PERSPECTIVE Management Paradigms for Diabetic Macular Edema
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
PERSPECTIVE
Management Paradigms for Diabetic Macular Edema
PAUL MITCHELL AND TIEN YIN WONG, FOR THE DIABETIC MACULAR EDEMA TREATMENT GUIDELINE
WORKING GROUP
D
PURPOSE: To provide evidence-based recommenda- IABETES MELLITUS (DM) IS A GLOBAL EPIDEMIC
tions for diabetic macular edema (DME) management with significant morbidity.1 Although diabetic
based on updated information from publications on retinopathy (DR) affects 1 in 3 people with
DME treatment modalities. DM,1 the leading cause of vision loss in this population is
DESIGN: Perspective. diabetic macular edema (DME),2 which affects approxi-
METHODS: A literature search for ‘‘diabetic macular mately 6.8% of the diabetic population.3
edema’’ or ‘‘diabetic maculopathy’’ was performed using DME represents a spectrum of retinopathy signs charac-
the PubMed, Cochrane Library, and ClinicalTrials.gov terized by edema and thickening of the central macula and
databases to identify studies from January 1, 1985 to surrounding noncentral macula that are not explained by
July 31, 2013. Meta-analyses, systematic reviews, and the presence of an epiretinal membrane (ERM) at the mac-
randomized controlled trials with at least 1 year of ula. These symptoms are typically confirmed by slit-lamp
follow-up published in the past 5 years were preferred biomicroscopy and, increasingly, with the aid of optical
sources. coherence tomography (OCT).
RESULTS: Although laser photocoagulation has been the For nearly 30 years, focal/grid laser photocoagulation has
standard treatment for DME for nearly 3 decades, there is been the mainstay of treatment for clinically significant
increasing evidence that superior outcomes can be achieved DME (CSME).4 However, there have been substantial
with anti–vascular endothelial growth factor (anti-VEGF) advances in our understanding of DME since this method
therapy. Data providing the most robust evidence from large was first used. First, epidemiologic data indicate that
phase II and phase III clinical trials for ranibizumab demon- DME, more than DR severity, is the most common cause
strated visual improvement and favorable safety profile for of vision loss for patients.5 Second, there is now better
up to 3 years. Average best-corrected visual acuity change understanding that risk factors for DME (eg, serum lipids) may
from baseline ranged from 6.1-10.6 Early Treatment Dia- be different from those for DR, highlighting the importance
betic Retinopathy Study (ETDRS) letters for ranibizumab, of systemic management being targeted at DME.6,7 Third,
compared to 1.4-5.9 ETDRS letters with laser. The propor- improved knowledge of the pathophysiology of DME has
tion of patients gaining ‡10 or ‡15 letters with ranibizumab enabled the development of alternative therapies.1,8
was at least 2 times higher than that of patients treated with Fourth, the development of modern imaging techniques,
laser. Patients were also more likely to experience visual loss such as OCT, has allowed assessment of early DME,
with laser than with ranibizumab treatment. Ranibizumab including subclinical DME.9 Last, the results from several
was generally well tolerated in all studies. Studies for beva- large phase III randomized controlled trials (RCTs) for
cizumab, aflibercept, and pegaptanib in DME were limited alternative therapies, namely anti–vascular endothelial
but also in favor of anti-VEGF therapy over laser. growth factor (anti-VEGF) treatments, have now been
CONCLUSIONS: Anti-VEGF therapy is superior to laser reported.10–14
photocoagulation for treatment of moderate to severe The treatment algorithm for the selection of patients,
visual impairment caused by DME. (Am J the initiation of anti-VEGF therapy, and the assessment
Ophthalmol 2014;157:505–513. Ó 2014 by Elsevier and retreatment of DME using this group of therapies has
Inc. All rights reserved.) not yet been established. This Perspective article summa-
rizes major studies and RCTs examining DME treatment
modalities with the aim of providing an initial set of
Supplemental Material available at AJO.com.
Accepted for publication Nov 12, 2013.
evidence-based recommendations for DME management.
From the Centre for Vision Research, Westmead Millennium Institute,
University of Sydney, Sydney, Australia (P.M.); and Singapore Eye
Research Institute, Singapore National Eye Centre, National University
of Singapore, Singapore (T.Y.W.). METHODS
Inquiries to Professor Tien Yin Wong, Singapore Eye Research Institute,
Singapore National Eye Centre, National University of Singapore, 1E
Kent Ridge Road, NUHS Tower Block, Level 7, Singapore 119228; WE CONDUCTED A LITERATURE SEARCH USING THE
e-mail: ophwty@nus.edu.sg PubMed, Cochrane Library, and ClinicalTrials.gov
0002-9394/$36.00 Ó 2014 BY ELSEVIER INC. ALL RIGHTS RESERVED. 505
http://dx.doi.org/10.1016/j.ajo.2013.11.012databases with the terms ‘‘diabetes macular edema’’ or ‘‘dia- visual impairment, in addition to stabilizing and preventing
betic maculopathy’’ to identify studies published from future vision loss.5–13 Four VEGF-binding drugs are
January 1, 1985 to July 31, 2013. This was followed by a currently used for ophthalmic conditions: ranibizumab,
manual search of references cited in selected major papers. bevacizumab (off-label), aflibercept, and pegaptanib. Evi-
Meta-analyses, systematic reviews, and RCTs with at least dence for DME treatment with anti-VEGF therapies is
1 year of follow-up published in the past 5 years were largely based on data from phase II and phase III RCTs
preferred sources. Recommendations for DME treatment for ranibizumab, including Safety and Efficacy of Ranibizu-
were drafted by the Diabetic Macular Edema Treatment mab in Diabetic Macular Edema (RESOLVE):17 Two-year
Guideline Working Group and graded for importance of Outcomes of the Ranibizumab for Edema of the mAcula in
clinical outcome and strength of evidence.15 Diabetes (READ-2);18,19 A 12 Month Core Study to Assess
the Efficacy and Safety of Ranibizumab Intravitreal
Injections (RESTORE);10 Diabetic Retinopathy Clinical
Research Network (DRCR.net) Protocol I;11–13 and A
SYSTEMIC MANAGEMENT Study of Ranibizumab Injection in Subjects with CSDME
with Center Involvement Secondary to Diabetes Mellitus
OPTIMAL MANAGEMENT OF SYSTEMIC RISK FACTORS IS A
(RISE and RIDE).14,20
key component of the primary prevention of DR. Intensive
control of hyperglycemia, hypertension, and possibly Ranibizumab. RESOLVE was a phase II, double-masked,
hyperlipidemia delay the onset and progression of DR. sham-controlled RCT evaluating the efficacy and safety of
Whether the same is useful for DME is less clear, as there ranibizumab compared with sham treatment over
are fewer studies focused on DME alone. Because DME 12 months.17 Patients (n ¼ 151) with visual acuity (VA)
develops in a subset of patients with DR and the likelihood
20/40-20/160 and central retinal thickness (CRT)
of developing DME increases with DR severity, control of >
_300 mm were randomly assigned to ranibizumab 0.3 mg
systemic risk factors would be expected to have a major or 0.5 mg, or to sham injections. Dose doubling and
effect on DME. An overview of studies evaluating the rescue laser treatment were permitted according to
effects of improving blood glucose levels, blood pressure, predefined criteria. At the end of the study, a mean
and lipid profile is available online (Supplemental Refer- average change in best-corrected VA (BCVA) of þ7.8
ences, available at AJO.com). letters from baseline was observed in the ranibizumab
groups compared with -0.1 letters in the sham group (P <
.0001). Mean CRT reduction was parallel to mean
OCULAR MANAGEMENT BVCA improvement. More than 3 times the proportion
of patients who were treated with ranibizumab gained
LASER PHOTOCOAGULATION: The use of laser photoco- >
_10 and > _15 letters compared with those receiving sham
agulation has been the mainstay of treatment for CSME injections.
