Evaluating sexual health planning for the London 2012 Olympics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Journal of Public Health Advance Access published August 30, 2014
Journal of Public Health | pp. 1– 9 | doi:10.1093/pubmed/fdu064
Evaluating sexual health planning for the London 2012
Olympics
Ava Lorenc, Nicola Robinson
Faculty of Health and Social Care, London South Bank University, London SE1 0AA, UK
Address correspondence to Ava Lorenc, E-mail: lorenca@lsbu.ac.uk
A B S T R AC T
Background The public health impact of mass gatherings should not be underestimated, requiring careful planning. This evaluation identified the
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
successes and failures of a programme targeted to mitigate against potential increases in sexual ill health during the London 2012 Olympics.
Methods Programme planning was evaluated using documentary analysis. Stakeholders’ experiences were explored using an online survey.
Finally, selected stakeholders were interviewed in depth.
Results Over 100 documents were analysed, 36 survey responses received and 12 interviews conducted. Most respondents felt aims were
appropriate, potentially overambitious. ‘Business as usual’, with no disruption or increased demand, was reported in sexual health services. Some
interviewees felt evidence for increased demand was limited, although contingency planning was needed. Signposting service users and
providing ‘residual risk responses’ appeared successful. Planned service transformation was not fully achieved and perhaps inappropriate,
although new service collaborations emerged. Over 2000 individuals participated; wider public engagement was seen as inappropriate. A ‘Sex
Factor 2012’ competition was particularly successful. Legacy opportunities included planning work, groundwork for transformation, relationship
building and continuing the resilience changes.
Conclusions The Games allowed sexual health services to explore new ways of working, engage with stakeholders and develop new
relationships, although in reality demand for services did not increase.
Keywords health promotion, health services, Olympic Games; mass gatherings; sexual health
Introduction detected during the Atlanta 1996 Games.6 A literature review
to inform the London Olympic Games (unpublished) con-
Large-scale mass gatherings such as the Olympic Games
cluded that ‘increase in sexual health services in an Olympic
present significant health challenges to the host country, in-
Games host city is necessary. Adequate provision of STIs
cluding public health issues and increased risk of illness and
awareness and prevention and the provision of sufficient
injury such as respiratory and diarrhoeal diseases and sexually
sexual health services are vital prior to, during and post
transmitted infections (STIs).1
Games’ (S. Dakshina, unpublished results). A review to
However, published data on health service planning for
inform public health planning for the London Games recom-
events such as the Olympics is limited.2 The impact on
mended condom distribution and preventative literature for
sexual health is also unclear (S. Dakshina, unpublished
visitors on avoiding STIs.7
results), being difficult to study STIs in the context of mass
In addition to planning for the impact of events on public
gatherings or to attribute any changes.3 One study following
health, mass gatherings such as the Olympic Games have
the Sydney 2000 Games demonstrated an increase in use of
sexual health services and of bacterial STIs, and a surge in
demand for sex workers during Games time.4 Another study
of the 2010 Winter Olympics suggested adopting evidence- Ava Lorenc, Research Fellow
based public health strategies in relation to sex work.5 Nicola Robinson, Professor of Traditional Chinese Medicine (TCM) and Integrated
However, although anticipated, there was no increase in STIs Health
# The Author 2014. Published by Oxford University Press on behalf of Faculty of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com. 12 J O U R NA L O F P U B L IC H E A LT H
huge potential for health promotion of the population as a sexual health in previous Olympic and Paralympic games.
whole, including safe sex.8 Interventions might include provi- Information was extracted to quantify the process, including
sion of condoms, educational programmes and campaigns to the number and frequency of meetings convened, type of
raise awareness,3 for example the safe sex campaign at the e-mails sent/required, etc.
