Patient satisfaction and experience at migrant health centres in Turkey
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Patient satisfaction and experience at migrant health centres in Turkey

Abstract
A cross-sectional study of patients attending migrant health centres in 16 provinces in Turkey showed an overall
satisfaction rate of 78.2% with health services. This is relatively high compared with similar studies that have
evaluated services provided by a specialized unit for refugees or with sensitivity to language and cultural needs. The
service with the highest satisfaction rate was psychological or social assistance (84.8%). Factors related to service
and communication were significant determinants of patient satisfaction. Respondents who received explanations
of their medical condition from the doctor were 8.9 times more likely to be satisfied. Respondents who felt that they
had enough time with the health worker or received a comprehensive examination and respect from both doctors
and nurses were more likely to be satisfied. The amount of time spent waiting to see a health worker was also a
significant predictor of patient satisfaction. Some improvements in physician–patient interaction and communication
are recommended to empower patients to participate in managing their treatment and overall health.
Keywords © World Health Organization 2021
Some rights reserved. This work is available under the Creative Commons Attribution-
REFUGEE NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://
PATIENT SATISFACTION creativecommons.org/licenses/by-nc-sa/3.0/igo).
CLIENT SATISFACTION Under the terms of this licence, you may copy, redistribute and adapt the work for non-
REFUGEE HEALTH commercial purposes, provided the work is appropriately cited, as indicated below. In
any use of this work, there should be no suggestion that WHO endorses any specific
organization, products or services. The use of the WHO logo is not permitted. If you
adapt the work, then you must license your work under the same or equivalent Creative
Commons licence. If you create a translation of this work, you should add the following
disclaimer along with the suggested citation: “This translation was not created by the
World Health Organization (WHO). WHO is not responsible for the content or accuracy
of this translation. The original English edition shall be the binding and authentic edition:
Patient satisfaction and experience at migrant health centres in Turkey. Copenhagen:
WHO Regional Office for Europe; 2021”.
Any mediation relating to disputes arising under the licence shall be conducted in
accordance with the mediation rules of the World Intellectual Property Organization.
(http://www.wipo.int/amc/en/mediation/rules/).
Document number:
Suggested citation. Patient satisfaction and experience at migrant health centres in
WHO/EURO:2021-2488-42244-58324 Turkey. Copenhagen: WHO Regional Office for Europe; 2021. Licence: CC BY-NC-SA 3.0
IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/
bookorders. To submit requests for commercial use and queries on rights and licensing,
see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a
third party, such as tables, figures or images, it is your responsibility to determine whether
permission is needed for that reuse and to obtain permission from the copyright holder.
The risk of claims resulting from infringement of any third-party-owned component in the
work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material
in this publication do not imply the expression of any opinion whatsoever on the part of
WHO concerning the legal status of any country, territory, city or area or of its authorities,
or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on
maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply
that they are endorsed or recommended by WHO in preference to others of a similar
nature that are not mentioned. Errors and omissions excepted, the names of proprietary
products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained
in this publication. However, the published material is being distributed without warranty
of any kind, either expressed or implied. The responsibility for the interpretation and use
Photo coverpage: © SIHHAT of the material lies with the reader. In no event shall WHO be liable for damages arising
Design and layout: 4PLUS4.dk from its use.
Patient satisfaction and experience at migrant health centres in Turkey


iii Contents Preface............................................................................................................................. iv Acknowledgements........................................................................................................... v Abbreviations.................................................................................................................... v Executive summary........................................................................................................... vi Introduction....................................................................................................................... 1 Background............................................................................................................................................ 1 Methodology.......................................................................................................................................... 3 Results.............................................................................................................................. 7 Sociodemographic characteristics of participants........................................................................ 7 Access and utilization of services in MHCs..................................................................................... 8 Patient experience at MHCs............................................................................................................... 10 Patient satisfaction............................................................................................................................... 13 Determinants of patient satisfaction and experience.................................................................... 16 Discussion......................................................................................................................... 19 Patient satisfaction and expectations.............................................................................................. 19 Factors that determine patient satisfaction in MHCs.................................................................... 20 Strengths and limitations.................................................................................................................... 21 Patient feedback mechanisms........................................................................................................... 21 Recommendations............................................................................................................................... 22 Conclusions...................................................................................................................... 23 References........................................................................................................................ 24 Annex 1. Patient satisfaction form..................................................................................... 28 Annex 2. Patient experience by type of facility................................................................... 33
iv
Preface
The conflict in the Syrian Arab Republic has caused one (Improving the health status of the Syrian population
of the world’s largest and most dynamic displacement under temporary protection and related services
crises, affecting millions of lives. WHO is supporting the provided by Turkish authorities) project that is funded
response to the crisis through its operations in Turkey, by the European Union (EU). This project operates under
which comprise a cross-border response from the field the EU’s Facility for Refugees in Turkey and focuses on
office in Gaziantep and a health response to refugees strengthening the provision of primary and secondary
in Turkey, coordinated by the WHO Country Office in health services to Syrian migrant/refugee, building and
Ankara. In north-western Syrian Arab Republic, WHO supporting a network of migrant health centres across
is implementing interventions such as the delivery of the country, and employing additional health personnel,
vital medicines and medical supplies and providing including Syrian doctors and nurses.
