are on track for HCV
elimination.
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
PT
Second, our model only implicitly included the impact of harm reduction impact in our
calibrated transmission rates. We believe this is justifiable because there has been no evidence of
RI
a recent scale-up of harm reduction efforts in San Diego County. However, lifting the ban on
syringe service programs in 2021 provided an important opportunity for the scale-up of these
important prevention measures. If scaled-up, harm reduction could support HCV elimination
SC
efforts as explored in our behavior change scenario, prevent infection/reinfection among PWID,
and have other benefits on preventing HIV and other health harms among PWID 31-33.
U
Third, our model neglects immigration and emigration as we lack data on migration into and out
of San Diego county by HIV and HCV status. However, we note that the San Diego-Tijuana
N
border is one of the busiest land border crossings in the world. While import of HCV infections
could hamper elimination efforts, HCV treatment efforts in San Diego could aid in prevention of
A
transmission from individuals who emigrate to other areas.
M
Fourth, our model assumes a stable PWID population size due to a lack of data to suggest
otherwise, although we note the PWID population size estimate is old and uncertain. National
data indicates an increase in PWID population size, mainly driven by increases in rural areas 34.
D
If the PWID population size is increasing in San Diego, it will likely further hamper elimination
TE
efforts.
Fifth, our work focuses on PLWH and therefore does not consider what is needed for HCV
elimination more broadly, nor does it assess the cost implications of elimination. Future work
EP
should examine the most cost-effective HCV elimination strategies and the budgetary impact of
achieving HCV elimination.
CC
CONCLUSION
A
San Diego County is progressing towards HCV micro-elimination among PLWH, but increased
HCV screening, treatment scale-up, and monitoring of HCV viremia among PLWH are required
to reach the 2030 targets. To ensure treatment rates can be maintained, efforts to identify
remaining treatment barriers among PLWH are necessary. Scale-up of harm reduction services,
including medications for opioid use disorder, syringe exchange and supervised consumption
sites among PWID both with and without HIV, are needed to reduce the risk of
infection/reinfection.
DOI: 10.1093/ofid/ofad153 10TABLES
Table 1: HCV Calibration Data for San Diego County and Model Outputs
Year Observed Calibration Calibrated Model Reference
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
Data [95% C.I.] Output
PT
[95% C.I.]
HCV seroprevalence among MSM 2015 0.165 [0.155, 0.176] 0.163 [0.156, 0.172] Wynn et
with HIV al. 8
RI
HCV seroprevalence among all MSM 2015 0.046 [0.030, 0.061] 0.054 [0.047, 0.061] Wynn et
al. 8
HCV seroprevalence among PWID 2015 0.495 [0.428, 0.563] 0.494 [0.433, 0.552] Horyniak
SC
aged 18-39 years et al. 12
2010 0.4211 [0.3791, 0.4643] 0.4212 [0.4128, 0.4444] UCSD
U
HCV viremia prevalence among HCV Owen
seropositive PWLH Clinic 18
2018
N
0.1849 [0.1534, 0.2212] 0.1844 [0.1321, 0.2384] UCSD
Owen
A
Clinic 18
2021 0.0857 [0.0636, 0.1146] 0.0857 [0.0857, 0.0857] UCSD
M
Owen
Clinic 18
Number of PWID (total) 2007 24,991 [3,751, 49,503] 24,996 [24,991, 25,031] Tempalski
D
et al.19
TE
EP
CC
A
DOI: 10.1093/ofid/ofad153 11Presented as a late-breaker poster at Conference on Retroviruses and Opportunistic Infections
(CROI) 2022, Denver, February 15, 2022
Funding: This study was funded by the NoCo Grant funded by Gilead Sciences (IN-US-334-
4481). The funders played no role in the design or interpretation of this study. NM, EC, and SJ
were additionally funded by the San Diego Center for AIDS Research (SD CFAR), an NIH-
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
funded program (P30 AI036214), which the following NIH Institutes and Centers support:
PT
NIAID, NCI, NHLBI, NIA, NICHD, NIDA, NIDCR, NIDDK, NIGMS, NIMH, NIMHD, FIC,
and OAR. Data from the STAHR study were obtained with support from the National Institute of
RI
Drug Abuse (R01 DA031074).
