ICHIBAN, a non-interventional study evaluating tocilizumab long-term effectiveness and safety in patients with active rheumatoid arthritis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ICHIBAN, a non-interventional study evaluating tocilizumab
long-term effectiveness and safety in patients with active
rheumatoid arthritis
C. Specker1, A. Alberding2, M. Aringer3, G.-R. Burmester4, J.-P. Flacke5, M.W. Hofmann6,
P. Kästner7, H. Kellner8, F. Moosig9, M. Sieburg10, H.-P. Tony11, G. Fliedner12
1
Clinic of Rheumatology and Clinical Immunology, Evangelical Hospital, Clinic Essen-Mitte, Essen;
2
Internal Rheumatology, St. Josef Hospital, Wuppertal; 3 Department of Medicine III, University
Medical Center Carl Gustav Carus, TU Dresden; 4Department of Rheumatology and Clinical
Immunology Charité - Universitätsmedizin Berlin, Free University and Humboldt University Berlin;
5
Rheumatology, Roche Pharma AG, Grenzach-Wyhlen; 6Rheumatology, Chugai Pharma Germany
GmbH, Frankfurt am Main; 7MVZ Ambulant Rheumatology Center Erfurt; 8Rheumatology and
Gastroenterology Specialty Practice, Munich, Germany; 9Rheumatology Center Schleswig-Holstein
Middle, Neumünster; 10Allied Rheumatology Practice, Magdeburg; 11Medical Clinic II, Department
of Rheumatology and Clinical Immunology, University Clinic Würzburg;
12
Rheumatology Practice, Osnabrück, Germany.
Abstract
Objective
We aimed to measure long-term effectiveness and safety of tocilizumab in patients with rheumatoid arthritis in daily
German practice.
Methods
ICHIBAN was a prospective, multi-centre, non-interventional study (ML22928) that enrolled adult patients with active
moderate to severe rheumatoid arthritis. Patients were to be treated according to tocilizumab label and observed for up
to two years. Effectiveness outcomes included DAS28-ESR remission, EULAR response, CDAI and HAQ.
Results
Overall, 3164 patients received at least one dose of tocilizumab. Patient mean age was 55.5±13.1 years (74.8% female).
At baseline, 72.1% of patients had at least one comorbidity. Approximately 50.9% of patients received concomitant
csDMARDs, mostly methotrexate, and 80.7% received concomitant glucocorticoids (GCs). In patients receiving GCs at
baseline, the mean dose decreased from 9.32±16.36 mg/d to 4.60±4.48 mg/d at week 104. In the effectiveness population
with no prior TCZ (n=2902), 61.4% of patients achieved the primary outcome, DAS28-ESR remission. Improvements were
seen as early as week 4. At week 104, 77.9% of patients had DAS28-ESR low disease activity, 89.6% achieved good or
moderate EULAR response, and 29.5% achieved a CDAI-based remission. Effectiveness outcomes were similar in all
previous therapy subgroups. The incidence of serious infections was similar to the rates in former studies involving
tocilizumab. Patients receiving GC at baseline experienced slightly higher rates of treatment-related serious adverse
events, mainly infections. No new safety signals were observed.
Conclusion
Long-term effectiveness and safety in ICHIBAN were in line with previously reported tocilizumab efficacy and safety studies.
Key words
rheumatoid arthritis, interleukin-6, glucocorticoids, anti-rheumatic agents,
anti-rheumatic disease-modifying second-line drugs, tocilizumab
Clinical2020
Clinical and Experimental Rheumatology and Experimental Rheumatology 2021; 39: 319-328.Tocilizumab effectiveness in daily German practice / C. Specker et al.
Christof Specker, MD, PhD, Prof Introduction tients treated with TCZ for up to two
Annette Alberding, MD Rheumatoid arthritis (RA) is a chronic years, adding important long-term data
Martin Aringer, MD inflammatory disease that leads to pro- to previous observational datasets.
Gerd-Rüdiger Burmester, MD, Prof.
gressive joint destruction, pain, dis-
Jan-Paul Flacke, MD
Michael W. Hofmann comfort and decreased life expectancy, Patients and methods
Peter Kästner, MD, PhD and affects about 1% of the German Study design and patients
Herbert Kellner, MD, Prof. population (1). When patients respond The non-interventional, prospective
Frank Moosig, MD, Prof. inadequately to RA treatment with con- ICHIBAN study (NCT01194401) en-
Maren Sieburg ventional synthetic disease-modifying rolled adult patients with active mod-
Hans-Peter Tony, MD anti-rheumatic drugs (csDMARDs) and erate to severe RA from January 2010
Gerhard Fliedner, MD
have unfavourable prognostic mark- to January 2017 in both rheumatology
Please address correspondence to: ers, national and international guide- clinics and practices in Germany. Pa-
Christof Specker,
lines recommend adding biologic (b) tients were eligible for enrolment if the
Klinik für Rheumatologie
& Klinische Immunologie, DMARDS to treatment regimens (2, 3). decision to treat with TCZ (intravenous-
Evangelisches Krankenhaus, The disease mechanisms of RA are com- ly) according to the German Summary
Kliniken Essen-Mitte, plex and only partially known. Several of Product Characteristics (SmPC)
Pattbergstrasse 1-3, cytokines may play a role in sustain- was made prior to and independent of
45239 Essen, Germany. ing disease activity and inflammation. the decision to enrol the patient in the
E-mail: specker@uni-duesseldorf.de Cells in synovial tissue of patients with study. A maximum of one year of prior
Received on July 31, 2019; accepted in RA express the cytokine interleukin-6 TCZ treatment was also permitted. All
revised form on April 17, 2020. (IL-6) (4). Although the IL-6 receptor patients gave informed consent prior to
© Copyright Clinical and is only expressed by specific cell types, study enrolment.
Experimental Rheumatology 2021. trans-signalling enables IL-6 to target Effectiveness and safety data were
any cell of the body via soluble IL-6 collected in routine clinical practice.
receptors (5). Tocilizumab (TCZ) is a There was no intervention concern-
humanised, monoclonal antibody that ing therapeutic decisions or diagnostic
targets both membrane-bound and solu- procedures. All therapeutic and diag-
ble IL-6 receptors (6). Pivotal clinical nostic decisions, including concomitant
trials have shown that TCZ is an effica- medications, were made by the treating
cious treatment for RA with favourable physician. This study was reviewed and
safety and marked anti-inflammatory approved by the ethics committee at the
potency (7-12). In addition, TCZ treat- State Chamber of Physicians in North
ment slows the progression of joint Rhine (Germany) and registered at the
damage in patients with RA (13, 14). Paul-Ehrlich-Institute (ML22928).
