Prevalence of Lumbosacral Transitional Vertebrae in Patients With Symptomatic Femoroacetabular Impingement Requiring Hip Arthroscopy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Prevalence of Lumbosacral Transitional Vertebrae in
Patients With Symptomatic Femoroacetabular
Impingement Requiring Hip Arthroscopy
Roger Luo, M.D., Dena Barsoum, M.D., Humaira Ashraf, M.D., Jennifer Cheng, Ph.D.,
Nicole R. Hurwitz, B.S., Campbell Y. Goldsmith, B.A., and Peter J. Moley, M.D.
Purpose: The primary aim of this study was to determine the prevalence of lumbosacral transitional vertebrae (LSTVs) in
patients with symptomatic femoroacetabular impingement (FAI) requiring hip arthroscopy. The secondary aim was to
determine whether there is an association between LSTV anatomy and patient-reported outcomes. Methods: This
retrospective study included patients aged 18 to 45 years with symptomatic FAI who underwent arthroscopy between
March 2010 and March 2016 and had anteroposterior pelvic radiographs. The exclusion criteria included lack of an FAI
diagnosis, hip osteoarthritis (Tönnis grade 2), prior spinal fusion surgery, prior total hip arthroplasty, indications for total
hip arthroplasty, and revision surgery on the affected hip. All radiographs were assessed by an interventional spine and
sports fellow. The primary outcome was the prevalence of LSTVs, classified using the criteria of Castellvi et al. Secondary
outcomes included the modified Harris Hip Score, Hip Outcome Score, and International Hip Outcome Tool 33 score.
Results: A total of 1,880 patients were included. Review of the patients’ radiographs yielded 262 LSTVs, for an overall
prevalence of 13.9% (type IA in 104 [5.5%], type IB in 53 [2.8%], type IIA in 60 [3.2%], type IIB in 25 [1.3%], type IIIA
in 8 [0.4%], type IIIB in 0 [0%], and type IV in 12 [0.64%]). The prevalence of type II, III, and IV LSTVs was 5.6%
(n ¼ 105). Unilateral LSTV sidedness did not correlate with symptom laterality (k ¼ 0.07). There were no differences in
patient-reported outcomes between patients with LSTV anatomy and those without it. Conclusions: In this large cohort
of 1,880 patients with symptomatic FAI, the prevalence of LSTVs was 13.9%. There was no correlation between sidedness
of unilateral LSTVs and the symptomatic hip. Furthermore, there was no association between LSTV anatomy and patient-
reported outcomes. The prevalence of LSTVs in this cohort was similar to the prevalence rates previously reported in
patients with low-back pain. Level of Evidence: Level IV, case series.
See commentary on page 156
followed.1-5 Radiographic measures of either the acetab-
A wareness of anatomic variants in proximal femoral
and acetabular morphology has increased rapidly in
the past decade. Femoroacetabular impingement (FAI)
ular rim (pincer) or femoral head-neck junction (cam)
deformity have improved the ability to recognize FAI
has been recognized in hip pain and the development of when an active individual presents with hip pain. How-
early hip osteoarthritis. Methods to diagnose this defor- ever, recent studies have suggested a large discrepancy
mity in the young active population have been closely between the high prevalence of radiographic signs of FAI
and the number of symptomatic cases of impingement.6,7
Additional factors in the broader context of the kinetic
From the Department of Physiatry, Hospital for Special Surgery, New York, chain are increasingly being examined to better under-
New York, U.S.A. stand what causes some individuals to have hip
The authors report no conflicts of interest in the authorship and publication
of this article. Full ICMJE author disclosure forms are available for this article impingement pain whereas others with the same
online, as supplementary material. anatomic variant remain asymptomatic.5,8
Received December 2, 2019; accepted August 24, 2020. Lumbo-pelvic motion in the sagittal plane plays a role
Address correspondence to Peter J. Moley, M.D., Hospital for Special Sur- in hip mechanics. The angle between the sacroiliac
gery, 535 E 70th St, New York, NY 10021, U.S.A. E-mail: MoleyP@hss.edu
joints joining the spine and pelvis has increasingly
Ó 2020 Published by Elsevier on behalf of the Arthroscopy Association of
North America become a focus in understanding the complex spine-hip
0749-8063/191473/$36.00 relation.9 Additionally, mobility present in the lower
https://doi.org/10.1016/j.arthro.2020.08.034 spine has the ability to alter lumbo-pelvic movements
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 37, No 1 (January), 2021: pp 149-155 149
Downloaded for Anonymous User (n/a) at Hospital for Special Surgery from ClinicalKey.com by Elsevier on May 18,
2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.150 R. LUO ET AL.