Potential Conflicts of Interest: NM has received unrestricted research grants from Gilead and
SC
Merck. ERC has received unrestricted research grants from Gilead and Merck. He also
participated in an advisory board to Theratechnologies for an unrelated topic.
Patient Consent Statement: Our study does not include factors necessitating patient consent
U
References
1.
N
People Coinfected with HIV and Viral Hepatitis. Website. CDC. Updated September 21, 2020.
A
Accessed May 22, 2021, 2021. https://www.cdc.gov/hepatitis/populations/hiv.htm
2. Hepatitis C Questions and Answers for Health Professionals. Centers for Disease Control and
M
Prevention. Updated August 7, 2020. Accessed May 22, 2021, 2021.
https://www.cdc.gov/hepatitis/hcv/hcvfaq.htm
3. Hagan H, Jordan AE, Neurer J, Cleland CM. Incidence of sexually transmitted hepatitis C virus
D
infection in HIV-positive men who have sex with men. AIDS. Nov 2015;29(17):2335-45.
doi:10.1097/QAD.0000000000000834
TE
4. Consolidated strategic information guidelines for viral hepatitis: planning and tracking progress
towards elimination. 2018.
5. Cachay ER, Hill L, Ballard C, et al. Increasing Hepatitis C treatment uptake among HIV-infected
EP
patients using an HIV primary care model. AIDS research and therapy. 2013;10(1):9-9.
doi:10.1186/1742-6405-10-9
6. Kusejko K, Salazar-Vizcaya L, Shah C, et al. Sustained Effect on Hepatitis C Elimination Among
CC
Men Who Have Sex With Men in the Swiss HIV Cohort Study: A Systematic Re-Screening for
Hepatitis C RNA Two Years Following a Nation-Wide Elimination Program. Clinical Infectious
Diseases. 2022;doi:10.1093/cid/ciac273
7. Chen G-J, Ho S-Y, Su L-H, et al. Hepatitis C microelimination among people living with HIV in
A
Taiwan. Emerging Microbes & Infections. 2022:1-29. doi:10.1080/22221751.2022.2081620
8. Wynn A, Tweeten S, McDonald E, et al. The estimated hepatitis C seroprevalence and key
population sizes in San Diego in 2018. PLoS One. 2021;16(6):e0251635.
doi:10.1371/journal.pone.0251635
9. Suckow S, Ramers C. Eliminate Hepatitis C San Diego County Initiative. Live Well San Diego.
2019. Accessed May 22, 2021.
DOI: 10.1093/ofid/ofad153 12https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/bhs/documents/NOC/bhab/Elimi
nate%20Hepatitis%20C%20San%20Diego%20County%20Inititiative%20PPT_BHAB.
10. Chaillon A, Sun X, Cachay ER, et al. Primary Incidence of Hepatitis C Virus Infection Among
HIV-Infected Men Who Have Sex With Men in San Diego, 2000-2015. Open forum infectious
diseases. 2019;6(4):ofz160-ofz160. doi:10.1093/ofid/ofz160
11. Reports and Statistics San Diego Office of HIV and AIDS statistics. Accessed 10/15/2021, 2021.
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
https://www.sandiegocounty.gov/content/sdc/hhsa/programs/phs/hiv_aids_epidemiology_unit/repo
PT
rts_and_statistics.html
12. Horyniak D, Wagner KD, Armenta RF, Cuevas-Mota J, Hendrickson E, Garfein RS. Cross-border
injection drug use and HIV and hepatitis C virus seropositivity among people who inject drugs in
RI
San Diego, California. Int J Drug Policy. Sep 2017;47:9-17. doi:10.1016/j.drugpo.2017.06.006
13. HIV/AIDS Epidemiology Report - 2016. 2017.
https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/EpiReport2017fi
SC
nal.pdf
14. Prevention CfDCa. NCHHSTP AtlasPlus. Updated October 1, 2021. Accessed January 5, 2021.
https://gis.cdc.gov/grasp/nchhstpatlas/charts.html
U
15. Hoenigl M, Anderson CM, Green N, Mehta SR, Smith DM, Little SJ. Repeat HIV-testing is
associated with an increase in behavioral risk among men who have sex with men: a cohort study.
