The costs of scaling up HIV and syphilis testing in low- and middle-income countries: a systematic review
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Health Policy and Planning, 36, 2021, 939–954
doi: 10.1093/heapol/czab030
Advance Access Publication Date: 9 March 2021
Review
The costs of scaling up HIV and syphilis
testing in low- and middle-income
countries: a systematic review
Rabiah al Adawiyah1,*, Olga PM Saweri1,2, David C Boettiger1,
Tanya L Applegate1, Ari Probandari3, Rebecca Guy1, Lorna Guinness4,5,
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
and Virginia Wiseman1,4
1
The Kirby Institute, University New South Wales, High St, Kensington 2052, New South Wales, Australia,
2
Population Health and Demography, Papua New Guinea Institute of Medical Research, PO Box 60 Homate Street,
Goroka, Papua New Guinea, 3Department of Public Health, Faculty of Medicine, Universitas Sebelas Maret, Jl. Ir.
Sutami 36A. Surakarta, 57126, Indonesia, 4London School of Hygiene and Tropical Medicine, 15-17 Tavistock Place,
London WC1H 9SH, UK, 5Centre for Global DevelopmentEurope, Great Peter House, Great College St, London
SW1P 3SE, UK
*Corresponding author. The Kirby Institute, Wallace Wurth Building, Level 6, High St., Kensington, NSW 2052, Australia.
E-mail: radawiyah@kirby.unsw.edu.au
Accepted on 16 February 2021
Abstract
Around two-thirds of all new HIV infections and 90% of syphilis cases occur in low- and
middle-income countries (LMICs). Testing is a key strategy for the prevention and treatment of HIV
and syphilis. Decision-makers in LMICs face considerable uncertainties about the costs of scaling
up HIV and syphilis testing. This paper synthesizes economic evidence on the costs of scaling up
HIV and syphilis testing interventions in LMICs and evidence on how costs change with the scale of
delivery. We systematically searched multiple databases (Medline, Econlit, Embase, EMCARE,
CINAHL, Global Health and the NHS Economic Evaluation Database) for peer-reviewed studies
examining the costs of scaling up HIV and syphilis testing in LMICs. Thirty-five eligible studies
were identified from 4869 unique citations. Most studies were conducted in Sub-Saharan Africa
(N ¼ 17) and most explored the costs of rapid HIV in facilities targeted the general population
(N ¼ 19). Only two studies focused on syphilis testing. Seventeen studies were cost analyses,
17 were cost-effectiveness analyses and 1 was cost–benefit analysis of HIV or syphilis testing.
Most studies took a modelling approach (N ¼ 25) and assumed costs increased linearly with scale.
Ten studies examined cost efficiencies associated with scale, most reporting short-run economies
of scale. Important drivers of the costs of scaling up included testing uptake and the price of test
kits. The ‘true’ cost of scaling up testing is likely to be masked by the use of short-term decision
frameworks, linear unit-cost projections (i.e. multiplying an average cost by a factor reflecting
activity at a larger scale) and availability of health system capacity and infrastructure to supervise
and support scale up. Cost data need to be routinely collected alongside other monitoring
indicators as HIV and syphilis testing continues to be scaled up in LMICs.
Keywords: Scales, costs, review, healthcare costs
C The Author(s) 2021. Published by Oxford University Press in association with The London School of Hygiene and Tropical Medicine.
V
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unre-
stricted reuse, distribution, and reproduction in any medium, provided the original work is properly cited. 939940 Health Policy and Planning, 2021, Vol. 36, No. 6
Key Messages
• Scale is an important driver in determining the costs of HIV and syphilis testing programmes in resource-constrained
health systems
• Common methodological assumptions including short-run framework, linear unit cost projections and the availability of
health system capacity and infrastructure to supervise expanded delivery currently mask the ‘true’ costs of scaling up
HIV and syphilis testing in low- and middle-income countries.
• Financing and budgeting for the scale up of HIV and syphilis testing would benefit from the monitoring of costs across
delivery sites over multiple timepoints.
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
Introduction Scaling up, broadly defined as the ‘deliberate effort to increase
the impact of successfully tested health innovations, so as to benefit
HIV and syphilis infections are major public health problems world-
more people’ (Simmons and Shiffman, 2007), has a direct impact on
wide (Hook, 2017; Joint United Nations Programme on HIV/AIDS,
costs. Scaling up decentralized tests, outside of laboratories, requires
2018). In 2017, there were 1.8 million new HIV infections well
multiple systems to be considered other than the test itself, such as
above the targets set by the World Health Organization (WHO) of
training, quality management, stock managing, reporting and theseHealth Policy and Planning, 2021, Vol. 36, No. 6 941
the provider through a reduction in the number of visits and loss to Lending Groups classification in 2019 (World Bank, 2019); and
follow-up (Mabey et al., 2012; Fleming et al., 2017). Levels of test- (iv) were full research papers (reviews, editorials, letters and confer-
ing may also be lower in less densely populated rural areas while the ence papers were excluded). No date or language restrictions were
costs of delivery (e.g. cost of the test or transport) can be higher applied.
(Shelley et al., 2015).
Currently, decision-makers in LMICs lack a consolidated Study selection
evidence base from which to understand the cost implications of The search results were imported into an Endnote library and were
scaling up HIV and syphilis testing. Three reviews of economic stud- independently screened by two reviewers based on their titles and
ies evaluating the costs of scaling up of health interventions in abstracts. Both reviewers screened the first 10% of articles
LMICs (Kumaranayake et al., 2001; Johns and Torres, 2005) and (N ¼ 487) against the eligibility criteria to determine the inter-rater
HIV interventions specifically (Kumaranayake, 2008) have been reliability of the reviews. Agreement was assessed using a simple
published, each over a decade old. Each review found evidence of kappa analysis (McHugh, 2012) and near perfect agreement (kappa
economies of scale, recommending that future work take scale and score of 0.96) was achieved and subsequently the screening contin-
other cost drivers into account when estimating the costs of scaling ued with a single reviewer (RA) (McHugh, 2012; Wiseman et al.,
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
up (Kumaranayake et al., 2001; Johns and Torres, 2005; 2016). Two reviewers read the full text of the selected studies and
Kumaranayake, 2008). These reviews also identified best practice any disagreements regarding eligibility were resolved by consulting a
recommendations for measuring economies of scale and the costs of third reviewer. Reasons for exclusion were recorded. Scopus-
scaling up public health interventions in LMICs including: ensuring Elsevier was used to track the reference lists in the final papers to
sufficient and representative sample sizes to capture differences in identify any additional relevant studies.
cost characteristics across sites; distinguishing between and measur-
ing both fixed and variable costs; and using appropriate analytical Data extraction and appraisal
methods, e.g. econometric estimation. None of the reviews capture The variables used to describe the different studies in this review are
the recent proliferation of studies assessing the impact of rapid tests shown in Table 1. All data were extracted by two reviewers and all
for HIV and syphilis. In this paper, we systematically review the cur- differences were again resolved by a third reviewer. A narrative syn-
rent evidence on the costs of scaling up HIV and syphilis testing in thesis describing the included studies and their conclusions was con-
LMICs, with a focus on key findings, quality and methodological sidered to be the most appropriate approach to synthesizing the
issues. findings of the studies (Ryan and Cochrane Consumer and
Communication Review Group, 2013). The synthesis from data ex-
traction is presented according to the characteristic of studies
Methods
included, type of cost studies undertaken, methods to assess cost and
Search strategy impact of scale on costs.