TCZ is approved in the EU for the treat-
ment of adult patients with moderate Data collection and outcomes
to severe active RA who are intolerant All data were collected via an electron-
to or inadequately respond to previous ic case report form (eCRF). Study vis-
treatment with one or more DMARDs its were documented at baseline and at
or TNF-inhibitors (TNFi) (15), and can weeks 4, 12, 24, 36, 52, 64, 76, 88, and
be combined with methotrexate or given 104. Data collected at the initial visit in-
as monotherapy. cluded demographics and disease char-
In Germany, TCZ has been studied in acteristics, medical history including
real-life populations for 24 weeks (16) comorbidities, treatment history, and
and 52 weeks (17). The most recent concomitant treatment. At the initial vis-
analysis published on TCZ data from it and all follow-up visits, study centres
the RABBIT registry followed patients collected data on disease activity and
for up to three years (18). The objective details on RA medication. Effectiveness
of the present study, ICHIBAN, was to was assessed using the Disease Activity
measure long-term effectiveness and Score based on 28 joints and erythro-
Trial registration no.: ClinicalTrials.gov, safety of TCZ in patients with active RA cyte sedimentation rate (DAS28-ESR,
number NCT01194401; ML22928 in daily German practice. As TCZ treat- calculated according to (20)), European
Funding: this study was supported by ment has recently been examined for its League Against Rheumatism (EULAR)
Roche Pharma AG (Grenzach-Wyhlen, glucocorticoid (GC) saving effects (19), response (21), Clinical Disease Activ-
Germany) and Chugai Pharma Germany this aspect was addressed as well. The ity Index (CDAI), Boolean-based ACR/
GmbH (Frankfurt am Main, Germany). present large, prospective, multi-centre, EULAR remission (22), and measures
For competing interests, see page 327. non-interventional study followed pa- of physical functioning (Health Assess-
320 Clinical and Experimental Rheumatology 2021Tocilizumab effectiveness in daily German practice / C. Specker et al.
Table I. Baseline characteristics (SAF). Table II. Baseline characteristics by previous therapy subgroup (SAF).
Characteristic SAF Characteristic
Previous csDMARD Previous TNFi Previous non-TNFi
n=3164 (n=949) (n=2100) bDMARD
(n=87)
Age, years 55.5 ± 13.1
Sex, n (%) Age, years 57.7 ± 12.2 54.5 ± 13.4 55.6 ± 13.5
Female 2367 (74.8) Sex, n (%)
BMI, kg/m2 26.9 ± 5.3 Female 689 (72.6) 1593 (75.9) 65 (74.7)
Median duration of disease, 7 (3; 14) BMI, kg/m2 27.1 ± 5.0 26.7 ± 5.3 27.5 ± 7.6
years (Q1; Q3) Median duration of disease, years (Q1; Q3) 4 (2; 10) 9 (4; 15) 8 (4; 14)
Disease activity Disease activity
DAS28-ESR 5.01 ± 1.54 DAS28-ESR 4.78 ± 1.73 5.13 ± 1.43 4.70 ± 1.33
CDAI 26.45 ± 13.62 CDAI 24.56 ± 14.14 27.40 ± 13.36 24.15 ± 11.99
ESR (mm) 32.4 ± 25.3 Physical Functioning
CRP (mg/L) 28.74 ± 81.45 HAQ (%) 1.11 ± 0.71 1.34 ± 0.73 1.24 ± 0.76
Comorbidities, n (%)
Physical Functioning At least one 694 (73.1) 1509 (71.9) 63 (72.4)
HAQ (%) 1.27 ± 0.74 Hypertension 383 (40.4) 743 (35.4) 34 (39.1)
Anti-CCP status, n (%) Joint disorder or spinal disease 150 (15.8) 442 (21.0) 12 (13.8)
Positive 773 (24.4) Osteoporosis 149 (15.7) 376 (17.9) 14 (16.1)
Negative 165 (5.2) Diabetes 102 (10.7) 197 (9.4) 13 (14.9)
Unknown 2226 (70.4) Coronary heart disease 38 (4.0) 97 (4.6) 4 (4.6)
GC dose mg/d 6.48 ± 8.22 7.8 ± 17.0 7.16 ± 8.73
RF status, n (%)
Positive 937 (29.6) bDMARD: non-TNFi biological DMARDs; BMI: body mass index; CDAI: Clinical Disease Activity
Negative 263 (8.3) Index; CRP: C-reactive protein; csDMARD: conventional synthetic disease-modifying anti-rheumatic
Unknown 1964 (62.1) drugs; DAS28-ESR: Disease Activity Score based on 28 joints and erythrocyte sedimentation rate; GC:
Comorbidities, n (%) glucocorticoid; HAQ: Health Assessment Questionnaire; Q: Quartile; SAF: safety analysis set; TNFi:
At least one 2277 (72.1) tumour necrosis factor inhibitor.
Missing 6
Previous therapy, n (%)
least once during the study. Secondary patients without previous TCZ therapy.
csDMARDs only 949 (30.0) outcomes included time to DAS28-ESR Patients with previous TCZ therapy,
TNFi 2100 (66.4) remission, proportion of patients with patients changing from intravenous to
Non-TNFi bDMARDs 87 (2.7) good or moderate EULAR response as subcutaneous administration of TCZ,
Missing/Other 28 (0.9)
well as low disease activity, defined as and patients switching to a new RA
Concomitant csDMARD, n (%)
DAS28-ESR ≤3.2 or CDAI ≤10. treatment were analysed separately.
With 1604 (50.9)
Methotrexate, n (%) 1226 (38.7) Three subgroups were defined regard-
Leflunomide, n (%) 315 (10.0) Safety ing previous therapy: csDMARDs only
Without 1551 (49.1) Adverse events (AEs) were coded us- (all patients with previous csDMARDs
Missing 8
ing the Medical Dictionary for Regu- only), TNFi (all patients with previous
Concomitant GC, n (%) latory Activities (MedDRA), v. 13.0. TNF inhibitor therapy), and non-TNFi
With 2545 (80.7)
>0–5 mg/d 1331 (42.2)
Treatment-emergent AEs were used for bDMARD (all patients with previous
>5–10 mg/d 780 (24.7) safety analysis. AEs of special interest bDMARDs therapy excluding TNFi
>10 mg/d 434 (13.8) (AESI) were infections (opportunistic and TCZ). For concomitant treatment
Without 607 (19.3) and non-serious infections as defined at baseline subgroup analyses, patients
Missing 12
by treatment with IV anti-infectives), were grouped into monotherapy with
BMI: body mass index; CDAI: Clinical Dis- myocardial infarction/acute coronary TCZ or combination therapy with cs-
ease Activity Index; CRP: C-reactive protein; syndrome, gastrointestinal perforation DMARDs at baseline (including both
DAS28-ESR: Disease Activity Score based on and related events, malignant tumours, patients with or without GCs). In ad-
28 joints and erythrocyte sedimentation rate; GC:
glucocorticoid; HAQ: Health Assessment Ques- anaphylactic/hypersensitivity reactions, dition, four subgroups per baseline
tionnaire; Q: Quartile; SAF: safety analysis set; demyelinating diseases, stroke, bleed- treatment with csDMARDs and/or
TNFi: tumour necrosis factor inhibitor. ing and hepatic events. GC were defined: monotherapy+GC
(TCZ+GC), combination+GC
ment Questionnaire [HAQ]). Clinically Statistics (TCZ+csDMARD+GC), monotherapy-
relevant improvement or worsening in The safety analysis set (SAF) was com- GC (TCZ only), and combination-GC
HAQ score was defined as a decrease posed of all eligible patients enrolled in (TCZ+csDMARD).