Atlanta 1996 Games.6 Phase 2 was a survey of all key stakeholders, including
For the London 2012 Olympic Games, sexual health was those directly and indirectly involved with MBARC. A ques-
prioritized by the Government in public health planning. tionnaire was designed for the project using the Survey
London Sexual health Programme (LSHP) commissioned a Monkey software. In October 2012, the survey was sent as a
private company, MBARC Ltd, to deliver the London 2012 hyperlink in an explanatory email to 195 individuals identified
Games Sexual Health Planning and Legacy Programme (here- by the documentary analysis, MBARC staff and LSHP lists.
after referred to as ‘the programme’). Activities within this They represented key stakeholders, including:
programme were conducted by a range of stakeholders, sup-
† 2012 data group
ported and co-ordinated by MBARC. The programme was
† Members of the original sexual health promotion group
set up to understand the impact of London 2012 Games on
† Sexual health commissioning network
sexual health, to mitigate against increased sexual ill health
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
† Special health authority sexual health leads
and contribute to a positive sexual health legacy. It had three
† ‘Sex Factor’ Ideas 2012 winners
themes: ‘Resilience’ (‘business as usual’, safeguarding services,
† MBARC sexual health ambassadors
minimizing cost and call on the UK’s National Health Service
† 2012 Games sexual health management group
(NHS)), ‘Transformation’ (using resilience development to
† Organizers of sexual health Showcase events
transform services and relationships for lasting benefit) and
† Judging panel for ‘Sex Factor Ideas 2012’ competition
‘Engagement’ (maximizing public participation and raising
† MBARC staff
awareness).
† LSHP staff.
The overall 2012 public health work was funded by the
Department of Health; NHS London (NHSL) and the LSHP The survey questionnaire was designed based on Phase 1
set all the deliverables. The programme commenced in results and focussed on methods and success of methods of
2008 – 09; MBARC were funded from 2010 to 2011. engagement with stakeholders and whether objectives were
This paper reports an independent evaluation of MBARC’s achieved. Results were analysed using descriptive and bivariate
work on this project, including relevance and achievement of statistics and content analysis where appropriate.
aims (resilience, transformation and engagement), govern- Phase 3 used qualitative interviews with key informants
ance, challenges, need for sexual health planning and legacy selected from those completing the survey or suggested by
of the programme. NHS London/LSHP to ensure representation from a range
of stakeholder groups and experiences. Participants were
invited via email and provided with a copy of the participant
Methods
information sheet. Interviews were held either over the
The overall aim of the project was to evaluate MBARC’s de- phone, at their place of work or at London South Bank
livery and co-ordination of the public health interventions University (LSBU). A consent form was signed. Interviews
and support for sexual health service planning to plan for and were digitally recorded and transcribed.
mitigate against increased sexual ill health at the London 2012 All interviewees were assigned a code; no other identifiers
Games. were used on study materials. All materials were kept in a
The evaluation used a mixed-methods study design and locked filing cabinet at LSBU or on a password-protected
consisted of three separate phases, roughly sequential. The computer file.
evaluation was commissioned in August 2012 and completed We did not anticipate any sensitive issues would be dis-
in January 2013. cussed; however, participants were free to withdraw from the
Phase 1 used a documentary analysis to describe the study at any time for any reason.
process. Documents were provided by MBARC, LSHP and Ethical approval was given by London South Bank
NHSL and included minutes of contract meetings; heads University Research Ethics Committee in October 2012, ref-
of agreement documents; quarterly reports; management erence UREC 1268.
reports; planned activities with stakeholders; Dakshina’s lit- Quantitative analysis used frequency tables and bivariate
erature review (S. Dakshina, unpublished results); evaluation statistics. Qualitative data were analysed using content analysis
forms from events and a brief background of the literature on to identify key themes. Quotes were anonymized.S E X UA L H EA LT H P L A N NI N G FO R T H E LO N DO N 2 0 1 2 O LY M P I CS 3
The key issues to be explored in the analysis included: local stakeholder and distributing condoms. Ten respondents
were responsible for engaging or representing others.
† Success of stakeholder engagement
Most were involved in attending meetings and taking part
† Were deliverables achieved
in or helping to run an event or programme (Table 2).
† Skills set/qualifications required by personnel to carry out
The majority of the 24 answering the question felt able to
such a programme (over a short time scale)
contribute (5 very much so; 13 to some extent). Five felt that
† Details of the resources required (time, money etc) and
they were ‘not really’ or ‘not at all’ able to.
whether resources used were appropriate (especially
financially).