to maintain the center of gravity and hip coverage All male and female patients aged 18 to 45 years who had
during activity.10 These movements, such as an anterior hip pain evaluated by examination and imaging at an
pelvic tilt (PT), can increase relative anterior acetabular ambulatory center for hip pain and joint preservation
coverage and can protect and provoke contact with the between March 2010 and March 2016 and subsequently
femoral head-neck junction.11 In this way, the spine underwent arthroscopic surgical repair were eligible for
and its mechanics play an integral role in our under- inclusion. The exclusion criteria included (1) lack of a
standing of the hip and its associated pathology. diagnosis of symptomatic FAI; (2) a Tönnis classification
Symptomatic hip impingement occurs in younger in- of osteoarthritis of grade 2 or higher at the time of eval-
dividuals participating in cutting and rotational sports. uation; (3) prior lumbar spinal fusion surgery; (4) prior
There are contradictory studies looking at the role of the total hip arthroplasty (THA) or resurfacing surgery; (5)
pelvic incidence (PI) in hip impingement.12-14 Whereas indications for THA or resurfacing surgery at the time of
the PI is fixed, the PT can change, leading some in- evaluation; (6) prior revision surgery on the affected hip;
vestigators to believe that the lumbosacral junction may (7) lack of pelvic radiographs for LSTV determination;
also play a role in the creation of conflict between the and (8) missing electronic records.
femoral head-neck junction and the acetabulum.
Lumbosacral transitional vertebra (LSTV), also known as Data Collection
“Bertolotti syndrome,” is a known congenital condition Patients who met the eligibility criteria were evalu-
in which the transverse process of the fifth lumbar ated for the presence of LSTV anatomy on supine
vertebral body interacts with the sacrum and presents as anteroposterior pelvic radiographs that included the
an enlarged transverse process, a pseudo-joint, or even a pelvic crests and the coccyx-positioned midline. The
fused segment.15,16 It is often an incidental finding on the scoring of LSTV anatomy was determined using the
anteroposterior radiograph of the lumbar spine and is Castellvi classification system,23 which is in wide use in
characterized by 4 bilateral nonerib-bearing transverse the scientific literature, specifically for sacralization.
processes and assimilation of the fifth lumbar vertebra to This classification system is described in Table 1. To
the sacrum.17 The literature reports wide variations in improve inter-rater and intrarater reliability, further
the prevalence of LSTV among different pop- rule restrictions were added to more precisely identify
ulations.16-19 It has also been associated with low-back the anatomic abnormalities and to avoid uncertainty in
pain,15,18,20 with a prevalence of 15% (all types)16,17 or measurements. These additional rules are elucidated in
6.1% (types II-IV)21 in the low-back pain population. Table 1. A post hoc power analysis determined that a
LSTV has been proposed to cause increased shear stress to
the motion segment above during spine flexion and Table 1. Classification of LSTVs
extension. Review studies of LSTV population groups
have shown challenges with PT when compared with LSTV Type Classification Criteria (Modified From Castellvi et al.23)
matched controls owing to restrictions in motion.22 How IA or IB Dysplastic transverse process
the LSTV relates to individuals with symptomatic FAI has A large triangular transverse process 19 mm wide
yet to be explored. As the study of symptomatic FAI is present.
continues to expand and as more attention is placed on The widest aspect of the lateral one-third must be
greater than the widest aspect of the medial two-
pelvic parameters, a better grasp of the relation between thirds.
the lumbo-pelvic complex and the hip becomes essential. The trans-sacral line connecting the most superior
The primary aim of this study was to determine the aspect of the sacrum bilaterally must pass through
prevalence of LSTVs in patients with symptomatic FAI the transverse process in question.
requiring hip arthroscopy. The secondary aim was to IIA or IIB Incomplete lumbarization and/or sacralization
determine whether there is an association between An enlarged transverse process is present with
LSTV anatomy and patient-reported outcomes. We pseudarthrosis with the adjacent sacral ala.
hypothesized that the prevalence of LSTVs in patients Evidence of sclerosis must be shown.