16.
N
BMC Med. Sep 11 2015;13:218. doi:10.1186/s12916-015-0458-5
Hoenigl M, Green N, Mehta SR, Little SJ. Risk Factors for Acute and Early HIV Infection Among
A
Men Who Have Sex With Men (MSM) in San Diego, 2008 to 2014: A Cohort Study. Medicine
(Baltimore). Jul 2015;94(30):e1242. doi:10.1097/md.0000000000001242
M
17. Vanhommerig JW, Bezemer D, Molenkamp R, et al. Limited overlap between phylogenetic HIV
and hepatitis C virus clusters illustrates the dynamic sexual network structure of Dutch HIV-
infected MSM. Aids. Sep 24 2017;31(15):2147-2158. doi:10.1097/qad.0000000000001592
D
18. Cachay E TF, Hill L, Ballard C, Aquino A, Qin H, Jain S, Martin S, Mathews WmC. Progress and
real-life challenges for HCV elimination in People living with HIV. presented at: Conferences on
TE
Retrovirus and Opportunistic Infections; March 8-11 2020; Boston, USA.
19. Tempalski B, Pouget ER, Cleland CM, et al. Trends in the population prevalence of people who
inject drugs in US metropolitan areas 1992-2007. PLoS One. 2013;8(6):e64789.
EP
doi:10.1371/journal.pone.0064789
20. Cachay ER, Hill L, Torriani F, et al. Predictors of Missed Hepatitis C Intake Appointments and
Failure to Establish Hepatitis C Care Among Patients Living With HIV. Open Forum Infectious
CC
Diseases. 2018;5(7)doi:10.1093/ofid/ofy173
21. Thomas DL. State of the Hepatitis C Virus Care Cascade. Clin Liver Dis (Hoboken). Jul
2020;16(1):8-11. doi:10.1002/cld.915
22. Facente SN, Grebe E, Burk K, et al. Estimated hepatitis C prevalence and key population sizes in
A
San Francisco: A foundation for elimination. PLoS One. 2018;13(4):e0195575.
doi:10.1371/journal.pone.0195575
23. Graf C, Mücke MM, Dultz G, et al. Efficacy of Direct-acting Antivirals for Chronic Hepatitis C
Virus Infection in People Who Inject Drugs or Receive Opioid Substitution Therapy: A Systematic
Review and Meta-analysis. Clin Infect Dis. May 23 2020;70(11):2355-2365.
doi:10.1093/cid/ciz696
DOI: 10.1093/ofid/ofad153 1324. Platt L, Minozzi S, Reed J, et al. Needle and syringe programmes and opioid substitution therapy
for preventing HCV transmission among people who inject drugs: findings from a Cochrane
Review and meta-analysis. Addiction. Mar 2018;113(3):545-563. doi:10.1111/add.14012
25. Newsum AM, Matser A, Schinkel J, et al. Incidence of HCV Reinfection Among HIV-Positive
MSM and Its Association With Sexual Risk Behavior: A Longitudinal Analysis. Clin Infect Dis.
Aug 2 2021;73(3):460-467. doi:10.1093/cid/ciaa645
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
26. Vanhommerig JW, Lambers FA, Schinkel J, et al. Risk Factors for Sexual Transmission of
PT
Hepatitis C Virus Among Human Immunodeficiency Virus-Infected Men Who Have Sex With
Men: A Case-Control Study. Open Forum Infect Dis. Sep 2015;2(3):ofv115.
doi:10.1093/ofid/ofv115
RI
27. Volk JE, Marcus JL, Phengrasamy T, Hare CB. Incident Hepatitis C Virus Infections Among
Users of HIV Preexposure Prophylaxis in a Clinical Practice Setting. Clin Infect Dis. Jun 1
2015;60(11):1728-9. doi:10.1093/cid/civ129
SC
28. Hill LA, Martin NK, Torriani FJ, et al. Screening for Sexually Transmitted Infections During
Hepatitis C Treatment to Predict Reinfection Among People With HIV. Open forum infectious
diseases. 2020;8(2):ofaa643-ofaa643. doi:10.1093/ofid/ofaa643
U
29. Cooke GS, Andrieux-Meyer I, Applegate TL, et al. Accelerating the elimination of viral hepatitis:
a Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol Hepatol. Feb
30.