support for the operational costs of health facilities and
capacity-building of health staff. Through the Refugee In November 2018 the Refugee Health Programme
Health Programme in Turkey, efforts have been made conducted the Workshop on Refugee and Migrant
to strengthen the national health system through Health in Turkey: Survey and Research Consultation to
integrating Syrian health workers and translators, identify gaps in the information and evidence required
building capacity for mental health care, providing for Programme development and adaptation and for
linguistic and culturally sensitive health services, and informing policies on migrant health in Turkey. The
supporting home care for older refugees and those with Workshop brought together more than 57 national and
disabilities. international experts from academia, the Ministry of
Health, United Nations agencies and WHO collaborating
Activities of the Programme are defined within the centres and led to the formulation of the Programme’s
scope of the Regional Refugee and Resilience Plan research framework. Within this framework, a series
2018–2019, a broad partnership platform for over of studies was implemented in the fields of mental
270 development and humanitarian partners to health, health literacy, women and child health, health
provide coordinated support in countries bordering workforce, and noncommunicable diseases. This study,
the Syrian Arab Republic that are heavily impacted by Patient satisfaction and experience at migrant health
the influx of refugees. This platform capitalizes on the centres in Turkey, is one of the studies implemented
knowledge, capacities and resources of humanitarian within the Refugee Health Programme’s research
and development actors to provide a single strategic, framework. It was implemented within the scope of the
multisectoral and resilience-based response. Supported Improved access to health services for Syrian refugees
by several donors, WHO’s activities are complementary in Turkey project with funding from the EU Regional
to the Ministry of Health-implemented SIHHAT Trust Fund in Response to the Syrian Crisis.v
Acknowledgements
The WHO Health Emergencies team in Turkey would Country Office in Turkey and to Oguzhan Akyildirim,
like to thank all stakeholders who contributed to the Pinar Sağlik and Alev Yucel of TANDANS Data
implementation of this study. Special thanks go to Science Consulting for their valuable contributions to
Kanuni Keklik and Özlem Kahraman Tunay of the designing, data collection, data analysis and the overall
Migration Health Department, Ministry of Health of implementation of the study.
the Republic of Turkey, and to Mr Inanc Sogut and
Prof. Meliksah Ertem of the SIHHAT project, Ministry
of Health of the Republic of Turkey. Thanks also go to Authors
Omur Cinar Elci, Melda Keçik, Çetin Doğan Dikmen, Pelin The principal authors of this report are Hanna Radysh
Cebeci, Elif Göksu, Nurtaç Kavukcu, Kadriye Küçükbalci, and Monica Zikusooka, WHO Country Office in Turkey,
Mustafa Bahadir Sucakli and Altin Malaj of the WHO WHO Regional Office for Europe.
This document was produced with the financial assistance of the European Union.
The views expressed herein can in no way be taken to reflect the official opinion of the
European Union.
Abbreviations
3RP Regional Refugee and Resilience Plan
AOR adjusted odds ratio
CAHPS Consumer Assessment of Healthcare Providers
and Systems
CI confidence interval
EU European Union
MHC migrant health centre
MHTC migrant health training centre
NHS National Health Service (United Kingdom)
OR odds ratio
SDGs Sustainable Development Goals
SIHHAT Improving the health status of the Syrian
population under temporary protection and related
services provided by Turkish authorities (project)
UHC universal health coveragevi
Executive summary
Universal health coverage (UHC) is a global priority and When asked about the overall level of satisfaction with
the basis for achieving other health-related Sustainable the health services that they had received at the MHC,
Development Goals (SDGs) (1). At the core of several 78.2% of all respondents said they were satisfied:
international commitments, including the United 80.1% of men and 77.2% of women. Compared with
Nations Global Compact on Refugees (2) and the Global the other age groups, significantly more respondents
Compact for Safe, Orderly and Regular Migration (3), aged 60 years and over were satisfied with the health
is UHC, which was endorsed by the Sixty-first World services that they had received at the MHC (P < 0.001).
Health Assembly in resolution WHA61.17 on the health Higher proportions of respondents with no education
of migrants in 2008 (4). In line with these international and those who had arrived in Turkey in or before 2013
commitments, Turkey has taken steps to ensure access were satisfied compared with the other subgroups.
to health for its estimated 3.6 million Syrian refugees. Respondents had the highest level of satisfaction
with psychological or social assistance services
UHC should be embedded in a strong primary health- (84.8%), whereas lowest levels of satisfaction were for
care system offering people-centred health services. For emergency services (17.6%) and dental services (8.3%).
the Syrian refugee population in Turkey, this is pursued However, most respondents (89.4%) were unaware of
through a network of migrant health centres (MHCs) the existence of any feedback or complaint mechanism.
that provide cultural and linguistically sensitive services.
This study was undertaken to assess patient experience Although both gender and age had a significant
and satisfaction with services provided in MHCs, to effect on patient satisfaction, when other factors
identify the determinants of patient satisfaction and were considered none of the patient characteristics
potential areas to improve patient satisfaction or had a significant influence on patient satisfaction. All
dimensions of the patient experience. communication and quality of service-related variables
were significant predictors of patient satisfaction when
A patient survey was conducted between November all the other factors were controlled for. However,
2019 and March 2020. Data was collected through face- the type of MHC was not a significant predictor of
to-face interviews using a quantitative questionnaire patient satisfaction. The strongest service-related
developed by WHO in the Yemen emergency response. predictors of satisfaction were having sufficient length
The tool was adopted for this study because of its of consultation (adjusted odds ratios (AOR): 2.37; 95%
suitability to the context of the health humanitarian confidence interval (CI): 1.76–3.21; P < 0.000), receiving
response in Turkey. Prior to implementation, the a comprehensive examination (AOR: 2.01; 95% CI:
tool was adapted to the Syrian Arabic dialect and 1.49–2.70; P < 0.000) and being treated with respect
pre-tested. In all, 4548 patients and caregivers who by the nurse (AOR: 2.08; 95% CI: 1.52–2.85; P < 0.000).
received services from MHCs, extended MHCs and Receiving an explanation of the medical condition
migrant health training centres (MHTCs) in 16 provinces from the doctor was the strongest predictor of patient
participated in the study satisfaction among communication-related variables
(AOR: 1.98; 95% CI: 1.48–2.53; P < 0.000).
More than 70% of respondents had arrived in Turkey
after 2013, and 27.3% had arrived after 2016. Nearly Although most patients were satisfied with services in
two thirds (64.5%) of respondents were women. Most MHCs, improvements in physician–patient interactions
respondents (81.5%) were aged under 45 years, and and communication are recommended to empower
almost a quarter of the respondents (23.7%) were patients to participate in managing their treatment and
illiterate. Most respondents had visited the MHC at least overall health. In particular, physicians should inform
twice in the previous three months, and the majority had patients about medicine side-effects and danger signs
visited the MHC for a general consultation and consultation times should be increased, perhaps by
reducing the patient-to-physician ratio. Reducing waitingvii
times could also improve patient satisfaction. This
study provides evidence that greater promotion of MHC
services among refugee communities could increase
their utilization and reduce the burden on secondary
care facilities.