Articulation must be between the transverse process
with FAI would be similar to reported literature values and sacrumdnot the iliac crest or other structures.
in patients with low-back pain. IIIA or IIIB Complete lumbarization and/or sacralization
An enlarged transverse process is present with
Methods complete fusion with the adjacent sacral ala.
The inter-crestal line connecting the most superior
Study Design and Patient Inclusion aspect of each iliac crest must pass through the
This retrospective study was approved by the registry transverse processes.
steering committee and the institutional review board. IV “Mixed”
All study procedures were conducted in accordance with Type IIA is present on one side; type IIIA, on the
the Declaration of Helsinki and its later amendments. other side.
Patients were identified from an institutional hip registry. A, unilateral; B, bilateral; LSTV, lumbosacral transitional vertebra.
Downloaded for Anonymous User (n/a) at Hospital for Special Surgery from ClinicalKey.com by Elsevier on May 18,
2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.LUMBOSACRAL TRANSITIONAL VERTEBRAE AND FAI 151
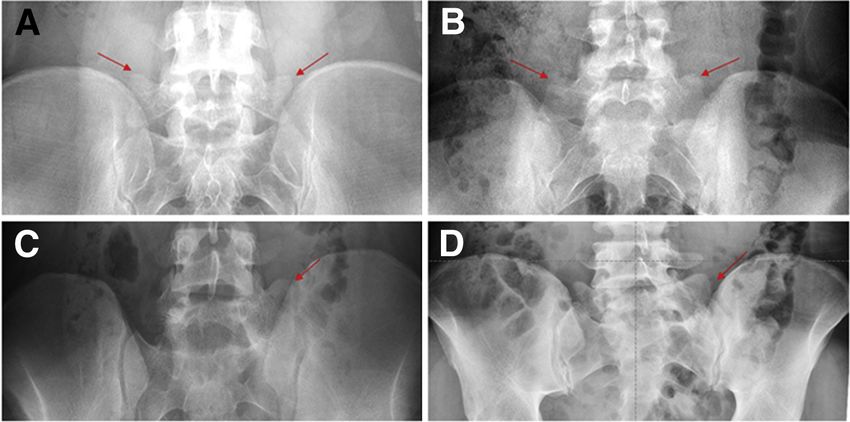
Fig 1. Radiographic classifica-
tion of lumbosacral transitional
vertebrae (arrows), showing
examples of type IB (bilateral
with dysplastic transverse pro-
cess) (A); type IIB (bilateral
with incomplete lumbarization
and/or sacralization) (B); type
IIIA (unilateral, left, with
complete lumbarization and/or
sacralization) (C); and type IV
(mixed) (D) on anteroposterior
pelvic radiographs.
sample size of 45 achieves 82% power with a k of 0.4 coefficients, standard errors, and 95% confidence in-
under the null hypothesis and a k of 0.8 under the tervals (CIs). All parameter estimates from the logistic
alternate hypothesis at an a of .05. Subsequently, data regression are reported as odds ratios, standard errors,
on the presence and sidedness of type I, II, III, or IV and 95% CIs. Statistical significance was defined as
LSTVs in patients with hip pain were analyzed using P < .05. All analyses were performed with Stata,
rate calculations. Radiographic examples of LSTV types version 14.2 (StataCorp, College Station, TX).
are shown in Fig 1.
