Insufficienza cardiaca: Stato dell'arte, nuove raccomandazioni della Società Europea di Cardiologia (ESC) e trattamento dello stato ferriprivo ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Corso di formazione continua online
Insufficienza cardiaca: Stato dell’arte, nuove
raccomandazioni della Società Europea di
Cardiologia (ESC) e trattamento dello stato ferriprivo
Giovedì, 18 novembre 2021, 18:00 – 19:00
Giorgio Moschovitis, MD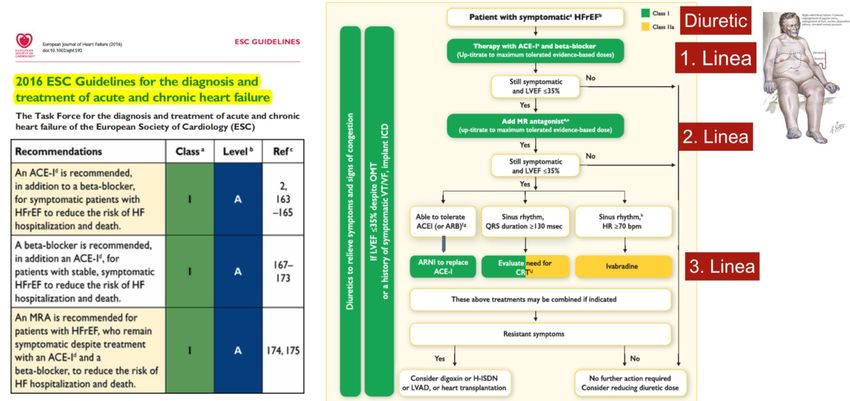
Disclosures partecipation to advisory boards and speaking fees Bayer, Vifor, Astra Zeneca, Böhringer Ingelheim, Daiichi Sankio, Novartis
Insufficienza cardiaca: Stato dell’arte, nuove
raccomandazioni della ESC e trattamento dello
stato ferriprivo
New ESC HF guidelines 2021
From ESC HF guidelines HF 2016
RAAS-inhibition is pillar: up-titration
Patiromer (VeltassaR)
One clinical case and few MC-Questions
Management of iron deficiency
FCM (FerinjectR)
Conclusions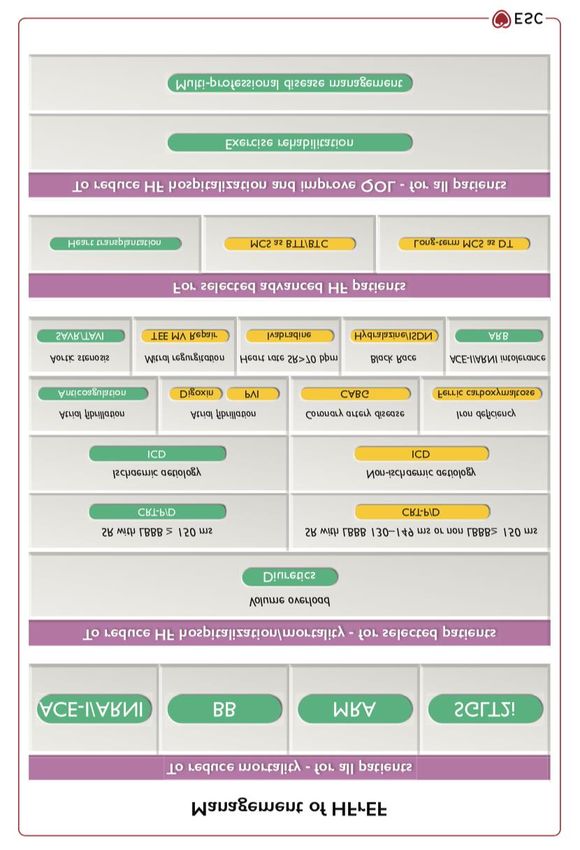
Clinical case presentation: Man born 1965 with HFrEF (56y) CAD, AMI anterior (7.2005), EF 25% PCI RIVA (7.2005), Stent-Thrombosis (9.2005) CABG (LIMA-RIVA 9.2005) PCI 1RMG (2.2007) Prophylactic ICD (3.2007) according to MADIT Perfusion scan /Scinti (5.2019): EF 22%, EDV 274 ml
