POCUS series: ultrasound during cardiopulmonary resuscitation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Netherlands Journal of Critical Care
Submitted February 2021; Accepted May 2021
REVIEW
POCUS series: ultrasound during cardiopulmonary
resuscitation
T.H.Gijtenbeek1, J. E. Lopez Matta1,3, P.R. Tuinman2,3, M.E. Haaksma2,3, M.L.A. Heldeweg2,3, J.M. Smit2,3, D.J. van Westerloo1,3,
J.A. Janson1,3, C.V. Elzo Kraemer1
Department of Intensive Care, Leiden University Medical Center, Leiden, the Netherlands
1
Department of Intensive Care, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam
2
Amsterdam Leiden Intensive care Focused Echography (ALIFE, www.alifeofpocus.com)
3
Correspondence
C.V. Elzo Kraemer - cvelzokraemer@lumc.nl
Keywords - ultrasound, POCUS, cardiopulmonary resuscitation
Abstract Protocols and training
This article is part of the point-of-care ultrasound (POCUS) series. Many POCUS protocols have been developed, each with their
During cardiopulmonary resuscitation, bedside ultrasound has own acronym, set of diagnostic algorithms, and required
important clinical value for confirming a diagnosis, establishing a training (examples in table 1).[4-6] What they all have in common
prognosis and in therapeutic decision-making. In this article we is the focus on the cardiac view from the subxiphoid window.
provide a practical review on how to implement and apply POCUS Any other cardiac window can be chosen in ACLS protocols,
during cardiopulmonary resuscitation and discuss its merits and provided interference with thoracic compressions is avoided.[4-6]
pitfalls. The differences in these protocols are mainly found in whether
they include pulmonary, abdominal and vascular examinations.
Introduction Also the order of sequence in which these organ systems are
Point-of-care ultrasound (POCUS) has shown promise in a variety evaluated differs. Applying such a protocol provides a standard
of clinical scenarios. In most emergency wards and intensive care of care for quality and training purposes and most of these
departments, ultrasound devices are standard equipment and protocols are being evaluated in studies on clinical outcome.
ultrasound skills are becoming more commonplace. An increasing Regardless of the protocol chosen, team training is essential
amount of evidence has been acquired from large clinical studies to appropriately integrate POCUS into the workflow of ACLS.
indicating the added diagnostic and prognostic value of dedicated Delays in the rhythm check can easily be caused, but should
ultrasound application during cardiac arrest.[1] During advanced be avoided at all costs. The operator should therefore be
cardiac life support (ACLS) in a patient in cardiac arrest, the skilled enough to make and save the required images during
establishment of a diagnosis and the early start of specific therapies the rhythm checks, with timeframes of no more than 10 sec.
can improve outcome. Next, the operator must systematically review the results
The traditional approach for the identification of treatable with the team members during the next CPR cycle. Given the
causes during a cardiac arrest can nowadays be bolstered by the demands these requirements take on the person performing
implementation of ultrasound. The merits of POCUS during ACLS the POCUS examination (figure 2), delegating the task of team
are threefold. Firstly, the use of POCUS improves standard ACLS, leader to another ACLS member should be considered early,
by confirming the return of spontaneous circulation (ROSC), based because maintaining an adequate level of situational awareness
on the presence of cardiac motion and carotid flow. Secondly, may not be possible during sonography. A therapeutic strategy
POCUS has proven to be a reliable tool for providing an ‘on the can be chosen from team-based decision-making and this may
spot’ diagnosis for common causes of cardiac arrest and to shorten improve the effectiveness of ACLS.[4-6]
time to treatment.[1-3] And lastly, POCUS may be used during Bringing POCUS to this performance level in cardiopulmonary
ACLS for prognostication of survival. Several clinical algorithms resuscitation requires practice during advanced life support
have been developed for the use of POCUS during cardiac arrest. training. This improves time efficiency and the overall
In this article, we provide a practical review on the use of POCUS performance of the team (figure 3).[6] Specific criteria for an
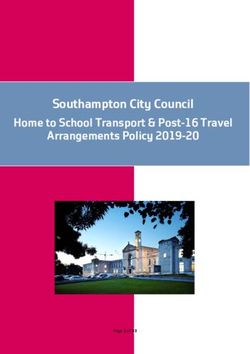
in ACLS, with our main focus on the subxiphoid view (figure 1).[2,3] adequate performance level could not be found in the literature.