or increase of ≥0.3 in HAQ score (23); the study who received at least one dose Descriptive statistics were used for all
functional HAQ remission was defined of TCZ, including patients with parameters. For time to reach DAS28-
as HAQTocilizumab effectiveness in daily German practice / C. Specker et al.
Table III. Baseline characteristics by concomitant therapy subgroup (SAF).
Characteristic Monotherapy Monotherapy Monotherapy Combination Combination Combination
± GC - GC + GC ± GC - GC + GC
(n=1551) n=316) (n=1235) (n=1605) (n=291) (n=1314)
Age, years 56.6 ± 13.6 53.3 ± 14.3 57.4 ± 13.3 54.4 ± 12.5 54.4 ± 12.8 54.4 ± 12.5
Sex, n (%)
Female 1218 (78.5) 263 (83.2) 955 (77.3) 1143 (71.2) 228 (78.4) 915 (69.6)
BMI, kg/m2 26.6 ± 5.4 26.4 ± 5.4 26.6 ± 5.4 27.1 ± 5.3 27.2 ± 5.2 27.1 ± 5.3
Median duration of disease, years (Q1; Q3) 8 (3; 15) 7 (3; 13) 8 (4; 15) 7 (3; 13) 7 (3; 12) 7 (3; 13)
Disease activity
DAS28-ESR 5.11 ± 1.47 4.73 ± 1.64 5.21 ± 1.41 4.91 ± 1.59 4.73 ± 1.59 4.95 ± 1.58
CDAI 26.91 ± 13.33 24.35 ± 13.16 27.53 ± 13.30 26.03 ± 13.89 24.62 ± 13.36 26.32 ± 13.98
Physical Functioning HAQ (%) 1.32 ± 0.75 1.16 ± 0.76 1.36 ± 0.74 1.22 ± 0.72 1.07 ± 0.69 1.25 ± 0.72
Comorbidities, n (%)
At least one 1157 (74.6) 215 (68.0) 942 (76.3) 1118 (69.7) 197 (67.7) 921 (70.1)
Hypertension 598 (38.6) 105 (33.2) 493 (40.0) 568 (35.4) 108 (37.1) 460 (35.0)
Joint disorder or spinal disease 308 (19.9) 35 (11.1) 273 (22.1) 297 (18.5) 51 (17.5) 246 (18.7)
Osteoporosis 285 (18.4) 32 (10.1) 253 (20.5) 256 (16.0) 23 (7.9) 233 (17.7)
Diabetes 171 (11.0) 37 (11.7) 134 (10.9) 143 (8.9) 24 (8.2) 119 (9.1)
Coronary heart disease 82 (5.3) 13 (4.1) 69 (5.6) 58 (3.6) 8 (2.7) 50 (3.8)
GC dose mg/d 7.34 ± 8.06 – 9.22 ± 8.02 7.42 ± 18.95 – 9.06 ± 20.59
BMI: body mass index; CDAI: Clinical Disease Activity Index; CRP: C-reactive protein; DAS28-ESR: Disease Activity Score based on 28 joints and eryth-
rocyte sedimentation rate; GC: glucocorticoid; HAQ: Health Assessment Questionnaire, Q: Quartile; SAF: safety analysis set.
ment/visit. Chi2 tests used to analyse TNFi had slightly higher baseline dis- effectiveness (21.3%) and intolerance
differences between subgroups for the ease activity (DAS28-ESR and CDAI) (6.3%). Twenty-eight patients (1.5%)
primary endpoint should be considered than those previously treated with cs- discontinued TCZ treatment because of
exploratory. Missing values were not DMARDs or non-TNFi bDMARDs remission. Unfortunately, 964 patients
substituted and the last observation only (Table II). The primary reason for (52.7%) were lost to follow-up.
carried forward (LOCF) method was change to TCZ was lack of effective- Among all concomitant therapy sub-
used for last visit (LV) data. Statistical ness of previous therapy (87.8%), as groups, the most common documented
analyses were performed using SAS® documented for 82% of the bDMARD- reason for premature study discontinua-
v. 9.4, (Cary, NC, USA). naïve patients and 91% of the patients tion was lack of effectiveness. Approxi-
with previous TNFi therapy. This was mately 13.0% of patients receiving csD-
Results followed by lack of tolerability of the MARDs at baseline discontinued due to
Patients and treatment previous therapy (22.2%). lack of effectiveness (11.7% of patients
Between January 2010 and January At baseline, approximately half of the pa- receiving no csDMARDs at baseline).
2017, 3404 patients were enrolled at tients received concomitant csDMARDs, These rates were similar regardless
255 rheumatology centres in Germany; mostly methotrexate, and four fifths were of the patient receiving methotrexate
3164 patients received at least one dose on concomitant GCs (Table I). Patients (MTX) or not at baseline (12.8% with
of TCZ (safety population, SAF). The with previous csDMARDs therapy only MTX; 12.0% without MTX)
mean age of patients was 55.5±13.1 received a lower mean baseline dose of Of the SAF, 2902 (91.7%) patients with
years, and about three-quarters of pa- GC (6.48±8.22 mg/d) than those with no previous TCZ were included in the
tients were female. At baseline, 72.1% previous TNFi (7.8±17.0 mg/d) or other EFF-NPT population. All effective-
of patients had at least one comorbidity, bDMARD-therapy (7.16±8.73 mg/d). ness analyses were performed on the
the most common being hypertension Patients receiving TCZ monotherapy EFF-NPT population only. The propor-
(37.0%), degenerative joint disorder/ with GC were older, had a longer dura- tions of patients with concomitant csD-
spinal disease (19.2%), osteoporosis tion of RA, higher disease activity, more MARDs and with concomitant GC de-
(17.2%) and diabetes (9.9%) (Table I). comorbidities and worse physical func- creased over time. At baseline, 50.6%
More than two thirds of the patients tioning than other subgroups (Table III). of patients were receiving csDMARDs
had previously been treated with TNFi The median duration of the observation- compared to 44.9% at week 104 (LV:
or other bDMARDs (Table I). Com- al period was 1.96 years, and 1307 pa- 46.3%). At baseline, 81.5% of patients
pared to these, the bDMARD-naïve tients remained in the study until week were receiving GC compared to 66.9%
subgroup, with previous csDMARD 104. at week 104 (LV: 74.4%). Mean GC dose
therapy only, was slightly older and Among 1830 patients with premature of patients with GC treatment at base-
had a shorter duration of disease (Ta- study discontinuation, the most com- line decreased from 9.32±16.36 mg/d
ble II). Patients previously treated with mon documented reasons were lack of to 4.60±4.48 mg/d at week 104 (LV:
322 Clinical and Experimental Rheumatology 2021Tocilizumab effectiveness in daily German practice / C. Specker et al.
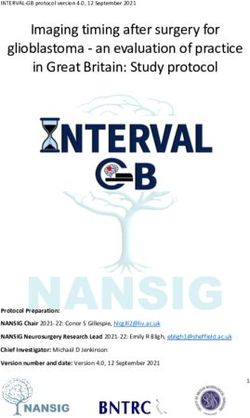
Fig. 1. DAS28-ESR and CDAI over time in the effectiveness population with no previous TCZ therapy (EFF-NPT).
A: DAS28-ESR categories and (B) mean score over time. C: CDAI categories and (D) mean score over time. Error bars represent standard deviation.
CDAI: Clinical Disease Activity Index; DAS28-ESR: Disease Activity Score based on 28 joints and erythrocyte sedimentation rate; effectiveness analysis
set – no previous TCZ treatment.
6.24±6.12 mg/d), with similar GC de- 29.5% and 17.5% of the patients, re- With TCZ therapy, proportions of pa-
creases in patients on TCZ+csDMARDs spectively, at week 104 (LV: 16.2 and tients achieving remission or low dis-
combination therapy (9.31±21.45 mg/d 10.4%, respectively). ease activity according to DAS28-ESR
at baseline to 4.46±4.08 mg/d at week Patients on TCZ treatment had rap- or CDAI over time were similar across
104) and patients on TCZ monother- idly improved physical functioning. At previous treatment subgroups (Fig. 2
apy (9.34±8.16 mg/d at baseline to week 4, 27.7% of patients experienced A-C). Patients in the previous csD-
4.78±4.92 mg/d at week 104). a clinically relevant improvement in MARDs-only subgroup had only slight-
HAQ score. HAQ improvement pla- ly higher mean changes from baseline in
Overall effectiveness of TCZ teaued between week 12 and 24 and was CDAI than patients with previous TNFi
Overall, 61.4% of patients in the EFF- sustained with only marginal changes at both early and late time points (LV:
NPT achieved the primary effective- throughout the observational period. -15.34±13.73 for csDMARDs vs.
ness outcome, DAS28-ESR remission By week 104, the proportion of patients -12.87±13.88 for TNFi, respectively).
documented at least once during the achieving a clinically relevant improve- There were no relevant differences in
treatment period, after a median time ment of HAQ had increased to 47.9% the proportions of patients achieving
of 148 days on TCZ treatment. Exclud- (LV: 34.1%) and 38.7% were in HAQ good or moderate EULAR response by
ing the 104 patients that were already remission (LV: 30.5%). Only 10.6% of week 104 or LV between the previous
in DAS28-ESR remission at baseline, patients experienced clinically relevant csDMARDs-only subgroup and pa-
the median duration to DAS28-ESR re- worsening (LV: 10.2%). tients with previous TNFi or non-TNFi
mission was 161 days (Suppl. Fig. S1). bDMARDs. Patients in the previous
TCZ treatment resulted in a quick re- TCZ effectiveness according to csDMARD-only subgroup had slightly
sponse, as reflected in the proportion of previous therapy greater gains in physical functioning at
patients achieving low disease activity The proportion of patients achieving early and late time points. The propor-
(DAS28-ESR ≤3.2) and the reduction DAS28-ESR remission was compa- tion of patients that had a clinically rel-
of mean DAS28-ESR already by weeks rable among subgroups per previous evant improvement of the HAQ score
4 and 12 (Fig. 1A-B). Similar improve- therapy, albeit slightly higher among at week 104 was 50.2% of patients with
ments were also seen in the propor- patients previously receiving csD- previous csDMARDs vs. 47.6% of pre-
tion of patients achieving CDAI low MARDs only (65.1%) compared to vious TNFi (LV: 38.3% vs. 32.8% re-
disease activity (≤10) within 12 weeks previous TNFi (60.3%) or non-TNFi spectively).
(Fig. 1C) and in the decrease of mean bDMARDs (56.5%; p-value for χ2 test:
CDAI (Fig. 1D). At week 104, 77.9% 0.0591) (Suppl. Table S1). Excluding TCZ effectiveness according to
of patients were in DAS28-ESR low patients in DAS28-ESR remission at concomitant therapy
disease activity (Fig. 1A) (LV: 57.6%) baseline, the median duration to reach According to an exploratory post-hoc
and 89.6% had achieved good or mod- DAS28-ESR for the first time was 105 analysis, the primary outcome was
erate EULAR response (LV: 74.9%). days in previous csDMARDs-only, 168 comparable between patients with
CDAI-based and Boolean-based ACR/ days in TNFi, and 93 days in non-TNFi and without concomitant GC therapy
EULAR remission were achieved for bDMARDs subgroups. at baseline. However, patients receiv-
Clinical and Experimental Rheumatology 2021 323Tocilizumab effectiveness in daily German practice / C. Specker et al.
for monotherapy-GC, and 114 days for
combination-GC groups.
Safety
Overall, 46.6% of 3164 patients in the
SAF experienced 4278 AEs over 3948
patient years (PY) of TCZ exposure
(Table IV). The most commonly docu-
mented AEs considered related to TCZ
treatment – infections and infestations
(9.5% of patients) – consisted largely
of nasopharyngitis (2.1% of patients)
and bronchitis (1.4% of patients). Oth-
er frequent AEs considered related to
TCZ treatment were gastrointestinal
disorders (3.7% of patients), skin and
subcutaneous tissue disorders (3.3%
of patients), and general disorders and
administration site conditions (3.2% of
TNFi
patients).
In patients with previous TNFi and
csDMARDs only, rates of treatment-
related SAEs were comparable with
5.5 and 5.6 events/100 PY, respectively.