Clinical case presentation: Man born 1965 with HFrEF: Medication (3.2017) Aspirin 100 mg 1— Xanax 1 mg 1-0-0 Triatec 5 mg 0.5---0.5 Sertralin 50 mg 0.5-0-0 Nebilet 5 mg 0.5---0.5 Abilify 5 mg 0.5-- Simvastatine 40 mg ---1 Ezetrol 10 mg 1--- (from 26.06.2017)
Insufficienza cardiaca: Stato dell’arte, nuove
raccomandazioni della ESC e trattamento dello
stato ferriprivo
New ESC HF guidelines 2021
From ESC HF guidelines HF 2016
RAAS-inhibition is pillar: up-titration
Patiromer (VeltassaR)
One clinical case and few MC questions
Management of iron deficiency
FCM (FerinjectR)
Conclusions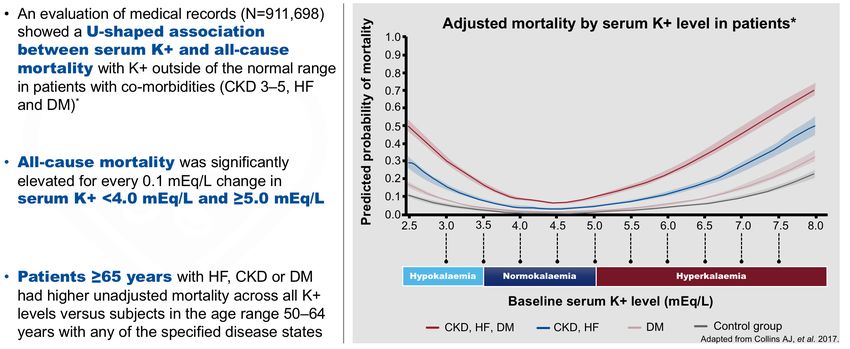
2016 ESC GL for the diagnosis and treatment of acute and chronic HF Ponikowski P. et al. Eur Heart J 2016
ESC HF GL 2021: Diagnostic algorithm for HF
X
McDonagh TA, et al. Eur Heart J 2021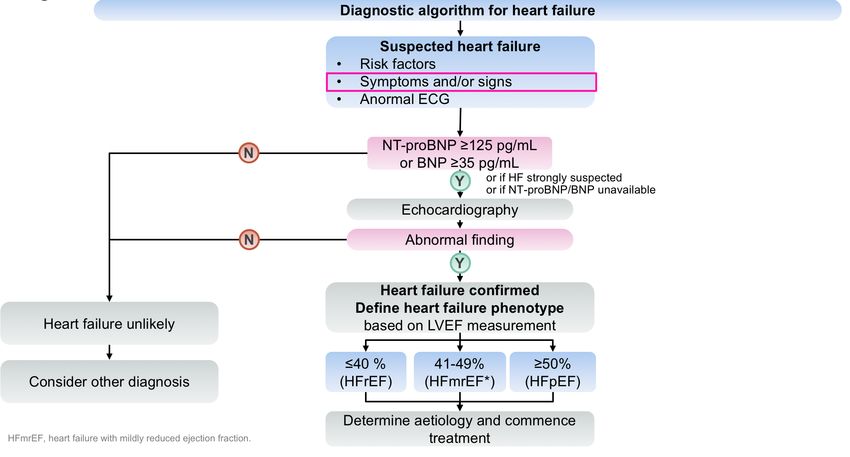
2021 ESC GL for the diagnosis and treatment
of acute and chronic HF
Linee Guida HF 2021 ESC
X
McDonagh TA, et al. Eur Heart J 2021BCT, bridge to candidacy; BTT, bridge to transplantation;
DT, destination therapy; ISDN, isosorbide dinitrate; LBBB,
left bundle branch block; MCS, mechanical circulatory
support; MV, mitral valve; PVI, pulmonary vein isolation;
SAVR, surgical aortic valve replacement; TAVI, transcatheter
aortic valve implantation; TEE, transcatheter edge to edge.
