Safety and Efficacy of Specially Designed Texture-Modified Foods for Patients with Dysphagia Due to Brain Disorders: A Prospective Study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
healthcare
Article
Safety and Efficacy of Specially Designed Texture-Modified
Foods for Patients with Dysphagia Due to Brain Disorders:
A Prospective Study
Soyoung Kwak, Yoo Jin Choo , Kyu Tae Choi and Min Cheol Chang *
Department of Physical Medicine & Rehabilitation, College of Medicine, Yeungnam University, Daegu 42415,
Korea; sk315@ynu.ac.kr (S.K.); cyj361@hanmail.net (Y.J.C.); choi3190@ynu.ac.kr (K.T.C.)
* Correspondence: wheel633@gmail.com; Tel.: +82-53-620-3270
Abstract: Providing texture-modified food for patients with dysphagia is a cornerstone of dysphagia
treatment. This study aimed to evaluate the safety and efficacy of a specially designed texture-
modified food that can be easily swallowed while maintaining the unique taste by adjusting hardness
and adhesiveness in patients with brain disorders using a videofluoroscopic swallowing study. We
included 101 patients with oropharyngeal dysphagia due to brain disorders who were referred to the
rehabilitation department. To evaluate the safety and efficacy of a specially designed texture-modified
food, rice gruel was compared with a regular instant rice porridge, and bulgogi mousse was compared
with ground bulgogi, which normally serves as a texture-modified diet for patients with dysphagia in
our hospital during the videofluoroscopic swallowing study. The Penetration–Aspiration Scale score,
oropharyngeal transit time, number of swallows required to maximally eliminate food materials
from the oropharyngeal space, and vallecular and pyriform sinus residue after swallowing scale
score were compared. Rice gruel required a shorter oropharyngeal transit time and fewer number of
Citation: Kwak, S.; Choo, Y.J.; Choi,
K.T.; Chang, M.C. Safety and Efficacy
swallowing per the given amount of food than regular instant rice porridge; however, no statistical
of Specially Designed difference was found in the vallecular and pyriform sinus residue after swallowing scale scores
Texture-Modified Foods for Patients and the Penetration–Aspiration Scale scores. Bulgogi mousse required more swallowing and had
with Dysphagia Due to Brain lower Penetration–Aspiration Scale scores than ground bulgogi; however, no significant difference
Disorders: A Prospective Study. was found in the oropharyngeal transit time and the vallecular and pyriform sinus residue after
Healthcare 2021, 9, 728. https:// swallowing scale scores. The study foods were safe and efficacious compared to control foods usually
doi.org/10.3390/healthcare9060728 provided for patients with dysphagia from various brain disorders.
Academic Editor: Pedram Sendi Keywords: dysphagia; texture-modified foods; dysphagia diet; brain disorders; texture analysis
Received: 14 May 2021
Accepted: 10 June 2021
Published: 13 June 2021
1. Introduction
Publisher’s Note: MDPI stays neutral
Texture is one of the four principal quality factors in food, along with its appearance,
with regard to jurisdictional claims in
flavor and nutrition [1]. It is not a single property; it is a group of physical properties
published maps and institutional affil- derived from the structure of the food. Adhesiveness, cohesiveness, firmness, fracturability,
iations. hardness, springiness, viscosity and yield stress have been suggested to be the most
significant components of texture in dysphagia diet and management [2]. Previous studies
using kinematic analysis of dysphagia elucidated that bolus transit time and velocity are
highly dependent on the patient’s medical conditions and food texture [3–7].
Copyright: © 2021 by the authors.