† Recommendations and key learning on the above to Governance and communications
inform future planning of mass events which could be Governance was originally managed by four groups (sexual
used worldwide health promotion, data surveillance, sexual health services
† The themes ‘Resilience’, ‘Transformation’ and ‘Engagement’. and people who sell sex). As the programme moved towards
delivery (as MBARC became involved), this structure was
reorganized by NHSL. Various governance methods were
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
Results used, including a project management group, a ‘Fresh
Thinking Group’, a manager at MBARC, LSHP and sexual
Participants health commissioners reviewing progress reports. Records
Over 100 individual documents were analysed. Invitations were kept of all meetings, and of achievement of deliverables,
and one reminder to participate in the survey were sent to 195 risks and contingencies. The only concern about governance
individuals. Thirty-six responses were received, an 18% re-
sponse rate. Twenty individuals were invited to participate in Table 2 Participants’ role in the programme
interviews, 10 from the survey and 10 suggested by NHSL/
LSHP/ MBARC. They were selected to represent a range of Number of % of respondents
organizations and experiences. A total of 12 agreed. responsesa (n ¼ 26b)
Nineteen (53%) of survey participants were currently
working in the NHS—nine in management, six in commis- Member of the sexual health 9 34.6
sioning and four clinical (data were unavailable for four) commissioners group
Involved in running ‘Sex Factor 7 26.9
(Table 1). Involvement in the programme varied, including
Ideas’
attending meetings, mentoring young people, local dissemin-
Member of 2012 Olympics sexual 4 15.4
ation, contributing to materials, management board member,
health management group
Participant in ‘Sex Factor Ideas’/ 4 15.4
Table 1 Participants supporting participant
Involved in running sexual health 3 11.5
Job categorya Survey respondent number Interviewee showcases
number Staff member at NHS London 3 11.5
Working in NHS to implement the 4 15.4
NHS clinical 07, 17, 27, 33, 34 programme
NHS managerial 03, 11, 12, 13, 14, 15, 19, 22, Member of the HIV and sexual 3 11.5
28, 29, 31 health commissioners group
NHS 02, 04, 05, 11, 16, 35, 36 01, 06, 08, 10, England
commissioning 11 NHS sexual health or public 3 11.5
Public health 18, 24 02, 07, 09, 12 health lead
Voluntary sector/ 37 Participant in sexual health 2 7.7
NGO showcases
Local authority 20 Staff member at LSHP 1 3.8
Government 28 Sexual health ambassador with 1 3.8
Education sector 08, 21, 25 MBARC
Studying 05, 09, 26, 27 Sponsor 1 3.8
Private sector 06, 10, 32
a
Respondents could tick all that applied.
a b
Respondents could tick more than one category. 10 missing responses.4 J O U R NA L O F P U B L IC H E A LT H
was a loss of leadership prior to appointment of a programme [it may have been better to] concentrate on achieving less
manager. Also, interviewees felt that accountability was initial- but better [Interviewee 08]
ly blurred.
The key methods of communication with stakeholders I think [they were] pretty ambitious aims. . . But no, I think
were as follows: those were the right ones [Interviewee 09].
† Communications strategy linked to NHSL Communications Interviewees’ opinions conflicted as to the appropriateness of
Team, which aimed to signpost and provide key messages to having a separate sexual health programme to other health
the public issues. Most (apart from NHSL, LSHP and MBARC) felt that
† Reporting from MBARC to LSHP/NHSL it could have been within existing public health plans and
† Flyers, ‘Sex Factor Ideas 2012’ competition blog, Twitter, messaging.