Recommendations are as follows.
• Improving patient experiences related to
consultation time, waiting time and quality of
physician–patient communication could improve
satisfaction with MHCs. In addition, examining
and addressing the causes of dissatisfaction for
services that had a lower level of satisfaction would
help to improve patient satisfaction.
• Implement a targeted campaign to increase the
use of MHC services, especially as the Ministry of
Health plans to expand the MHC network. The high
level of patient satisfaction established in this study
could be useful for the campaign.
• With increased service utilization in MHCs, an
objective estimation of the patient-to-physician ratio
based on patient records is needed to determine
physician workload and its potential impact on the
quality of services and patient satisfaction.
• Support physicians in MHCs to improve their
communication skills. Specific emphasis on
communicating with patients about medicines
would cover the observed gap in patient satisfaction
while improving the rational use of medicines.
• MHCs should consider implementing and
promoting a variety of feedback and complaint
mechanisms that can be safely accessed and
used by a diverse population to gather feedback to
improve services. These may include, but are not
limited to, complaint boxes and toll-free telephones.© WHO
Patient satisfaction and experience at migrant health centres in Turkey 1 Introduction UHC is a global priority and the basis for achieving other health-related SDGs (1). Under UHC, all people have access to health services when they need them, wherever they are and without financial hardship. UHC provision for refugees and migrants is the subject of several international commitments on human rights, including the United Nations Global Compact on Refugees (2) and the Global Compact for Safe, Orderly and Regular Migration (3), and was endorsed by the Sixty-first World Health Assembly in resolution WHA61.17 on the health of migrants in 2008 (4). Turkey currently hosts an estimated 3.6 million Syrians, of whom 23% are women of reproductive age and 14% are children aged 0–4 years (5). Law No. 6458 on Foreigners and International Protection provides emergency and temporary protection under Article 91 for foreigners in Turkey who have been forced to leave their country and cannot return (6). Syrian refugees in Turkey are classified as Syrians under temporary protection. In line with these international commitments, the country has taken steps to ensure access to health for its large refugee population. Globally, refugees and migrants often face challenges in accessing health care, including language and cultural differences (7–9), low health literacy (7,10), difficulties in understanding the health system (8), legal status, lack of awareness of their health rights (11) and financial limitations (7). The Government of Turkey has sought to address such challenges by expanding the capacity of its health system and developing legislation to ensure access to health care for refugees. According to WHO, UHC should be embedded in a strong primary health-care system offering people-centred health services that “consciously adopts the perspectives of individuals, families and communities, and sees them as participants as well as beneficiaries of trusted health systems that respond to their needs and preferences in humane and holistic ways” (9). People-centred health services focus on individuals rather than diseases, coordinate care around people’s needs while respecting their preferences, and enable people to participate in managing their own health affairs. Further, providing integrated people-centred services is critical to achieving UHC goals, especially for disadvantaged populations. Assessments of patient experience and satisfaction with health services provide insight into the patient-centredness of services. Background Refugee access to health care in Turkey In 2015 the Government of Turkey adopted a regulation to allow Syrians registered as under temporary protection access to free emergency medical treatment and to preventive and primary health services (10). In addition to the existing primary health facilities, a network of MHCs was later introduced to provide culturally sensitive health services in their own language. The Government’s response to refugee health needs is complemented by interventions supported through the SIHHAT project, with the main objective to increase national health system capacity to provide high-quality, free-of-charge health services to Syrians under temporary protection in Turkey (10). The SIHHAT project is implemented in 29 provinces with a high population density of Syrian refugees. As of August 2020, SIHHAT had 175 MHCs that have provided 13 million primary health-care consultations (10). The health services provided through MHCs in Turkey are free of charge for registered Syrians and are expected to meet national equity standards. Overall, a response to the needs of Syrians under temporary protection in Turkey is annually articulated in the Regional Refugee and Resilience Plan (3RP) with the health sector focusing on building resilience of the health system (12). In contributing to the 3RP objectives, WHO is implementing a refugee health programme with activities that include capacity-building for Syrian health workers, provision of quality people-centred health services for refugees, support for mental and psychosocial needs, and coordination of the Health Working Group.