170 NETH J CRIT CARE - VOLUME 29 - NO 4 - JULY 2021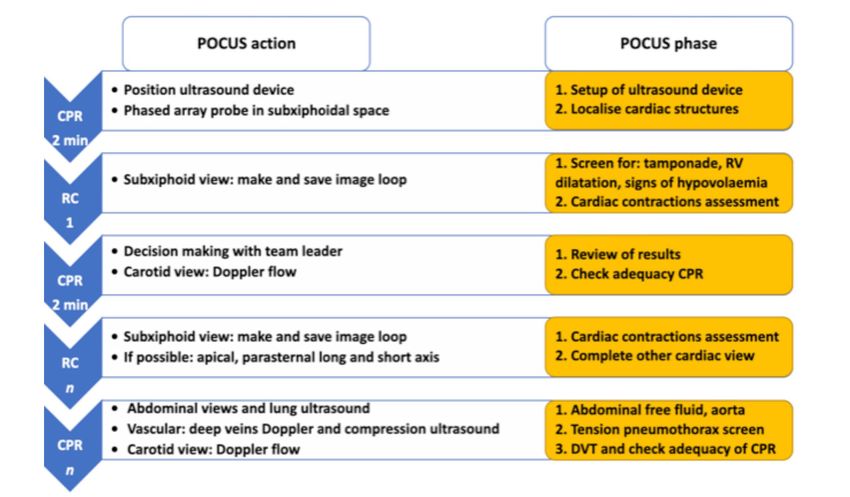
Netherlands Journal of Critical Care
Ultrasound during cardiopulmonary resuscitation
Figure 1. A) Frozen image of the subxiphoid view from a patient without cardiac pathology. B) Subxiphoid view (rotation of probe from position A), inflow from the vena
cava into the right atrium. C) Pathology: Dilated right atrium and right ventricle, with shift from interatrial septum and interventricular septum to the left. D) Pathology:
Pericardial fluid resulting in cardiac tamponade
RA = right atrium; RV = right ventricle; LA = left atrium; LV = left ventricle; IVC = inferior vena cava; HV = hepatic vein; DRA = dilated right atrium; DRV = dilated right
ventricle; PE = pericardial effusion
Figure 2. The main recommendation is to separate the role of team leader (red) and the person performing the POCUS (green). During CPR, the probe should be placed
in the correct position for the required view. Images can then be made during the rhythm check and the results discussed in the next cycle.