Facebook, posters and press releases for ‘Sex Factor’
[we] should have focussed on [our work] being part of a
† Direct contact with young people at sexual health show-
broader area which wouldn’t have exceptionalised sexual
cases and ‘Sex Factor’ events, as well as peer interviewers,
health, it would have put sexual health back into the idea of
online blog, posters and newspaper adverts.
health [Interviewee 08]
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
† Monthly E-newsletters sent to over 700 people
† NHS Choices website I suppose, why sexual health and why not harm reduction
† Briefing papers for the LSHP Board which reported to per se, or why not drug prevention, what was, why chose
London specialized commissioning group. sexual health and isolate that? That would be my question
[Interviewee 09]
Overall aims, focus and achievement
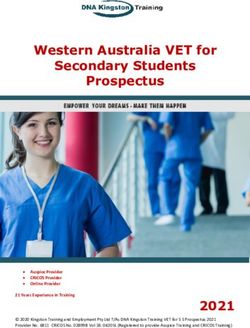
More survey participants felt the planning aims were achieved I’m really pleased that we, London, were able to prioritise
than the legacy aims (Fig. 1). Some people felt the aims were sexual health in the way we have, and I think there will be
only partly achieved, attributed to external influences, lack of lots of lessons [from it] [Interviewee 10]
buy-in and limited resources. Some felt the aims changed Three interviewees felt sexual health messaging during the
during the programme to ensure delivery. Games was inappropriate, opportunistic and attention grab-
The majority of survey respondents (22/36; 61%) thought bing, and likely to be lost in other messages/advertising.
the programme focus was appropriate. A minority felt it was
not appropriate (5/36); reasons included a lack of increased you’ve got everybody in public health with their own little
service use, overambitious ideas and unclear focus from the baby wanting to use it as an opportunity for smoking or
outset. Three interviewees felt the aims were overambitious, for sexual health and it would have been just too many
especially given the budget. mixed messages [Interviewee 06].
12
12.5
10
10.0
8
Count
Count
7.5
6
5.0
4
2.5 2
0.0 0
Yes, very Yes to Not sure No not No not Yes, very Yes to Not sure No not No not
much so some extent really at all much so some extent really at all
Do you think sexual health planning for the London 2012 games was achieved? Do you think a lasting legacy for health was achieved?
Fig. 1 Survey responses regarding achievement of aims.S E X UA L H EA LT H P L A N NI N G FO R T H E LO N DO N 2 0 1 2 O LY M P I CS 5
Resilience: achieved but was it necessary? we did a lot of signposting to pharmacies, to GP practices
The programme aimed to achieve resilience by safeguarding and to other sexual health services not so close to the
sexual health services during the Games, ensuring lower cost Games site. . .we were able to direct people away from the
interventions and minimizing the call upon NHS resources. It main sexual health services so we know that can be done
used planning templates and a communications strategy (cir- [Interviewee 12]
culated to sexual health commissioning and 2012 regional
The most popular signposting methods (from 21 (58%)
leads), public health messaging (including signposting users
survey respondents) were NHS Choices 2012 webpages (par-
away from GUM (Genito Urinary Medicine) and condom dis-
ticularly NHS managers and clinicians), ‘Summer Lovin’ cam-
tribution (500 000 ‘Capital City Condoms 2012’ condoms
paign materials (also particularly NHS managers and clinicians),
were distributed). Resilience was discussed extensively by
sexual health legacy e-news (all sectors) and stakeholder
interviewees.
presentations (all sectors).
The evidence base for planning for an increase in demand
The strategy stated that MBARC would distribute 440 000
for services was seen as perhaps being limited and anecdotal.
condoms; the October 2012 newsletter says that 500 000 were
Participants unanimously recognized that there was no in-
distributed.
crease in demand for services, perhaps even a decrease, attrib-
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
MBARC set up a daily assurance reporting template for a
uted to Londoners leaving London due to ‘marketing’ by
sexual assault referral centre (SARC) covering the Olympic
Transport for London (the ‘Sherman’ effect). However, most
boroughs, a last-minute provision. The SARC did experience
respondents felt it was ‘better to be safe than sorry’ rather
increased referrals during the Games. Respondents felt that
than risk ‘a PR disaster’ [Interviewee 02].
this initiative was very successful, providing routes for escal-
Generally London was a lot quieter during the Games, ation for any problems, ensuring the SARC could stay open.