Patient-Reported Outcomes
Results
As part of the registry, the modified Harris Hip Score Patient Flow
(mHHS),24 Hip Outcome Score (HOS),25 and Inter- An initial review of the patient registry yielded 2,388
national Hip Outcome Tool 33 (iHOT-33) score26 were patients in the age range of 18 to 45 years who pre-
administered to patients at baseline and at 1 year after sented for hip pain and underwent arthroscopic surgical
surgery. The HOS includes an activity of daily living repair between 2010 and 2016. Of these patients, 508
(ADL) scale (HOS-ADL) and a sports scale (HOS- were excluded based on the study criteria (no diagnosis
Sports). All outcome measures are reported on a scale of FAI [n ¼ 90]; no appropriate radiograph of the pelvis
of 0 to 100, with higher scores representing better available [n ¼ 109]; no electronic medical records
function, less difficulty with ADLs and sports, and less available to confirm the diagnosis [n ¼ 115]; and
disability. The minimal clinically important differences revision surgery performed on the affected hip
in the mHHS, HOS-ADL, HOS-Sports, and iHOT-33 [n ¼ 194]). The institutional registry maintains strict
score are 8.2, 8.3, 14.5, and 12.1, respectively.27 criteria and precludes registration of patients with the
radiographic presence of osteoarthritis.
Data Analysis
Continuous variables are presented as means and Demographic Characteristics
standard deviations (SDs), and discrete variables are Among the eligible 1,880 patients, the average age
presented as frequencies and percentages in the was 29.3 years (SD, 8.0 years). Slightly over half of the
descriptive analysis. The HOS-ADL, HOS-Sports, patients were men (n ¼ 1,063; 56.5%). Most patients
mHHS, and iHOT-33 score were available for 50 pa- had unilateral symptoms (n ¼ 1,464; 77.9%).
tients with LSTV anatomy. A 2:1 case-control match
on age (2 years) and sex was performed to compare Reliability of LSTV Classification Scoring
LSTV cases with non-LSTV controls. Analyses of The inter-rater reliability of LSTV classification scoring
changes in patient-reported outcomes per visit by was assessed. Among 60 radiographs, there was 87%
LSTV status were performed using linear regression agreement between an attending physiatrist (P.J.M.)
and including an interaction term with LSTV status and an interventional spine and sports medicine fellow
and discrete time. The association between LSTV (R.L.). This resulted in a statistically significant k of
sidedness and symptom laterality was analyzed using 0.67 (standard error ¼ 0.086), based on an expected
a logistic regression. All parameter estimates from agreement of 60%, and was classified as substantial
the linear regression are reported as regression agreement (P < .001).
Downloaded for Anonymous User (n/a) at Hospital for Special Surgery from ClinicalKey.com by Elsevier on May 18,
2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.152 R. LUO ET AL.
Table 2. Overall Prevalence and Relative Prevalence by Type There were no significant differences in baseline or
and Laterality 1-year postoperative patient-reported outcomes be-
Patients, n Prevalence (of 1,880), % % of Total LSTVs
tween patients with LSTV anatomy and those without it
Type
(Tables 4 and 5). In both groups, all improvements in
IA 104 5.5 39.7 scores at 1 year postoperatively were clinically relevant,
IB 53 2.8 20.2 based on the minimal clinically important difference
IIA 60 3.2 22.9 criteria of 8.2, 8.3, 14.5, and 12.1 for the mHHS,
IIB 25 1.3 9.5 HOS-ADL, HOS-Sports, and iHOT-33 score, respec-
IIIA 8 0.43 3.1
IIIB 0 0 0
tively27 (Tables 4 and 5).
IV 12 0.64 4.6
Total 262 13.9 100 Discussion
A, unilateral; B, bilateral; LSTV, lumbosacral transitional vertebra. In this study of a large cohort of 1,880 patients with
symptomatic FAI, the overall prevalence of LSTVs was
13.9%. Additionally, the prevalence of type II, III, and
LSTV Prevalence IV LSTVs was 5.6%. These prevalence rates were
On the basis of the Castellvi classification system, 262 similar to those reported in low-back pain populations
patients (13.9%) had type I, II, III, or IV transitional in the literature, as hypothesized. There were no sig-
anatomy present. A further analysis of the 262 LSTV nificant associations between the presence of LSTV
types showed that type IA was the most common anatomy and baseline or follow-up patient-reported
(n ¼ 104, 39.7%). Distributions of LSTV by type are outcomes in a cohort of 50 LSTV cases and 100 age- and
shown in Table 2. The prevalence of type II, III, and IV sex-matched, non-LSTV controls.