NETH J CRIT CARE - VOLUME 29 - NO 4 - JULY 2021 171
Netherlands Journal of Critical Care
Ultrasound during cardiopulmonary resuscitation
Table 1. POCUS protocols for CPR ultrasound
COACHRED FEEL CASA POCUS PEA CAUSE SESAME
Cardiac 1 1 1 1 2 1 4
Subxiphoid view ✓ ✓ ✓ ✓ ✓ ✓ ✓
Inclusion other views ✓ ✓ ✓ ✓ — ✓ ✓
Tamponade ✓ ✓ ✓ ✓ ✓ ✓ ✓
Right ventricular strain ✓ ✓ ✓ ✓ — ✓ ✓
Cardiac wall motion ✓ ✓ ✓ ✓ ✓ ✓ ✓
Hypovolaemia ✓ ✓ ✓ ✓ ✓ ✓ ✓
Regional wall abnormality ✓ ✓ ✓ ✓ — ✓ ✓
Pulmonary — — 2 4 1 2 1
Pneumothorax — — ✓ ✓ ✓ ✓ ✓
Consolidation — — — — — — ✓
Pleural effusion — — — — — — ✓
Abdominal — — 3 2 3 — 3
Aortic rupture — — ✓ ✓ ✓ — ✓
Peritoneal fluid — — ✓ ✓ ✓ — ✓
Vascular — — — 3 4 — 2
Carotid flow — — — — — — —
Distal venous thrombosis — — — ✓ ✓ — ✓
COACHRED: Continue compressions, Oxygen away, All others away, Charging, Hands off, Evaluate rhythm and Defibrillate or Disarm charge
FEEL: Focused Echocardiographic Evaluation in Life support
CASA: Cardiac Arrest Sonographic Assessment
POCUS: Point Of Care UltraSound
PEA: Pulmonary; Epigastric; Abdominal scans
CAUSE: Cardiac Arrest Ultrasound Exam
SESAME: (originally SESAMOOSIC) Sequential Emergency Scanning Assessing Mechanism Or Origin of Shock of Indistinct Cause
The numbers in the table indicate the order of acquisition of views, pathology or organ system. ✓ : included in exam. — : not included in exam
In general, being certified for an already existing ultrasound the rhythm check.[4,6] Other cardiac views, such as the apical,
protocol, having received a period of supervision or reviews parasternal short-axis and long-axis views are usually less
from peers and maintaining the obtained skills with a minimum appropriate and inaccessible since these views generally require
amount of images per unit of time should suffice. Incorporating more time to acquire and interfere with the resuscitation
ultrasound in regular ACLS training should condition the team procedure.[7] Views directed at excluding tension pneumothorax
for the presence of POCUS during a real event. or at signs of pulmonary embolism (e.g. venous duplex exam of
As previous studies have pointed out, adhering to and practising popliteal and femoral veins) can be incorporated as a next step,
established ultrasound protocols is necessary to benefit from as is done in the SESAME protocol of Lichtenstein.[2]
POCUS, without interfering with the standards of care of ACLS.[6]
Quality of CPR, presence of cardiac activity and
Technique confirmation of ROSC
As mentioned in the previous section, the only moment for Recently, two studies were performed that compared ultrasound
acquiring images is during the rhythm check. Usage of this detection of flow through the carotid artery with manual
limited timeframe should be optimised by placing the phased array carotid pulse palpation.[8,9] Badra et al. found that ultrasound
probe (cardiac probe) in the subxiphoidal space in anticipation of pulse confirmation was more successful than manual palpation
172 NETH J CRIT CARE - VOLUME 29 - NO 4 - JULY 2021Netherlands Journal of Critical Care
Ultrasound during cardiopulmonary resuscitation
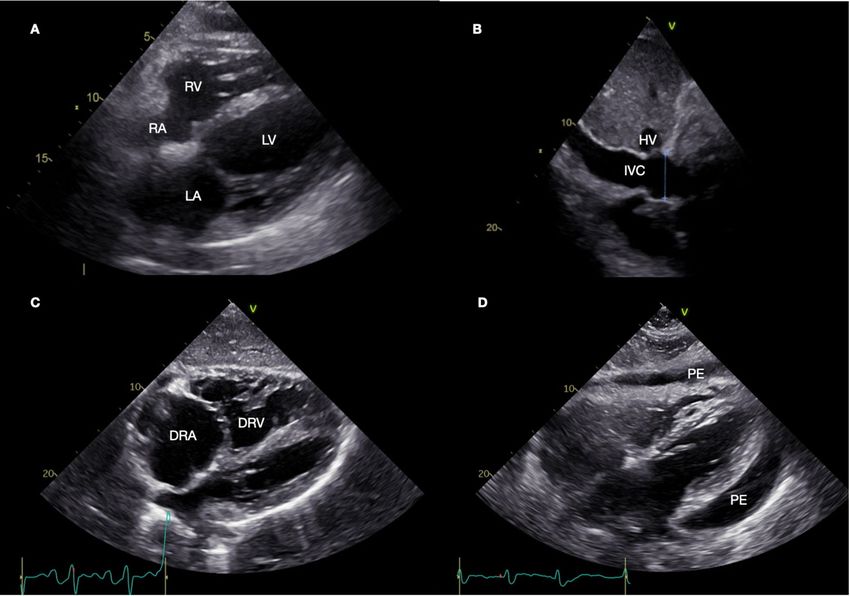
Figure 3. Flowchart showing the deployment phases of POCUS during ongoing ACLS. Every specific action of POCUS connects to a diagnostic ultrasound phase. These
actions and phases should be assigned to either the rhythm check (RC) or thoracic compression blocks (CPR). In this way POCUS can follow the ACLS workflow and reach
completion in a limited number of blocks. This proposed flowchart is based on the concept that a dedicated POCUS ACLS member can obtain a complete evaluation and
that priority is given to the subxiphoid view.