The review team defined the search terms according to four domains The reporting and methodological quality of studies estimating
based on the aims of this review. The four domains included: infec- cost at scale were assessed using a checklist designed for this review
tious disease; screening and testing; economics; and LMICs. Despite (Table 2). The checklist was developed in consultation with global
the frequent use of the term ‘scaling up’ in international health, in experts in the development of existing checklists for costing exer-
practice it has been interpreted in many different ways (Mangham cises and include a checklist for good practice in the economic evalu-
and Hanson, 2010). Search terms relating to ‘scaling up’ were not ation of health interventions (Husereau et al., 2013); checklists for
included in the initial screening, rather an extensive manual screen- appraising priority setting studies in the health sector (Peacock
ing was conducted to filter articles according to the eligibility crite- et al., 2007; Wiseman et al., 2016); Global Health Cost Consortium
ria listed below. The search terms were applied in six databases: guiding principles (Vassall et al., 2017); and best practice guidelines
Medline via Ovid; Econlit via Proquest; Embase via Ovid; for calculating the costs of scaling up health interventions (Johns
EMCARE via EBSCO; CINAHL via EBSCO; and Global Health via and Baltussen, 2004; Johns and Torres, 2005; Kumaranayake,
Ovid. The search strategy used medical subject headings for 2008). Three reviewers independently appraised the studies against
Medline and comparable terms for the other databases (complete this checklist, and any disagreements were resolved by consulting
Medline search terms can be found in Supplementary Appendix S1). two additional reviewers.
The NHS Economic Evaluation Database, a bibliographic record of
published health technology assessments, was also searched using
the same search strategy. A librarian from the authors institute was Results
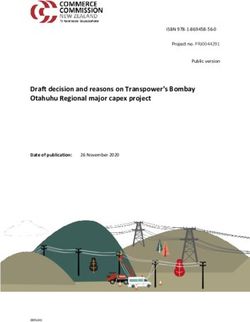
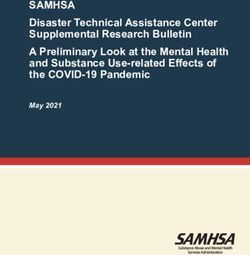
consulted on the search strategy including the selection of domains We identified 35 eligible studies from 4869 unique citations as
and search terms. The systematic review followed the Preferred shown in the PRISMA flow diagram (see Figure 1).
Reporting Items for Systematic Reviews and Meta-Analyses
(PRISMA) guidelines (Moher et al., 2009) and is registered on the Characteristics of the studies included
International Prospective Register of Systematic Review Table 3 summarizes the characteristics of 35 included studies in this
(PROSPERO), identification number CRD42018103890. review. The majority of studies were conducted in Sub-Saharan
Africa (N ¼ 17), published after 2010 (N ¼ 24) and focused on HIV
Eligibility criteria testing (N ¼ 33). Only two studies examined the costs of scaling up
Studies were eligible for this review if they: (i) measured the costs of syphilis testing (Schackman et al., 2007; Shelley et al., 2015). Most
scaling up HIV and/or syphilis testing at scale using empirical data, of the HIV studies involved facility-based testing using rapid tests in
modelling or a hybrid of these approaches; (ii) focused on HIV and/ the general adult population (N ¼ 19) or among pregnant women
or syphilis testing to identify new infections; (iii) were conducted in (N ¼ 6), while all syphilis studies were focused on pregnant women
an LMICs, defined according to the World Bank Country and (N ¼ 2). Only three studies explored the use of HIV self-testing in942 Health Policy and Planning, 2021, Vol. 36, No. 6
Table 1 List of data extraction variables
Study characteristics
Intervention(s) Type of HIV and/or syphilis testing activity or programme
Country Location of study
Study population Group targeted by intervention(s)
Setting Service through which the intervention is delivered (e.g. health centre, hospital) and sector (e.g. public/private)
Time horizon The duration over which costs and/or consequences are calculated
Study design Randomized controlled trial, cross-sectional, cohort, case–control, modelling
Type of economic analysis Cost analysis, cost-effectiveness, cost-utility or cost–benefit analysis. Includes ratio used (e.g. cost per DALY
(and ratio if applicable) averted)
Data source(s) Primary data collection, expert/stakeholder opinion, published data or literature or combination of those
Analytical approach to measure Econometric, empirical, modelling or a hybrid of these approaches (Kumaranayake, 2008)
costs at scale
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
Costs of scaling up
Definition of scaling up As described by authors
Year (costs) Year of currency values presented (e.g. 2018 dollars)
Unit(s) of output Choice of output measure (e.g. number of clients tested, number of facilities with testing available)
Sample size Total number of, e.g facilities, individuals, tests
Timeframe for decision Short run (fixed inputs cannot be changed) and long run (all inputs can be changed) (Kumaranayake, 2008)
Cost categories Categorization of costs as defined by author(s)
Economies/diseconomies of scale How costs changed with scale of output and by how much.
Empirical results Specific findings related to the costs of scaling up (e.g. coefficients of scale)
Key drivers of costs identified Key drivers of the costs of scaling up (e.g. geography, population sub-group, type of providers)
Table 2 List of appraisal checklist questions
Standard of reporting costs
#1 Was the research question(s) well defined? (Yes/No/Partially addressed)
#2 Was the perspective of the cost estimation clearly stated? (Yes/No/Partially addressed)
#3 Was the time horizon of sufficient length to capture the costs of the intervention at scale? (Yes/No/Partially addressed)
#4 Did the study include relevant inputs in the cost estimation (i.e. consumables, human resour- (Yes/No/Partially addressed)
ces, equipment and infrastructure, and managerial practice) (Johns and Torres, 2005)?
#5 Were the methods for estimating the quantities of inputs clearly described? (Yes/No/Partially addressed)
#6 Did the study clearly report the selection of data source(s) for the ‘units’ estimated in the cost (Yes/No/Partially addressed)
per unit?
#7 Was the sample size determined by the precision required for costing? If not, was the sample (Yes/No/Partially addressed)
designed to be an accurate representation of the study population?
#8 Did the study use relevant and appropriate discount, inflation, and currency conversion rates (Yes/No/Partially addressed)
to enable cost adjustment over setting and time?
#9 Did the study perform sensitivity analyses to characterize uncertainty associated with cost (Yes/No/Partially addressed)
estimates?
#10 Were cost estimates reported and communicated in a clear and transparent way? (Yes/No/Partially addressed)
Methodological quality of estimating costs at scale
#11 Were average costs estimated for different levels of scale; and if so, did the study account for (Yes/No/Partially addressed)
changes in input costs associated with increasing scale of the intervention?