since the landmark Early Treatment Diabetic Retinopathy READ-2 was a phase II, multicenter, interventional
Study (ETDRS) in 1985.4 However, laser photocoagula- RCT comparing ranibizumab with focal laser treatment
tion mostly does not improve vision, and a significant pro- and a combination of both in DME among patients with
portion of patients experience progressive worsening of type 1 or 2 DM. Patients (n ¼ 126) with VA 20/40-20/
vision despite laser photocoagulation (Supplemental 320 and CRT > _250 mm were randomized to receive
Table 1, available at AJO.com). Furthermore, long-term 0.5 mg ranibizumab injections at baseline and at months
use of this treatment is limited by significant risks and 1, 3, and 5 (Group 1); laser treatment at baseline and
adverse effects, such as central and paracentral scotomata, then at month 3 as needed (Group 2); or ranibizumab
loss of color vision, progressive enlargement of laser scars injections and laser treatment at baseline and at month 3
(‘‘laser creep’’), and occasional secondary choroidal neovas- (Group 3).18 This was followed by a maintenance regimen
cularization.16 The subthreshold micropulse diode laser of 0.5 mg ranibizumab every 2 months and/or laser treat-
and the patterned scan laser are 2 innovations developed ment every 3 months for residual edema. Mean BVCA
to minimize scar formation. However, long-term experi- change from baseline to month 24 was þ7.7 letters for
ence is needed to define their precise roles in DME treat- Group 1, þ5.1 letters for Group 2, and þ6.8 letters for
ment. Group 3, although the mean differences were not signifi-
cantly different among all groups. Patients in Groups 2
ANTI–VASCULAR ENDOTHELIAL GROWTH FACTOR and 3 who received ranibizumab injections on top of laser
AGENTS: VEGF is a potent factor in the pathogenesis of treatment required less frequent injections without
DME that is upregulated in hypoxic and hyperglycemic compromising visual outcomes at 2 years than those who
states. Elevated VEGF levels in the intraocular fluid corre- received ranibizumab only in Group 1. More aggressive
late with vascular hyperpermeability and DME severity. treatment with ranibizumab from year 2 to year 3 demon-
Current evidence shows that anti-VEGF therapies reverse strated that mean BCVA could be further improved by
506 AMERICAN JOURNAL OF OPHTHALMOLOGY MARCH 20143.1 letters (P ¼ .009) in Group 1.19 Resolution of edema reduced risk of DR progression, and regression of DR was
was more frequent in Groups 2 and 3, in which laser treat- observed in eyes with DME.20
ment was included as part of the treatment regimen.
RESTORE was a double-masked, multicenter, laser- Bevacizumab. The Bevacizumab or Laser Therapy
controlled phase III study examining the efficacy of ranibi- (BOLT) study was a single-center, 2-year, phase II RCT
zumab 0.5 mg as monotherapy or combined with laser ther- comparing the effects of repeated intravitreal bevacizumab
apy over laser treatment alone.10 Patients (n ¼ 345) with (ivB) and laser therapy in 80 patients with persistent
visual impairment 20/32-20/160 were enrolled in the study. DME causing moderate visual impairment of > _20/200 or
Significant improvement in BVCA was seen with ranibizu- <
_20/40 and whose CRT was > _270 mm at baseline.21,22
mab alone (þ6.1 letters) and combined with laser (þ5.9 These patients were randomized to receive intravitreal
letters) compared with laser monotherapy (þ0.8 letters) bevacizumab (ivB) 1.25 mg every 6 weeks or laser
at 12 months. The proportions of patients who gained treatment every 4 months. Retreatment was based on CRT
>
_10 and > _15 letters were 2-3 times greater in the ranibizu- stability. Results at 2 years showed that patients who were
mab groups compared within the laser group (37.4% vs treated with ivB had þ8.6 mean letter gain compared with
15.5% and 22.6% vs 8.2%, respectively). Approximately a mean loss of 0.5 letters with laser. The proportion of
9.2% more patients experienced > _10 letters loss with laser patients who gained > _10 letters was significantly greater for
than with ranibizumab. Up to 8.2% of patients experienced ivB than for laser (49% vs 7%, P ¼ .001). Approximately
loss of >
_15 letters with laser only compared with 0.9% in 32% of patients in the ivB group gained > _15 letters,
the ranibizumab-only group. compared with 4% in the laser group (P ¼ .004). No
DRCR.net protocol I was a 5-year, independent, multi- patient lost >_15 letters with ivB but 14% of patients in the
center RCT involving 854 study eyes with center- laser group sustained > _15 letters loss (P ¼ .03).
involved DME causing vision impairment 20/32-20/320 Soheilian and associates reported a phase III RCT exam-
and central subfield thickness > _250 mm.11 Patients were ining the efficacy of ivB alone or in combination with
randomized to receive sham injection plus prompt laser, intravitreal triamcinolone acetonide (IVTA) vs laser photo-
ranibizumab 0.5 mg plus prompt laser, ranibizumab coagulation as primary treatment for DME.23 One hundred
0.5 mg plus deferred (> _24 weeks) laser, or triamcinolone and fifty eyes of 129 treatment-naı̈ve patients with VA 20/
4 mg plus prompt laser. Results demonstrated that ranibizu- 50-20/300 were randomized to receive ivB, combined ivB
mab combined with prompt or deferred laser therapy was and IVT, or laser treatment. The treatments were adminis-
more effective than laser alone for the treatment of tered at 12-week intervals. After 3 loading doses, further
DME, with substantially more eyes gaining ETDRS letters ivB injections were given if DME persisted and VA was not
and fewer eyes losing ETDRS letters (Supplemental better than 20/40. Mean VA improvement for ivB was
Table 1, available at AJO.com). The mean change from 12.8% compared with 9.5% for ivB and IVTA and 10.9%
baseline VA at 1 year was þ9 letters in the ranibizumab for laser, but the results were not statistically significant.
plus prompt or deferred laser groups, compared with þ3 let- The superior effect of ivB over other treatments was signifi-
ters in the sham plus prompt laser group. VA continued to cant at 6 months but diminished thereafter. The proportion
improve in the second year by a mean change of þ3.7 let- of eyes with >
_15 letter gain was 41.0% for ivB, 36.1% for com-
ters more with ranibizumab plus prompt laser and þ5.8 bined ivB and IVTA, and 23.7% for laser treatment.