in healthy volunteers, with ultrasound being correct in 99.1% Diagnosing specific causes and guidance of treatment
of cases, whereas manual palpation was correct in only 85.6% The findings obtained during POCUS-guided ACLS may lead to
(pNetherlands Journal of Critical Care
Ultrasound during cardiopulmonary resuscitation
Cardiac tamponade Prognostication
Cardiac tamponade can be easily diagnosed by POCUS. Pericardial Life support assisted by POCUS can also be used for predicting the
effusions can be visualised as an increased space (usually >10 mm) prognosis of resuscitation efforts. In a non-randomised prospective
separating the two pericardial layers. The earliest signs of tamponade study of 223 patients, those with absent cardiac activity on ultrasound
are a widened inferior vena cava and atrial late systolic collapse. were less likely to have a return of spontaneous circulation (ROSC)
Later in the process, early diastolic right ventricular collapse may be than those with activity: 19.5% ROSC (95% CI 13-25%) vs 76%
observed.[11] POCUS examination for the clinical question of cardiac ROSC (95% CI 57-94%).[16] Beckett et al. performed a study in cardiac
tamponade has excellent diagnostic accuracy with a sensitivity of arrest patients presenting to the emergency ward. When asystole
96% and a specificity of 98%.[11] Amongst the common pitfalls is was seen on ultrasound, survival to discharge was only 0.8%.[17]
mistaking epicardial fat for pericardial effusion or intrapericardial In a systematic review of 1486 patients, visible cardiac activity on
thrombus. During the assessment, one should keep in mind that ultrasound was associated with an odds ratio for survival to hospital
pericardial fat is usually hyperechoic as compared with pericardial discharge of 8.03 (95% CI 3.01-21.39) compared with absence of
effusions and does not cause compression of the atria and ventricles. cardiac activity.[18] The ACLS teams in the included studies were not
Pericardial collections consisting of pus, fibrin-rich material or blinded, making the review vulnerable to bias. A second systematic
haematoma will usually have a more inhomogeneous appearance review, however, found similar results.[19] Based on the trend in these
with varying echogenicity. These can be regionally localised and studies, it may be argued that presence of cardiac activity on POCUS
are therefore more easy to miss on a single subxiphoid view. When warrants continuation of resuscitation.[20,21]
pericardial fluid is found to be the cause of cardiac arrest, immediate Integrating POCUS into resuscitation care may therefore lead to
needle pericardiocentesis should be performed.[11,14] Circulation can more patients achieving ROSC and prevent premature cessation
be immediately restored in a significant proportion of cases.[8] of resuscitation efforts, by continuing CPR in those with cardiac
contractions on ultrasound, irrespective of the tracings on
Hypovolaemia the ECG. The presumed rationale behind it is that POCUS
Ultrasound can be used to diagnose hypovolaemia, indicating the distinguishes those patients with unrecoverable cardiac standstill
need for aggressive fluid resuscitation. However, the collapsability from those that still have recoverable heart function (e.g. pseudo-
of the inferior vena cava (IVC) is unreliable as a parameter for fluid pulseless electrical activity, low grade ventricular fibrillation, and
responsiveness. Many factors, including chest compressions and incorrect diagnosis of asystole).