LSTVs was 5.6% (n ¼ 105). LSTV anatomy was present Not all individuals with signs of anatomic impinge-
unilaterally in 172 patients and bilaterally in 90. The ment have hip pain, but changes to the lumbo-pelvic
mean age of patients with LSTV anatomy was similar to complex can provide insight into how FAI becomes
that of patients without LSTV anatomy (29.6 years symptomatic in a subset of patients. A recent study of
[SD, 7.0 years] vs 29.2 years [SD, 8.1 years]). standing pelvic posture showed that anterior PT
changes the acetabular orientation by decreasing
Unilateral LSTV and Symptomatic Hip Sidedness version and increasing femoral head coverage.28 Simi-
Of the 172 patients with unilateral LSTVs, 89 (52%) larly, analysis of the sitting posture showed that pos-
had left-sided LSTVs and 83 (48%) had right-sided terior PT accommodates hip flexion, and the inability to
LSTVs. Of the 89 patients with left-sided LSTVs, 24 perform the tilt increases relative hip flexion, thus
(27%) had ipsilateral symptoms, 51 (57%) had creating the potential for impingement.14 In conditions
contralateral symptoms, and 14 (16%) had bilateral of abnormal spine mobility, such as with LSTVs, there is
symptoms. Of the 83 patients with right-sided LSTVs, reduced motion in the lumbosacral junction due to the
36 (43%) had ipsilateral symptoms, 30 (36%) had bony articulation or fusion that occurs.29 Consequently,
contralateral symptoms, and 17 (21%) had bilateral the spine does not accommodate the pelvis fully, and
symptoms. Overall, 81 patients (51%) were symptom- the contact forces are distributed unevenly. A recent
atic on the side contralateral to their LSTVs, whereas study showed that patients with fixed spinopelvic pa-
ipsilateral symptoms occurred in 60 patients (35%). In rameters from the standing to sitting position are at
31 patients (18%), regardless of the laterality of their
LSTVs, bilateral symptoms were experienced. When the
Table 3. LSTVs and Symptom Laterality
bilateral symptoms were counted as ipsilateral, 38 pa-
tients (43%) with left-sided LSTVs and 53 patients Odds Ratio (SE) 95% CI P Value
(64%) with right-sided LSTVs had ipsilateral symptoms. Unilateral symptoms only
There was no correlation between LSTV laterality and Intercept 0.5 (0.1) 0.3-0.8 .002*
symptom laterality (k ¼ 0.07, P ¼ .19). However, pa-
Symptom side
Left REF
tients with unilateral right-sided LSTVs were signifi- Right 2.6 (0.9) 1.3-5.1 .007*
cantly more likely to have ipsilateral symptoms (odds Overally
ratio, 2.4; 95% CI, 1.3-4.4; P ¼ .006) compared with Intercept 0.8 (0.2) 0.5-1.1 .170
patients with unilateral left-sided LSTVs (Table 3). Symptom side
Left REF
Right 2.4 (0.7) 1.3-4.4 .006*
Patient-Reported Outcomes
CI, confidence interval; LSTV, lumbosacral transitional vertebra;
The baseline and follow-up mHHS, HOS-ADL, HOS-
REF, reference; SE, standard error.
Sports, and iHOT-33 score were compared between a *P < .05.
subset of 50 patients with LSTV anatomy and 100 age- y
Overall includes bilateral symptoms, which were counted as the
and sex-matched patients without LSTV anatomy. respective LSTV side.
Downloaded for Anonymous User (n/a) at Hospital for Special Surgery from ClinicalKey.com by Elsevier on May 18,
2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.LUMBOSACRAL TRANSITIONAL VERTEBRAE AND FAI 153
Table 4. LSTV Anatomy and Patient-Reported Outcomes
Non-LSTV Controls LSTV Anatomy
Estimate (SE) 95% CI P Value Estimate (SE) 95% CI P Value
Change in mHHS 20.4 (1.9) 16.7-24.1154 R. LUO ET AL.