letters more with ranibizumab plus deferred treatment,
compared with sham plus prompt laser treatment.12 At 3 Aflibercept. A key RCT of note is the phase II, double-
years, prompt laser treatment was related to fewer cumula- masked, active-controlled DME and VEGF Trap-Eye:
tive ranibizumab injections than deferred, but patients who INvestigation of Clinical Impact (DA VINCI) study,
received deferred laser experienced better visual outcomes which was designed to examine the effects of intravitreal
(þ6.8 letters vs þ9.7 letters, respectively, P ¼ .02).13 aflibercept compared to those of standard laser
RISE and RIDE were 2 parallel, phase III, double- treatment.24,25 Patients (n ¼ 221) with CSME with
masked, sham-controlled RCTs comparing the efficacy baseline BCVA 20/40-20/320 and CRT > _250 mm were
and safety of ranibizumab 0.3 mg and 0.5 mg over randomized to receive VEGF Trap-Eye at different dosage
24 months.14 The overall study population involved 759 and schedules or laser treatment (Supplemental Table 1,
patients (1 eye per patient) with center-involved DME available at AJO.com). Results at 52 weeks showed greater
who had VA 20/40-20/320 and central subfield thickness VA gains for aflibercept (9.7-12.0 letters) than for laser
>
_275 mm. In both studies, the proportion of patients who treatment (1.3 letters).25 Patients who were treated with
gained > _15 letters with ranibizumab was twice that of VEGF Trap-Eye were more likely to experience gains of
patients receiving sham injections (Supplemental >
_10 and > _15 letters than those who received laser
Table 1, available at AJO.com), with an average gain of treatment (45%-71% vs 30% and 23.8%-45.5% vs 11.4%,
8.5-9.9 letters from baseline at month 24 with ranibizumab respectively). The following phase III studies are currently
compared with sham treatment (P < .0001). In addition, underway: VEGF Trap-Eye in Vision Impairment due to
patients treated with ranibizumab were found to have a DME (VIVID-DME; NCT01331681), VIVID EAST-DME
VOL. 157, NO. 3 DIABETIC MACULAR EDEMA MANAGEMENT 507(NCT01783886), Japanese Safety Study of VEGF Trap-Eye well as aflibercept (NCT01627249), in DME are in progress
in DME (VIVID-Japan; NCT01512966), and Study of and should provide additional insights on this issue. Systemic
Intravitreal Administration of VEGF Trap-Eye (BAY86- adverse events in patients who received ranibizumab for DME
5321) in Patients with DME (VISTA; NCT01363440). occurred at rates equal to those in patients who received laser
treatment or sham injection. The incidences of cardiovascu-
Pegaptanib. A phase II/III, multicenter, double-masked, lar events and arterial thromboembolism reported in these
sham-controlled, parallel-group study reported by Sultan studies were low, possibly because high-risk patients were
and associates was performed to compare the effects of excluded. A definitive conclusion regarding the safety of
pegaptanib 0.3 mg and sham injections in patients with type bevacizumab could not be drawn from the BOLT study owing
1 and type 2 DM, center-involved DME (CRT > _250 mm), to its small sample size.21,22 The safety profile of aflibercept
and vision loss (BVCA 20/50-20/200).26 Efficacy results reported in the DA VINCI study was consistent with those
were derived from 1-year (n ¼ 260) and 2-year (n ¼ 207) seen with other intravitreal anti-VEGF agents.24,25 Data
intention-to-treat analyses. Treatment was administered at from both the RESTORE and BOLT studies also showed
6-week intervals during the first year and as needed that anti-VEGF treatment had no deleterious effect on capil-
subsequently. Rescue focal/grid photocoagulation was lary perfusion at the macula.10,21,22
permitted after week 18. At 1 year, 36.8% of patients in the
pegaptanib group achieved > _10-letter gains compared with INTRAVITREAL CORTICOSTEROIDS: Triamcinolone
19.7% in the sham group. These proportions increased to Acetonide. In a 2-year, phase II/III, double-masked,
38.3% and 30.0%, respectively, in the second year. Mean placebo-controlled RCT, 84 eyes in 54 patients with
BCVA change from baseline was 6.1 letters in the diffuse or focal DME with VA 20/40-20/400 and CRT
pegaptanib group compared with 1.3 letters in the sham >250 mm were randomized to receive IVTA 4 mg vs
group at 2 years (P < .01). Significantly fewer patients in placebo 6 weeks before laser treatment.35 Although the
the pegaptanib group required laser treatment than in the proportion of patients in the IVTA plus laser group who
sham group in the first (23.3% vs 41.7%, P ¼ .0023) and experienced 10-letter improvement was double that in
second years (25.2% vs 45.0%, P ¼ .0032). the laser-only group, there was no difference in mean VA
or CRT change between the 2 groups. The need for
ANTI–VASCULAR ENDOTHELIAL GROWTH FACTOR further treatment during the second year of the study was
SAFETY: Ranibizumab was generally well tolerated in all no lower in the IVTA group than in the laser-only group
studies.10–14,17–20 The most commonly reported ocular- (69% vs 45%, P ¼ .187).
related serious adverse events were endophthalmitis and In another 2-year, prospective, double-masked RCT, 69
increased intraocular pressure (IOP). Because patients eyes in 43 patients with advanced, refractory DME and
with DM have a higher risk of cardiovascular disease that impaired vision (BCVA 20/30 or worse) were given 4 mg
is exacerbated in the presence of DME, the safety profile IVTA or placebo.36 IVTA improved BCVA by > _5 letters
of anti-VEGF agents should be carefully considered.24–31 in 19 of 34 eyes (56%) compared with in 9 of 35 eyes
For age-related macular degeneration (AMD), the 2-year (26%) treated with placebo. Mean VA improvement was
Comparison of Age-related Macular Degeneration Treat- 5.7 letters more with IVTA than with placebo. The BVCA
ment Trial (CATT) demonstrated no significant difference gains with IVTA were maintained after 5 years in 42% of
in arteriothromboembolic events or deaths between beva- eyes.37 However, initial treatment with IVTA did not reduce
cizumab and ranibizumab.32 The incidence of systemic the risk of recurrent edema and need for further injections.
serious adverse events was significantly higher in patients The phase III DRCR.net study compared the effects of
who received bevacizumab, although it was uncertain if 1 mg and 4 mg IVTA against those of laser treatment in
these were drug related. In contrast to the CATT, interim 840 eyes of 693 patients with DME and visual impairment
analysis from the Alternative Treatments to Inhibit VEGF 20/40-20/320.38 Laser treatment was superior to IVTA at 2
in Age-related Choroidal Neovascularization (IVAN) years, despite an initial greater response with IVTA. The
study demonstrated a more favorable safety profile for beva- mean difference in VA change for laser vs 1 mg IVTA
cizumab over ranibizumab.33 Even if inferences were to be was 3.5 (P ¼ .02) and 4.6 (P ¼ .002) for laser vs 4 mg
drawn from the CATT and IVAN studies, DME and AMD IVTA. There was no significant difference between the 2
should be considered as separate disease entities. IVTA groups (mean difference 1.1, P ¼ .49).
If ranibizumab and bevacizumab were equally effective and In the DRCR.net protocol I study evaluating patients
safe, bevacizumab would be considered more cost effective.34 receiving 0.5 mg ranibizumab combined with prompt or
The annual risk of cerebrovascular accident would have to be deferred laser, 4 mg IVTA plus prompt laser, or laser
at least 1.5% higher with bevacizumab in order for ranibizu- only, treatment with IVTA plus laser resulted in a mean
mab to be the preferred anti-VEGF treatment.34 Whether loss of 1.5 letters from baseline compared with laser-only
one anti-VEGF drug is safer than the other for DME remains treatment at 12 months.11 In an analysis limited to pseudo-
to be answered. Head-to-head studies comparing ranibizumab phakic eyes, the mean change in VA was 1.6 letters greater
and bevacizumab (NCT00545870 and NCT01610557), as in the IVTA plus prompt laser group compared within the
508 AMERICAN JOURNAL OF OPHTHALMOLOGY MARCH 2014laser-only group, and this was comparable to the improve- well-designed RCTs with long-term follow-up is needed
ments achieved with ranibizumab plus prompt/deferred to establish a role for this treatment approach in DME.
laser.