N
2019;4(2):135-184. doi:10.1016/s2468-1253(18)30270-x
Hoenigl M, Abramovitz D, Flores Ortega RE, Martin NK, Reau N. Sustained impact of the
A
COVID-2019 pandemic on HCV treatment initiations in the United States. Clin Infect Dis. Mar 2
2022;doi:10.1093/cid/ciac175
M
31. MacArthur GJ, Minozzi S, Martin N, et al. Opiate substitution treatment and HIV transmission in
people who inject drugs: systematic review and meta-analysis. Bmj. Oct 3 2012;345:e5945.
doi:10.1136/bmj.e5945
D
32. Aspinall EJ, Nambiar D, Goldberg DJ, et al. Are needle and syringe programmes associated with a
reduction in HIV transmission among people who inject drugs: a systematic review and meta-
TE
analysis. Int J Epidemiol. Feb 2014;43(1):235-48. doi:10.1093/ije/dyt243
33. Sordo L, Barrio G, Bravo MJ, et al. Mortality risk during and after opioid substitution treatment:
systematic review and meta-analysis of cohort studies. Bmj. Apr 26 2017;357:j1550.
EP
doi:10.1136/bmj.j1550
34. Bradley H, Hall EW, Asher A, et al. Estimated Number of People Who Inject Drugs in the United
States. Clin Infect Dis. Jan 6 2023;76(1):96-102. doi:10.1093/cid/ciac543
CC
35. Borroni G, Andreoletti M, Casiraghi MA, et al. Effectiveness of pegylated interferon/ribavirin
combination in 'real world' patients with chronic hepatitis C virus infection. Aliment Pharmacol
Ther. May 2008;27(9):790-7. doi:10.1111/j.1365-2036.2008.03657.x
36. Scotto R, Buonomo AR, Moriello NS, et al. Real-World Efficacy and Safety of Pangenotypic
A
Direct-Acting Antivirals Against Hepatitis C Virus Infection. Rev Recent Clin Trials.
2019;14(3):173-182. doi:10.2174/1574887114666190306154650
37. Hézode C. Treatment of hepatitis C: Results in real life. Liver Int. Feb 2018;38 Suppl 1:21-27.
doi:10.1111/liv.13638
38. Davies A, Singh KP, Shubber Z, et al. Treatment outcomes of treatment-naïve Hepatitis C patients
co-infected with HIV: a systematic review and meta-analysis of observational cohorts. PLoS One.
2013;8(2):e55373. doi:10.1371/journal.pone.0055373
DOI: 10.1093/ofid/ofad153 1439. Micallef JM, Kaldor JM, Dore GJ. Spontaneous viral clearance following acute hepatitis C
infection: a systematic review of longitudinal studies. J Viral Hepat. Jan 2006;13(1):34-41.
doi:10.1111/j.1365-2893.2005.00651.x
40. Benova L, Mohamoud YA, Calvert C, Abu-Raddad LJ. Vertical transmission of hepatitis C virus:
systematic review and meta-analysis. Clin Infect Dis. Sep 15 2014;59(6):765-73.
doi:10.1093/cid/ciu447
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
41. Frederick T, Burian P, Terrault N, et al. Factors associated with prevalent hepatitis C infection
PT
among HIV-infected women with no reported history of injection drug use: the Women's
Interagency HIV Study (WIHS). AIDS Patient Care STDS. Nov 2009;23(11):915-23.
doi:10.1089/apc.2009.0111
RI
42. Martin NK, Vickerman P, Miners A, et al. Cost-effectiveness of hepatitis C virus antiviral
treatment for injection drug user populations. Hepatology. Jan 2012;55(1):49-57.
doi:10.1002/hep.24656
SC
43. Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N. Interferon alpha (pegylated and
non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and
economic evaluation. Health Technol Assess. Mar 2007;11(11):1-205, iii. doi:10.3310/hta11110
U
44. Walker JG, Kuchuloria T, Sergeenko D, et al. Interim effect evaluation of the hepatitis C
elimination programme in Georgia: a modelling study. The Lancet Global Health. 2020;8(2):e244-
45.
e253. doi:10.1016/s2214-109x(19)30483-8 N
van der Meer AJ, Veldt BJ, Feld JJ, et al. Association between sustained virological response and
A
all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. Jama.