2 Patient satisfaction and experience at migrant health centres in Turkey MHC mechanism Primary health care is the basis to achieving UHC and the SDGs (13). In Turkey, primary health care is provided through community health centres and family health centres. As part of the community health centre network, the Government of Turkey established MHCs under the SIHHAT project to meet the health needs of the Syrian population in Turkey. The MHC mechanism was planned and implemented based on the organization of primary health services in Turkey; the first MHCs were established in August 2015. The mechanism includes MHCs (or standard MHCs), extended MHCs and MHTCs. MHCs comprise several refugee health units, with each consisting of a physician and nurse pair. Extended MHCs provide additional services, including internal medicine, paediatric, obstetrics and gynaecology, oral and dental health, psychosocial support, and simple imaging and laboratory services. There are also seven MHTCs that, in addition to providing all of the services of extended MHCs, have training facilities for health workers and are jointly managed by the Ministry of Health and WHO. MHCs mainly provide services to Syrian refugees but, like all health-care facilities in Turkey, provide communicable disease prevention services (such as vaccination) and emergency health services to all people in need, regardless of nationality and registration status. Most health service providers in MHCs are Syrian nationals. Before being employed in MHCs, they are trained and oriented to work in the Turkish health-care system through a tailored adaptation training programme implemented by WHO in collaboration with the Ministry of Health. The adaptation training is delivered in MHTCs located in seven provinces: Ankara, Gaziantep, Hatay, Istanbul, Izmir, Mersin and Şanlıurfa. Through this action, the Ministry of Health and WHO aim to fill a human resources gap in the delivery of primary health services to Syrian refugees in order to increase access to quality and equitable health care for all. Up to March 2020, WHO and the Ministry of Health had trained 638 physicians, 806 nurses, 927 translators and 337 auxiliary staff who were currently providing services in 178 MHCs located in 29 provinces, and over 1 270 000 Syrian refugees had received health services in MHCs. Patient experience and satisfaction Understanding patient experience and satisfaction with health services is important for monitoring and improving the quality of care. Assessments of patient satisfaction also give patients the opportunity to participate in tailoring health-care provision to their needs, which is a core principle of people-centred health services. Although definitions/ concepts of patient satisfaction vary, examining patients’ views on health care and which attributes they value most can provide insights to improve the quality of care and inform strategic decision-making (14,15). In addition, satisfied patients are more likely to adhere to treatment plans, which increases the chance of good health outcomes, and to have fewer diagnostic tests and referrals, which increases the efficiency of care (14,16). Satisfied patients are also likely to return or recommend the services they have received to others, thereby helping to improve service utilization (17). Studies on people-centred care and patient satisfaction have produced a wide body of evidence and analytical tools (18–22). For refugees, migrants and asylum seekers, high levels of patient satisfaction were found when health services were provided in specialized units or delivered with language and cultural sensitivity (18–21). Assessments have shown that multiple factors related to the health worker influence patient satisfaction, including technical expertise, interpersonal care (e.g. communication), physical environment, access (i.e. accessibility, availability and cost), organizational characteristics, continuity of care, treatment outcome, and length of consultation with the doctor (14,22). In addition, patient characteristics such as age, gender, education, socioeconomic status, marital status, race, religion, geographical characteristics, frequency of visits, length of stay in Turkey, health status, personality and expectations were also found to influence patient satisfaction, but with inconsistent strength and direction of effect (22). Although patient satisfaction is a common outcome measure in health care assessments, it may be influenced by patients’ expectations as much as by the quality of the care provided. That is, the match between patient expectations and what care is provided also influences patient satisfaction (18–25). Within the humanitarian context, assessing the satisfaction of patients who receive services from MHCs is critical for accountability to the people most affected by the Syrian conflict. Accountability demands that actions to help people in need are driven by the needs, desires and capacities of the people affected and implemented in a respectful way. In this regard, the humanitarian sector has committed to giving affected populations the opportunity to provide feedback on the goods and services they have received through humanitarian actions (25,26).
Patient satisfaction and experience at migrant health centres in Turkey 3
A SIHHAT baseline survey on health needs of Syrian refugees in Turkey assessed their utilization and satisfaction
with health services. Of the 869 respondents, 88% had accessed services from state/university hospitals, whereas
only 29.5% had accessed services from MHCs. In all, 72% of those who had received services from hospitals were
satisfied, compared with 65% of those who had attended MHCs. The main reasons given for satisfaction were
the availability of medicine, quality of treatment and quality of nursing; in contrast, the main reasons given for
dissatisfaction were lack of good treatment and difficulty in communicating owing to a lack of interpreters. Although
this information is important for improving access, utilization and satisfaction with health services for Syrian
refugees, it may have limited applicability to MHCs because of the small proportion of respondents who had used
MHC services. However, the study provides a benchmark for monitoring improvements in MHCs. The present patient
satisfaction survey included a larger patient sample and collected data in MHCs to ensure that respondents had
recent experience of receiving MHC services.
Study aims and objectives
Understanding the level of patient satisfaction in MHCs is useful to ensure a people-centred approach to health
service delivery. Although MHCs have been operational since 2015, evidence is lacking on patient experience and
satisfaction with services from a representative sample of users. This study was undertaken to collect evidence
and beneficiary feedback on services received and their expectations to improve the humanitarian response. The
objectives were to:
• assess patient experience and satisfaction level with services provided in MHCs in Turkey;
• identify the determinants of patient satisfaction; and
• identify potential areas to improve the quality of care in terms of patient satisfaction or dimensions of the patient
experience.
Methodology
A patient survey was conducted between November 2019 and March 2020. Participants were patients and caregivers
who received services from MHCs, extended MHCs and MHTCs in 16 provinces (Table 1).
Study design and population
This cross-sectional survey targeted patients attending MHCs with more than 10 refugee health units in 16 Turkish
provinces. Provinces with the highest number of patient consultations were selected to enable representative
sampling of patients receiving services from MHCs. A proportional stratified sampling approach was followed to
estimate the required sample size based on the number of total patient consultations in each province from 2015
until March 2019. The sample size was estimated using WinPepi (version 11.65) with a 95% CI, 0.05 error margin and
20% loss to follow-up. The final sample size was estimated at 4460 individuals, which was distributed proportionally
between the 16 provinces and three types of MHC. Table 1 shows the sample distribution by province and type of
MHC.4 Patient satisfaction and experience at migrant health centres in Turkey
Table 1. Sample distribution by province and type of MHC
Province Sample estimation Final study
population
Refugee health units (n) Patients interviewed (n)
MHCs E-MHCs MHTCs MHCs E-MHCs MHTCs
Adana 5 7 0 150 210 0 353
Ankara 1 2 1 65 130 65 202
Bursa 4 3 0 120 90 0 224
Gaziantep 3 2 1 150 100 50 451
Hatay 6 4 1 450 300 75 759
Istanbul 7 8 1 210 240 30 566
Izmir 2 1 1 116 58 58 197
Kahramanmaraş 4 5 0 120 150 0 317
Kayseri 2 2 0 60 60 0 100
Kilis 1 9 0 30 270 0 207
Konya 2 3 0 60 90 0 169
Malatya 1 1 0 30 30 0 81
Mardin 1 0 0 37 0 0 90
Mersin 3 2 1 93 62 31 224
Osmaniye 1 4 0 30 120 0 140
Şanlıurfa 4 4 1 232 230 58 468
Total sample 47 57 7 1953 2140 367 4548
4460
E-MHC: extended MHC.
Participants were recruited to the study if they were adult patients (aged > 18 years) or an immediate caregiver of a
patient (child, spouse, elderly) receiving health services from the MHC on the day of the survey.