Fluocinolone acetonide. The Fluocinolone Acetonide in
Diabetic Macular Edema (FAME) study, a 36-month, TREATMENT GUIDELINES
double-masked, sham-controlled, phase III study,
examined the efficacy and safety profile of fluocinolone TREATMENT OF DME SHOULD BE PRECEDED BY ASSESSMENT
acetonide (FA) compared with that of sham injection in of VA, a full ocular examination, and confirmation of
patients with persistent or recurrent DME.39,40 Patients DME. Although the ETDRS definition of CSME has
(n ¼ 956) with BCVA 20/50-20/200 and CRT > _250 mm long been considered the ‘‘gold standard’’ for characterizing
were randomized to receive 0.2 mg or 0.5 mg FA DME severity, it remains difficult to use and does not help
intravitreal inserts or sham injection. Treatment efficacy identify patients at risk of vision loss.49 Another definition
was similar for low- and high-dose FA but the benefit-to- for DME is the International Clinical Classification Scale
risk profile was more favorable with the low dose. FA (Supplemental Table 2, available at AJO.com).[C:III]49
provided no benefit in preventing vision loss compared As outlined earlier, DME should be more simply defined
with nontreatment, as similar proportions of patients as thickening of the central or noncentral macula,
progressed to blindness (BCVA 20/200 or worse). In confirmed either at slit-lamp biomicroscopy or with
another phase II/III study evaluating the efficacy and OCT, which is not explained by thickening from an
safety of FA 0.59 mg inserts against standard of care (ie, ERM. Currently, qualitative assessment of thickening
laser treatment or observation), there was no significant seen on OCT is used to define DME. Further research is
difference in the proportion of eyes gaining > _15 letters needed to clarify if specific features (eg, intraretinal cysts
between patients in both arms after 3 years post implant.41 or disruption of the inner segment/outer segment junction)
and quantitative measures (eg, volume of thickening) are
INTRAVITREAL CORTICOSTEROID SAFETY: The high useful in assessing the need for anti-VEGF treatment or
incidence of premature cataract formation and increased in predicting outcomes.
IOP with intravitreal corticosteroids compared to with
sham and laser treatments raises important concerns INDICATIONS FOR ANTI–VASCULAR ENDOTHELIAL
in clinical practice.35–41 The risk for interventional GROWTH FACTOR THERAPY: Findings from meta-
procedures, such as cataract surgery, laser trabeculoplasty, analyses by Virgili and associates50 and Wang and associ-
and incisional glaucoma surgery, increases treatment ates51 support the use of anti-VEGF agents, namely ranibi-
morbidity. There was no significant difference in the rate zumab, as an alternative or adjunctive treatment to laser.
of adverse events when IVTA was extended to 5 years.37 Treatment with anti-VEGF should be considered if
A minority of patients in the IVTA study who underwent center-involving DME is present and VA is 20/30 or worse,
steroid-induced cataract surgery became unresponsive to as this was the basis for entry into both the RESTORE and
further IVTA treatments and experienced poorer visual the DRCR.net Protocol I studies. Outcomes showed visual
prognosis than those who did not need surgery.3 Patients benefit for subgroups with this level of VA.[A:I]10–14,17–20
who received FA were also more likely to report cardiovas- Focal laser photocoagulation using ETDRS guidelines
cular adverse events than sham-treated patients, although should still be considered for patients with DME without
the incidence seemed to be low (TABLE. Summary of Diabetic Macular Edema Treatment
Recommendations
Key Points Evidence Levela
Laser therapy remains the standard of care A:I4
for patients with non-center-involving
edema or early DME without decreased
VA
Commence anti-VEGF treatment in patients A:I10–14,17–20
with center-involving DME and VA of 20/
30 or worse
In patients who do not meet the threshold A:III4
for anti-VEGF treatment, manage
according to ETDRS guidelines using
focal or grid laser treatment
Ranibizumab injections should be A:I10–13,53
administered on a monthly basis for at
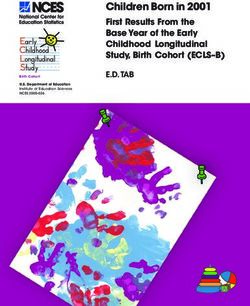
FIGURE. Diabetic macular edema (DME) treatment flow dia- least 3 visits, then as needed depending
gram. Treatment should be given according to the Early Treat- on VA (with or without OCT) stability
ment for Diabetic Retinopathy Study (ETDRS) guidelines in Follow-up should be monthly for A:I10–14,53
patients without center involvement, and in patients with center 6-12 months; once visual stability
involvement but with vision better than 20/30. Anti–vascular can be maintained for 3 consecutive
endothelial growth factor (anti-VEGF) treatment is recommended visits, follow-up intervals can be
in patients with center involvement and vision 20/30 or worse. prolonged to between 2 and 4 months
OCT [ optical coherence tomography; VA [ visual acuity. Administer ETDRS laser treatment if A:I10–14,53
response to anti-VEGF treatment is
unsatisfactory, generally after at least
given for at least 3 consecutive months (‘‘loading’’ dose) 6 months
followed by monthly assessment visits.[A:I]10–13,53 The Vitrectomy may be indicated when A:II56,57
decision to continue anti-VEGF injections may be guided vitreomacular traction is responsible for C:III46–48
either by VA stability (RESTORE) or by VA and OCT sta- reduced VA, after confirming its presence
using spectral-domain OCT; such cases
bility (DRCR.net Protocol I). The rationale for using VA
may also respond to adjunctive
stability is that if VA is still improving, or if VA has fallen
intravitreal anti-VEGF, corticosteroid,
and this reduction is considered attributable to DME, then and/or laser therapy
injection should be continued. If VA is stable for at least 2 There may be a role for IVTA as an adjunct B:I11,12
consecutive visits, then injections could be suspended and to laser treatment in pseudophakic eyes
monthly follow-up continued. Stability of signs on OCT, of DME patients; further data are needed
particularly the presence of intraretinal or subretinal fluid,
could also guide either the continuation or the suspension DME ¼ diabetic macular edema; ETDRS ¼ Early Treatment
Diabetic Retinopathy Study; IVTA ¼ intravitreal triamcinolone
of injections.[C:III]53
acetonide; OCT ¼ optical coherence tomography; VA ¼ visual
The fixed monthly schedule used in RISE and RIDE
acuity; VEGF ¼ vascular endothelial growth factor.
was designed to optimize treatment outcomes based on a
Presented as importance of clinical outcome, strength of
the pharmacokinetic studies of ranibizumab,54 but this evidence. A indicates that the recommendation is considered
schedule leads to considerable burden in DME patients very important or crucial to a good clinical outcome; B, moder-
who frequently have multiple comorbidities, with regular ately important to clinical outcome; C, may be relevant but cannot
visits needed to many other subspecialists. Fixed dosing be definitely related to clinical outcome. I indicates data providing
also leads to greater exposure to treatment-related risks strong evidence in support of clinical recommendation; II, sub-
and increased treatment costs. stantial evidence in support of recommendation but the
The treatment approach proposed was therefore based on evidence lacks some qualities; III, insufficient evidence to provide
flexible dosing schedules used in both the RESTORE support for or against recommendation, or panel consensus.15
(Supplemental Figure 1, available at AJO.com) and
DRCR.net (Supplemental Figure 2, available at AJO.com) follow-up visits, and the visual and quality-of-life outcomes
treatment protocols. The validity of a flexible dosing between flexible and fixed dosing schedules.
schedule is supported by its ability to maintain visual stability Doubling of follow-up intervals may be considered within
achieved early in the treatment initiation phase with less the first 6 months if visual stability can be maintained for 3
than monthly injections.10–13,53 Future studies should consecutive visits.[C:I]10–13,53 If DME continues to progress
quantify and compare costs associated with treatment, and other causes of vision loss have been excluded,
510 AMERICAN JOURNAL OF OPHTHALMOLOGY MARCH 2014laser treatment should be considered using ETDRS to aid in patient selection. The appropriate dose for anti-
guidelines.[A:I]10–13,53 In patients with DME undergoing VEGF treatment remains to be defined, as existing
cataract surgery, efforts should be made to resolve the DME trials were not powered to compare different doses (eg,
before surgery.[A:I]55 The DRCR.net cautions against the ranibizumab 0.3 mg vs 0.5 mg). The clinical impact and
long-term use of IVTA owing to increased risk of glaucoma cost effectiveness of both flexible and fixed monthly dosing
and almost inevitable progression of cataract.[A:I]11,12,38 regimens also require further exploration.