However, more treatment-related SAEs
were seen in patients with previous non-
TNFi-bDMARDs (11.9 events/100 PY;
n=87). Patients receiving GCs at base-
line experienced higher rates of TCZ-
≤2.8
related SAEs than those receiving none
(6.4 events/100 PY vs. 3.0 events/100
PY, respectively) and serious infections
>2.8-10
(4.3 events/100 PY vs. 2.4 events/100
PY, respectively). Thirty-six patients
(1.1%) died during this study; 19 of
these deaths occurred while a patient
was receiving TCZ (0.5 events/100 PY)
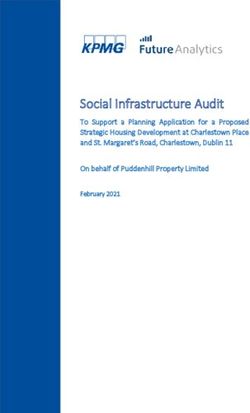
Fig. 2. DAS28-ESR categories, and EULAR response over time per previous therapy (EFF-NPT). (Suppl. Table. S2), and 11 of these pa-
A: DAS28-ESR categories and (B) proportion of patients to achieve DAS28-ESR low disease activity tients had SAEs considered to be related
(≤3.2) over time in subgroups per previous therapy. C: CDAI low disease activity over time in sub- to TCZ treatment. AESIs were reported
groups per previous therapy.
bDMARD: non-TNFi bDMARDs; csDMARD: only previous csDMARD therapy; DAS28-ESR: Dis-
in 422 patients (13.3%). The most com-
ease Activity Score based on 28 joints and erythrocyte sedimentation rate; EFF-NPT: effectiveness mon AESIs were infections requiring
analysis set – no previous TCZ treatment; TNFi: previous TNF inhibitor therapy. treatment with intravenous anti-infec-
tives (2.5 events/100 PY). Nine patients
ing concomitant csDMARDs at base- concomitant csDMARDs, both with (0.3%) experienced gastrointestinal
line had a significantly higher rate of and without GCs. Excluding patients in perforations (0.3 events/100 PY) (Ta-
reaching the primary outcome during DAS28-ESR remission at baseline, the ble IV), and three of these patients died
the study than those without (64.4% median duration to DAS28-ESR remis- (Suppl. Table S2).
with csDMARDS vs. 58.4% without) sion was 149 days for patients receiv-
(Suppl. Table SI). Mean changes in ing concomitant csDMARDs and 166 Discussion
DAS28-ESR from baseline, changes days for those without csDMARDs The present non-interventional study
in CDAI category (Fig. 3 A-D), pro- at baseline (Suppl. Fig. S1). Exclud- ICHIBAN evaluated the long-term ef-
portions of patients achieving good ing patients in DAS28-ESR remission fectiveness and safety of TCZ in pa-
or moderate EULAR response and at baseline, the median duration to tients with active RA in daily practice.
improvement in physical functioning DAS28-ESR remission was 169 days Baseline characteristics, such as age,
were similar in patients receiving TCZ for monotherapy+GC (TCZ+GC), 158 severity and disease duration were sim-
as monotherapy or in combination with days for combination+GC, 116 days ilar to recent observational studies with
324 Clinical and Experimental Rheumatology 2021Tocilizumab effectiveness in daily German practice / C. Specker et al.
reflected by the proportions of patients
achieving DAS28-ESR remission,
CDAI remission and clinically relevant
improvement in physical functioning.
Moreover, 61.2% patients achieved
DAS28-ESR remission at least once
during TCZ treatment. Considering the
relatively long disease duration of this
population, these remission rates un-
derscore the effectiveness of TCZ. TCZ
treatment also improved all other ef-
fectiveness outcomes (CDAI, DAS28-
ESR, Boolean EULAR remission),
with results comparable with other TCZ
real-world datasets (17, 26, 29).
Previous therapy subgroups
Patients with previous TNFi therapy
on average were younger, had longer
duration of disease and worse physical
function at baseline compared to the
subgroup of biological-naïve previous
csDMARD only patients. This obser-
vation corresponds with results from
studies based on the German RABBIT
registry (18) and British BSRBR-RA
study (25). Furthermore, the ICHIBAN
population also had a higher proportion
of biologic-naïve patients compared to
Scandinavian datasets (24, 26).
In ICHIBAN, 64.7% of patients with
previous csDMARDs therapy only
achieved the primary outcome com-
pared to 60.1% of the previous TNFi
subgroup, only a 4.6% difference, al-
though the previous TNFi group had a
5-year longer median duration of dis-
≤2.8 ease at baseline. This is consistent with
>2.8-10
other real-world studies that showed no
statistically significant differences in
TCZ effectiveness outcomes between
patients previously treated with other
bDMARDs (including TNFi therapy)
or csDMARDs only (17, 25). The pre-
sent data supports results from the Ger-
Fig. 3. DAS28-ESR, EULAR response, CDAI and mean GC dose over time per concomitant therapy
at baseline. man RABBIT registry that found TCZ
A: DAS28-ESR categories and (B) CDAI categories over time in subgroups per concomitant therapy to be similarly effective in biologics-
and GC use. C: DAS28-ESR categories and (D) CDAI categories over time in subgroups per concomi- naïve patients and those with three or
tant csDMARD therapy regardless of GC use.
more previous bDMARD failures (18)
CDAI: Clinical Disease Activity Index; Combi: TCZ + csDMARD combination therapy at baseline;
DAS28-ESR: Disease Activity Score based on 28 joints and erythrocyte sedimentation rate; EFF-NPT: and data from global the ACT UP pro-
effectiveness population with no prior TCZ treatment; EULAR: European League Against Rheuma- ject, which showed similar effective-
tism; GC: glucocorticoid; Mono: tocilizumab monotherapy at baseline. ness of TCZ among biologics-exposed
and naïve patients (30).
TCZ in Europe (17, 18, 24-27). Howev- German data from the international,
er, ICHIBAN had a relatively high pro- cross-sectional study, COMORA (28). Concomitant therapy and GC saving
portion of patients with hypertension or Results over up to 104 weeks showed In the present study, a six-percent-high-
diabetes, which is consistent with the that TCZ was effective in routine care as er proportion of patients treated with
Clinical and Experimental Rheumatology 2021 325Tocilizumab effectiveness in daily German practice / C. Specker et al.
Table IV. Summary of treatment emergent adverse events (SAF). with multiple comorbidities usually ex-
cluded from clinical trials.
Event, SAF (n=3164) Total events Patients, n (%) Rate per 100
patient years The incidence of anaphylaxis in
ICHIBAN (1.4/100 PY) was higher
AE 4278 1474 (46.6) 108.4 than that of integrated safety data from
AE considered related to treatment 1435 699 (22.1) 36.3 TCZ clinical trials (0.1/100 PY) (32).