Providing texture-modified food for patients with dysphagia has been accepted as
Licensee MDPI, Basel, Switzerland.
a cornerstone of dysphagia treatment [2,8,9]. However, previous studies have reported
This article is an open access article
poor adherence to texture-modified diets due to limited choice, unsatisfactory taste, lack
distributed under the terms and of experience and knowledge for preparing texture-modified diet, higher cost and longer
conditions of the Creative Commons time to prepare the foods as they require additional processing such as blending, grinding
Attribution (CC BY) license (https:// or chopping [10–12]. Poor adherence to texture-modified diet may lead to decreased oral
creativecommons.org/licenses/by/ intake, dehydration, increased risk of chest infection and malnutrition in patients with
4.0/). dysphagia [13–15]. In addition, no specific food texture has been demonstrated to have
Healthcare 2021, 9, 728. https://doi.org/10.3390/healthcare9060728 https://www.mdpi.com/journal/healthcareHealthcare 2021, 9, x 2
Healthcare 2021, 9, 728 2 of 9
dysphagia [13–15]. In addition, no specific food texture has been demonstrated to h
clear, measurable positive
clear, impactpositive
measurable on the swallowing
impact on the pattern [16,17]. Even
swallowing pattern though there
[16,17]. Even arethough th
several clinicalare
guidelines for dysphagia
several clinical guidelines diet,
formost adopt diet,
dysphagia viscosity
mostcategory boundaries,
adopt viscosity category boun
which are based onwhich
ries, consensus
are basedrather than evidence
on consensus rather[16].
than Therefore,
evidence [16].it isTherefore,
important toimportan
it is
develop texture-modified foods that canfoods
develop texture-modified addressthatthe
canaforementioned issues.
address the aforementioned issues.
In this study, In
wethis
aimed
study,to we
evaluate
aimed the safety and
to evaluate efficacy
the safety andofefficacy
specially designeddesigned
of specially
texture-modified foods (rice foods
ture-modified gruel and(rice bulgogi
gruel and mousse)
bulgogifor patients
mousse) forwith dysphagia
patients that
with dysphagia that
can be easily swallowed while maintaining
be easily swallowed the unique
while maintaining the taste of taste
unique foodsofby adjusting
foods their their ha
by adjusting
hardness and adhesiveness using videofluoroscopic
ness and adhesiveness swallowingswallowing
using videofluoroscopic study (VFSS). This(VFSS).
study study This st
aimed to compareaimedthetoairway
compare safety measured
the airway by measured
safety the Penetration–Aspiration Scale (PAS) Scale (P
by the Penetration–Aspiration
scores of the study
scoresand control
of the study foods and compare
and control the efficacy
foods and compareofthe theefficacy
study and control
of the study and con
foods using the foods using the oropharyngeal
oropharyngeal transit time,
transit time, number number required
of swallows of swallows required to elimin
to eliminate
food materialsfood
frommaterials from the oropharyngeal
the oropharyngeal space, and thespace,amountandofthe amount
residue in of
theresidue
pharynx in the phar
after swallowing.
after swallowing.
2. Materials and Methods and Methods
2. Materials
2.1. Study Design
2.1. Study Design
The study foodsThewere
studyrice gruel
foods andrice
were bulgogi
gruel mousse (Shinsegae
and bulgogi mousseFood Inc., Seoul,
(Shinsegae Food Inc., Se
Korea). To evaluate the safety and efficacy of the study foods, rice gruel
Korea). To evaluate the safety and efficacy of the study foods, rice was compared
gruel was compa
with a regular with
instant rice porridge
a regular instant widely available
rice porridge in the
widely marketinand
available thebulgogi
market andmousse
bulgogi mou
was compared was
withcompared
ground bulgogi, which normally serves as a texture-modified diet for
with ground bulgogi, which normally serves as a texture-modified die
patients with dysphagia
patients within dysphagia
our hospital (Figure
in our 1). Since
hospital it was
(Figure impractical
1). Since to compare
it was impractical to compare
the VFSS findings
VFSSoffindings
the study andstudy
of the control
andfood in different
control patientspatients
food in different controlling for po-for poten
controlling
tential confounding factors,factors,
confounding the study
theand control
study foods were
and control foodstested in the same
were tested in the patient.
same patient. S
Since we had two
we pairs
had twoof study and
pairs of control
study andfoods,
controlthe patients
foods, were divided
the patients into two
were divided dif-two diffe
into
ferent groups—the rice gruel group and the bulgogi mousse group- to avoid excessive
groups—the rice gruel group and the bulgogi mousse group- to avoid excessive radia
radiation exposure.
exposure.