Dec 26 2012;308(24):2584-93. doi:10.1001/jama.2012.144878
M
46. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C
virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational
studies. Ann Intern Med. Mar 5 2013;158(5 Pt 1):329-37. doi:10.7326/0003-4819-158-5-
D
201303050-00005
47. Arias E, Xu J. United States Life Tables, 2018. Vol. 69. 2020. National Vital Statistics Reports.
TE
48. HIV Disease Among Adult/Adolescent Males, San Diego County, 2017. 2017:22.
https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/Adult_Adol_Mal
e_Through_12312017_final.pdf
EP
49. HIV Disease Among Females in San Diego County, 2017. 2017:26.
https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/Females_Throug
h_12312017v04-11-19.pdf
CC
A
DOI: 10.1093/ofid/ofad153 15FIGURE LEGENDS
Figure 1 : Model schematic of (a) HCV disease progression and (b) stratification by age, HIV
status, and risk. PWID: people who inject drugs. MSM: men who have sex with men.
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
PT
RI
SC
U
N
A
M
D
TE
EP
CC
A
DOI: 10.1093/ofid/ofad153 16Figure 2: Annual number of new HCV infections among PLWH in San Diego County.
Scenarios shown are: (1) counterfactual continuation of pre-2018 treatment rates (29%/year, blue
solid line); (2) observed scale-up from 2018 (to 54% at UCSD and 61%/year non-UCSD, green
round dotted line); (3) county-wide scale-up to peak treatment achieved by UCSD (71%/year)
from 2021 (71%/year, yellow square dotted line); (4) as in Scenario #3 plus halved transmission
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
risk behavior from 2021 onwards (red dashed line). Mean model projections (lines), with shading
PT
denoting the 95% uncertainty interval around the observed scenario (Scenario 2).
RI
SC
U
N
A
M
D
TE
EP
CC
A
DOI: 10.1093/ofid/ofad153 17Figure 3: HCV viremia prevalence among HCV seropositive PLWH in San Diego County.
Scenarios shown are: (1) counterfactual continuation of pre-2018 treatment rates (29%/year, blue
solid line); (2) observed scale-up from 2018 (to 54% at UCSD and 61%/year non-UCSD, green
round dotted line); (3) county-wide scale-up to peak treatment achieved by UCSD (71%/year)
from 2021 (71%/year, yellow square dotted line); (4) as in Scenario #3 plus halved transmission
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
risk behavior from 2021 onwards (red dashed line). Mean model projections (lines), with shading
PT
denoting the 95% uncertainty interval around the observed scenario (Scenario 2).
RI
SC
U
N
A
M
D
TE
EP
CC
A
DOI: 10.1093/ofid/ofad153 18Figure 4: HCV reinfection rate among previously treated PLWH in San Diego County.
Mean model projections (lines) and observed data from UCSD Owen Clinic (dots and whiskers)
to which the model was not calibrated. Shading denotes the 95% uncertainty interval around the
observed scenario (Scenario 2). Scenarios shown are: (1) counterfactual continuation of pre-2018
treatment rates (29%/year, blue solid line); (2) observed scale-up from 2018 (to 54% at UCSD
Downloaded from https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofad153/7083533 by UC Davis user on 30 March 2023
and 61%/year non-UCSD, green round dotted line); (3) county-wide scale-up to peak treatment
PT
achieved by UCSD (71%/year) from 2021 (71%/year, yellow square dotted line); (4) as in
Scenario #3 plus halved transmission risk behavior from 2021 onwards (red dashed line).
RI
SC
U
N
A
M
D
TE
EP
CC
A
DOI: 10.1093/ofid/ofad153 19You can also read