One question is whether individuals with LSTVs and and contained only patients who underwent arthro-
hip impingement become symptomatic because of a scopic surgery for FAI. Future studies should observe
concomitant decrease in lumbosacral adaptation. In this the prevalence of asymptomatic patients with LSTVs in
scenario, the lumbo-pelvic junction is unable to a similar age group. In the workup of hip impingement,
appropriately adapt during motion. Of the 2,388 pa- radiographs play a major role, and we hope clinicians
tients originally screened for the study, 508 (21%) were can consider the potential role of the lumbosacral
excluded based on lack of pelvic radiographs, lack of junction in their examination and treatment of symp-
electronic records to confirm the diagnosis, or the ex- tomatic patients.
istence of revision surgery. Including these patients and
obtaining appropriate radiographs may have influenced Limitations
the results. Furthermore, owing to the restraints of our This study has several limitations. First, the preva-
study and our specific aim of measuring the prevalence lence of type I LSTVs may have been underestimated
of LSTVs, we did not record PI or version. The majority after the application of additional diagnostic criteria,
of patients in the study did not have the imaging although doing so improved inter-rater reliability.
available for these measurements. Further research is There were no type IIIB LSTV anomalies identified
required to investigate the relation between individuals using current parameters, potentially because of the
with concurrent FAI and lower PI and an increased requirement for the inter-crestal line to pass through
prevalence of LSTVs. the transverse processes. Second, the patients enrolled
In addition, our findings show a slightdbut not sta- were aged 18 to 45 years, and these results may not be
tistically significantdpreponderance toward left-sided generalizable to other age groups. Finally, we did not
LSTVs when unilaterally present, which is consistent include a group with asymptomatic FAI for comparison;
with findings in the literature.35 The exact develop- thus, the prevalence of LSTVs in patients with asymp-
mental mechanism for unilateral sidedness, particularly tomatic FAI remains unknown.
toward the left side, is unknown but may relate to
mutations in HOX1 and HOX2, which contribute to Conclusions
LSTV development.36 In our cohort, the majority of In this large cohort of 1,880 patients with symptom-
left-sided LSTVs had contralateral hip symptoms (57% atic FAI, the prevalence of LSTVs was 13.9%. There was
vs 27% on the ipsilateral side), whereas more right- no correlation between sidedness of unilateral LSTVs
sided LSTVs had ipsilateral hip symptoms (43% vs and the symptomatic hip. Furthermore, there was no
36% on the contralateral side); these differences were association between LSTV anatomy and patient-
statistically significant. Additionally, 18% of patients reported outcomes. The prevalence of LSTVs in this
with unilateral LSTVs had bilateral hip impingement cohort was similar to the prevalence rates previously
symptoms regardless of the laterality. There did not reported in patients with low-back pain.
appear to be a correlation at baseline between sidedness
of unilateral LSTVs and the symptomatic hip. More- Acknowledgment
over, it is unknown whether any of these patients had The authors thank Zafir Abutalib, M.H.S., for con-
concurrent low-back pain or spine conditions. Howev- ducting the statistical analyses.
er, these results are expected because the pelvis moves
as one unit. Our study also revealed no association
between the presence of LSTV anatomy and baseline or References
follow-up patient-reported outcomes; both groups in 1. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H,
the matched analysis reported improvements in out- Siebenrock KA. Femoroacetabular impingement: A cause
comes after arthroscopy. A future goal will be to for osteoarthritis of the hip. Clin Orthop Relat Res 2003:
analyze whether differences in surgical treatment out- 112-120.
comes for FAI occur when both features are ipsilaterally 2. Beall DP, Sweet CF, Martin HD, et al. Imaging findings of
located. femoroacetabular impingement syndrome. Skeletal Radiol
With the ideas proposed in this study, we aimed to 2005;34:691-701.
understand the environment in which hip impinge- 3. Parvizi J, Leunig M, Ganz R. Femoroacetabular impinge-
ment becomes symptomatic and to show anatomic ment. J Am Acad Orthop Surg 2007;15:561-570.