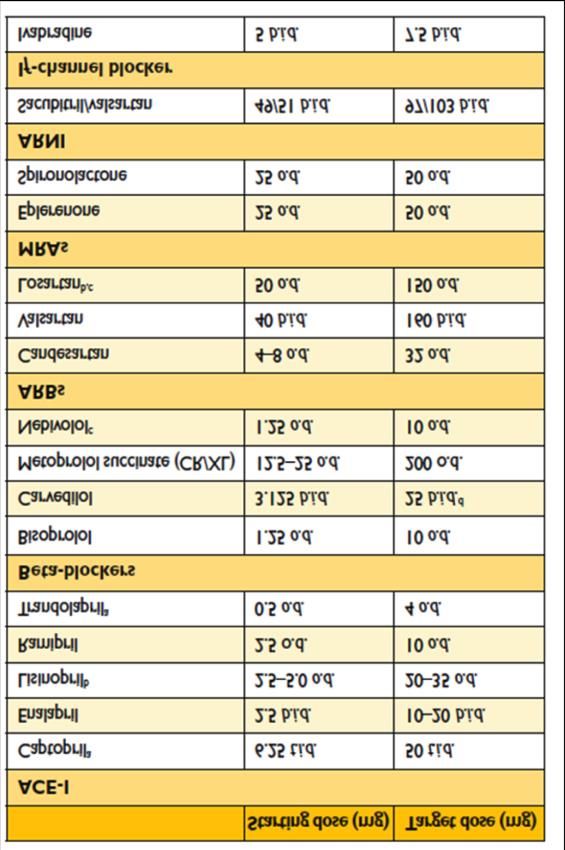
McDonagh TA, et al. Eur Heart J 20212021 ESC GL for the diagnosis and treatment
of acute and chronic HF:
Drugs recommended in all patients with HFrEF
McDonagh TA, et al. Eur Heart J 20212021 ESC GL for the diagnosis and treatment
of acute and chronic HF:
Drugs recommended in all patients with HFpEF
McDonagh TA, et al. Eur Heart J 2021Prevalence of HFpEF is increasing: in 2020,
HFpEF: prevalenza in aumento: nel 2020,
65% of65%all
deipatients with
pazienti ricoverati per AHF
HF, avrà have
FE >40% EF>40%
HFrEF or HFpEF
H FpEF H Fr EF
• Pr eser ved systolic LV function • Systolic LV dysfunction
• No LV dilation • LV dilation
• Concentr ic LV remodeling • Eccentr ic LV remodeling
• Diastolic LV dysfunction • Diastolic LV dysfunction
HFrEF, heart failure with reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; LV, left ventricular
Jessup M, Brozena S. N Engl J Med 2003;348:2007–2018
X
Ponikowski P. et al. Eur Heart J 2016EURObservational Research Programme
HF PILOT
n=4’600
Prognosis of HFrEF vs HFpEF
(1987-2001)
Mayo Clinic
N=4’600 (1987-2001)
Owan TE, NEJM (2006)The risk of adverse clinical events decreases
with time after AHF decompensation
Salomon et al. Circulation. 2007, 116-
16HF ESC GL 2021: New recommendations for pre-discharge and early post-discharge follow- up of patients hospitalized for acute HF McDonagh TA, et al. Eur Heart J 2021
2) MC: Le seguenti affermazioni sui pepidi
natriuretici sono corrette, ad accezione di:
A. BNP e NT-proBNP sono dei biomarker che
permettono una presa carico del paziente con
insufficienza cardiaca immediata e specifica, con un
rapporto costi/benefici favorevole.
B. Sono da correlare sempre con i sintomi e/o segni
clinici dell’insufficienza cardiaca.
C. Hanno un elevato valore predittivo negativo.
D. In caso di trattamento con ARNI (Entresto), si
consiglia di misurare piuttosto NT-proBNP.
E. I cut-offs per BNP e NT-proBNP non variano con
l’età, ma piuttosto secondo contesto clinico (acuto vs.
cronico).5. MC: Clinical case presentation: Man born 1965 with HFrEF – cont. ICD intervention (TV/FV) (12.2019), FE 35% ACS with PCI TC-RCX (01.2020), FE 24% 3° Hospitalizations for AHF (acute decompensated CHF) in October 2020 : NYHA III
Clinical case presentation: Man born 1965 with HFrEF – cont. Clinical exam: 55 y old, W 82 kg, H 165 cm, PA 112/80 mmHg, P 60 bpm, JV neg, HJR neg. No edema ECG baseline: atrial ICD-mediated rhythm, atypical LBB with QRS 137 ms NT-pro-BNP 410 ng/L (n < 386)
Clinical case presentation:
Man born 1965 with HFrEF – cont.