Participants were recruited in MHC reception areas on normal working days at an interval calculated from the average
daily patient load of the facility. Interviewers identified potential participants, gave them detailed information about the
study and confirmed that they met the inclusion criteria before inviting them to participate. Those who agreed were
interviewed in areas that ensured privacy for the respondent. Of the 4665 people who met the recruitment criteria and
were asked for interview, 117 refused; therefore, 4548 participants were included in the study.Patient satisfaction and experience at migrant health centres in Turkey 5
Data collection
Data was collected through face-to-face interviews using a quantitative questionnaire (Annex 1). Tools used in
previous studies to assess patient satisfaction in different contexts include the National Health Service (NHS) Patient
Reported Outcome Measures (27) and the National Institute for Health and Care Excellence quality standard on
patient experience in adult NHS services (28) (United Kingdom); the Picker Patient Experience Questionnaire (29)
and the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Outpatient and Ambulatory Surgery
Survey (30) and CAHPS Hospital Survey (31) (Agency for Healthcare Research and Quality) and a patient satisfaction
tool used by WHO in the Yemen emergency (unpublished). The latter was used for this study because of its suitability
to the context: it was designed and applied in a humanitarian setting. The questionnaire also addressed the need for
accountability to the affected population. It included questions on the accessibility of health-care facilities (including
distance from home, physical barriers, waiting time and out-of-pocket costs), overall satisfaction with the health
service and the health worker–patient relationship. The questionnaire was pre-tested in a MHC in Altındağ, Ankara to
ensure clarity of meaning of translated questions, questionnaire flow, content and language suitability. Following this,
minor language adaptations were made to suit the Syrian Arabic dialect.
Prior to commencing data collection, interviewers received training from WHO, the Ministry of Health and Tandans
Data Science Consulting.1 Data was collected in Arabic; all interviewers spoke Arabic as a first language. Interviewers
used an electronic version of the questionnaire in KoBoToolbox (32) to collect data from interviews conducted in
December 2019 and January 2020.
Study variables
Based on a literature review and the context of Syrian refugees in Turkey, study variables were identified and
categorized into four clusters:
• patient characteristics: age, gender, education and year of arrival in Turkey;
• accessibility of health services: taken as time taken to reach the MHC;
• communication: health worker explains medical tests, doctor explains medical condition, health worker explains
the danger signs; and
• quality of service: health worker spends enough time with the patient, health worker carries out a comprehensive
examination, health worker treats me with respect, waiting time and type of MHC.
Data cleaning and analysis
Data cleaning was done to identify and resolve inconsistencies and ensure completeness. A total of 15 incomplete
records were removed because answers were missing for more than 60% of the questions, especially those related
to satisfaction statements. Records with entry errors that could be corrected based on other entries were corrected,
whereas those with errors that could not be corrected were removed. Further, responses to multiple choice questions
that had the “other” option were recoded into new categories during the analysis.
Information on variables in the communication and service clusters was collected on a five-point scale (strongly
disagree, disagree, neither agree nor disagree, agree, strongly agree) and re-categorized into two for analysis: the
first three responses were categorized as “disagree” and the last two as “agree”. Patient responses for the statement
“Overall, the health services I have been receiving are satisfactory” were also collected on a five-point scale (shown
above) and re-categorized as two (disagree—unsatisfied) and (agree–satisfied) for analysis.
Descriptive analyses were conducted to describe the distribution of sociodemographic characteristics and other study
variables. Patient experiences and satisfaction were analysed both overall and for the different facility types. Logistic
1 An independent consultancy based in Ankara.6 Patient satisfaction and experience at migrant health centres in Turkey regression was conducted to identify factors that influenced patient satisfaction. To fit the logistic regression models, variables with a significant influence on patient satisfaction (P < 0.05) were included, and AORs were calculated with 95% CIs. In the first model fitted, only patient characteristics (age, gender, education, year of arrival in Turkey) were adjusted, whereas in the second model all variables were adjusted by including them in the model. Data analysis was performed using IBM SPSS Statistics version 25.
Patient satisfaction and experience at migrant health centres in Turkey 7 Results Sociodemographic characteristics of participants More than 70% of participants had arrived in Turkey after 2013, and 27.3% had arrived after 2016 (Table 2). The average household size was 5.9 people. Nearly two thirds (64.5%) of respondents were women. Most participants (81.5%) were aged under 45 years. Almost a quarter of the respondents (23.7%) were illiterate (not able to read and write) and nearly half (48.4%) had completed primary education only. Table 2. Sociodemographic characteristics of respondents Characteristic Number (n) Percentage (%) Gender (n = 4533) Men 1608 35.5 Women 2925 64.5 Age, years (n = 4533) 18–29 1794 39.6 30–44 1900 41.9 45–59 677 14.9 60 and above 162 3.6 Education level (n = 4505) No education 1069 23.7 Completed primary education 2180 48.4 Completed secondary education 762 16.9 University degree/equivalent or higher 494 11.0 Employment status (n = 4522) Working 1080 23.9 Not working 3442 76.1 Year of migration (n = 4528) ≤ 2013 1205 26.6 2014 1057 23.3 2015 1028 22.7 ≥ 2016 1238 27.3 Overall, about a quarter of respondents (23.9%) were currently employed, but the proportion was higher for men than for women (52.3% vs 8.2%). Regarding employment sectors, half of employed respondents (50.5%) were working in sales and services, 13.8% in agriculture and 12.4% in teaching. Most male respondents were employed in the sales and services sector (57.6%), and similar proportions of female respondents were working in the teaching (28.7%), sales and services (25.4%), and agricultural (23.8%) sectors.
8 Patient satisfaction and experience at migrant health centres in Turkey
Access and utilization of services in MHCs
Most respondents had visited the MHC without obtaining any information about the services available in MHCs.
Only 6.2% had been referred to the MHC; of theses, most (61.8%) had been referred from another MHC (Table 3). The
Turkish Red Crescent was another important source of information about MHCs.
Table 3. Access to health facilities
Dimension Standard MHC Extended MHC MHTC Total
n % n % n % n %
Did you have information about this health
facility before you visited?