SAE 943 472 (14.9) 23.9
Fatal 37 19 (0.6) 0.9
None of these events were fatal. The in-
SAE considered related to treatment 224 146 (4.6) 5.7 cidence of serious infections observed
AE leading to withdrawal 364 267 (8.4) 9.2 during ICHIBAN (3.9 events/100 PY)
Infections 1160 676 (21.4) 29.4 was similar to that of integrated safe-
SAE 153 113 (3.6) 3.9
ty data from TCZ clinical trials (4.7
AESI 718 422 (13.3) 18.2
Infection#, n (%) 98 82 (2.6) 2.5 events/100 PY) (32) and other real-
Medically significant hepatic event, n (%) 62 51 (1.6) 1.6 world studies such as REGATE (4.7
Anaphylaxis, n (%) 56 42 (1.3) 1.4 events/100 PY) (34) and ROUTINE
Myocardial infarction/Acute coronary syndrome, n (%) 28 23 (0.7) 0.7 (4.4 events/100 PY) (17). However, we
Serious or spontaneous bleeding, n (%) 17 13 (0.4) 0.4
Stroke 15 13 (0.4) 0.4 observed an incidence of myocardial
Gastrointestinal perforation and related events 10 9 (0.3) 0.3 infarction and acute coronary syndrome
Malignant neoplasms 8 8 (0.3) 0.2 in ICHIBAN, which, at 0.7 events/100
Demyelinating diseases 2 2 (0.1) 0.1 PY, was higher than reported in inte-
AE: adverse event; AESI: adverse event of special interest; SAE: serious adverse event; SAF: safety
grated safety data from TCZ clinical
analysis set. trials (0.25 events/100 PY) (32), as was
#
Infections including all opportunistic and non-serious infections as defined by treatment with IV anti- stroke (0.4 events/100 PY in ICHIBAN
infectives. vs. 0.19 events/100 PY in integrated tri-
als). These findings may reflect the car-
concomitant csDMARD at baseline ish (25), and pan-European (27) reg- diovascular risk profile of the German
achieved DAS28-ESR remission than istry studies. However, throughout real-world population: of 17 countries
those on TCZ monotherapy (64.4% vs. ICHIBAN, the percentage of patients in the COMORA study, patients with
58.4%). While monotherapy may have receiving GCs decreased from 80.6 RA in Germany had the third highest
resulted in an insufficient response in to 66.9%, and mean GC dose was re- prevalence of myocardial infarction
some patients, we believe that the deci- duced from 9.32 to 4.60 mg/d, in line and stroke (28). Furthermore, incidence
sion not to add a csDMARD was made with previous studies (18, 19). In the rates from 15,164 TCZ-naïve RA pa-
in a responsible way by the individual SPARE-1 study, 40% of the patients tients of the US-based MarketScan for
treating physicians. Not all patients treated with TCZ were able to achieve myocardial infarction (0.8 events/100
may tolerate csDMARDs, and there the GC-saving target dose of ≤5 mg/d PY) and stroke (0.51 events/100 PY)
was indeed a further reduction of pa- (19). Furthermore, in an analysis of the were similar to those seen in ICHIBAN
tients receiving csDMARDs throughout German RABBIT cohort, numbers of (35). The rate of gastrointestinal per-
the study (50.7% baseline vs. 46.3% patients receiving GCs decreased under forations was not increased by the in-
LV). Furthermore, similar to other TCZ and so did the numbers of patients clusion of real-life populations. Inci-
real-world studies (17, 18, 25, 27), receiving high doses of GCs (18). In dence of gastrointestinal perforations
concomitant therapy subgroups had the SEMIRA study, a randomised clini- in ICHIBAN (0.3 events/100 PY) cor-
similar mean changes in DAS28-ESR cal trial (NCT02573012), GC discon- responded with integrated safety data
from baseline, proportions of patients tinuation could be achieved in patients from TCZ clinical trials (0.28/100 PY)
achieving good or moderate EULAR treated with TCZ without an increased (32) and German RABBIT registry
response, changes in CDAI category risk of flares (31). studies (0.27/100 PY) (36).
and improvements in physical func- The incidence of malignancies in
tioning. Due to the natural limitations Safety ICHIBAN (0.2/100 PY) was lower
of a non-interventional study, such Overall, the rate of AEs in ICHIBAN than integrated safety data from TCZ
as the lack of randomization of sub- was lower than that of integrated safety clinical trials (1.1/100 PY) (32) or a
groups, patients receiving monothera- data from randomised controlled TCZ Swedish register-based cohort study
py at baseline were on average slightly clinical trials (32) or cumulative analy- (0.96/100 PY).(37), possibly due to un-
older, had a longer duration of disease, sis of controlled clinical trials and ex- derreporting.
more comorbidities and higher disease tension phases (33); however, the rate
activity. Thus, effectiveness results of SAEs in ICHIBAN was higher. The Limitations
should be interpreted with caution. lower incidence of AEs may be caused Several limitations are inherent within
ICHIBAN had a higher proportion of by underreporting, while the higher in- non-interventional studies, such as the
patients on concomitant GCs at base- cidence of SAEs may reflect the inclu- possibility of selection bias. Given the
line compared to Danish (26), Brit- sion of higher risk patients and patients nature of non-interventional studies,
326 Clinical and Experimental Rheumatology 2021Tocilizumab effectiveness in daily German practice / C. Specker et al.
there was no control arm or randomisa- Competing interests 3. SINGH JA, SAAG KG, BRIDGES SL JR et al.:
2015 American College of Rheumatology
tion, meaning that physician or patient C. Specker has received honoraria for
Guideline for the Treatment of Rheumatoid
perception of effectiveness could bias consulting from AbbVie, Boehringer Arthritis. Arthritis Rheumatol 2016; 68: 1-26.
the results. Furthermore, due to the re- Ingelheim, Chugai, Lilly, Novartis, 4. STEINER G, TOHIDAST-AKRAD M, WITZ-
al-world nature of physician treatment Sobi and UCB; speakers’ bureau from MANN G et al.: Cytokine production by syno-
vial T cells in rheumatoid arthritis. Rheuma-
decisions, there may have been a risk of AbbVie, Celgene, Chugai, Janssen- tology (Oxford) 1999; 38: 202-13.
underreporting of safety data and a pos- Cilag, Lilly, MSD, Novartis, Pfizer, 5. SCHETT G: Physiological effects of modu-
sible exclusion of patients that had ad- Roche and UCB; and grant/research/ lating the interleukin-6 axis. Rheumatology
verse events during TCZ exposure prior study support from Boehringer, Chugai, (Oxford) 2018; 57 (Suppl. 2): ii43-ii50.