Aspirin 100 mg 1— Forxiga 5 mg 1– (from
Eliquis 5 mg 1—1 beginning of 2020)
Beloc ZOK 0.5—0.5 Ramipril def. paused
Aldactone 25mg ½-- (4.2018) =>
Ranexa 375 mg 1—1 Entresto 50 mg 1—1
(from 04.2018)
Inegy 10/40 mg ---1
Antidepressiv drugsInsufficienza cardiaca: Stato dell’arte, nuove
raccomandazioni della ESC e trattamento dello
stato ferriprivo
New ESC HF guidelines 2021
From ESC HF guidelines HF 2016
RAAS-inhibition is pillar: up-titration
Patiromer (VeltassaR)
One clinical case and few MC questions
Management of iron deficiency
FCM (FerinjectR)
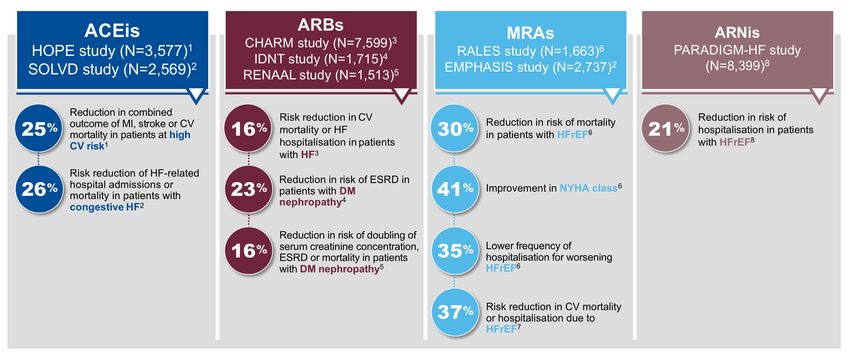
ConclusionsNumerous landmark studies have
demonstrated RAASI treatment benefits
1. Heart Outcomes Prevention Evaluation Study Investigators. Lancet. 2000;355:253–9; 5. Brenner BM, et al. N Engl J Med. 2001;345:861–9;
2. The SOLVD investigators. N Engl J Med. 1991;325:293–302; 6. Pitt B, et al. N Engl J Med. 1999;341:709–17;
3. Desai AS, et al. J Am Coll Cardiol. 2007;50:1959–66; 7. Zannad F, et al. N Engl J Med. 2011;364:11–21.
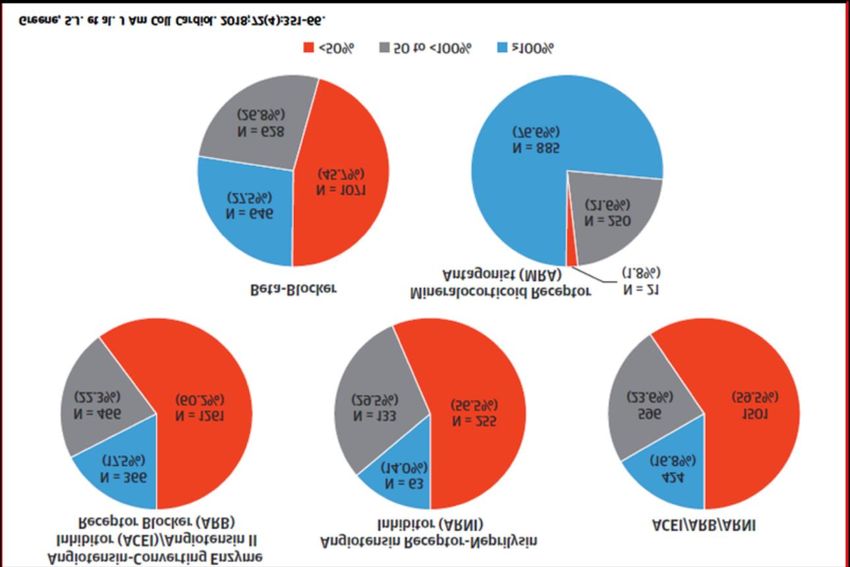
4. Lewis EJ, et al. N Engl J Med. 2001;345:851–60; 8. McMurray JJV, et al. N Engl J Med. 2014;371:993–1004.Subotpimal treatment: USA data (CHAMP-HF
register)
Trattamento subottimale: dati USA recenti (registro CHAMP-HF)
HFrEF, N=3518, Amb.