#12 Did the study quantify the relationship between average cost and scale? (Yes/No/Partially addressed)
#13 Were fixed and variable costs analysed separately as scale increased? (Yes/No/Partially addressed)
#14 Were factors other than scale, that could impact on cost, accounted for in the analysis? (e.g. (Yes/No/Partially addressed)
scope, geography, target population, type of provider)
the community and general population (N ¼ 3) (Cambiano et al., distributed (N ¼ 2) or an expansion of a geographical catchment
2015; McCreesh et al., 2017; Mangenah et al., 2019). Four studies area (N ¼ 1).
evaluated community-based testing (Tromp et al., 2013; McCreesh
et al., 2017; Cherutich et al., 2018; Mangenah et al., 2019),
only one on home-based testing (Sharma et al., 2016), one on mobile Type of cost studies undertaken
testing (Verstraaten et al., 2017) and one in the prison (Nelwan Around half of the studies undertook a cost analysis (N ¼ 17) and an-
et al., 2016). ‘Scale up’ was most commonly defined in terms of other half conducted a cost-effectiveness analysis (CEA) (N ¼ 17)
an increase in population coverage (N ¼ 32) with the remaining typically comparing facility-based HIV testing using rapid tests with
studies defining it as an increase in the number of test kits laboratory-based testing, with two of those complemented theirHealth Policy and Planning, 2021, Vol. 36, No. 6 943
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
Figure 1 PRISMA flow diagram
CEAs with budget impact analysis (BIA) (Cherutich et al., 2018; economies of scale were possible (i.e. confirmed through a negative
Luong Nguyen et al., 2018). One cost–benefit analysis of HIV testing coefficient on the scale variable), with coefficient of scale is ranging
in pregnant women was reported (Kumar et al., 2006). Around half from 0.18 to 0.83 (Dandona et al., 2005; McConnel et al., 2005;
of the studies relied on primary data (N ¼ 18) and the remaining half Galárraga et al., 2017; Mwenge et al., 2017; Bautista-Arredondo
used a combination of published evidence and expert opinion et al., 2018b; Mangenah et al., 2019). The main driver of these
(N ¼ 17). Most studies took a modelling approach to the estimation economies of scale is the distribution of fixed cost to a larger num-
of the costs of scaling up testing for HIV and/or syphilis (N ¼ 25). ber of patients or outputs. The remaining four studies took an
empirical-based approach whereby the relationship between scale
Methods to assess cost according to scale and cost was based on observations of the actual cost at different
Of the 35 eligible studies, 10 measured how costs varied with scale levels of scale (Forsythe, 2002; McConnel et al., 2005; Dandona
(see Table 4). All other studies used a constant average cost assump- et al., 2008a,b; Shelley et al., 2015). Three of the four studies
tion (i.e. no adjustment for scale) to estimate resource requirements showed that the costs of screening per person decreased as scale
of scaling up, implicitly assuming that costs were indifferent to scale increased (Forsythe, 2002; McConnel et al., 2005; Dandona et al.,
and other potential cost drivers. Of the 10 studies measuring the im- 2008a,b). One empirical study reported an increase in the average
pact of scale on costs, six conducted an econometric analysis by esti- cost per client tested as the intervention was rolled out to new sites,
mating the relationship between cost and cost determinants using which was attributed to several factors including higher rapid point-
regression analysis and remaining four are empirical studies of-care syphilis tests prices and lower rapid syphilis testing (RST)
(Forsythe, 2002; McConnel et al., 2005; Dandona et al., 2008a,b; uptake in the targeted population (Shelley et al., 2015).
Shelley et al., 2015; Galárraga et al., 2017; Mwenge et al., 2017;
Bautista-Arredondo et al., 2018a; Mangenah et al., 2019). Fixed vs variable costs
All studies in this review were based on a short-run decision frame-
Impact of scale on costs work, during which the amount of fixed inputs could not be easily
The six studies measuring the impact of scale on costs found that the varied. The costs of scaling up HIV and syphilis testing tended to be
average cost per person tested (most commonly for HIV using a narrowly defined as the cost of the test, personnel and associated
rapid test) decreased as scale increased, demonstrating that consumables such as gloves and cotton swabs (N ¼ 18). Only 10 outTable 3 Studies of the cost of scaling up HIV and syphilis testing
944
Study Intervention(s) Country Study population Setting Time horizon Study design Type of economic Data source (s) Analytical ap-
analysis (and ratio proach to meas-
if applicable) ure scale
#1 (Shelley et al., Syphilis testing/RST/POC Zambia Pregnant women (age ANC clinic 5 months Cross-sectional Cost analysis Primary data Empirical
2015) not specified) study collection
#2 (Schackman Syphilis testing, comparing: Haiti Pregnant women (age ANC clinic Not specified Modelling Cost-effectiveness Published lit- Modelling
et al., 2007) #1 Syndromic surveillance/not not specified) analysis erature/data
POC
#2 RPR for syphilis/not POC
#3 RST/POC
#3 (Bautista- HIV voluntary and provider-initi- Nigeria General population Health facility 6 months Cross-sectional Cost analysis Primary data Econometric
Arredondo et al., ated counselling and testing/ (age not specified) study collection
2018a,b) HIV rapid test/not POC
#4 (Dandona et al., HIV voluntary counselling and India General population Health facility 1 year Cross-sectional Cost analysis Primary data Empirical
2008a,b) testing/HIV rapid test/not POC (age not specified) study collection
#5 (Galárraga HIV testing and counselling/HIV Kenya General population Health facility 22 months Cross-sectional Cost analysis Primary data Econometric
et al., 2017) rapid test/not POC (age not specified) study collection
#6 (Hontelez et al., HIV testing/type of test not speci- South Africa General population Not specified Lifetime Modelling Cost-effectiveness Published lit- Modelling
2013) fied/not POC, comparing: (aged 15–65 years) analysis erature/data
#1 ART at CD4 count 350 cells/
ml
#2 Universal testing and treatment
#7 (Ishikawa et al., HIV testing/HIV rapid test/not Namibia, Kenya, Pregnant women ANC clinic 20 years Modelling Cost-effectiveness Published lit- Modelling
2016) POC, comparing: Haiti and (aged 15–49 years analysis erature/data
#1 The current coverage Vietnam old)
#2 A focused approach
#3 A universal approach