positive pressure ventilation, can alter the diagnostic accuracy of
IVC diameter and collapsability Therefore, relying on ultrasound Limitations
alone to determine hypovolaemia as the cause for cardiac arrest is One of the important points to consider is that up to this point in
likely to be inaccurate. However, collapsing hyperdynamic atria and/ time, randomised trials have not been performed to definitely prove
or ventricles can be seen in extreme cases. ROSC can be achieved that POCUS improves outcome. Yet, in individual cases performing
when adequate preload is restored.[11] POCUS can be decisive in finding a treatable cause of cardiac arrest.
In this regard, a crucial limitation of POCUS assisted ACLS is that
Tension pneumothorax POCUS may prolong the rhythm check. This potentially reduces
Tension pneumothorax can be reliably diagnosed in patients with the effectiveness of the cardiopulmonary resuscitation and thereby
spontaneous circulation, without mechanical ventilation. Absence of an immediate reduction in cerebral blood flow.[22]
ultrasound ‘lung sliding’ between the visceral and parietal pleura has a One study found a medium increase of 6 sec in the duration of
sensitivity of over 92% and specificity of 99% for pneumothorax. The the pulse check pause by applying ultrasound.[23] Two factors were
visualisation of a ‘lung point’ carries a specificity for pneumothorax identified to influence the increase. The first factor was the level of
close to 100%.[11] It is likely that these percentages can still be ultrasound skill and the second was related to the POCUS provider
approximated in intubated patients during CPR, as long as the tube being the resuscitation leader at the same time. In another study of
has been placed at the correct depth such that both lungs are equally 23 patients, an increase in mean pulse check duration of 8.4 sec was
ventilated by either a bag-mask-valve apparatus or mechanical found.[24] The prerequisites of the POCUS provider are therefore
ventilator. Abdominal ultrasound is usually not part of POCUS an adequate training level and delegating the team leadership task.
during cardiopulmonary resuscitation, but significant free fluid can Resuscitation efforts can be unnecessarily obstructed if too much
be reliably excluded and signs for a ruptured aortic aneurysm can emphasis is placed on taking better images. Placing the probe in
be found.[9] The ultrasound sensitivity and specificity of experienced advance during ongoing CPR may prevent this from happening.
sonographers for diagnosing abdominal aortic aneurysms can Other modalities for obtaining a diagnosis should be sought if acquiring
reach 99% and 98%, respectively.[15] The Focussed Assessment with adequate images is simply not possible. At all times, priority should
Sonography in Trauma (FAST) protocol can be followed to screen be given to recommencing high-quality chest compressions after
for intrapericardial and intraperitoneal free fluid. The FAST exam completing the rhythm check. Preventing delays in administering
consists of a subxiphoid, left flank, right flank view and pelvic view.[15] defibrillation during ventricular fibrillation equally applies.
174 NETH J CRIT CARE - VOLUME 29 - NO 4 - JULY 2021Netherlands Journal of Critical Care
Ultrasound during cardiopulmonary resuscitation
5. Finn TE, Ward JL, Wu CT, Giles A. COACHRED: A protocol for the safe and timely
The time for producing adequate images is therefore highly limited.
incorporation of focused echocardiography into the rhythm check during
Saving images provides the opportunity to analyse these during the cardiopulmonary resuscitation. Emerg Med Australas. 2019;31:1115-8.
6. Clattenburg EJ, Wroe PC, Gardner K, et al. Implementation of the Cardiac Arrest
next cycle of compressions.[25] Taken together, POCUS may only Sonographic Assessment (CASA) protocol for patients with cardiac arrest is
be of use during ACLS if it is performed swiftly by experienced associated with shorter CPR pulse checks. Resuscitation. 2018;131:69-73.
7. Atkinson P, Bowra J, Milne J, et al. International Federation for Emergency Medicine
sonographers and only minimally increases down time during Consensus Statement: Sonography in hypotension and cardiac arrest (SHoC): An
ACLS compressions. international consensus on the use of point of care ultrasound for undifferentiated
hypotension and during cardiac arrest. CJEM. 2017;19:459-70.