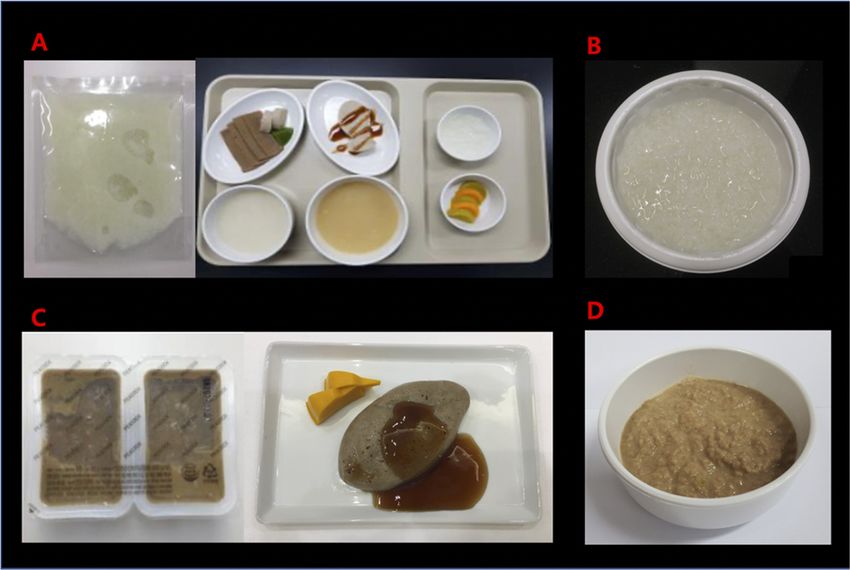
FigureFigure
1. Study
1. and control
Study and foods.
control(A) rice gruel;
foods. (B) gruel;
(A) rice rice porridge;
(B) rice (C) bulgogi(C)
porridge; mousse; andmousse;
bulgogi (D) ground
andbulgogi.
(D)
ground bulgogi.
2.2. Participants
The inclusion criteria were as follows: (1) patients who were referred to the reha-
bilitation department for VFSS; (2) patients who were diagnosed with stroke, traumatic
brain injury, Parkinson’s disease, Alzheimer’s disease, brain tumor or hypoxic-ischemicHealthcare 2021, 9, 728 3 of 9
encephalopathy; (3) patients who could sit and maintain upright posture during VFSS;
(4) patients with alert mentality and sufficient cognitive function and could follow the
directions during VFSS; and (5) patients confirmed to have oropharyngeal dysphagia in the
VFSS. The exclusion criteria were as follows: (1) patients agedHealthcare 2021, 9, 728 4 of 9
of the control food during the study period. Texture analyses were performed three times
for each food, and the mean values for each food were used to determine the UDF stage.
Statistical analysis was not performed to determine the changes in the texture of the food
after being mixed with Bonorex because the sample size was judged to be insufficient. All
texture analyses were performed at the Food Processing Laboratory of Sejong University.
Table 1. The Universal Design Foods guidelines for elderly people.
Stage 1 Stage 2 Stage 3 Stage 4
Able to smash Able to smash Able to swallow
Classifications Able to chew easily
with gums with tongue without chewing
Contains hard and big Contains hard and big Contains soft and small
Hard to swallow if
Standards of chewing ingredients, a little ingredients not easy ingredients, easy
contains solid food
hard to swallow to swallow to swallow
Depends on Have experience hard
Standards of Able to Hard to swallow water
ingredients, hard to swallow water or
swallowing swallow commonly or liquid ingredients
to swallow liquid ingredients
Hardness (N/m2 ) 5 × 105 5 × 104 2 × 104 5 × 103
Reproduced from [20] via license: CC BY-NC 4.0. No changes were made to this table.
2.6. Standard Protocol Approvals, Registrations and Patient Consents
This study was conducted in accordance with the Declaration of Helsinki and was
reviewed and approved by the Institutional Review Board of the University Hospital.
Written informed consent was obtained from all participants.