#8 (McConnel HIV rapid voluntary counselling South Africa General population VCT clinic 1 year Cross-sectional Cost analysis Primary data Empirical
et al., 2005) and testing/HIV rapid test/POC (age not specified) study collection
#9 (Ahaibwe and HIV testing/HIV rapid test/not Uganda General population Stand alone, integrated Lifetime Modelling Cost-effectiveness Published lit- Modelling
Kasirye, 2013) POC, comparing: (adult 15–49 years) w/health facility, analysis erature/data
#1 The current coverage non- health facility
#2 100% coverage of adult and mobile VCT
population services
#10 (Alsallaq et al., HIV testing/HIV rapid test/not Kenya Youth population Health facility 20 years Modelling Cost-effectiveness Published lit- Modelling
2017) POC, comparing: (aged 15–24 years) analysis erature/data
#1 HIV strategies focusing on
youth (15–24 years old)
#2 HIV strategies focusing on
adults (15þ years)
#11 (Cambiano HIV testing/HIV rapid test/not Zimbabwe General population Not specified 20 years Modelling Cost-effectiveness Published lit- Modelling
et al., 2015) POC, comparing: (aged 15–65 years analysis erature/data
#1 Provider-delivered HIV testing old)
and counselling
#2 HIV self-testing
#12 (Cherutich aPS HIV testing/rapid HIV test/not Kenya General population Health facility and 5 years Modelling Cost-effectiveness Published lit- Modelling
et al., 2018) POC, comparing: (age not specified) community-based analysis and erature/data
#1 Current coverage at 5% health services budget impact
#2 Scale up to reach coverage of analysis
50%
Health Policy and Planning, 2021, Vol. 36, No. 6
(continued)
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022Table 3 (continued)
Study Intervention(s) Country Study population Setting Time horizon Study design Type of economic Data source (s) Analytical ap-
analysis (and ratio proach to meas-
if applicable) ure scale
#13 (Mwenge HIV voluntary and provider-initi- Malawi, Zambia General population Health facility 1 year Cross-sectional Cost analysis Primary data Econometric
et al., 2017) ated counselling and testing/ and Zimbabwe (aged 15–49 years) study collection
rapid HIV test/not POC
#14 (Stuart et al., HIV testing/type of test not speci- South Africa General population Not specified 30 years Modelling Cost analysis Published lit- Modelling
2018) fied/not POC (age not specified) erature/data
#15 (Tromp et al., HIV voluntary counselling and Indonesia Key populations Community-based 20 years Modelling Cost-effectiveness Published lit- Modelling
2013) testing/HIV rapid test/not POC, (FSWs, IDUs, VCT clinic analysis erature/data
comparing: higher-risk MSM,
#1 Current practice transgender, pris-
#2 Scaling up to reach coverage oner, clients of
80% FSWs and partner
IDUs) (age not
specified)
#16 (Zhuang et al., HIV testing and treatment/type of China MSM (age not Health facility 20 years Modelling Cost-effectiveness Published lit- Modelling
Health Policy and Planning, 2021, Vol. 36, No. 6
2018) test not specified/not POC, specified) analysis erature/data
comparing:
#1 Current strategy
#2 Reached 90–90–90 target by
2020
# Reached 90–90–90 target by
2025
#17 (Dandona HIV counselling and testing/HIV India Pregnant women (age Hospital and commu- 1 year Cross-sectional Cost analysis Primary data Econometric
et al., 2008a,b) rapid test/not POC not specified) nity health centre study collection
#18 (Dandona HIV counselling and testing/HIV India General population VCT clinics 1 year Cross-sectional Cost analysis Primary data Econometric
et al., 2005) rapid test/not POC (age not specified) study collection
#19 (Forsythe, HIV voluntary counselling and Kenya General population Health facility A year Cross-sectional Cost analysis Primary data Empirical
2002) testing/serial of HIV rapid test- (age not specified) study collection
ing/POC
#20 (Granich et al., HIV testing/type of test not speci- South Africa General population Not specified 42 years Modelling Cost-effectiveness Published lit- Modelling
2009) fied/not POC, comparing: (age not specified) analysis erature/data
#1 Reference scenario
#2 Universal voluntary HIV test-
ing and immediate ART
#21 (Kasymova, HIV testing and counselling/serial Tajikistan Youth population Youth friendly health 2 years Cross-sectional Cost analysis Primary data Modelling
Johns and of HIV rapid test/not POC (aged 15–25 years) services study collection
Sharipova, 2009)
#22 (Kato et al., HIV testing type of test not speci- Vietnam Key population: Health facility 50 years Modelling Cost effectiveness Published lit- Modelling
2013) fied/not POC, comparing: PWID, MSM, analysis erature/data
#1 Reference scenario FSWs, MCF, IDU
#2 Targeted PTIT scenario and low-risk
#3 Universal PTIT scenario women (age not
specified)
#23 (Kumar et al., HIV testing and counselling/rapid India Pregnant women (age ANC clinic Lifetime Modelling Cost–benefit Published lit- Modelling
2006) HIV test/not POC, comparing: not specified) analysis erature/data
#1 A universal testing
#2 A targeted testing
(continued)
945
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022Table 3 (continued)
946
Study Intervention(s) Country Study population Setting Time horizon Study design Type of economic Data source (s) Analytical ap-
analysis (and ratio proach to meas-
if applicable) ure scale
#24 (Dandona HIV voluntary counselling and India General population VCT clinic 1 year Cross-sectional Cost analysis Primary data Modelling
et al., 2009) testing/HIV rapid test/not POC (age not specified) study collection
#25 (Mangenah HIVST/HIV rapid testing/not POC Malawi, Zambia, General population Community based dis- 1 year Cross-sectional Cost analysis Primary data Econometric
et al., 2019) and Zimbabwe (aged 15–59 years) tributing agent study collection
#26 (McCreesh HIV self-testing/HIV rapid test/not Uganda General population Door-to-door commu- 15 years Modelling Cost-effectiveness Published lit- Modelling
et al., 2017) POC, comparing (aged under nity-based analysis erature/data
#1 Current coverage 51 years)
#2 Increased HIV testing
(doubled)
#27 (Minh et al., HIV voluntary counselling and Vietnam General population Facility based and free- 4 months Costing study Cost analysis Primary data Modelling
2012) testing/type of test not specified/ (age not specified) standing VCT clinic collection
not POC
#28 (Sharma et al., HIV home-based partner educa- Kenya Partner of pregnant Home based 10 years Modelling along- Cost-effectiveness Primary data Modelling
2016) tion and testing (HOPE)/HIV women (aged 0– side random- analysis collection
rapid test/not POC, comparing: 59 years) ized controlled
#1 Standard care (facility-based trial
HIV testing)
#2 Adding HOPE to standard care