N=3518. HRrEF. Ambulatoriali Greene, JACC 2018
Greene S.J. et al. J Am Coll Cardiol. 2018, 724):351Subotpimal treatment: USA data (CHAMP-HF
register) Proporzione pazienti trattati con < 50%, 50-100, ≥ 100 dose farmaco
ESC 2016
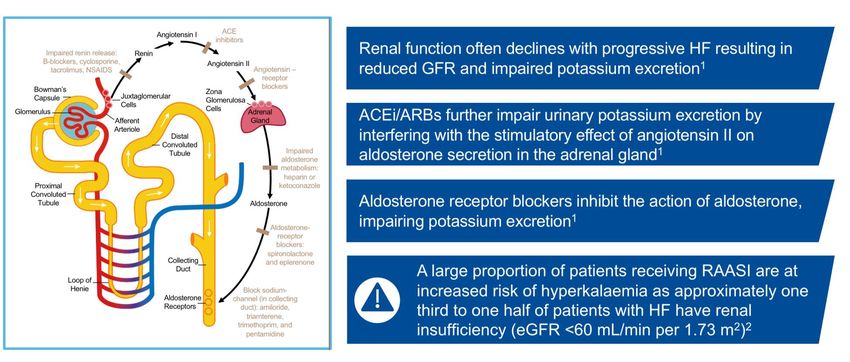
N=3518. HRrEF. AmbulatorialiRAASI use is associated with higher risk
of hyperkalaemia
* Hyperkalaemia defined as >6.0 mEq/L.
1. Tromp J, et al. Eur Heart J Suppl. 2019;21:A6–A11;
2. Desai AS. Curr Heart Failure Rep 2009;6:272–80;
3. Solomon SD, et al. N Engl J Med. 2019; 381:1609–20;
4. McMurray JJV, et al. N Engl J Med. 2014;371:993–1004.Mechanisms leading to hyperkalaemia
Hyperkalaemia is common in real-world patients with HF Savarese G, et al. JACC Heart Fail. 2019;7:65–76.
Potassium levels outside the normal range
are associated with higher risk of mortality
Shading surrounding lines indicates 95% confidence limits. * Evaluated through de-identified medical records (2007–2012) of individuals with ≥2
serum K+ readings (Humedica, Cambridge, MA). Spline analyses were performed to assess mortality at 0.1 mEq/L increments of serum K+ after
adjusting for covariates and interactions. Patiromer clinical trials were not designed to measure mortality outcomes.
Collins AJ, et al. Am J Nephrol. 2017;46:213–21.Sub-maximal dosing and discontinuation of
RAASI are associated with poor outcomes
Adverse outcomes = CKD progression and progression to end-stage renal disease, stroke
and acute MI, and CABG and PCI
Epstein M, et al. Am J Manag Care. 2015;21:212–20.BIOSTAT-CHF: Mortality increased in HF patients receiving
Treatment options for chronic hyperkalaemia come with significant limitations SPS = Sodium polystyrene sulfonate: is a non-absorbed cation-exchange resin, approved by the FDA in 1958. The recommended dose is 15-60 g given as a 15 g dose 1-4 times daily. CPS = Calcium polystyrene sulfonate 1. National Kidney Foundation. K/DOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease. Guideline 11. 2004. Available at: kidneyfoundation.cachefly.net/professionals/KDOQI/guidelines_bp/guide_11.htm (accessed July 2020); 2. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl 2013;3:S1–150; 3. National Kidney Foundation. The DASH Diet. Available at: kidney.org/atoz/content/Dash_Diet (accessed July 2020); 4. Carrero JJ, et al. Nat Rev Nephrol 2020;16:525–42; 5. Palmer BF, et al. Kidney360 2020:1;65–71; 6. Epstein M, et al. Am J Manag Care 2015;21:S212–20; 7. Linde C, et al. J Am Heart Assoc 2019;8:e012655; 8. Dunn JD, et al. Am J Manag Care 2015;21:S307–15; 9. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int Suppl 2020;98:S1–115; 10. Ter Maaten JM, et al. Clin Res Cardiol 2020;109:1048–59; 11. Kapelios CJ, et al. Eur J Heart Fail 2020; doi: 10.1002/ejhf.1796; 12. Ishikawa S, et al. PLoS One 2018;13:e0192990; 13. Kayexalate® US PI. Sanofi 2017; 14. Resonium Calcium PI. Sanofi 2018; 15. Noel JA, et al. JAMA Intern Med 2019;179:1025−33; 16. Laureati P, et al. Nephrol Dial Transplant 2020;35:1518–26.