4. Clohisy JC, Carlisle JC, Beaulé PE, et al. A systematic
factors that may affect the outcomes and treatment of
approach to the plain radiographic evaluation of the
FAI. Hip impingement is a multifactorial problem that
young adult hip. J Bone Joint Surg Am 2008;90:47-66
provokes numerous consequences, with a significant (suppl 4).
association with osteoarthritis.1,3 Additionally, other 5. Shin J, Adeyemi TF, Hobson T, Peters CL, Maak TG. The
hip parameters such as femoral version could be bipolar hip: How acetabular and femoral pathomorphol-
assessed and associated with outcomes in patients with ogy affect hip motion in femoral acetabular impingement
LSTVs. Our patient population was one of convenience syndrome. Arthroscopy 2020;36:1864-1871.
Downloaded for Anonymous User (n/a) at Hospital for Special Surgery from ClinicalKey.com by Elsevier on May 18,
2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.LUMBOSACRAL TRANSITIONAL VERTEBRAE AND FAI 155
6. Van Houcke J, Yau WP, Yan CH, et al. Prevalence of 21. Benlidayi IC, Coskun NC, Basaran S. Does lumbosacral
radiographic parameters predisposing to femo- transitional vertebra have any influence on sacral tilt?
roacetabular impingement in young asymptomatic Chi- Spine (Phila Pa 1976) 2015;40:E1176-E1179.
nese and white subjects. J Bone Joint Surg Am 2015;97: 22. Jain A, Agarwal A, Jain S, Shamshery C. Bertolotti syn-
310-317. drome: A diagnostic and management dilemma for pain
7. Mascarenhas VV, Rego P, Dantas P, et al. Imaging prev- physicians. Korean J Pain 2013;26:368-373.
alence of femoroacetabular impingement in symptomatic 23. Castellvi AE, Goldstein LA, Chan DP. Lumbosacral tran-
patients, athletes, and asymptomatic individuals: A sys- sitional vertebrae and their relationship with lumbar
tematic review. Eur J Radiol 2016;85:73-95. extradural defects. Spine (Phila Pa 1976) 1984;9:493-495.
8. Pierannunzii L. Pelvic posture and kinematics in femo- 24. Byrd JW, Jones KS. Prospective analysis of hip arthros-
roacetabular impingement: A systematic review. J Orthop copy with 2-year follow-up. Arthroscopy 2000;16:578-587.
Traumatol 2017;18:187-196. 25. Martin RL, Kelly BT, Philippon MJ. Evidence of validity
9. Rivière C, Hardijzer A, Lazennec JY, Beaulé P, Muirhead- for the Hip Outcome Score. Arthroscopy 2006;22:
Allwood S, Cobb J. Spine-hip relations add un- 1304-1311.
derstandings to the pathophysiology of femoro-acetabular 26. Mohtadi NG, Griffin DR, Pedersen ME, et al. The devel-
impingement: A systematic review. Orthop Traumatol Surg opment and validation of a self-administered quality-of-life
Res 2017;103:549-557. outcome measure for young, active patients with symp-
10. Kim D-H, Park J-K, Jeong M-K. Influences of posterior- tomatic hip disease: The International Hip Outcome Tool
located center of gravity on lumbar extension strength, (iHOT-33). Arthroscopy 2012;28:595-605. quiz 606-610.e1.
balance, and lumbar lordosis in chronic low back pain. 27. Nwachukwu BU, Fields K, Chang B, Nawabi DH,
J Back Musculoskelet Rehabil 2014;27:231-237. Kelly BT, Ranawat AS. Preoperative outcome scores are
11. Ross JR, Nepple JJ, Philippon MJ, Kelly BT, Larson CM, predictive of achieving the minimal clinically important
Bedi A. Effect of changes in pelvic tilt on range of motion difference after arthroscopic treatment of femo-
to impingement and radiographic parameters of acetab- roacetabular impingement. Am J Sports Med 2017;45:
ular morphologic characteristics. Am J Sports Med 2014;42: 612-619.