6. AVCI AB, FEIST E, BURMESTER GR: Target-
to this study. Moreover, a total of 104 GSK and Roche. ing IL-6 or IL-6 Receptor in Rheumatoid
patients (of 2902 in the EFF-NPT) had A. Alberding has received support for Arthritis: What’s the Difference? BioDrugs
already achieved baseline DAS28-ESR this study from Roche and Chugai that 2018; 32: 531-46.
remission, when given the first dose of went directly to her employer. 7. SMOLEN JS, BEAULIEU A, RUBBERT-ROTH A
et al.: Effect of interleukin-6 receptor inhibi-
TCZ. Another limitation of ICHIBAN M. Aringer has received consulting fees tion with tocilizumab in patients with rheu-
was the missing data for RF- and anti- (or other payment) from Roche and matoid arthritis (OPTION study): a double-
CCP-status at baseline. Importantly, Chugai; speakers’ bureau from Roche blind, placebo-controlled, randomised trial.
Lancet 2008; 371: 987-97.
documentation was incomplete for 964 and Chugai; and grant/research/study 8. YAZICI Y, CURTIS JR, INCE A et al.: Efficacy
patients, leading to a 58.7% proportion support from Roche. of tocilizumab in patients with moderate to
of patients prematurely ending the study. G.-R. Burmester has received consult- severe active rheumatoid arthritis and a pre-
To address this, LOCF analyses were ing fees from Lilly, Pfizer, Sanofi and vious inadequate response to disease-modi-
fying antirheumatic drugs: the ROSE study.
conducted for all endpoints, and Kaplan- Roche; and grant/research/study sup- Ann Rheum Dis 2012; 71: 198-205.
Meier analyses were conducted for the port from Roche. 9. JONES G, SEBBA A, GU J et al.: Comparison of
primary endpoint. The proportion of pa- J.-P. Flacke is an employee of Roche tocilizumab monotherapy versus methotrex-
tients prematurely ending the study was Pharma AG. ate monotherapy in patients with moderate to
severe rheumatoid arthritis: the AMBITION
higher than in comparable real-world M.W. Hofmann is an employee of Chu- study. Ann Rheum Dis 2010; 69: 88-96.
studies that had discontinuation rates of gai Pharma Germany GmbH. 10. GENOVESE MC, MCKAY JD, NASONOV EL
only about 35% (17, 24, 26). This may P. Kästner has received grant/research/ et al.: Interleukin-6 receptor inhibition with
in part be related to the larger size and study support from Roche. tocilizumab reduces disease activity in rheu-
matoid arthritis with inadequate response to
longer duration than other observational H. Kellner has received consulting fees disease-modifying antirheumatic drugs: the
studies, and may also be related to alter- from Roche and has received grant/re- tocilizumab in combination with traditional
ations in the monitoring due to a change search/study support from Roche. disease-modifying antirheumatic drug thera-
py study. Arthritis Rheum 2008; 58: 2968-80.
in the clinical research organization dur- F. Moosig has received grant/research/
11. EMERY P, KEYSTONE E, TONY HP et al.: IL-6
ing the ongoing study. study support from Roche. receptor inhibition with tocilizumab improves
In summary, this prospective, multi- M. Sieburg has received grant/research/ treatment outcomes in patients with rheuma-
centre, non-interventional study showed study support from Roche. toid arthritis refractory to anti-tumour necro-
sis factor biologicals: results from a 24-week
rapid and long-term effectiveness and H.-P. Tony has received consulting fees multicentre randomised placebo-controlled
safety of TCZ in daily practice in Ger- from Roche, Abbvie, BMS, Chugai, trial. Ann Rheum Dis 2008; 67: 1516-23.
many and adds data supporting the GC Janssen, Novartis, Sanofi and Lilly; 12. BURMESTER GR, RUBBERT-ROTH A, CANTA-
saving potential of TCZ. Tolerability has received speakers‘ bureau from GREL A et al.: A randomised, double-blind,
parallel-group study of the safety and ef-
was similar to other real-world data and Roche, Abbvie, BMS, Chugai, Jans- ficacy of subcutaneous tocilizumab versus
no new safety signals were observed. Ef- sen, Novartis, Sanofi and Lilly; and has intravenous tocilizumab in combination with
fectiveness was similar to other observa- received grant/research/study support traditional disease-modifying antirheumatic
tional studies and thus supports the use from Roche. drugs in patients with moderate to severe
rheumatoid arthritis (SUMMACTA study).
of TCZ both after bDMARD failure and G. Fliedner has received grant/research/ Ann Rheum Dis 2014; 73: 69-74.
in biologic-naïve patients. Effectiveness study support from Roche. 13. NISHIMOTO N, HASHIMOTO J, MIYASAKA N
of TCZ was not markedly influenced by et al.: Study of active controlled monotherapy
concomitant csDMARDs (e.g. metho- used for rheumatoid arthritis, an IL-6 inhibi-
References tor (SAMURAI): evidence of clinical and ra-
trexate), in line with previous literature 1. HENSE S, LUQUE RAMOS A, CALLHOFF J, diographic benefit from an x ray reader-blind-
on TCZ monotherapy in RA. ALBRECHT K, ZINK A, HOFFMANN F: [Prev- ed randomised controlled trial of tocilizumab.
alence of rheumatoid arthritis in Germany Ann Rheum Dis 2007; 66: 1162-7.
based on health insurance data: Regional dif- 14. FLEISCHMANN RM, HALLAND AM, BRZOS-
Acknowledgements ferences and first results of the PROCLAIR KO M et al.: Tocilizumab inhibits structural
We thank the patients, their families study]. Z Rheumatol 2016; 75: 819-27. joint damage and improves physical function
and all of the centres that participated 2. SMOLEN JS, LANDEWE R, BIJLSMA J et al.: in patients with rheumatoid arthritis and in-
in ICHIBAN. Writing support was EULAR recommendations for the manage- adequate responses to methotrexate: LITHE
ment of rheumatoid arthritis with synthetic study 2-year results. J Rheumatol 2013; 40:
provided by Physicians World Europe and biological disease-modifying antirheu- 113-26.
GmbH (Mannheim, Germany), sup- matic drugs: 2016 update. Ann Rheum Dis 15. RoActemra® SmPC.
ported by Roche Pharma AG. 2017; 76: 960-77. 16. BURMESTER GR, FEIST E, KELLNER H,
Clinical and Experimental Rheumatology 2021 327Tocilizumab effectiveness in daily German practice / C. Specker et al.