8. Sanchez S, Miller, Asha S. Assessing the validity of two-dimensional carotid
Future directions ultrasound to detect the presence and absence of a pulse. Resuscitation.
2020;157:67-73.
Transoesophageal echocardiography (TEE) has the potential to 9. Badra K, Coutin A, Simard R, et al. The POCUS pulse check: A randomized controlled
overcome the limitations mentioned in the previous section. For a crossover study comparing pulse detection by palpation versus by point-of-care
ultrasound. Resuscitation. 2019;139:17-23.
detail explanation of POCUS-TEE, see our recent POCUS-article 10. Breitkreutz R, Price S, Steiger HV, et al. Focused echocardiographic evaluation in life
about this topic.[26] This technique allows cardiac images to be support and peri-resuscitation of emergency patients: A prospective trial.
Resuscitation. 2010;81:1527-33.
taken without disrupting the CPR cycles. One retrospective study 11. Long B, Alerhand S, Maliel K, Koyfman A. Echocardiography in cardiac arrest: An
emergency medicine review. Am J Emerg Med. 2018;36:488-93.
of 139 pulse checks by Fair et al. showed that TEE had a shorter
12. Milne J, Atkinson P, Lewis D, Fraser J. Sonography in Hypotension and Cardiac
mean compression pause of 9 sec (95% CI 5-12 sec) as compared Arrest (SHoC): Rates of Abnormal Findings in Undifferentiated Hypotension and
During Cardiac Arrest as a Basis for Consensus on a Hierarchical Point of Care
with TTE: 19 sec (95% CI 16-22 sec).[27] Measuring colour Ultrasound Protocol. Cureus. 2016;8:1-6.
Doppler flow from transoesophageal images allows for continuous 13. Piggott Z, Jelic T, Pulmonary embolism with cardiac arrest: a STEMI patient’s
unexpected course. CJEM. 2018;20:31-6.
monitoring of the adequacy of thoracic compression. Furthermore, 14. Schellenberg M, Inaba K, Critical Decisions in the Management of Thoracic Trauma.
TEE can be used to detect left ventricular outflow tract Emerg Med Clin N Am. 2018;36:135-47.
15. Whitson MR, Mayo PH. Ultrasonography in the emergency department. Mayo Crit
obstruction caused by malpositioned thoracic compressions.[28] Care. 2016;20:227:1-8.
These and other studies conducted on the application of TEE 16. Atkinson P, Beckett N, French J, Banerjee A, Fraser J, Lewis D. Does Point-of-care
Ultrasound Use Impact Resuscitation Length, Rates of Intervention, and Clinical
during CPR have shown promising results.[29,30] Outcomes During Cardiac Arrest? A Study from the Sonography in Hypotension
and Cardiac Arrest in the Emergency Department (SHoC-ED) Investigators. Cureus.
2019;11:1-9.
Conclusion 17. Beckett N, Atkinson P, Fraser J, et al. Do combined ultrasound and
The application of POCUS has opened up new vistas for improving electrocardiogram- rhythm findings predict survival in emergency department
cardiac arrest patients? The Second Sonography in Hypotension and Cardiac Arrest
ACLS, by aiding in establishing a diagnosis, implementing specific in the Emergency Department (SHoC-ED2) study. CJEM. 2019;21:739-43.
18. Lalande E, Burwash-Brennan T, Burns K, et al. Is point-of-care ultrasound a reliable
treatments and prognostication. The subxiphoidal view can be
predictor of outcome during atraumatic, non-shockable cardiac arrest? A
quickly obtained at the bedside, with modest ultrasound skills. systematic review and meta-analysis from the SHoC investigators. Resuscitation.
2019; 139:159-66.