Data from the European register HF Long Term
ESC HF LongTerm. 2016Recent ESC guidelines consider new solutions for the treatment of Hyperkalaemia in patients with HF receiving RAASi treatment: Patiromer *Based on radio-labelled drug-absorption studies. 1. Li L, et al. J Cardiovasc Pharmacol Ther. 2016;21:456–65; 2. Patiromer® EU SmPC, 2019.
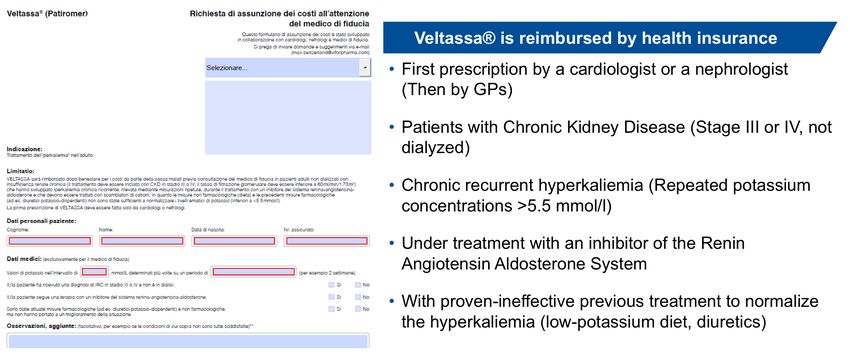
Veltassa® is reimbursed by health insurance
Fachinformation Veltassa, www.swissmedicinfo.ch
Veltassa® packaging is a dose of 8,4 or 16,8 g
One dose of Veltassa® must be mixed into 80 ml of water. Veltassa®
can also be mixed into apple juice or cranberry juice.
*Based on radio-labelled drug-absorption studies.
1. Li L, et al. J Cardiovasc Pharmacol Ther. 2016;21:456–65; 2. Patiromer® EU SmPC, 2019.Nearly half of patients in the patiromer clinical programme had HF 1. Veltassa® EU SmPC, 2020; 2. Bushinsky DA, et al. Clin J Am Soc Nephrol 2016;11:1769–76; 3. Bushinsky DA, et al. Kidney Int 2015;88:14–27; 4. Lesko LJ, et al. J Cardiovasc Pharmacol Ther 2017;22:434–46; 5. Bushinsky DA, et al. Am J Nephrol 2016;44:404–10; 6. Pitt B, et al. Eur Heart J 2011;32:820−8; 7. Buysse J, et al. Future Cardiol 2012;8:17–28; 8. Pitt B, et al. ESC Heart Fail 2018;5:257−66; 9. Bakris GL, et al. JAMA 2015;314:151–61; 10. Agarwal R, et al. Lancet 2019;394:1540–50; 11. ClinicalTrials.gov identifier: NCT03087058; 12. Weir MR, et al. N Engl J Med 2015;372:211–21; 13. ClinicalTrials.gov identifier: NCT03888066; 14. Pergola P, et al. Am J Nephrol 2017;46:323–32; 15. ClinicalTrials.gov identifier: NCT04443608.
PEARL-HF: In patients with HF, Patiromer significantly lowered serum K+ levels vs placebo Pitt B, et al. Eur Heart J 2011;32:820–8.
Patiromer enables RAASI treatment: preserving the potential of RAASI to improve clinical outcomes 1. Weir MR, et al. N Engl J Med. 2015;372:211–21; 2. Pitt B, et al. Eur Heart J. 2011;32:820–8. 3. Agarwal R, et al. Lancet. 2019;394:1540–50.
Patiromer: Safety and tolerability profile Patiromer EU SmPC, 2019.
ESC 2021 HF guideline considerations for the management of chronic hyperkalaemia McDonagh TA, et al. Eur Heart J 2021;ehab368. doi: 10.1093/eurheartj/ehab368.