BRAUN J, IKING-KONERT C, RUBBERT-ROTH 23. KREMER JM, BLANCO R, BRZOSKO M et al.: 30. HARAOUI B, CASADO G, CZIRJAK L et al.:
A: Effectiveness and safety of the interleukin Tocilizumab inhibits structural joint dam- Tocilizumab patterns of use, effectiveness,
6-receptor antagonist tocilizumab after 4 and age in rheumatoid arthritis patients with in- and safety in patients with rheumatoid arthri-
24 weeks in patients with active rheumatoid adequate responses to methotrexate: results tis: final results from a set of multi-national
arthritis: the first phase IIIb real-life study from the double-blind treatment phase of a non-interventional studies. Rheumatol Ther
(TAMARA). Ann Rheum Dis 2011; 70: 755-9. randomized placebo-controlled trial of toci- 2019; 6: 231-43.
17. IKING-KONERT C, VON HINUBER U, RICH- lizumab safety and prevention of structural 31. BURMESTER G, BUTTGEREIT F, BERNASCO-
TER C et al.: ROUTINE-a prospective, mul- joint damage at one year. Arthritis Rheum NI C et al.: A randomized controlled 24-week
ticentre, non-interventional, observational 2011; 63: 609-21. trial evaluating the safety and efficacy of
study to evaluate the safety and effectiveness 24. FORSBLAD-D’ELIA H, BENGTSSON K, KRIS- blinded tapering versus continuation of long-
of intravenous tocilizumab for the treatment TENSEN LE, JACOBSSON LT: Drug adher- term prednisone (5 mg/day) in patients with
of active rheumatoid arthritis in daily prac- ence, response and predictors thereof for rheumatoid arthritis who achieved low dis-
tice in Germany. Rheumatology (Oxford) tocilizumab in patients with rheumatoid ease activity or remission on tocilizumab [ab-
2016; 55: 624-35. arthritis: results from the Swedish biologics stract]. Arthritis Rheumatol 2018; 70 (Suppl
18. BAGANZ L, RICHTER A, KEKOW J et al.: register. Rheumatology (Oxford) 2015; 54: 10).
Long-term effectiveness of tocilizumab in pa- 1186-93. 32. SCHIFF MH, KREMER JM, JAHREIS A, VER-
tients with rheumatoid arthritis, stratified by 25. KIHARA M, DAVIES R, KEARSLEY-FLEET L NON E, ISAACS JD, VAN VOLLENHOVEN RF:
number of previous treatment failures with bi- et al.: Use and effectiveness of tocilizumab Integrated safety in tocilizumab clinical tri-
ologic agents: results from the German RAB- among patients with rheumatoid arthritis: an als. Arthritis Res Ther 2011; 13: R141.
BIT cohort. Rheumatol Int 2018; 38: 579-87. observational study from the British Soci- 33. GENOVESE MC, RUBBERT-ROTH A, SMOLEN
19. SARAUX A, ROUANET S, FLIPO RM et al.: ety for Rheumatology Biologics Register for JS et al.: Longterm safety and efficacy of to-
Glucocorticoid-sparing in patients suffering rheumatoid arthritis. Clin Rheumatol 2017; cilizumab in patients with rheumatoid arthri-
from rheumatoid arthritis and treated with 36: 241-50. tis: a cumulative analysis of up to 4.6 years
tocilizumab: the SPARE-1 study. Clin Exp 26. LEFFERS HC, OSTERGAARD M, GLINTBORG of exposure. J Rheumatol 2013; 40: 768-80.
Rheumatol 2016; 34: 303-10. B et al.: Efficacy of abatacept and tocili- 34. MOREL J, CONSTANTIN A, BARON G et al.:
20. PREVOO ML, van‘t HOF MA, KUPER HH, van zumab in patients with rheumatoid arthritis Risk factors of serious infections in patients
LEEUWEN MA, van de PUTTE LB, van RIEL treated in clinical practice: results from the with rheumatoid arthritis treated with toci-
PL: Modified disease activity scores that nationwide Danish DANBIO registry. Ann lizumab in the French Registry REGATE.
include twenty-eight-joint counts. Develop- Rheum Dis 2011; 70: 1216-22. Rheumatology (Oxford) 2017; 56: 1746-54.
ment and validation in a prospective longi- 27. GABAY C, RIEK M, HETLAND ML et al.: 35. GALE S, TRINH H, TUCKWELL K et al.:
tudinal study of patients with rheumatoid Effectiveness of tocilizumab with and with- Adverse events in giant cell arteritis and
arthritis. Arthritis Rheum 1995; 38: 44-8. out synthetic disease-modifying antirheu- rheumatoid arthritis patient populations:
21. van GESTEL AM, PREVOO ML, van ‘t HOF matic drugs in rheumatoid arthritis: results analyses of tocilizumab clinical trials and
MA, van RIJSWIJK MH, van de PUTTE LB, from a European collaborative study. Ann claims data. Rheumatol Ther 2019; 6: 77-88.
van RIEL PL: Development and validation of Rheum Dis 2016; 75: 1336-42. 36. STRANGFELD A, RICHTER A, SIEGMUND B
the European League Against Rheumatism 28. DOUGADOS M, SOUBRIER M, ANTUNEZ A et et al.: Risk for lower intestinal perforations
response criteria for rheumatoid arthritis. al.: Prevalence of comorbidities in rheuma- in patients with rheumatoid arthritis treated
Comparison with the preliminary American toid arthritis and evaluation of their monitor- with tocilizumab in comparison to treatment
College of Rheumatology and the World ing: results of an international, cross-section- with other biologic or conventional synthetic
Health Organization/International League al study (COMORA). Ann Rheum Dis 2014; DMARDs. Ann Rheum Dis 2017; 76: 504-10.
Against Rheumatism Criteria. Arthritis 73: 62-8. 37. WADSTROM H, FRISELL T, ASKLING J;
Rheum 1996; 39: 34-40. 29. IKING-KONERT C, ARINGER M, WOLLEN- Anti-Rheumatic Therapy In Sweden (ARTIS)
22. FELSON DT, SMOLEN JS, WELLS G et al.: HAUPT J et al.: Performance of the new 2011 Study Group: Malignant neoplasms in pa-
American College of Rheumatology/Euro- ACR/EULAR remission criteria with tocili- tients with rheumatoid arthritis treated with
pean League against Rheumatism provisional zumab using the phase IIIb study TAMARA tumor necrosis factor inhibitors, tocilizumab,
definition of remission in rheumatoid arthritis as an example and their comparison with tra- abatacept, or rituximab in clinical practice:
for clinical trials. Ann Rheum Dis 2011; 70: ditional remission criteria. Ann Rheum Dis a nationwide cohort study from Sweden.
404-13. 2011; 70: 1986-90. JAMA Intern Med 2017; 177: 1605-12.
328 Clinical and Experimental Rheumatology 2021You can also read