Obtaining other cardiac views can be included as long as the cycles 19. Kedan I, Ciozda W, Palatinus JA, Palatinus HN, Kimchi A. Prognostic value of point-
of thoracic compressions are not interrupted. A holistic diagnostic of-care ultrasound during cardiac arrest: a systematic review. Cardiovasc
Ultrasound. 2020;18:1-10.
approach, in which pulmonary and abdominal pathology are sought 20. Lalande E, Woo MY. POCUS predicts prognosis in cardiac arrest. CJEM. 2019;21:689-
after, as well as deep vein thrombosis, only adds to the value that 90.
21. Reynolds JC, Del Rios M. Point-of-care cardiac ultrasound during cardiac arrest: a
ultrasound skills have to offer. POCUS should therefore be an reliable tool for termination of resuscitation? Curr Opin Crit Care. 2020;26:603-11.
integral part of the practice of ACLS. 22. De Wilde RBP, Helmerhorst HJF, Westerloo DJ. Cerebral blood flow velocity during
chest compressions in cardiac arrest. Neth J Crit Care. 2017;25:137-9.
23. Clattenburg EJ, Wroe P, Brown S, et al. Point-of-care ultrasound use in patients with
Disclosures cardiac arrest is associated prolonged cardiopulmonary resuscitation pauses: A
prospective cohort study. Resuscitation. 2018;122:65-8.
All authors declare no conflict of interest. No funding or financial 24. Huis in ’t Veld MA, Allison MG, Bostick DS, et al. Ultrasound use during
support was received. cardiopulmonary resuscitation is associated with delays in chest compressions.
Resuscitation. 2017;119: 95-8.
25. Smallwood N, Dachsel M. Point-of-care ultrasound (POCUS): unnecessary gadgetry
or evidence-based medicine? Clin Med. 2018;18:219-24.
Acknowledgements
26. Elzo Kraemer CV, López Matta JE, Friedericy HJ, Elzo Kraemer AX. POCUS series:
We would like to thank Bostjan van Hemel for his assistance with Focused transoesophageal echocardiography, a view from the inside. Neth J Crit
Care May 2021;29:130-9.
the illustrations in figure 2. 27. Fair III J, Mallin MP, Adler A, et al. Transesophageal Echocardiography During
Cardiopulmonary Resuscitation Is Associated With Shorter Compression Pauses
Compared With Transthoracic Echocardiography. Ann Emerg Med. 2019;73:610-6.
References 28. Hwang SO, Zhao PG, Choi HJ, et al. Compression of the Left Ventricular Outflow
Tract During Cardiopulmonary Resuscitation. Acad Emerg Med. 2019;16:928-33.
1. Hussein L, Rehman MA, Sajid R, Annajjar F, Al-Janabi T. Bedside ultrasound in 29. Teran F, Prats MI, Nelson BP, et al. Focused Transesophageal Echocardiography
cardiac standstill: a clinical review. Ultrasound J. 2019;11:1-8. During Cardiac Arrest Resuscitation: JACC Review Topic of the Week. J Am Coll
2. Blanco P, Martínez Buendía C, Point-of-care ultrasound in cardiopulmonary Cardiol. 2020;76:745-54.
resuscitation: a concise review. J Ultrasound. 2017;20:193-8. 30. Orihashi K. Transesophageal Echocardiography During Cardiopulmonary
3. Atkinson P, Taylor L, Milne J, Diegelmann L. Does Point of Care Ultrasound Improve Resuscitation (CPR-TEE). Circulation. 2020;84:820-4.
Resuscitation Markers in Undifferentiated Hypotension? An International
Randomized Controlled Trial From The Sonography in Hypotension and Cardiac
Arrest in the Emergency Department (SHoC-ED) Series. Cureus. 2020;12:1-8.
4. Niewiara S, Strychar J, Liniarski M, Kilian T, et al. Ultrasonography protocols used in
the diagnosis of reversible causes of cardiac arrest. J Publ Health Nurs Med Rescue.
2017;6:13-23.
NETH J CRIT CARE - VOLUME 29 - NO 4 - JULY 2021 175You can also read