#29 (Nelwan et al., HIV testing and counselling/HIV Indonesia Prisoner (age not Outpatient clinic in 3 years Case–control Cost analysis Primary data Modelling
2016) rapid test/not POC specified) prison study collection
#30 (Luong HIV voluntary counselling and Kenya General population Health facility 20 years Modelling Cost-effectiveness Published lit- Modelling
Nguyen et al., testing/HIV rapid test/not POC, (age not specified) analysis and erature/data
2018) comparing: budget impact
#1 Current testing coverage of analysis
62%
#2 Scale up testing coverage to
90%
#31 (Rely, 2003) HIV counselling and testing/HIV Mexico Pregnant women (age Health facility Lifetime Modelling Cost-effectiveness Published lit- Modelling
rapid test/not POC, comparing: not specified) analysis erature/data
#1 Status quo (with 4% testing
coverage)
#2 Increase in coverage to 85%
#32 (Tchuenche VEID/DNA-PCR/not POC Lesotho HIV-exposed infants Health facility 1 year Retrospective ob- Cost analysis Primary data Modelling
et al., 2018) (0–2 weeks) servational collection
study
#33 (Verstraaten HIV voluntary counselling and Indonesia FSWs (age not Mobile VCT services 1 year Cost analysis Primary data Modelling
et al., 2017) testing/HIV rapid test/not POC specified) collection
#34 (Zang et al., HIV testing, comparing: China General population Hospital 1, 5 and 25 Modelling Cost-effectiveness Published lit- Modelling
2016) #1 One4All (include testing, coun- (aged 15–64 years years analysis along- erature/data
selling, CD4 results, and viral old) side clustered
load)/HIV rapid test/POC randomized trial
#2 Standard care/HIV rapid testþ
western blot confirmatory test/
POC
(continued)
Health Policy and Planning, 2021, Vol. 36, No. 6
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022Health Policy and Planning, 2021, Vol. 36, No. 6 947
proach to meas-
diagnostic testing using DNA sequencing; HIVST, HIV self-testing; IDUs: injected drug users; MCF, male clients of female sex workers; POC: point-of-care; PTIT, HIV periodic testing and immediate treatment; PWID, people
therapy will have viral suppression. ANC, antenatal care; aPS, assisted partner service; ART, antiretroviral treatment; CD4, cluster of differentiation 4; DNA-PCR, deoxyribonucleic acid-polymerase chain reaction, a molecular
90–90–90 target: 90% of all people living with HIV will know their HIV status, 90% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy and 90% of all people receiving antiretroviral
of 35 included studies separated the fixed and variable component
Analytical ap-
ure scale
of costs. A small number of studies (N ¼ 8) attempted to include
Modelling
more cost items such as the costs of educational materials, monitor-
ing and supervision or waste management. Few studies (N ¼ 4) con-
sidered the costs of managing the scaling up process including the
costs of quality management and investment in procuring new
Data source (s)
Primary data
collection
equipment. In addition to scale, other key drivers of cost included
availability of transport infrastructure, variation in the price of local
goods (e.g. test kits, medicines, fuel), costs and frequency of super-
visory trips and the recruitment and training of health personnel, es-
pecially in remote areas.
analysis (and ratio
Type of economic
Cost-effectiveness
if applicable)
Quality of studies included
analysis
Table 5 summarizes the results of the appraisal. Most studies clearly
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
reported the research question(s), perspective taken and the time
horizon for the analysis (N ¼ 29). No study justified their sample
size for the costing and around half undertook a sensitivity analysis
Study design
for major cost inputs (N ¼ 19). There were widespread gaps in the
Modelling
methodological quality of estimating costs at scale. Specifically, less
than half of the studies in this review estimated average costs at dif-
ferent levels of scale (N ¼ 6), measured the relationship between
average costs and scale (N ¼ 9) or separated fixed and variable costs
Time horizon
(N ¼ 10), which are all necessary to accurately measure economies
3-,5-and 10-
or diseconomies of scale (Kumaranayake, 2008).
years
Discussion
with injected drug; RPR, rapid plasma regain; VCT, HIV voluntary counselling and testing; VEID, very early infant diagnosis.
To expand access to HIV and syphilis testing and reach elimination
targets, successful small-scale programmes need to cover broader
Setting
Health facility
populations in LMICs. The availability of reliable and detailed in-
formation on the resources required to do this is a key determinant
of success (Johns and Torres, 2005; Kumaranayake, 2008; World
Health Organization and ExpandNet, 2009; Mangham and
Hanson, 2010). This review validates that scale is an important
Study population
driver in determining the costs of HIV and syphilis testing pro-
grammes in resource-constrained health systems. It also reveals the
MSM (age not
specified)
potential for economies of scale (i.e. a reduction in average costs as
the number of people tested increases) at least in the short run when
structural changes to health systems (e.g. training, quality manage-
ment and stock management) necessary for the large scale delivery
of testing have not yet been undertaken.
Country
Despite syphilis testing being widely recommended for use in
LMICs, particularly in pregnancy (Newman et al., 2013; Storey
Thailand
et al., 2019), only two studies explored the costs of scaling up syph-
ilis testing. Recent pilot studies have demonstrated the cost-
effectiveness of HIV and syphilis screening using a dual rapid test
HIV testing/type of test not speci-
over single HIV and syphilis tests or HIV testing alone (Bristow
#2 Reach universal coverage by
#3 Reach universal coverage by
#4 Reach universal coverage by
et al., 2016). It has been argued that dual tests for HIV and syphilis
fied/not POC, comparing
Intervention(s)
may potentially contribute to economies of scale and scope (associ-
ate with the sharing of fixed costs across activities) in terms of start-
up, training, quality management, supervision and monitoring while
#1 Status quo
also serving to promote syphilis testing, which is lagging well behind
HIV testing in many LMICs (Bristow et al., 2016; Taylor et al.,
2015
2017
2022
2017). While there were many studies that found community-based
strategies are effective in increasing uptake of testing (Asiimwe
Table 3 (continued)
et al., 2017; Ahmed et al., 2018), this review revealed a lack of at-
#35 (Zhang et al.,
tention paid to the economic impact of scaling up these strategies.