Yes 114 5.6 130 7.7 39 5.3 283 6.3
No 1931 94.4 1566 92.3 699 94.7 4196 93.7
If so, where did you get the information from?
Another MHC 61 53.5 97 74.6 17 43.6 175 61.8
Turkish Red Crescent 15 13.2 19 14.6 7 17.9 41 14.5
Other outreach team 8 7.0 3 2.3 7 17.9 18 6.4
Other _____ 30 26.3 11 8.5 8 20.5 49 17.3
In the last 3 months, how many times have
you/the patient visited this health facility?
1 430 20.8 300 17.6 141 18.6 871 19.2
2 613 29.7 571 33.4 303 39.9 1487 32.8
3 473 22.9 406 23.8 159 20.9 1038 22.9
>3 549 26.6 431 25.2 157 20.7 1137 25.1
How did you get to the facility today?
Walked 1316 63.8 942 55.2 342 45.0 2600 57.4
Private transport or taxi 301 14.6 304 17.8 151 19.9 756 16.7
Public transport 408 19.8 400 23.4 256 33.7 1064 23.5
Other means 39 1.9 62 3.6 11 1.4 112 2.5
How long did it take you to get here today from
your home?
0–15 minutes 1290 62.5 1001 58.7 365 48.1 2656 58.7
16–30 minutes 605 29.3 556 32.6 301 39.7 1462 32.3
31–45 minutes 89 4.3 78 4.6 50 6.6 217 4.8
> 45 minutes 80 3.9 69 4.0 43 5.7 192 4.2
How much did it cost you/the patient to get
here today (one way)?
< 5 TL 308 52.0 320 55.7 221 60.7 849 55.5
5–10 TL 154 26.0 137 23.8 72 19.8 363 23.7
≥ 10 TL 130 22.0 118 20.5 71 19.5 319 20.8
Once you arrived at the health facility, how long
did you wait to be seen by a health worker?
< 20 minutes 1366 66.3 978 57.3 428 56.3 2772 61.2
21–60 minutes 519 25.2 564 33.1 277 36.4 1360 30.0
61–90 minutes 40 1.9 45 2.6 24 3.2 109 2.4
> 90 minutes 136 6.6 119 7.0 31 4.1 286 6.3Patient satisfaction and experience at migrant health centres in Turkey 9
Most respondents had visited the MHC at least twice in the previous three months. Respondents aged 45–59 years
had visited the MHC slightly more frequently than other age groups. More than half had walked to the MHC on the
day of the interview (57.4%; Table 3). Of those who had used some other means of transport, most (55.5%) had paid
transportation costs of less than 5 Turkish lira. Irrespective of the means of transport, the average time taken to reach
the MHC was 19.3 minutes.
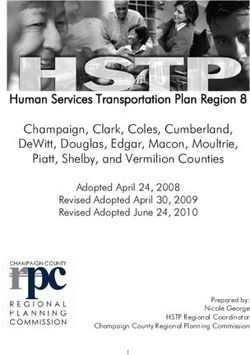
Almost one fifth of the respondents had visited the MHC to consult a specialist physician (19.2%). About two thirds
of respondents (63.7%) had attended the MHC for one service, 29.3% had attended for two services and 6.9% for
more than two services (Table 4). Most respondents had visited the MHC for a general consultation, followed by
investigation – diagnostic tests, vaccination, and pregnancy-related (pregnancy or prenatal care) and infant-care
services (Fig. 1).
Fig. 1. Overall service utilization in MHCs
General consulta�on
Inves�ga�on – diagnos�c tests
Vaccina�on
Pregnancy-related consulta�on
Infant care
Family planning
Emergency care
Medical cer�ficate
Dental care
Psychological/social assistance
Wound care
Other
0 500 1000 1500 2000 2500 3000 3500
Respondents
Table 4. Service utilization by type of MHC
Reason/s for this visit Standard MHC Extended MHC MHTC
n % n % n %
Pregnancy-related consultation 64 3.1 122 7.1 46 6.1
Infant consultation (postnatal care) 70 3.4 51 3.0 51 6.7
Vaccination 447 21.6 294 17.2 178 23.4
General consultation 1409 68.2 1183 69.3 480 63.2
Dental care 22 1.1 21 1.2 5 0.7
Family planning 54 2.6 50 2.9 41 5.4
Investigation – diagnostic tests 713 34.5 680 39.8 290 38.2
Emergency 46 2.2 64 3.7 25 3.3
Wound care 17 0.8 7 0.4 2 0.3
Psychological or social assistance 8 0.4 20 1.2 6 0.8
Medical certificate 32 1.5 47 2.8 11 1.4
Other 0 0.0 2 0.1 0 0.0
Total 2882 100 2541 100 1135 10010 Patient satisfaction and experience at migrant health centres in Turkey
Slightly more than half of the respondents (56.3%) had visited the MHC to obtain health services for themselves,
34.2% to obtain health services for their children and 8.0% to obtain health services for their spouse.
More than half (54.1%) of the respondents had attended the MHC within a day of needing health care (Fig. 2). Among
those who delayed seeking health care by one day or more, the main reason was that they thought that they (or the
patient) was not sick enough and would get better on their own (67.1%; Fig. 3).
Fig. 2. Time to seek care
60
50
40
Percentage (%)
30
20
10
0
30
Time (days)
Fig.
Fig 33. Reasons for delayed care seeking
Didn’t think I was sick enough or thought the problem
would getter better on its own
Other
Appointment
Didn’t think the health facility would be able to help
due to lack of doctors, medicines or supplies
Worried about the safety of travelling to care
Worried about the cost of care
0 10 20 30 40 50 60 70 80
Percentage (%)
Patient
Fig 4
experience at MHCs
Participants were asked about their experiences at the health facility regarding services received and waiting time;
interaction with physicians and nurses, receiving medication, their willingness to recommend services and intention to
The doctor told me about danger signals related to my
return. Annex 2 presentsdiagnosisthe responses
to look by type of health facility.
out for at home
When I come to the MHC, I don’t have to wait long to see
a doctor
The doctor explains the reason for medical tests
Services received and waiting time
I trust the nurse’s skills at the MHC
On the day of the survey, 88.5% of respondents thought that they had fully received the health service that they needed
I trust the doctor’s skills at the MHC
at the MHC, and very few thought that they had partially received (6.9%) or not received (4.5%) the health service that
they needed.