However, pseudophakic eyes may benefit from combined
IVTA and laser therapy, although similar outcomes were
achieved with ranibizumab plus laser without steroid
complications.[A:I]11–13 IVTA may provide an alternative
CONCLUSIONS
to anti-VEGF therapy in patients who are either hypersensi- DME IS THE MAJOR CAUSE OF VISION LOSS IN PATIENTS
tive or nonresponsive to anti-VEGF therapy.[A:I]11–13 The with DM. Although laser treatment has long been the pri-
Table summarizes the recommendations discussed in this mary therapy for preventing blindness in patients with
section. DME, treatment goals should now aim to restore impaired
vision, prevent further vision loss, and improve visual func-
tion. Recent RCTs suggest that these goals can be obtained
DISCUSSION using intravitreal anti-VEGF therapy, with a well-
documented tolerable safety profile. As a result of these
RECOMMENDATIONS MADE IN THIS GUIDELINE WERE BASED recent data, we propose the use of anti-VEGF therapy as
on the best available data; results from ongoing and future the first line of treatment in place of laser photocoagulation
RCT studies may alter treatment recommendations. There in DME causing vision loss.
are certain limitations to our recommendations. As high- We note that the current evidence is largely based on
lighted, although there is value in using OCT to define studies with ranibizumab. Until additional data for the
DME, a standardized OCT-based DME classification has use of bevacizumab and aflibercept become available, this
yet to be developed, and the features that predict the guideline recommends ranibizumab as the treatment of
need or type of treatment and the treatment outcomes choice for patients with center-involving DME with mod-
remain unclear. Comparative evidence on the long-term erate visual impairment. This is recommended to be given
efficacy and safety of anti-VEGF agents in DME are absent. in a flexible dosing schedule, rather than continuously.
There is currently no evidence to support the use of anti- Patients who do not yet meet the treatment threshold
VEGF agents in eyes with VA better than 20/30. More should be managed with laser therapy according to ETDRS
data on predictors of treatment response are also needed guidelines or should continue to be closely observed.
BOTH AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OF INTER-
est. Paul Mitchell has served on advisory boards for Abbott, Allergan, Bayer, Novartis, and Pfizer, and has received honoraria for travel, service on advisory
boards, and research support from these companies. Tien Yin Wong is on advisory boards for Abbott, Allergan, Bayer, Novartis, and Pfizer, and has received
honoraria for travel, service on advisory boards, and research support from these companies. Funding for Diabetic Macular Edema Treatment Guideline
Working Group member meetings and the medical writing service was provided by Novartis AG, Basel, Switzerland. Contributions of authors: concept and
outline (P.M., T.Y.W.); literature search (T.Y.W.); manuscript development (P.M., T.Y.W.); review and final approval (P.M., T.Y.W.). All content was
reviewed, discussed, and given final approval by the DME Treatment Guideline Working Group Members.
The Diabetic Macular Edema Treatment Guideline Working Group consists of the following members from the Asia-Pacific region: Paul Mitchell
(Centre for Vision Research, Westmead Millennium Institute, University of Sydney, Australia); David Liu (Chinese University of Hong Kong, China);
Taraprasad Das (L.V. Prasad Eye Institute, Bhubaneswar, India); Iwan Sovani (National Eye Center Cicendo Eye Hospital, Bandung, Indonesia);
Hakyoung Kim (Hallym University Medical Center, Seoul, South Korea); Hyung Chan Kim (Konkuk University School of Medicine, Seoul, South
Korea); Hyung Woo Kwak (Kyung Hee University Medical Center, Seoul, South Korea); Harvey Uy (Pacific Eye and Laser Institute, Makati City,
Manila, Philippines); Tien Yin Wong (Singapore Eye Research Institute, Singapore National Eye Centre, National University of Singapore, Singapore);
Shwu-Jiuan Sheu (Kaoshiung Veterans Hospital, Kaoshiung, Taiwan); Paisan Ruamviboonsuk (Rajavithi Hospital, Bangkok, Thailand).
The authors thank Charity Yii Tien Jen of In Vivo Communications (Asia) Pte Ltd for medical writing support, which encompassed research, drafting,
and revisions of the manuscript, tables, and figures, all under the direction of the authors. Novartis AG did not influence any content of this paper. The
authors and the Diabetic Macular Edema Treatment Guideline Working Group did not receive any honorarium for their involvement in the development
of this manuscript.
REFERENCES 3. Yau JWY, Rogers SL, Kawasaki R, et al; for the Meta-Analysis
for Eye Disease (META-EYE) Study Group. Global prevalence
1. Cheung N, Mitchell P, Wong TY. Diabetic retinopathy. and major risk factors of diabetic retinopathy. Diabetes Care
Lancet 2010;376(9735):124–136. 2012;35(3):1–9.
2. Moss SE, Klein R, Klein BE. The 14-year incidence of visual 4. Early Treatment Diabetic Retinopathy Study Research
loss in a diabetic population. Ophthalmology 1998;105(6): Group. Photocoagulation for diabetic macular edema. ETDRS
998–1003. report number 1. Arch Ophthalmol 1985;103(12):1796–1806.
VOL. 157, NO. 3 DIABETIC MACULAR EDEMA MANAGEMENT 5115. Ding J, Wong TY. Current epidemiology of diabetic retinop- 21. Michaelides M, Kaines A, Hamilton RD, et al. A prospective
athy and diabetic macular edema. Curr Diab Rep 2012;12(4): randomized trial of intravitreal bevacizumab or laser therapy
346–354. in the management of diabetic macular edema (BOLT
6. Benarous R, Sasongko MB, Qureshi S, et al. Differential asso- study) 12-month data: report 2. Ophthalmology 2010;117(6):
ciation of serum lipids with diabetic retinopathy and diabetic 1078–1086.
macular edema. Invest Ophthalmol Vis Sci 2011;52(10): 22. Rajendram R, Fraser-Bell S, Kaines A, et al. A 2-year prospec-
7464–7469. tive randomized controlled trial of intravitreal bevacizumab
7. Lim LS, Wong TY. Lipids and diabetic retinopathy. Expert or laser therapy (BOLT) in the management of diabetic mac-
Opin Biol Ther 2012;12(1):93–105. ular edema: 24-months data: report 3. Arch Ophthalmol 2012;
8. Bhagat N, Grigorian RA, Tutela A, Zarbin MA. Diabetic 130(8):972–979.
macular edema: pathogenesis and treatment. Surv Ophthalmol 23. Soheilian M, Garfami KH, Ramezani A, Yaseri M,
2009;54(1):1–32. Peyman GA. Two-year results of a randomized trial of intra-
9. Bressler NM, Miller KM, Beck RW, et al; for the Diabetic vitreal bevacizumab alone or combined with triamcinolone
Retinopathy Clinical Research Network. Observational study versus laser in diabetic macular edema. Retina 2012;32(2):
of subclinical diabetic macular edema. Eye (Lond) 2012; 314–321.