Many key populations have expressed a strong preference for
community-based testing, which is seen as less stigmatizing and
2015)
Study
more accessible (Suthar et al., 2013). Despite the growing import-
ance of the private sector in the delivery of HIV and syphilis care inTable 4 Studies that report on how costs of testing change with scale
948
Ref Definition of scal- Year (costs) Units of Sample size Timeframe Authors’ categorization of costs Findings related Results Key drivers of costs identifieda
ing up output for decision to scale and
cost
#1 (Shelley et al., Increase in geo- 2012 Number of Pilot: 5 facilities in Short run Incremental costs Diseconomies Average unit cost Geography and infrastructure: central
2015) graphic coverage facilities two districts Start-up costs: personnel, per diems, of scale per woman level supervision and transport costs
Scale up: 4 facilities conference hire, training equipment tested USD 3.19 Managing the process of scaling up:
in two districts and supplies, and vehicle transport (pilot) and USD quality assurance/control
Capital costs: vehicles and computers 11.16 (scale up) Other: higher RST kit cost and lower
Recurrent costs: personnel, supplies RST uptake
(syphilis testing, shared supplies,
treatment), vehicle fuel and main-
tenance, quality assurance/control
and supervision
#3 (Bautista- Increase in number 2013 Number of 414 540 clients in Short run Economic cost Economies of Average unit cost Managing the process of scaling up:
Arredondo et al., of clients receiv- clients 141 HIV testing Personnel: staff salaries scale per client tested central-level financial decision, and
2018a,b) ing a test and counselling Recurrent inputs and services: HIV USD 30 task-shifting (i.e. reorganizing
facility testing kit and treatment Coefficient of scaleb human resource to delegate some
Capital: equipment (i.e. PCR machine, ¼ 0.44 tasks to less specialized health
CD4 testing machine, refrigerator) workers)
and vehicles Fixed costs: the distribution of fixed
Training: Incl. opportunity costs of cost to a larger number of people
staff involved Other: services integration, external
supervision, and different level of
service delivery
#4 (Dandona et al., Increase in number 2006 Number of Pilot: 32 413 clients Short run Economic cost Economies of Average unit cost Fixed costs: the distribution of fixed
2008a,b) of clients receiv- clients Scale up: 66 445 Personnel: staff payroll scale per client tested cost to a larger number of people
ing a test clients Recurrent goods: HIV test kits, con- USD 5.46 (pilot)
17 hospital based doms, IEC (information, education, and USD 3.3
VCT clinic and communication) materials, (scale up)
medical supplies, and stationery
Recurrent services: staff training, local
travel, building maintenance and
utilities
Capital goods: furniture, medical and
administrative equipment
Building: based on area-specific rentals
#5 (Galárraga Increase in number 2011 Number of 237 160 clients in Short run Economic cost Economies of Average cost per Managing the process of scaling up:
et al., 2017) of clients receiv- clients 56 sites HTC Personnel: staff and volunteer time scale client tested is task shifting (i.e. using qualified
ing a test per year clinic Recurrent supplies: HIV test kits, USD 7 lower level staff instead of
b
condoms Coefficient of scale physicians)
Recurrent operating costs: utilities and ¼ 0.18 Fixed costs: the distribution of fixed
maintenance cost to a larger number of people
Capital goods: equipment—purchase,
maintenance, and replacement
Other inputs: administration, supervi-
sion, training
(continued)
Health Policy and Planning, 2021, Vol. 36, No. 6
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022Table 4 (continued)
Ref Definition of scal- Year (costs) Units of Sample size Timeframe Authors’ categorization of costs Findings related Results Key drivers of costs identifieda
ing up output for decision to scale and
cost
#8 (McConnel Increase in number 2003 Number of 693 clients Short run Economic and financial costs Economies of Average cost per Fixed costs: the distribution of fixed
et al., 2005) of clients receiv- clients Personnel: Staff and volunteer time scale VCT client tested cost to a larger number of people
ing a test Other recurrent goods and services: is USD 161.03
Staff and community training, cam- (pilot) and USD
paign and publicity materials, util- 53.02 (scale up)
ities, stationary and donated HIV
test kits, and condoms
Capital: Office equipment and building
mortgage
#13 (Mwenge Increase in the total 2016 Number of A total of 7735 test Short run Economic and financial costs Economies of Average cost per Fixed costs: the distribution of fixed
et al., 2017) number of test test kits kits distributed Capital costs: Buildings and storage, scale client tested is cost to a larger number of people
kits distributed in 54 HIV testing equipment, and vehicles USD 4.92 Personnel: staff salaries and training
services units Recurrent costs: Personnel, training, (Malawi), USD Other: service integration and lack of
HIV testing commodities, general 4.24 (Zambia) demand
Health Policy and Planning, 2021, Vol. 36, No. 6
supplies, facility-level operation, and USD 8.79
and waste management (Zimbabwe)
Overhead costs: facility level and HTS Coefficient of scaleb
centre-level ¼ not provided
#17 (Dandona Increase in number 2006 Number of 125 073 clients in Short run Economic and financial costs Economies of Average cost per Fixed costs: the distribution of fixed
et al., 2008a,b) of clients receiv- clients 16 PMTCT Rental: building and land scale client tested is cost to a larger number of people
ing a test centres Personnel: Staff time USD 4.29 (pilot)
Capital goods: Furniture, medical and and USD 1.61
administrative equipment (scale up)
Recurrent goods: HIV test kits,
Nevirapine, disposable supplies, sta-
tionary and miscellaneous item
Recurrent services: Staff training, build-
ing maintenance and utilities, and
waste disposal
#18 (Dandona Increase in number 2003 Number of 32 413 clients in 17 Short run Economic cost Economies of Average cost per Fixed costs: the distribution of fixed
et al., 2005) of clients receiv- clients VCT clinics Salaries: staff and volunteer time scale client tested is cost to a larger number of people
ing a test Rentals: building and land USD 5.46 Other: lack of demand
Capital goods: Furniture and medical Coefficient of scaleb
equipment ¼ 0.83
Recurrent goods: HIV test kits, male
condoms, IEC material, recurrent
medical supplies, and stationery
Recurrent services: Staff training, build-
ing maintenance and utilities, and
waste disposal
#19 (Forsythe Increase in number 1999 Number of 519 clients in three Short run Economic costs Economies of Average cost per Fixed costs: the distribution of fixed
2002) of clients receiv- clients health centres Labour costs: staff salaries scale client tested is cost to a larger number of people
ing a test Materials and medication: HIV test USD 16
b
kits, needles, syringes, and gloves Coefficient of scale
Equipment and furniture: no detail ¼ not provided
provided
Property and utilities: building rental
value
949
(continued)
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022950 Health Policy and Planning, 2021, Vol. 36, No. 6
CD4, cluster of differentiation 4; DALY, Disability-adjusted life years; HTC, HIV testing and counselling; HTS, HIV testing services; PCR, polymerase chain reaction; PMTCT, prevention mother-to-child transmission;
LMICs (Rao et al., 2011; Wang et al., 2017), only one study explor-
ing the costs of scaling up the delivery of testing through private or
Average cost per kit Fixed costs: the distribution of fixed
cost to a larger number of people
Key drivers of costs identifieda
non-government providers (Verstraaten et al., 2017) was identified.
Further research on the costs of scaling up syphilis testing and mod-
elling community-based HIV and syphilis testing in public and pri-
vate sectors are needed.
Our review highlighted that while the overall standard of report-
ing costs was reasonable, with most studies partially or fully
addressing seven or more of the ten questions, shortcomings mani-
fested in two key areas. First, none of the studies in this review justi-
Categories for key drivers are summarized as geography and infrastructure, fixed costs, personnel, managing the process of scaling up and others, as discussed by Johns and Torres (2005).
fied their sample size for the costing. Economic evaluations often
require larger sample sizes for adequate power compared to a typical
Coefficient of scaleb
16.42 (Zambia),
¼ not provided
and USD 13.84
(Malawi), USD
clinical study evaluating the health impact of a testing intervention
distributed is
(Zimbabwe)
(Taylor et al., 2017). However, clinical studies and economic evalu-
Results
USD 8.15
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
ations generally investigate differences in outcomes at the individual
level. Cost drivers, such as scale, are better identified through multi-
site cost studies with the production unit or clinic as the unit of ana-
lysis (Tagar et al., 2014). A representative sample should capture
Findings related
to scale and
Economies of
differences in clinic characteristics such as geographical setting,
cost
ownership, and management systems. However, commonly the trial
scale
sample size or convenience sampling, in a limited number of sites,
determines sample size for a full or partial economic evaluation.