Insufficienza cardiaca: Stato dell’arte, nuove
raccomandazioni della ESC e trattamento dello
stato ferriprivo
New ESC HF guidelines 2021
From ESC HF guidelines HF 2016
RAAS-inhibition is pillar: up-titration
Patiromer (VeltassaR)
One clinical case and few MC questions
Management of iron deficiency
FCM (FerinjectR)
ConclusionsGoals of pharmacotherapy when managing HFrEF patients McDonagh TA, et al; the ESC Scientific Document Group. Eur Heart J. 2021 Aug 27; doi: 10.1093/eurheartj/ehab368.
Iron deficiency is common in HF regardless of the presence of anaemia Adapted from Rocha BML, et al. J Am Coll Cardiol. 2018;71(7):782–793.
ID Reduces Exercise Capacity in HFrEF N=443 patients with stable HFrEF. HFrEF=heart failure with reduced ejection fraction; ID=iron deficiency. Jankowska EA, et al. J Cardiac Fail. 2011;17:899–906.
Pathophysiology, briefly
ID is a Stronger Prognostic Factor for Mortality This study population consists of patients from 5 cohorts from Poland, Spain and The Netherlands, comprising 1506 chronic HF patients with reduced or preserved left ventricular ejection fraction. CHF=chronic heart failure; CI=confidence interval; HR=hazard ratio; ID=iron deficiency. Klip IT, et al. Am Heart J. 2013;165:575–82.e3.
Patients with chronic HF and ID are at increased risk of mortality # Results of an analysis of a pooled cohort comprising 1484 patients with HF, LVEF< 40% recruited from 12/2010 to 10/2015 by 11 centres in Germany and Switzerland; * Results of the analysis of an international pooled cohort comprising 1,506 patients with chronic HF in Poland, Spain and the Netherlands; ID was defined as a ferritin level
New recommendations for anemia and iron
deficiency in patients with HF
XStudying the Effects of IV FCM on
Symptoms and Functional Health in HF
CHF=chronic heart failure; FAS=full analysis set; FCM=ferric carboxymaltose; HFrEF=heart failure with reduced ejection
fraction; IV=intravenous; NYHA=New York Heart Association; PGA=physician’s global assessment;
pVO2=peak oxygen consumption; 6MWT=6-minute walk test; SoC=standard of care.
1. Anker SD, et al. Eur J Heart Fail. 2009;11:1084–91;
2. Ponikowski P, et al. ESC Heart Fail. 2014;52–8;
3. van Veldhuisen DJ, et al. Circulation. 2017;136:1374–83.AFFIRM-AHF
A multicentre, randomised, double -blind, placebo-controlled trial
At 121 sites in Europe, South America, and Singapore
ClinicalTrials.gov identifier: NCT02937454
Between March 21, 2017, and July 30, 2019
1525 patients were screened, of whom 1132 patients were randomly
assigned to study groups: 558 in the carboxymaltose group and 550 in
the placebo group
Each subject is being followed for 52 weeksAFFIRM – AHF : study design
Age mean 71
Medication:
Female 44%
-MRA 67%
NYHA class III-IV 52%
-BB 81%
EF 32%
-RAAS-i 76%
Newly diagnosed HF 27-30%FCM significantly reduced the risk of HF
hospitalisations with no apparent effect on
the risk of CV death
*Total hospitalisations included first and recurrent events. If a patient was hospitalised for heart failure and died within 24 h of admission or if a
patient was hospitalised for a cardiovascular reason and died within 24 h of admission, this was counted as one event
AHF = acute heart failure; CI = confidence interval; CV = cardiovascular; FCM = ferric carboxymaltose; HF = heart failure; IV = intravenous; RRR =
relative risk reduction
Ponikowski P et al. The Lancet. 2020;396(10266):1895–1904Adverse Events of Interest