26(6):833–840. 24. Do DV, Schmidt-Erfurth U, Gonzalez VH, et al. The DA
10. Mitchell P, Bandello F, Schmidt-Erfurth U, et al; for the VINCI Study: phase 2 primary results of VEGF Trap-Eye in
RESTORE study group. The RESTORE study: ranibizumab patients with diabetic macular edema. Ophthalmology 2011;
monotherapy or combined with laser versus laser monother- 118(9):1819–1826.
apy for diabetic macular edema. Ophthalmology 2011;118(4): 25. Do DV, Nguyen QD, Boyer D, et al. One-year outcomes of
615–625. the DA VINCI Study of VEGF Trap-Eye in eyes with diabetic
11. Elman MJ, Aiello LP, Beck RW, et al; for the Diabetic macular edema. Ophthalmology 2012;119(8):1658–1665.
Retinopathy Clinical Research Network. Randomized trial 26. Sultan MB, Zhou D, Loftus J, Dombi T, Ice KS, for the Macu-
evaluating ranibizumab plus prompt or deferred laser or triam- gen 1013 Study Group. A phase 2/3, multicenter, random-
cinolone plus prompt laser for diabetic macular edema. ized, double-masked, 2-year trial of pegaptanib sodium for
Ophthalmology 2010;117(6):1064–1077. the treatment of diabetic macular edema. Ophthalmology
12. Elman MJ, Bressler NM, Qin H, et al; for the Diabetic Reti- 2011;118(6):1107–1118.
nopathy Clinical Research Network. Expanded 2-year follow- 27. Hirai FE, Knudtson MD, Klein BE, Klein R. Clinically signif-
up of ranibizumab plus prompt or deferred laser or triamcino- icant macular edema and survival in type 1 and type 2 dia-
lone plus prompt laser for diabetic macular edema. Ophthal- betes. Am J Ophthalmol 2008;145(4):700–706.
mology 2011;118(4):609–614. 28. Nguyen-Khoa BA, Goehring EL Jr, Werther W, et al. Hospi-
13. Elman MJ, Qin H, Aiello LP, et al; for the Diabetic Retinop- talized cardiovascular events in patients with diabetic macu-
athy Clinical Research Network. Intravitreal ranibizumab for lar edema. BMC Ophthalmol 2012;12(1):11.
diabetic macular edema with prompt versus deferred laser 29. Cheung N, Lam DS, Wong TY. Anti-vascular endothelial
treatment: three-year randomized trial results. Ophthalmology growth factor treatment for eye diseases. BMJ 2012;344:
2012;119(11):2312–2318. e2970.
14. Nguyen QD, Brown DM, Marcus DM, et al; for the RISE and 30. van der Reis MI, La Heij EC, De Jong-Hesse Y,Ringens PJ,
RIDE Research Group. Ranibizumab for diabetic macular Hendrikse F, Schouten JS. A systematic review of the adverse
edema: results from 2 phase III randomized trials: RISE and events of intravitreal anti-vascular endothelial growth factor
RIDE. Ophthalmology 2010;119(4):789–801. injections. Retina 2011;31(8):1449–1469.
15. Minckler D. Evidence-based ophthalmology series and 31. Lim LS, Cheung CM, Mitchell P, Wong TY. Emerging evi-
content-based continuing medical education for the journal. dence concerning systemic safety of anti-VEGF agents—
Ophthalmology 2000;107(1):9–10. should ophthalmologists be concerned? Am J Ophthalmol
16. Luttrull JK, Dorin G. Subthreshold diode micropulse laser 2011;152(3):329–331.
photocoagulation (SDM) as invisible retinal phototherapy 32. Martin DF, Maguire MG, Fine SL, et al; for the Comparison
for diabetic macular edema: a review. Curr Diabetes Rev of Age-related Macular Degeneration Treatments Trials
2012;8(4):274–284. (CATT) Research Group. Ranibizumab and bevacizumab
17. Massin P, Bandello F, Garweg JG, et al. Safety and efficacy of for treatment of neovascular age-related macular degen-
ranibizumab in diabetic macular edema (RESOLVE Study): a eration: two-year results. Ophthalmology 2012;119(7):
12-month, randomized, controlled, double-masked, multi- 1388–1398.
center phase II study. Diabetes Care 2010;33(11):2399–2405. 33. Chakravarthy U, Harding SP, Rogers CA, et al; for the IVAN
18. Nguyen QD, Shah SM, Khwaja AA, et al. Two-year out- Study. Ranibizumab versus bevacizumab to treat neovascular
comes of the ranibizumab for edema of the macula in diabetes age-related macular degeneration: one-year findings from
(READ-2) study. Ophthalmology 2010;117(11):2146–2151. the IVAN randomized trial. Ophthalmology 2012;119(7):
19. Do DV, Nyuyen QD, Khwaja AA, et al. Ranibizumab for 1399–1411.
edema of the macula in diabetes study. 3-year outcomes and 34. Stein JD, Newman-Casey PA, Kim DD, Nwanyanwu KH,
the need for prolonged frequent treatment. JAMA Ophthalmol Johnson MW, Hutton DW. Cost-effectiveness of various
2013;131(2):139–145. interventions for newly diagnosed diabetic macular edema.
20. Ip MS, Domalpally A, Hopkins JJ, Wong P, Ehrlich JS. Long- Ophthalmology 2013;120(9):1835–1842.
term effects of ranibizumab on diabetic retinopathy severity 35. Gillies MC, McAllister IL, Zhu M, et al. Intravitreal triam-
and progression. Arch Ophthalmol 2012;130(9):1145–1152. cinolone prior to laser treatment of diabetic macular edema:
512 AMERICAN JOURNAL OF OPHTHALMOLOGY MARCH 201424-month results of a randomized controlled trial. Ophthal- 47. Kang SW, Park SC, Cho HY, Kang JH. Triple therapy of vit-
mology 2011;118(5):866–872. rectomy, intravitreal triamcinolone, and macular laser photo-
36. Gillies MC, Sutter FK, Simpson JM, et al. Intravitreal triam- coagulation for intractable diabetic macular edema. Am J
cinolone for refractory diabetic macular edema: two-year Ophthalmol 2007;144(6):878–885.
results of a double-masked, placebo-controlled, randomized 48. Robaszkiewicz J, Chmielewska K, Figurska M, Wierzbowska J,
clinical trial. Ophthalmology 2006;113(9):1533–1538. Stankiewicz A. Triple therapy: phaco-vitrectomy with ILM
37. Gillies MC, Simpson JM, Gaston C, et al. Five-year results of peeling, retinal endophotocoagulation, and intraoperative
a randomized trial with open-label extension of triamcino- use of bevacizumab for diffuse diabetic macular edema. Med
lone acetonide for refractory diabetic macular edema. Sci Monit 2012;18(4):CR241–CR251.
Ophthalmology 2009;116(11):2182–2187. 49. Wilkinson CP, Ferris FL III, Klein RE, et al; for the Global
38. Diabetic Retinopathy Clinical Research Network. A ran- Diabetic Retinopathy Project Group. Proposed interna-
domized trial comparing intravitreal triamcinolone acetonide tional clinical diabetic retinopathy and diabetic macular
and focal/grid photocoagulation for diabetic macular edema. edema disease severity scales. Ophthalmology 2003;110(9):
Ophthalmology 2008;115(9):1447–1449, 1449.e1–10. 1677–1682.
39. Campochiaro PA, Brown DM, Pearson A, et al. Long-term 50. Virgili G, Parravano M, Menchini F, Brunetti M. Antiangio-
benefit of sustained-delivery fluocinolone acetonide vitreous genic therapy with anti-vascular endothelial growth factor
inserts for diabetic macular edema. Ophthalmology 2011; modalities for diabetic macular oedema. Cochrane Database
118(4):626–635.e2. Syst Rev 2012;12:CD007419.