2.7. Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences version 20.0 (IBM
Corp., Armonk, NY, USA). Demographic data of the study participants were compared
using the Mann-Whitney U test for age, Chi-squared test for gender and disease duration,
and Fisher’s exact test for diagnosis. Among the outcome measures, the oropharyngeal
transit time was compared using the paired t-test and the rest were compared using
the Wilcoxon signed-rank test. All tests were two-tailed and uncorrected for multiple
comparisons. Statistical significance was set at p < 0.05.
3. Results
A total of 101 patients were enrolled in this study (50 and 51 in the rice gruel and
bulgogi mousse groups, respectively; Table 2). The mean patient age was 72 years in
the rice gruel group and 72.73 years in the bulgogi mousse group. Furthermore, 25 of
50 patients in the rice gruel group and 23 of 51 patients in the bulgogi mousse group had a
disease duration of ≥6 months. No significant difference was found in the demographic
data of the participants in the rice gruel and bulgogi mousse groups.
According to the texture analysis of the study and control foods, rice gruel and rice
porridge were classified as UDF stage 4 (food can be swallowed without chewing) and
bulgogi mousse was classified as UDF stage 3 (food can be smashed with the tongue at
temperatures of 20 ◦ C–25 ◦ C and 40 ◦ C–50 ◦ C; Table 3). The UDF stage of each food was
maintained on mixing it with Bonorex 300, which was used as a contrast medium.
After mixing with Bonorex 300, all the foods tested showed increased hardness at a
temperature of 20 ◦ C–25 ◦ C; however, rice gruel showed decreased hardness and bulgogi
mousse showed increased hardness at a temperature of 40 ◦ C–50 ◦ C. In terms of adhesive-
ness, all the foods tested showed decreased values after mixing with a contrast medium at
all temperatures.Healthcare 2021, 9, 728 5 of 9
Table 2. Demographic data of the study participants.
Rice Gruel vs. Bulgogi Mousse vs.
p-Value
Rice Porridge Ground Bulgogi
Age (years) (mean ± SD) 72.00 ± 15.17 72.73 ± 12.05 0.736 a
Male: Female (n) 23:27 26:25 0.482 b
Diagnosis (n) 0.350 c
Ischemic stroke 23 27
Hemorrhagic stroke 13 6
Alzheimer’s disease 6 12
Parkinson’s disease 4 3
Brain tumor 2 1
Hypoxic ischemic brain injury 1 0
Traumatic brain injury 1 2
Disease duration (n) 0.622 bHealthcare 2021, 9, 728 6 of 9
Table 4. Comparison of outcome measure.
Bulgogi Ground
Rice Gruel a Rice Porridge b p-Value p-Value
Mousse a Bulgogi b
Oropharyngeal transit time
39.88 ± 18.40 61.08 ± 28.59Healthcare 2021, 9, 728 7 of 9
lower PAS score, could result from differences in the texture of the ground bulgogi and
bulgogi mousse. It appears that the viscosity of ground bulgogi was lower than that of
bulgogi mousse, which is compatible with the results of previous studies that reported
that boluses with lower viscosity are more difficult to swallow safely than boluses with
higher viscosity [22,23]. However, objective texture analysis for ground bulgogi was not
performed in this study; thus, further studies are needed to elucidate its association. It
should also be noted that despite the statistical significance, the mean difference in PAS
scores might not be significant in the clinical setting.
Several previous studies have identified the beneficial effect of high shear viscosity in
reducing the risk of aspiration during swallowing. It is assumed that high-viscosity boluses
are transported more slowly than low-viscosity boluses, thus allowing more time for the
oropharyngeal mechanism to secure the airways until the bolus enters the esophagus [9].
Therefore, the nutritional management of patients with dysphagia is based on increasing
the viscosity to a certain range that is considered safe for swallowing. However, very thick
foods are poorly accepted by patients, and high-viscosity foods may result in an increase in
residues after swallowing, reduction of palatability and increased risk of dehydration [24,25].
Therefore, it is important for clinicians to understand the physical properties of foods and
their relation to dysphagia and be more specific in prescribing texture-modified diets for
patients with dysphagia.