The doctor Thetoaverage
is careful waiting
check everything when time to be seen by a health worker was 29.9 minutes (Table 3). Most respondents
examining
me
felt that they had not had to wait long to see the doctor (71.5%), but almost 20% disagreed (Fig. 4).
The doctor spends enough time with me to explain my
medical condition
The doctor spends enough time with me to answer all my
questions
I understand the diagnosis from doctors at MHCs
The nurse treats me with respect
The doctor treats me with respect
0 10 20 30 40 50 60 70 80 90 100Patient satisfaction and experience at migrant health centres in Turkey 11
© SIHHATFig 3
Didn’t think I was sick enough or thought the problem
12 would getter better on its own Patient satisfaction and experience at migrant health centres in Turkey
Other
Appointment
Didn’t think the health facility would be able to help
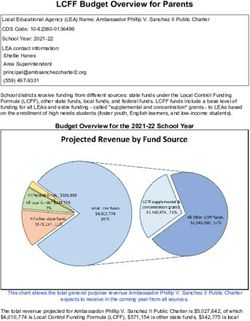
Physician–patient interaction and communication
due to lack of doctors, medicines or supplies
Over 80% of about
Worried the respondents said
the safety of travelling that the doctors and nurses had treated them with respect (Fig. 4). A similar
to care
proportion (80.0%) thought that the doctor had taken care to examined them fully and taken enough time to explain
Worried about the cost of care
the medical condition and answer their questions. Nevertheless, almost 20% were not sure or disagreed that the
doctor had comprehensively examined 0
them
10
or spent
20 30
enough
40 50
time70with
60 80
them. In all, 10% of respondents thought the
doctor had not spent long enough examining them or explaining
Percentage (%) their medical condition. Slightly over 50% had been
told about danger signs to look out for at home.
Fig.
Fig 4 4. Patient experience in MHCs
The doctor told me about danger signals related to my
diagnosis to look out for at home
When I come to the MHC, I don’t have to wait long to see
a doctor
The doctor explains the reason for medical tests
I trust the nurse’s skills at the MHC
I trust the doctor’s skills at the MHC
The doctor is careful to check everything when examining
me
The doctor spends enough time with me to explain my
medical condition
The doctor spends enough time with me to answer all my
questions
I understand the diagnosis from doctors at MHCs
The nurse treats me with respect
The doctor treats me with respect
0 10 20 30 40 50 60 70 80 90 100
Percentage (%)
Agree Neutral Disagree
Medicines
Most respondents had been prescribed medicine on the day of the survey (87.0%) and 81% considered that the doctor
had explained the medication use either fully or partially. Most said that they understood the purpose of the treatment
and the prescribed medicines (79.5%; Fig. 5). In all, 79.4% said that they understood how to use the medicines that
they had been prescribed that day; however, 12% did not understand how to use the medicines and 8.6% were not
sure. Less than 50% of the respondents said that they had been informed about medication side-effects.
Fig.
Fig 5 5. Use of medicines
I was informed about medication side-effects
I understand how to use the medicines that
were prescribed to me today
I understand the purpose of the treatment and
prescribed medicines
0 10 20 30 40 50 60 70 80 90 100
Percentage (%)
Agree Neutral Disagree
Willingness to recommend services and intention to return
Based on their experience at the MHC, 86.1% of respondents said that they would return to the facility if they needed
Fig 6
another health service, and 83.7% said that they would recommend the health facility to other people (Fig. 6). Only
11.6% of respondents said that they would go to a private practice for further consultation after visiting the MHC.
Based on my experience here, I will return to
this health facility for a service in the future
if needed
Based on my experience here, I will
recommend this health facility to other
people0 10 20 30 40 50 60 70 80 90 100
Percentage (%)
Agree Neutral Disagree
Patient satisfaction and experience at migrant health centres in Turkey 13
Fig.
Fig 6 6. Intention to return and recommendation
Based on my experience here, I will return to
this health facility for a service in the future
if needed
Based on my experience here, I will
recommend this health facility to other
people
0 20 40 60 80 100
Percentage (%)
Agree Neutral Disagree
Patient satisfaction
When asked about their overall level of satisfaction with the health services that they had received at the MHC, 78.2%
of all respondents said that they were satisfied: 80.1% of men and 77.2% of women (Table 5). Compared with the
other age groups, significantly more respondents aged 60 years and over were satisfied with the health services that
they had received at the MHC (P < 0.001). Higher proportions of respondents with no education and those who had
arrived in Turkey in or before 2013 were satisfied compared with the other subgroups.
Table 5. Patient satisfaction with the MHC services, by demographic characteristic
Characteristic Satisfieda Neutral Dissatisfieda P valueb
n % n % n %
Gender
Men 1286 80.1 240 14.9 80 5.0 0.017
Women 2257 77.2 533 18.2 132 4.5
Age, years
18–29 1369 76.4 337 18.8 86 4.8 0.002
30–44 1475 77.7 334 17.6 89 4.7
45–59 557 82.4 87 12.9 32 4.7
≥ 60 142 87.7 15 9.3 5 3.1
Education level
No education 888 83.1 144 13.5 37 3.5 < 0.001
Completed primary 1697 78.0 382 17.5 98 4.5
Completed secondary 583 76.6 129 17.0 49 6.4
University degree/equivalent or higher 359 72.8 108 21.9 26 5.3
Year of arrival in Turkey
≤ 2013 976 81.0 179 14.9 50 4.1 0.004
2014 831 78.8 176 16.7 47 4.5
2015 766 74.5 195 19.0 67 6.5
≥ 2016 967 78.2 221 17.9 48 3.9
Employment status
Employed 827 76.7 188 17.4 63 5.8 0.092
Unemployed 2710 78.8 581 16.9 148 4.3
a
Satisfied: agreed with the questionnaire statement; dissatisfied: disagreed with the questionnaire statement.