2402-2409. 28. Dandachli W, Ul Islam S, Richards R, Hall-Craggs M,
12. Grammatopoulos G, Speirs AD, Ng KCG, et al. Acetabular Witt J. The influence of pelvic tilt on acetabular orienta-
and spino-pelvic morphologies are different in subjects tion and cover: A three-dimensional computerised to-
with symptomatic cam femoro-acetabular impingement. mography analysis. Hip Int 2013;23:87-92.
J Orthop Res 2018;36:1840-1848. 29. Brenner AK. Use of lumbosacral region manipulation and
13. Hellman MD, Haughom BD, Brown NM, Fillingham YA, therapeutic exercises for a patient with a lumbosacral
Philippon MJ, Nho SJ. Femoroacetabular impingement transitional vertebra and low back pain. J Orthop Sports
and pelvic incidence: Radiographic comparison to an Phys Ther 2005;35:368-376.
asymptomatic control. Arthroscopy 2017;33:545-550. 30. Esposito CI, Carroll KM, Sculco PK, Padgett DE,
14. Fader RR, Tao MA, Gaudiani MA, et al. The role of lumbar Jerabek SA, Mayman DJ. Total hip arthroplasty patients
lordosis and pelvic sagittal balance in femoroacetabular with fixed spinopelvic alignment are at higher risk of hip
impingement. Bone Joint J 2018;100-b:1275-1279. dislocation. J Arthroplasty 2018;33:1449-1454.
15. Bertolotti M. Contributo alla conoscenza dei vizi di dif- 31. Nardo L, Alizai H, Virayavanich W, et al. Lumbosacral
ferenzazione regionale del rachide con speciale riguardo transitional vertebrae: Association with low back pain.
all’ assimilazione sacrale della v. lombare. Radiol Med Radiology 2012;265:497-503.
1917;4:113-144 [in Italian]. 32. Tini PG, Wieser C, Zinn WM. The transitional vertebra of
16. Vergauwen S, Parizel PM, van Breusegem L, et al. Dis- the lumbosacral spine: Its radiological classification, inci-
tribution and incidence of degenerative spine changes in dence, prevalence, and clinical significance. Rheumatol
patients with a lumbo-sacral transitional vertebra. Eur Rehabil 1977;16:180-185.
Spine J 1997;6:168-172. 33. Luoma K, Vehmas T, Raininko R, Luukkonen R,
17. Quinlan JF, Duke D, Eustace S. Bertolotti’s syndrome. A Riihimaki H. Lumbosacral transitional vertebra: Relation
cause of back pain in young people. J Bone Joint Surg Br to disc degeneration and low back pain. Spine (Phila Pa
2006;88:1183-1186. 1976) 2004;29:200-205.
18. Tang M, Yang XF, Yang SW, et al. Lumbosacral transi- 34. Connolly LP, Drubach LA, Connolly SA, Treves ST. Young
tional vertebra in a population-based study of 5860 in- athletes with low back pain: Skeletal scintigraphy of
dividuals: Prevalence and relationship to low back pain. conditions other than pars interarticularis stress. Clin Nucl
Eur J Radiol 2014;83:1679-1682. Med 2004;29:689-693.
19. French HD, Somasundaram AJ, Schaefer NR, 35. Dzupa V, Slepanek M, Striz M, et al. Developmental
Laherty RW. Lumbosacral transitional vertebrae and its malformations in the area of the lumbosacral transitional
prevalence in the Australian population. Glob Spine J vertebrae and sacrum: Differences in gender and left/right
2014;4:229-232. distribution. Surg Radiol Anat 2014;36:689-693.
20. Gopalan B, Yerramshetty JS. Lumbosacral transitional 36. Jancuska JM, Spivak JM, Bendo JA. A review of symp-
vertebra-related low back pain: Resolving the contro- tomatic lumbosacral transitional vertebrae: Bertolotti’s
versy. Asian Spine J 2018;12:407-415. syndrome. Int J Spine Surg 2015;9:42.
Downloaded for Anonymous User (n/a) at Hospital for Special Surgery from ClinicalKey.com by Elsevier on May 18,
2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.You can also read

















