However, the assessment and application of texture modification is subjective in
clinical settings; the preparation as well as the rheological evaluation and administration
of thickened foods to patients are universally subjective and a wide range of viscous
properties are recommended for the same level of dysphagia [26,27]. In addition, despite
the established knowledge on the close connection between dysphagia and rheological
properties of food bolus, knowledge has not been incorporated into the national guidelines
for the dietary management of dysphagia, such as the National Dysphagia Diet Task Force
(2002) of the American Dietetic Association [28] or the British Dietetic Association (2009) in
the National Description for Texture Modification in Adults [29]. However, attempts have
been made to establish an international terminology for texture-modified foods used in
dysphagia management [8,30,31].
The results of this study are meaningful because to the best of our knowledge, this
is the first study to evaluate the safety and efficacy of specially designed dysphagia food
in patients with brain disorders using VFSS. Previous studies have focused mainly on the
nutritional state of patients with dysphagia [12,31–33], but limited information is available
regarding the safety and efficacy of swallowing foods with different physical properties
other than viscosity using VFSS.
Study Limitations
First, the lack of randomization of the sequence of study and control foods is a major
limitation of this study. Due to the limited staffing, blinding for the sequence was not
possible, and this could lead to bias. Second, texture analyses of ground bulgogi and
rice porridge mixed with Bonorex at a temperature of 40 ◦ C–50 ◦ C were not performed.
In addition, the ease of preparation (compared to conventional texture-modified foods
prepared at home), adherence to the prescribed diet, patient satisfaction and long-term
outcomes such as nutritional state or frequency of chest infection, were not included in the
current study.
5. Conclusions
In conclusion, the specially designed texture-modified foods—rice gruel and bulgogi
mousse—were found to be safe and efficacious for patients with dysphagia and various
brain disorders. Therefore, practical application of these foods is warranted.
Author Contributions: Conceptualization, S.K. and M.C.C.; methodology, S.K. and M.C.C.; software,
S.K. and M.C.C.; validation, S.K. and M.C.C.; formal analysis, Y.J.C. and K.T.C.; investigation, Y.J.C.
and K.T.C.; resources, Y.J.C. and K.T.C.; data curation, Y.J.C. and K.T.C.; writing—original draftHealthcare 2021, 9, 728 8 of 9
preparation, S.K., Y.J.C., K.T.C. and M.C.C.; writing—review and editing, S.K., Y.J.C., K.T.C. and
M.C.C.; visualization, S.K., Y.J.C., K.T.C. and M.C.C.; supervision, M.C.C. All authors have read and
agreed to the published version of the manuscript.
Funding: This study was supported by Shinsegae Food Inc., Korea; and a National Research Founda-
tion of Korea Grant funded by the Korean government (grant number NRF-2019M3E5D1A02068106).
Institutional Review Board Statement: The study was conducted according to the guidelines of the
Declaration of Helsinki and approved by the Institutional Review Board of Yeungnam University
Hospital (2019-02-022-001).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: The data presented in this study are available on request from the
corresponding author.
Conflicts of Interest: The authors declare no conflict of interest. The funder had no involvement in
study design, methods, subject recruitment, data collections, analysis and preparation of paper. In
addition, the funder was not involved in the decision to submit the article for publication.
References
1. Bourne, M. Food Texture and Viscosity, 2nd ed.; Academic Press: London, UK, 2002.
2. Murry, T.; Carrau, R.L.; Chan, K. Clinical Management of Swallowing Disorders, 2nd ed.; Plural Publishing: San Diego, CA,
USA, 2006.
3. Takasaki, K.; Umeki, H.; Enatsu, K.; Tanaka, F.; Sakihama, N.; Kumagami, H.; Takahashi, H. Investigation of pharyngeal
swallowing function using high-resolution manometry. Laryngoscope 2008, 118, 1729–1732. [CrossRef]
4. Bredenoord, A.J.; Smout, A.J. High-resolution manometry. Dig. Liver Dis. 2008, 40, 174–181. [CrossRef]
5. Omari, T.I.; Rommel, N.; Szczesniak, M.M.; Fuentealba, S.; Dinning, P.G.; Davidson, G.P.; Cook, I.J. Assessment of intraluminal
impedance for the detection of pharyngeal bolus flow during swallowing in healthy adults. Am. J. Physiol. Gastrointest. Liver
Physiol. 2006, 290, G183–G188. [CrossRef]
6. Hasegawa, A.; Otoguro, A.; Kumagai, H.; Nakazawa, F. Velocity of Swallowed Gel Food in the Pharynx by Ultrasonic Method.