40. Campochiaro PA, Brown DM, Pearson A, et al; for the FAME 51. Wang H, Sun X, Liu K, Xu X. Intravitreal ranibizumab
Study Group. Sustained delivery fluocinolone acetonide vitre- (Lucentis) for the treatment of diabetic macular edema: a sys-
ous inserts provide benefit for at least 3 years in patients with dia- tematic review and meta-analysis of randomized clinical con-
betic macular edema. Ophthalmology 2012;119(10):2125–2132. trol trials. Curr Eye Res 2012;37(8):661–670.
41. Pearson PA, Comstock TL, Ip M, et al. Fluocinolone aceto- 52. Bressler SB, Qin H, Beck RW, et al; for the Diabetic Retinop-
nide intravitreal implant for diabetic macular edema: a 3- athy Clinical Research Network. Factors associated with
year multicenter, randomized, controlled clinical trial. changes in visual acuity and central subfield thickness at 1
Ophthalmology 2011;118(8):1580–1587. year after treatment for diabetic macular edema with ranibi-
42. Yanyali A, Horozoglu F, Celik E, Ercalik Y, Nohutcu AF. Pars zumab. Arch Ophthalmol 2012;130(9):1153–1161.
plana vitrectomy and removal of the internal limiting mem- 53. Aiello LP, Beck RW, Bressler NM, et al; for the Diabetic
brane in diabetic macular edema unresponsive to grid laser Retinopathy Clinical Research Network. Rationale for the
photocoagulation. Eur J Ophthalmol 2006;16(4):573–581. diabetic retinopathy clinical research network treatment pro-
43. Thomas D, Bunce C, Moorman C, Laidlaw DA. A randomised tocol for center-involved diabetic macular edema. Ophthal-
controlled feasibility trial of vitrectomy versus laser for mology 2011;118(12):e5–14.
diabetic macular oedema. Br J Ophthalmol 2005;89(1):81–86. 54. Bakri SJ, Snyder MR, Reid JM, Pulido JS, Ezzat MK, Singh RJ.
44. Dhingra N, Sahni J, Shipley J, et al. Vitrectomy and internal Pharmacokinetics of intravitreal ranibizumab (Lucentis).
limiting membrane (ILM) removal for diabetic macular Ophthalmology 2007;114(12):2179–2182.
edema in eyes with absent vitreo-macular traction fails to 55. Dowler JG, Hykin PG, Lightman SK, Hamilton AM. Visual
improve visual acuity: results of a 12 months prospective ran- acuity following extracapsular cataract extraction in diabetes:
domized controlled clinical trial. Invest Ophthalmol Vis Sci a meta-analysis. Eye (Lond) 1995;9(Pt 3):313–317.
2005;46:E-Abstract 1467. 56. Haller JA, Qin H, Apte RS, et al; for the Diabetic Retinop-
45. Bahadir M, Ertan A, Mertoglu O. Visual acuity comparison of athy Clinical Research Network. Vitrectomy outcomes in
vitrectomy with and without internal limiting membrane eyes with diabetic macular edema and vitreomacular traction.
removal in the treatment of diabetic macular edema. Int Ophthalmology 2010;117:1087–1093.e3.
Ophthalmol 2005;26(1-2):3–8. 57. Chhablani JK, Kim JS, Cheng L, Kozak I, Freeman W.
46. Kim YT, Kang SW, Kim SJ, Kim SM, Chung SE. Combination External limiting membrane as a predictor of visual
of vitrectomy, IVTA, and laser photocoagulation for diabetic improvement in diabetic macular edema after pars plana vit-
macular edema unresponsive to prior treatments; 3-year rectomy. Graefes Arch Clin Exp Ophthalmol 2012;250(10):
results. Graefes Arch Clin Exp Ophthalmol 2012;250(5):679–684. 1415–1420.
VOL. 157, NO. 3 DIABETIC MACULAR EDEMA MANAGEMENT 513SUPPLEMENTAL REFERENCES 12. Diabetes Control and Complications Trial Research Group.
The effect of intensive treatment of diabetes on the develop-
1. Mohamed Q, Gillies MC, Wong TY. Management of diabetic ment and progression of long-term complications in insulin-
retinopathy: a systematic review. JAMA 2007;298(8): dependent diabetes mellitus. N Engl J Med 1993;329(14):
902–916. 977–986.
2. UK Prospective Diabetes Study (UKPDS) Group. Intensive 13. White NH, Sun W, Cleary PA, et al. Prolonged effect of
blood-glucose control with sulphonylureas or insulin intensive therapy on the risk of retinopathy complications
compared with conventional treatment and risk of complica- in patients with type 1 diabetes mellitus: 10 years after the
tions in patients with type 2 diabetes (UKPDS 33). Lancet Diabetes Control and Complications Trial. Arch Ophthalmol
1998;352(9131):837–853. 2008;126(12):1707–1715.
3. Diabetes Control and Complications Trial Research Group. 14. Beulens JW, Patel A, Vingerling JR, et al; AdRem project
The effect of intensive diabetes treatment on the progression team; ADVANCE management committee. Effects of blood
of diabetic retinopathy in insulin dependent diabetes melli- pressure lowering and intensive glucose control on the inci-
tus. The Diabetes Control and Complications Trial. Arch dence and progression of retinopathy in patients with type
Ophthalmol 1995;113(1):36–51. 2 diabetes mellitus: a randomised controlled trial. Diabetologia
4. Diabetes Control and Complications Trial Research Group. 2009;52(10):2027–2036.
The relationship of glycaemic exposure (HbA1c) to the risk 15. Patel A, MacMahon S, Chalmers J, et al; for the ADVANCE
of development and progression of retinopathy in the Dia- Collaborative Group. Intensive blood glucose control and
betes Control and Complications Trial. Diabetes 1995; vascular outcomes in patients with type 2 diabetes. N Engl J
44(8):968–983. Med 2008;358(24):2560–2572.
5. Chew EY, Ambrosius WT, Davis MD, et al; for the ACCORD 16. Chaturvedi N, Sjolie AK, Stephenson JM, et al. Effect of lisi-
Study Group and the ACCORD Eye Study Group. Effects of nopril on progression of retinopathy in normotensive people
medical therapies on retinopathy progression in type 2 dia- with type 1 diabetes. The EUCLID Study Group. EURO-
betes. N Engl J Med 2010;363(3):233–244. DIAB Controlled Trial of Lisinopril in Insulin-Dependent
6. Matthews DR, Stratton IM, Aldington SJ, Holman RR, Diabetes Mellitus. Lancet 1998;351(9095):28–31.
Kohner EM, for the UK Prospective Diabetes Study Group. 17. Raman R, Rani PK, Kulothungan V, et al. Influence of serum
Risks of progression of retinopathy and vision loss related to lipids on clinically significant versus nonoclinically signifi-
tight blood pressure control in type 2 diabetes mellitus: cant macular edema: SN-DREAMS Report number 13.
UKPDS 69. Arch Ophthalmol 2004;122(11):1631–1640. Ophthalmology 2010;117(4):766–772.
7. UK Prospective Diabetes Study Group. Tight blood pressure 18. Rema M, Srivastava BK, Anitha B, Deepa R, Mohan V. As-
control and risk of macrovascular and microvascular compli- sociation of serum lipids with diabetic retinopathy in urban
cations in type 2 diabetes: UKPDS 38. BMJ 1998;317(7160): South Indians–the Chennai Urban Rural Epidemiologi Study
703–713. (CURES) Eye Study-2. Diabet Med 2006;23(9):1029–1036.