Given the considerable uncertainties around the costs of going to
Start-up costs: training and community
HIV self-test kits vehicle and build-
ing operation/maintenance, recur-
Recurrent costs: personnel, supplies,
scale including the varying cost of procuring and delivering test kits
Authors’ categorization of costs
Capital costs: building and storage,
(Johns and Torres, 2005; Shelley et al., 2015), it was surprising that
Economic and financial costs
almost half of the studies failed to explore the influence of different
rent training, and waste
equipment, and vehicle
sensitization activities
key inputs on unit costs or total programme costs by conducting sen-
sitivity analysis. For example, volume purchasing, which is being
explored in many LMICs, is likely to impact the cost and uptake of
management
rapid diagnostic tests (Taylor et al., 2017) and worth closer
consideration.
From a methodological viewpoint, the appraisal revealed that
only eight studies adjusted for changes in unit costs as HIV and
syphilis testing was scaled up (McConnel et al., 2005; Dandona
for decision
Timeframe
Short run
et al., 2008a,b; Shelley et al., 2015; Galárraga et al., 2017; Mwenge
et al., 2017; Bautista-Arredondo et al., 2018a; Mangenah et al.,
2019). Scaling up HIV and syphilis testing programmes typically
involves transporting supplies longer distances and to more remote
Coefficient of scale is a measure of association between average cost and level of scale.
A total of 349 719
test kits distrib-
uted in 71 sites
areas compared to pilot programs, which can lead to variations in
Sample size
the prices of consumables such as testing kits. The impact on pro-
gramme outcomes must also be considered alongside any changes in
costs. Sweeney et al. (2014) have argued that, while devolving super-
RST, Rapid syphilis testing; VCT, HIV voluntary counselling and testing.
vision and monitoring of RST in Tanzania to authorities at the sub-
national level may lead to reductions in the frequency and cost of ex-
Number of
test kits
Units of
output
ternal quality assurance, this may pose challenges for quality main-
tenance (Sweeney et al., 2014) . Our appraisal also revealed that
despite majority (22 out of 35) of studies have clearly stated their
Year (costs)
perspective, only three of these adopted a societal perspective. This
2019
means that a significant proportion of direct and indirect cost
incurred by patients for accessing tests is not considered. Moreover,
while most studies included a range of recurrent costs (e.g. staff
Increase in the total
Definition of scal-
kits distributed
number of test
time, training, testing commodities and other medical supplies) and
capital costs (e.g. vehicles and computers) and were focused at the
ing up
level of a clinic or health centre, few acknowledged the required
investments in infrastructure (e.g. quality management, reporting
system) and broader health systems strengthening needed as HIV
Table 4 (continued)
and syphilis testing programmes are scaled up to the national level
across all clinics and facilities (Kumaranayake et al., 2001). These
#25 (Mangenah
et al., 2019)
‘higher level’ investments refer ‘to the policy, political, legal, regula-
tory, budgetary or other health systems changes needed to institu-
tionalize new innovations at the national or sub-national level’
b
a
Ref
(World Health Organization and ExpandNet, 2010).Health Policy and Planning, 2021, Vol. 36, No. 6 951
Table 5 Results of the appraisal
References Costs Costs at scale
13 Fixed and variable costs
14 Factors other than scale
5 Methods for quantities
9 Sensitivity analysis
11 Costs and scale
10 Costs reporting
12 Quantification
4 Relevant inputs
6 Data source(s)
3 Time horizon
8 Discount rate
7 Sample size
1 Question(s)
2 Perspective
Shelley et al. (2015) () X () ()
Schackman et al. (2007) X () X () () X X
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
Bautista-Arredondo et al. (2018a,b) () () X
Dandona et al. (2008a,b) () () X () X X
Galárraga et al. (2017) X () X
Hontelez et al. (2013) () () () () () () X X X
Ishikawa et al. (2016) () () X X () () X X X ()
McConnel et al. (2005) X X () X X X
Ahaibwe G & Kasirye I (2013) X X X X () () () X X X X
Alsallaq et al. (2017) () () () () () X X X X
Cambiano et al. (2015) () () () X () () X X X ()
Cherutich et al. (2018) () () () X ()
Mwenge et al. (2017) () 冑
Stuart et al. (2018) X () () () () X X X () () X X ()
Tromp et al. (2013) () () () () 冑 () X X ()
Zhuang et al. (2018) () () X X X () () X X X
Dandona et al. (2008a,b) () () X
Dandona et al. (2005) X () X () ()
Forsythe (2002) () X () X X
Granich et al. (2009) X () () () () X X X () X X X X
Kasymova et al. (2009) () X () X () X
Kato et al. (2013) X () X () () X () X X
Kumar et al. (2006) 冑 () () () () X () () X X
Dandona et al. (2009) () () () () X ()
Mangenah et al. (2019) () X
McCreesh et al. (2017) () X () () () X X X
Minh et al. (2012) () () X X X () X
Sharma et al. (2016) () () () X () ()
Nelwan et al. (2016) () X () X X X () X X X X
Luong Nguyen et al. (2018) () () () X X () X
Rely. (2003) () () X () X () () X X X ()
Tchuenche et al. (2018) () () () X X X
Verstraaten et al. (2017) () () () X X () X
Zang et al. (2016) () () () () () X X ()
Zhang et al. (2015) () () () X () ()
: yes; X: no; (): partially addressed.
Another area for methodological improvement relates to the or buildings—leading to economies of scale. For one study on the
quantification of the relationship between average costs and the roll out of syphilis rapid testing in Zambia, lower clinic catchment
scale of delivering HIV or syphilis testing. Most studies undertook a populations combined with higher unit costs for transport, supervi-
simple form of modelling whereby costs were scaled up linearly. For sion and test kits reduced the economies of scale achieved in the
these studies, an empirical average cost associated with a testing high coverage pilot sites (Shelley et al., 2015). This resonates with
programme was multiplied by a factor representing activity at a economic theory as output increases average costs will first fall and
larger scale. For example, if the unit cost per person tested for HIV then rise, following a ‘u’-shaped curve (Guinness, Kumaranayake
and syphilis is United States Dollar (USD) 10 for 100 people then and Hanson, 2007; Kumaranayake, 2008). This small subset of
expanding coverage by another 50 people would be USD 500 studies represents an important step forward in providing a more ac-
(Kumaranayake, 2008). Only 10 of the 35 studies developed non- curate estimation of the costs of scaling up HIV and syphilis testing
linear cost functions, allowing some costs to be fixed regardless of interventions in LMICs, painting a more complex picture of the rela-
the size of the population reached—e.g. medical equipment, vehicles tionship between scale and costs.952 Health Policy and Planning, 2021, Vol. 36, No. 6
There are some limitations of this review that need to be Bautista-Arredondo S, Colchero MA, Amanze OO et al. 2018b. Explaining
acknowledged. Studies were restricted to those found in the pub- the heterogeneity in average costs per HIV/AIDS patient in Nigeria: the role
lished literature, a potential source of reporting bias. In addition, the of supply-side and service delivery characteristics. PLoS One 13(5):
e0194305.
studies identified varied by analytical approach (empirical, econo-
Bert F, Gualano MR, Biancone P et al. 2018. HIV screening in pregnant
metric or model), testing intervention and types of costs measured.
women: a systematic review of cost-effectiveness studies. The International
This diversity prevented the pooling of results for a meta-analysis. Journal of Health Planning and Management 33: 31–50.