Nippon Shokuhin Kagaku Kogaku Kaishi 2005, 52, 441–447. [CrossRef]
7. Lee, S.H.; Oh, B.M.; Chun, S.M.; Lee, J.C.; Min, Y.; Bang, S.H.; Kim, H.C.; Han, T.R. The accuracy of the swallowing kinematic
analysis at various movement velocities of the hyoid and epiglottis. Ann. Rehabil. Med. 2013, 37, 320–327. [CrossRef]
8. Hanson, B. A review of diet standardization and bolus rheology in the management of dysphagia. Curr. Opin. Otolaryngol. Head
Neck Surg. 2016, 24, 183–190. [CrossRef]
9. Ekberg, O. Dysphagia: Diagnosis and Treatment, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2019.
10. Flynn, E.; Smith, C.H.; Walsh, C.D.; Walshe, M. Modifying the consistency of food and fluids for swallowing difficulties in
dementia. Cochrane Database Syst. Rev. 2018, 9, Cd011077. [CrossRef]
11. O’Keeffe, S.T. Use of modified diets to prevent aspiration in oropharyngeal dysphagia: Is current practice justified? BMC Geriatr.
2018, 18, 167. [CrossRef] [PubMed]
12. Painter, V.; Le Couteur, D.G.; Waite, L.M. Texture-modified food and fluids in dementia and residential aged care facilities. Clin.
Interv. Aging 2017, 12, 1193–1203. [CrossRef] [PubMed]
13. Vucea, V.; Keller, H.H.; Morrison, J.M.; Duizer, L.M.; Duncan, A.M.; Carrier, N.; Lengyel, C.O.; Slaughter, S.E.; Steele, C.M.
Modified Texture Food Use is Associated with Malnutrition in Long Term Care: An Analysis of Making the Most of Mealtimes
(M3) Project. J. Nutr. Health Aging 2018, 22, 916–922. [CrossRef] [PubMed]
14. Cichero, J.A.Y. Age-Related Changes to Eating and Swallowing Impact Frailty: Aspiration, Choking Risk, Modified Food Texture
and Autonomy of Choice. Geriatrics 2018, 3, 69. [CrossRef] [PubMed]
15. Shimizu, A.; Maeda, K.; Tanaka, K.; Ogawa, M.; Kayashita, J. Texture-modified diets are associated with decreased muscle mass
in older adults admitted to a rehabilitation ward. Geriat.r Gerontol. Int. 2018, 18, 698–704. [CrossRef]
16. Frazier, J.; Chestnut, A.H.; Jackson, A.; Barbon, C.E.; Steele, C.M.; Pickler, L. Understanding the Viscosity of Liquids used in
Infant Dysphagia Management. Dysphagia 2016, 31, 672–679. [CrossRef]
17. Steele, C.M.; Alsanei, W.A.; Ayanikalath, S.; Barbon, C.E.; Chen, J.; Cichero, J.A.; Coutts, K.; Dantas, R.O.; Duivestein, J.; Giosa, L.;
et al. The influence of food texture and liquid consistency modification on swallowing physiology and function: A systematic
review. Dysphagia 2015, 30, 2–26. [CrossRef] [PubMed]
18. Rosenbek, J.C.; Robbins, J.A.; Roecker, E.B.; Coyle, J.L.; Wood, J.L. A penetration-aspiration scale. Dysphagia 1996, 11, 93–98.