Ponikowski P, et al. The Lancet. 2020. https://doi.org/10.1016/S0140-6736(20)32339-44) MC: quali delle seguenti affermazioni è
corretta, ad eccezione di:
A. In AFFIRM-AHF la somministrazione di FCM nei pazienti con
stato ferriprivo, LV EF 20%.Clinical case presentation: Man born 1965 with HFrEF ICD intervention (TV/FV) (12.2019), FE 35% ACS with PCI TC-RCX (01.2020), FE 24% 3° Hospitalizations for AHF (acute decompensated CHF) in October 2020 : NYHA III
Clinical case presentation:
Man born 1965 with HFrEF
Aspirin 100 mg 1— Forxiga 5 mg 1– (from
Eliquis 5 mg 1—1 beginning of 2020)
Beloc ZOK 0.5—0.5 Ramipril def. paused
Aldactone 25mg ½-- (4.2018) =>
Ranexa 375 mg 1—1 Entresto 50 mg 1—1
(from 04.2018)
Inegy 10/40 mg ---1
Antidepressiv drugsClinical case presentation: Man born 1965 with HFrEF Clinical exam: 55 y old, W 82 kg, H 165 cm, PA 112/80 mmHg, P 60 bpm, JV neg, HJR neg. No edema ECG baseline: atrial ICD-mediated rhythm, atypical LBB with QRS 137 ms NT-pro-BNP 410 ng/L (n < 386)
5) MCQ: Clinical case: what do the new GL
suggest to consider to improve prognosis
A. Upgrade to CRT-D (=class 1 A) recommendation since he
has CAD, atypical LBBB and QRS < 150 ms
B. UpTitration of RAAS-i or Entresto (Sac/Vals)
C. Iron deficiency with/without anemia
D. The GL-recommended dose of SGLT2-inhibitor
(Dapagliflozin) is 10 mg 1x/day
E. HF Rehabilitation
F. Heart transplantationAnswer to 5. MCQ: Clinical case presentation:
Man born 1965 with HFrEF
Iron deficiency with/without anemia?
(28.06.2021): Hb 139 g/L (n: 140-180)
Ferritin 11 mcg/L (n 30-400), TSAT 15%
=> FCM 1’000 mg (GP)
(10.08.2021): Hb 149 g/L , Ferritin 516 mcg/LAnswer to 5. MCQ: Clinical case: to improve prognosis and symptoms, you may consider HF Rehabilitation: 29.10.2021- 25.05.2021 Initial : peak VO2 max 15.4 ml/min/kg (49%) Final : peak VO2 max 19.5 ml/min/kg (62%) => NO need for HTx June 2021: NYHA II NT-pro-BNP 324 mcg/L (13.09.2021)
Key messages Main novelties of the ESC 2021 GL HF RAAS inihitor therapy remains pillar in management of HF Implications and management of hyperkalaemia: Patiromer binds potassium in the colon and counter exchanges calcium: it’s well tolerated and effective Iron deficiency w/o anemia is very frequent in HF FCM in AHF patients with LVEF
Giorgio Moschovitis, MD
1) MCQ: Quale dei seguenti segni clinici e esami diagnostici non permette di valutare un quadro di congestione nel paziente con AHF? A. Turgore vene giugulari B. Pressione arteriosa sistolica C. Ecocardiografia D. X-ray torace E. Sonografia polmonare
1) MCQ risposte 1. A 2. B 3. B, C 4. D 5. D, E
2) MCQ: quali delle seguenti affermazioni sui
diuretici dell’ansa è corretta, ad eccezione di:
A. Diuretici dell’ansa aumentano il rischio di gotta, diabete e
sarcopenia (perdita della massa e funzione muscolare)
B. L’obiettivo della terapia diuretica é di ottenere uno stato di
euvolemia e di mantenerlo con la dose più piccola possible
C. La loro efficacia non dipende dalla funzione renale residua
D. L’uso di alti dosi di diuretici dell’ansa limita la titolazione
della terapia con ACEi/ARB nei pazienti con HF senza
tuttavia limitarne la prognosi
E. In pazienti normo- o ipo-volemici, il dosaggio dei diuretici
andrebbe ridotto o sospeso.2) MCQ risposte 1. A 2. AeC 3. C 4. D 5. CeD
4) MC: quali delle seguenti affermazioni è
corretta, ad eccezione di:
A. In AFFIRM-AHF la somministrazione di FCM nei pazienti con
stato ferriprivo, LV EF 20%.4) MCQ risposte 1. A 2. AeC 3. C 4. D 5. E
You can also read

















