b
Pearson’s chi-squared test.14 Patient satisfaction and experience at migrant health centres in Turkey
© SIHHATPatient satisfaction and experience at migrant health centres in Turkey 15
Overall satisfaction by type of MHC
Although over 70% of all respondents were satisfied with the health services they had received, some variations were
noted between the type of MHC (Fig. 7). A significantly higher proportion of respondents was satisfied with standard
MHCs (80.0%) than with extended MHCs (79.6%) and MHTCs (70.4%; P < 0.001).2
Fig. 7. Overall satisfaction from the services received by type of facility
MHTC
Extended MHC
Standard MHC
0 10 20 30 40 50 60 70 80 90 100
Percentage (%)
Agree (satisfied) Neutral Disagree (dissatisfied)
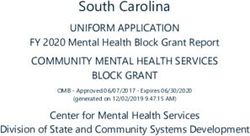
Overall satisfaction by type of health service
The overall level of satisfaction with services received at MHCs was then stratified by type of health service (Fig. 8).
Respondents had the highest level of satisfaction with psychological or social assistance services (84.8%), followed
by medical certificate services (82.2%) and wound care (80.8%). The lowest levels of satisfaction were for emergency
services (17.6%) and dental services (8.3%), followed by reproductive health and child-care services (6.4%)
Fig. 8. Overall satisfaction by type of services received
Psychological/social assistance
Medical certifi cate
Wound care
General consul tation for feeling si ck
Investigation – diagnostic tests
Vaccination
Reproductive healt h and child care
Dental care
Emergency care
0 10 20 30 40 50 60 70 80 90 100
Percentage (%)
Agree (satisfi ed) Neutral Disagree (dissatisfied)
2 Based on Pearson’s chi-squared test.16 Patient satisfaction and experience at migrant health centres in Turkey
Patient satisfaction feedback mechanism
Most respondents (89.4%) were unaware of the existence of any feedback or complaint mechanism (Fig. 9).
Fig. 9. Patient awareness of a feedback mechanism
100
90
80
70
Percentage (%)
60
50
40
30
20
10
0
Standard MHC Extended MHC MHTC Total
Pa�ents who are aware of the feedback mechanism
Pa�ents who are not aware of the feedback mechanism
Determinants of patient satisfaction and experience
Logistic regressions models were used to examine patient characteristics and factors related to MHC services
(accessibility, communication and service quality) that might influence patient satisfaction.
Patient characteristics
Both gender and age had a significant effect on patient satisfaction (Table 6). In simple logistic regression
comparisons, the following groups were more likely to be satisfied with the health services they had received at
MHCs: women, older people, people with lower education levels and people who had arrived in Turkey before 2013.
However, none of the patient characteristics were found to significantly influence patient satisfaction in the multiple
regression analysis (i.e. when other factors were added).
Table 6. Logistic regression analysis of patient characteristics that might influence patient satisfaction
Category OR 95% CI P value
Gender (Ref: women)
Men 0.85 0.73–0.98 0.027
Age, years (Ref: 18–29)
30–44 1.08 0.92–1.26 0.341
45–59 1.45 1.15–1.81 0.001
≥ 60 2.19 1.36–3.55 0.001
Education level (Ref: no education)
Completed primary 0.72 0.60–0.87 0.001
Completed secondary 0.67 0.53–0.84 0.001
University degree/equivalent or higher 0.55 0.42–0.71 0.000
Year of arrival in Turkey (Ref: ≤ 2013)
2014 0.87 0.71–1.08 0.202
2015 0.69 0.56–0.84 0.000
≥ 2016 0.84 0.69–1.03 0.091
OR: odds ratio.Patient satisfaction and experience at migrant health centres in Turkey 17 Accessibility Accessibility was measured as the time taken for patients to reach a health facility. Using this measure, the accessibility of health services was significantly associated with patient satisfaction. Respondents with longer journey times to reach the health facility were less satisfied (P < 0.05). However, when patient characteristics were controlled for in multiple logistic regression analysis, accessibility ceased to be a significant factor (Table 7). Communication Patient experiences in receiving health information were used to assess communication between the health worker and patient. Respondents who felt that medical tests, medical condition, medication side-effects and danger signs related to their health condition to look out for at home had been explained were more likely to be satisfied than those who did not (P < 0.0001). Respondents who had received explanations about their medical condition from the doctor were 8.9 times more likely to be satisfied than those who had not (odds ratio (OR): 8.93; 95% CI: 7.56–10.56; P < 0.000). All communication variables remained significant predictors of patient satisfaction when all the other factors were controlled for. Receiving an explanation of the medical condition from the doctor was the strongest predictor of patient satisfaction in this category (AOR: 1.98; 95% CI: 1.48–2.53; P < 0.000). Quality of service The influence of quality of service on patient satisfaction was assessed using the participants’ assessment of length of time spent with the health worker, adequacy of the examination, and level of perceived respect from doctors and nurses, along with the waiting time to see a health worker (from arrival at the facility) and type of MHC. Respondents who felt that they spent enough time with the health worker, received a comprehensive examination and thought that they were treated with respect by both doctors and nurses were more likely to be satisfied (P < 0.05). The length of waiting time was also a significant predictor of patient satisfaction (P < 0.000). Respondents who received services from extended MHCs and MHTCs were less likely to be satisfied than those who received services from standard MHCs. However, when patient characteristics and other factors were controlled for, the type of MHC was not a significant predictor of patient satisfaction. Multiple logistic regression in the fully adjusted model showed that all service-related variables except for type of MHC were significant predictors of patient satisfaction. The strongest predictors of satisfaction were having a sufficient consultation time (AOR: 2.37; 95% CI: 1.76–3.21; P < 0.000), receiving a comprehensive examination (AOR: 2.01; 95% CI: 1.49–2.70; P < 0.000) and being treated with respect by the nurse (AOR: 2.08; 95% CI: 1.52–2.85; P < 0.000).
You can also read