8. Estachio RO, Jeffers BW, Gifford N, Schrier RW. Effect of 19. Klein BE, Moss SE, Klein R, Surawicz TS. The Wisconsin
blood pressure control on diabetic microvascular complica- Epidemiologic Study of Diabetic Retinopathy. XIII. Relation-
tions in patients with hypertension and type 2 diabetes. Dia- ship of serum cholesterol to retinopathy and hard exudate.
betes Care 2000;23(Suppl 2):B54–B64. Ophthalmology 1991;98(8):1261–1265.
9. Benarous R, Sasongko MB, Qureshi S, et al. Differential associ- 20. Keech AC, Mitchell P, Summanen PA, et al; FIELD study
ation of serum lipids with diabetic retinopathy and diabetic mac- investigators. Effect of fenofibrate on the need for laser treat-
ular edema. Invest Ophthalmol Vis Sci 2011;52(10):7464–7469. ment for diabetic retinopathy (FIELD study): a randomised
10. Henricsson M, Sellman A, Tyrberg M, Groop L. Progression controlled trial. Lancet 2007;370(9600):1687–1697.
to proliferative retinopathy and macular oedema requiring 21. Chew EY, Klein ML, Ferris FL, et al. Association of elevated
treatment. Assessment of the alternative classification of serum lipid levels with retinal hard exudate, in diabetic retinop-
the Wisconsin Study. Acta Ophthalmol Scand 1999;77(2): athy: Early Treatment Diabetic Retinopathy Study (ETDRS)
218–223. Report 22. Arch Ophthalmol 1996;114(9):1079–1084.
11. Klein R, Knudtson MS, Lee KE, Gangnon R, Klein BE. The 22. Wong TY, Simó R, Mitchell P. Fenofibrate – a potential sys-
Wisconsin Epidemiologic Study of Diabetic Retinopathy temic treatment for diabetic retinopathy? Am J Ophthalmol
XXIII. The twenty-five-year incidence of macular edema in 2012;154(1):6–12.
persons with type 1 diabetes. Ophthalmology 2009;116(3): 23. Liew G, Wang JJ, Mitchell P. Retinopathy progression in type
497–503. 2 diabetes. N Engl J Med 2010;363(22):2171–2172.
513.e1 AMERICAN JOURNAL OF OPHTHALMOLOGY MARCH 2014SUPPLEMENTAL FIGURE 1. Anti–vascular endothelial growth factor (anti-VEGF) treatment decision tree based on the treat- ment and retreatment schedule from A 12 Month Core Study to Assess the Efficacy and Safety of Ranibizumab Intravitreal Injections (RESTORE).10 Flow diagram showing anti-VEGF treatment for diabetic macular edema (DME) based on initial treatment with three consecutive monthly injections and whether stable visual acuity (VA) is achieved. VOL. 157, NO. 3 DIABETIC MACULAR EDEMA MANAGEMENT 513.e2
SUPPLEMENTAL FIGURE 2. Anti–vascular endothelial growth factor (anti-VEGF) treatment decision tree based on the Diabetic Retinopathy Clinical Research Network (DRCR.net) retreatment and follow-up schedule.53 Flow diagram showing anti-VEGF treat- ment for diabetic macular edema (DME) based on assessment 1 month after initial injections and whether DME improves. Reprinted from Ophthalmology, 118/12, Aiello LP, Beck RW, Bressler NM, et al., Rationale for the diabetic retinopathy clinical research network treatment protocol for center-involved diabetic macular edema, e5–14, Copyright (2011), with permission from Elsevier. 513.e3 AMERICAN JOURNAL OF OPHTHALMOLOGY MARCH 2014
VOL. 157, NO. 3
SUPPLEMENTAL TABLE 1. Overview of Selected Randomized Controlled Trials for Treatment in Diabetic Macular Edema
Mean 6 SD Mean 6 SD
Study (Where (Where Available) Proportion of Patients With BCVA Change (%) Licensed
Randomized Design Available) ETDRS Letter Indication for
Controlled and Treatment VA at Change From >
_10 Letters >
_10 Letters >
_15 Letters >
_15 Letters Ophthalmic
Treatment Trial (n) Duration Arms (n) Baseline Baseline Gained Lost Gained Lost Use
Anti-VEGF agents
RBZ RESOLVE Phase II, Study treatment: Yes
(151)17 12 months 0.3/0.6 mg RBZ (51) 60.2 6 9.9 RBZ pooled: RBZ pooled: 60.8 RBZ pooled: 4.9 RBZ pooled: 32.4 RBZ pooled: 2.9
0.5/1.0 mg RBZ (51) 7.8 6 7.7
Comparator:
Sham (49) 61.1 6 9.0 Sham: 0.1 6 9.8 Sham: 8.4 Sham: 24.5 Sham: 10.2 Sham: 20.4
READ-2 Phase II, Study treatment:
(126)18 24 months 0.5 mg RBZ (33) 24.85 0.5 mg RBZ: 7.7 0.5 mg RBZ: 43 N/A 0.5 mg RBZ: 25 N/A
DIABETIC MACULAR EDEMA MANAGEMENT
Comparator:
Laser (34) 23.83 Laser: 5.1 Laser: 23% Laser: 9
0.5 mg RBZ 24.84 0.5 mg RBZ 0.5 mg RBZ þ 0.5 mg þ laser: 7
þ laser (34) þ laser: 6.8 laser: 38
READ-2 Phase II, Study treatment:
(126)18 36 months 0.5 mg RBZ (28) N/A 0.5 mg RBZ: 10.3 0.5 mg RBZ: 46 N/A 0.5 mg RBZ: 32 N/A
Comparator:
Laser (22) Laser: 1.4 Laser: 23% Laser: 9
0.5 mg RBZ 0.5 mg RBZ 0.5 mg RBZ þ 0.5 mg RBZ þ laser:
þ laser (24) þ laser: 8.9 laser: 38 21
RESTORE Phase III, Study treatment:
(345)10 12 months 0.5 mg RBZ (116) 64.8 6 10.11 0.5 mg RBZ: 0.5 mg RBZ: 37.4 0.5 mg RBZ: 3.5 0.5 mg RBZ: 22.6 0.5 mg RBZ: 0.9
0.5 mg RBZ 63.4 6 9.99 6.1 6 6.43 0.5 mg RBZ þ laser: 0.5 mg RBZ þ 0.5 mg RBZ þ laser: 0.5 mg RBZ þ
þ laser (118) 0.5 mg RBZ þ 43.2 laser: 4.2 27.9 laser: 3.4
Comparator: laser: 5.9 6 7.92
Laser (111) 62.4 6 11.11 Laser: 0.8 6 8.56 Laser: 15.5 Laser: 12.7 Laser: 8.2 Laser: 8.2
DRCR.net Phase III, Study treatment:a At 12 months:
Protocol I 60 months 0.5 mg RBZ þ 63 6 12 0.5 mg RBZ þ 0.5 mg RBZ þ 0.5 mg RBZ þ 0.5 mg RBZ þ 0.5 mg RBZ þ
(854 eyes)11 prompt laser prompt laser: þ9 prompt laser: 30 prompt laser: 50 prompt laser: 4 prompt
(187 eyes) 6 11 laser: 2%
0.5 mg RBZ þ 0.5 mg RBZ þ 0.5 mg RBZ þ 0.5 mg RBZ þ 0.5 mg RBZ þ 0.5 mg RBZ þ
deferred laser (188 deferred laser: þ9 deferred laser: 28 deferred laser: 47 deferred laser: 3 deferred
eyes) 6 12 laser: 2
Comparator:
4 mg TA þ prompt 4 mg TA þ prompt 4 mg TA þ prompt 4 mg TA þ prompt 4 mg TA þ prompt 4 mg TA þ prompt
laser (186 eyes) laser: 4 6 13 laser: 21 laser: 33 laser: 14 laser: 8
513.e4
Continued on next pageYou can also read