[CrossRef] [PubMed]
19. Han, T.R.; Paik, N.J.; Park, J.W. Quantifying swallowing function after stroke: A functional dysphagia scale based on videofluoro-
scopic studies. Arch. Phys. Med. Rehabil. 2001, 82, 677–682. [CrossRef]
20. Kang, A.; Kim, D.; Kang, S.; Seo, K.; Park, H.; Park, K. EMG Activity of Masseter Muscles in the Elderly According to Rheological
Properties of Solid Food. Ann. Rehabil. Med. 2016, 40, 447–456. [CrossRef]Healthcare 2021, 9, 728 9 of 9
21. Tokifuji, A.; Matsushima, Y.; Hachisuka, K.; Yoshioka, K. Texture, sensory and swallowing characteristics of high-pressure-heat-
treated pork meat gel as a dysphagia diet. Meat Sci. 2013, 93, 843–848. [CrossRef] [PubMed]
22. Zargaraan, A.; Rastmanesh, R.; Fadavi, G.; Zayeri, F.; Mohammadifar, M.A. Rheological aspects of dysphagia-oriented food
products: A mini review. Food Sci. Hum. Wellness 2013, 2, 173–178. [CrossRef]
23. Nyström, M. Extensional Rheometry through Hyperbolic Contraction; Chalmers University of Technology: Göteborg, Sweden, 2015.
24. Steele, C.M.; Molfenter, S.M.; Péladeau-Pigeon, M.; Stokely, S. Challenges in preparing contrast media for videofluoroscopy.
Dysphagia 2013, 28, 464–467. [CrossRef] [PubMed]
25. Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of Bolus Viscosity on the Safety and Efficacy of Swallowing and the
Kinematics of the Swallow Response in Patients with Oropharyngeal Dysphagia: White Paper by the European Society for
Swallowing Disorders (ESSD). Dysphagia 2016, 31, 232–249. [CrossRef]
26. Steele, C.M.; Cichero, J.A. A question of rheological control. Dysphagia 2008, 23, 199–201. [CrossRef] [PubMed]
27. Steele, C.M.; Van Lieshout, P.H.; Goff, H.D. The rheology of liquids: A comparison of clinicians’ subjective impressions and
objective measurement. Dysphagia 2003, 18, 182–195. [CrossRef]
28. National Dysphagia Diet Task, F.; American Dietetic, A. National Dysphagia Diet: Standardization for Optimal Care; American
Dietetic Association: Chicago, IL, USA, 2002.
29. The British Dietetic Association and the Royal College of Speech and Language Therapist. National Descriptors for Texture
Modification in Adults; The British Dietetic Association and the Royal College of Speech and Language Therapist: London,
UK, 2002.
30. Cichero, J.A.; Steele, C.; Duivestein, J.; Clavé, P.; Chen, J.; Kayashita, J.; Dantas, R.; Lecko, C.; Speyer, R.; Lam, P.; et al. The
Need for International Terminology and Definitions for Texture-Modified Foods and Thickened Liquids Used in Dysphagia
Management: Foundations of a Global Initiative. Curr. Phys. Med. Rehabil. Rep. 2013, 1, 280–291. [CrossRef]
31. Cichero, J.A.; Lam, P.; Steele, C.M.; Hanson, B.; Chen, J.; Dantas, R.O.; Duivestein, J.; Kayashita, J.; Lecko, C.; Murray, J.; et al.
Development of International Terminology and Definitions for Texture-Modified Foods and Thickened Fluids Used in Dysphagia
Management: The IDDSI Framework. Dysphagia 2017, 32, 293–314. [CrossRef] [PubMed]
32. Higashiguchi, T.; Ito, A.; Nishiyama, H.; Shigematsu, T.; Ishikawa, A.; Kato, H.; Iijima, S.; Kikuchi, N. Appropriate nutritional
management in patients with impaired mastication and those with mild dysphagia: A multicenter study of the usefulness of
novel foods processed and softened by enzymes. Asia Pac. J. Clin. Nutr. 2017, 26, 1007–1015. [CrossRef] [PubMed]
33. Shimizu, A.; Momosaki, R.; Kayashita, J.; Fujishima, I. Impact of Multiple Texture-Modified Diets on Oral Intake and Nutritional
Status in Older Patients with Pneumonia: A Retrospective Cohort Study. Dysphagia 2020, 35, 574–582. [CrossRef]You can also read