Instead, studies were qualitatively reviewed, and their results and Bristow CC, Larson E, Anderson LJ et al. 2016. Cost-effectiveness of HIV and
characteristics tabulated which helped to highlight evidence gaps syphilis antenatal screening: a modelling study. Sexually Transmitted
and methodological weaknesses. Infections 92: 340–6.
In summary, this review highlights evidence of the relationship Cambiano V, Ford D, Mabugu T et al. 2015. Assessment of the potential im-
between the costs and scale of delivering HIV and syphilis testing in pact and cost-effectiveness of self-testing for HIV in low-income countries.
LMICs. What is less clear is how costs change with scale and in turn Journal of Infectious Diseases 212: 570–7.
Cherutich P, Farquhar C, Wamuti B et al.; for the aPS Study Group. 2018.
the potential for economies of scale. Scaling up costs linearly, an as-
HIV partner services in Kenya: a cost and budget impact analysis study.
sumption that underpins most studies in this review, and runs the
Downloaded from https://academic.oup.com/heapol/article/36/6/939/6163122 by guest on 02 January 2022
BMC Health Services Research 18: 721.
risk of misleading policymakers as to the true costs of providing uni-
Dandona L, Sisodia P, Ramesh YK et al. 2005. Cost and efficiency of HIV vol-
versal access to HIV and syphilis testing. Collecting empirical cost untary counselling and testing centres in Andhra Pradesh, India. The
data alongside the roll-out of HIV and syphilis testing is a priority. National Medical Journal of India 18: 26–31.
Financing and budgeting for the scale up of HIV and syphilis testing Dandona L, Kumar SP, Ramesh YK et al. 2008a. Changing cost of HIV inter-
will benefit from the monitoring of costs across different sites, con- ventions in the context of scaling-up in India. AIDS 22: S43–9.
texts and settings as well as over time, for greater consistency in the Dandona L, Kumar SP, Ramesh YK et al. 2008b. Outputs, cost and efficiency
categorization of fixed and variables costs, and the inclusion of costs of public sector centres for prevention of mother to child transmission of
associated with strengthening health systems to support quality as- HIV in Andhra Pradesh, India. BMC Health Services Research 8: 26.
Dandona L, Kumar SP, Kumar GA et al.Economic analysis of HIV prevention
surance and stock management systems.
interventions in Andhra Pradesh state of India to inform resource allocation.
AIDS 23: 233–42. 10.1097/QAD.0b013e328320accc
Fleming K A, Naidoo M, Wilson M et al.. 2017. An Essential Pathology
Supplementary data
Package for Low- and Middle-Income Countries. American Journal of
Supplementary data are available at Health Policy and Planning online Clinical Pathology 147: 15–32. 10.1093/ajcp/aqw143 28158414
Forsythe S. 2002. Assessing the cost and willingness to pay for voluntary HIV
counselling and testing in Kenya. Health Policy and Planning 17: 187–95.
Acknowledgements Galárraga O, Wamai RG, Sosa-Rubı́ SG et al. 2017. HIV prevention costs and
The authors thank Monica O’Brien, the UNSW Academic Services Librarian; their predictors: evidence from the ORPHEA Project in Kenya. Health
Fern Terris-Prestholt, Associate Professor in Economics of HIV, London Policy and Planning 32: 1407–16.
School of Hygiene and Tropical Medicine (LSHTM); Anna Vassal, Professor Getzen TE. 2014. Health Economics and Financing, 5th edn, 3–6. https://
of Health Economics, London School of Hygiene and Tropical Medicine; and www.wiley.com/en-us/HealthþEconomicsþandþFinancing
Benjamin Johns, Abt Associates, International Health Division, Bethesda, %2Cþ5thþEdition-p-9781118184905, accessed 28 July 2020.
USA. Gomez GB, Mudzengi DL, Bozzani F et al. 2020. Estimating cost functions for
resource allocation using transmission models: a case study of tuberculosis
case finding in South Africa. Value in Health 23: 1606–12.
Funding Granich RM, Gilks CF, Dye C et al. 2009. Universal voluntary HIV testing
with immediate antiretroviral therapy as a strategy for elimination of HIV
Corresponding author has received funding from the Scientia PhD
transmission: a mathematical model. The Lancet 373: 48–57.
Scholarship scheme provided by the University of New South Wales.
Guinness L, Kumaranayake L, Hanson K. 2007. A cost function for HIV pre-
Conflict of interest statement. None declared. vention services: is there a “u”—shape?, Cost Effectiveness and Resource
Allocation 5: 13.
Ethical approval. No ethical approval was required for this study
Hontelez JAC, Lurie MN, Bärnighausen T et al. 2013. Elimination of HIV in
South Africa through expanded access to antiretroviral therapy: a model
comparison study. PLoS Medicine 10: e1001534.
References Hook EW. 2017. Syphilis. The Lancet 389: 1550–7.
Ahaibwe G, Kasirye I. 2013. HIV/AIDS prevention interventions in Uganda: a Husereau D, Drummond M, Petrou S et al. 2013. Consolidated Health
policy simulation. Research Series 167527, Economic Policy Research Economic Evaluation Reporting Standards (CHEERS) statement. The
Centre (EPRC). European Journal of Health Economics 14: 367–72.
Ahmed S, Autrey J, Katz IT et al. 2018. Why do people living with HIV not ini- Ishikawa N, Dalal S, Johnson C et al. 2016. Should HIV testing for all preg-
tiate treatment? A systematic review of qualitative evidence from low- and nant women continue? Costeffectiveness of universal antenatal testing com-
middle-income countries. Social Science & Medicine 213: 72–84. pared to focused approaches across high to very low HIV prevalence
Alsallaq RA, Buttolph J, Cleland CM et al. 2017. The potential impact and settings. Journal of the International AIDS Society, 19: 21212.
cost of focusing HIV prevention on young women and men: a modeling ana- Johns B. 2015. The link between modelling and doing. The Lancet HIV 2:
lysis in western Kenya. PLoS One 12: e0175447. e174–e175.
Asiimwe S, Ross JM, Arinaitwe A et al. 2017. Expanding HIV testing and link- Johns B, Baltussen R. 2004. Accounting for the cost of scaling-up health inter-
age to care in southwestern Uganda with community health extension work- ventions. Health Economics 13: 1117–24.
ers. Journal of the International AIDS Society 20(Suppl 4): 21633. Johns B, Torres TT. 2005. Costs of scaling up health interventions: a systemat-
Bautista-Arredondo S, La Hera-Fuentes G, Contreras-Loya D et al. 2018a. ic review. Health Policy and Planning, 20: 1–13.
Efficiency of HIV services in Nigeria: determinants of unit cost variation of Joint United Nations Programme on HIV/AIDS. 2018. UNAIDS Data 2018.
HIV counseling and testing and prevention of mother-to-child transmission https://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_
interventions. PLoS One 13(9): e0201706. en.pdf, accessed 10 September 2018.You can also read