which showed on the health services, it didn’t have a major
impact [Interviewee 06] Health promotion: some success
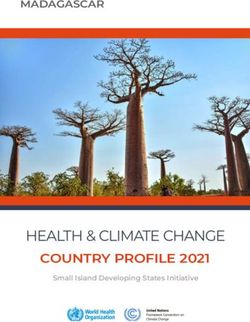
Most survey respondents felt health promotion aims were
Respondents felt supported and prepared and that resilience achieved to some extent (Fig. 2). ‘London Organising
was achieved, with additional capacity and ‘business as usual’ Committee of the Olympic and Paralympic Games’ (LOCOG)
and no evidence of disruption. Only one interviewee (07) felt commissioned a private sector provider to deliver the health
that resilience planning was not right. promotion messaging campaign and condom distribution, but
Signposting was most commonly reported as successful, this was withdrawn at short notice. Programme managers were
fewer felt the communications strategy was useful, especially unaware of the problem until it was too late, although MBARC
NHS managers. The FAQs and statements for press especial- and the Terrence Higgins Trust (THT) were praised by inter-
ly lifted spirits and prevented bad news stories about local viewees for putting together a campaign at the last minute.
sexual health. The planning template was least useful. Health promotion was perceived as having limited impact and
12 12
10 10
8
8
Frequency
Frequency
6
6
4
4
2
2
0
Yes, very Yes to Not sure No not No not 0
much so some extent really at all Yes, very Yes to Not sure No not No not
much so some extent really at all
Do you think the Programme raised awareness of personal responsibility
and positive behavioural changes to ensure good sexual health? Do you think the Programme improved sexual health promotion?
Fig. 2 Survey responses regarding achievement of health promotion aims.6 J O U R NA L O F P U B L IC H E A LT H
visibility and being scaled down from what was planned due to Transformation successes were providing groundwork for
avoiding negative association of STIs, limited funding and the future changes, and services’ successful resilience planning,
private sector provider issue. It was felt to be too generic, and considering how to be more evidence based and cost-
which NHSL explained was necessary and ‘it was more about effective:
making sure people knew how and when to access which
I think some of the transformation stuff was around ser-
health services if they needed them. . .facilitating people to act
vices knowing how flexible they can be. You don’t often
responsibly’ [Interviewee 06].
get forced to be flexible. . .So I think yes, it was transform-
The most successful health promotion was the ‘Sex Factor
ation in that services flexed their flexibility [Interviewee 09]
Ideas 2012’ competition. Ten/13 survey respondents (77%)
found the ‘Summer Lovin’ health promotion materials useful, [signposting is] something we ought to be doing all the
particularly NHS managers and clinicians. time, but the Games was sort of like a catalyst for us to
really look where our services are in terms of access to
If you raised awareness of a dozen young people I suppose
them, and if people can’t access them what alternatives do
that in itself is better than nothing [Interviewee 01]
we have in place [Interviewee 12].
Survey participants identified problems distributing the cam-
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
paign materials to the public and not reaching the right client
group. Engagement: successful
Estimates from documentation suggest that nearly 2000
Transformation: limited success people were engaged in the programme, plus many more
The programme aimed to transform services and relation- from the health promotion campaign. This included young
ships through resilience planning, a pharmacy self-testing people (450 people), NHS providers (280 people) and com-
pilot, signposting and the ‘Sex Factor Ideas 2012’ competi- missioners (80 people), voluntary and community organiza-
tion. However, the timetable appears to have been overambi- tions including British Pregnancy Advice Service (BPAS),
tious, not allowing sufficient time for required approvals. Brook, THT (around 20 people). Minimal (around 10 or less)
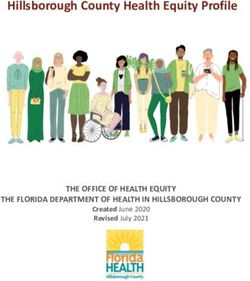
Data suggest that transformation was the least successful aim people were engaged from people who sell sex, NHS
(Fig. 3). The pathway pharmacy pilots were not implemented. London, LSCG, LSHP, local/national government, health
protection, educational sector and commercial sector.
the idea around. . .self-testing out into the community Key engagement methods were events, activities and
would have helped to deliver some of the QIPP [Quality presentations, collaborating on material design, meetings,
Innovation Productivity and Prevention] agenda, but as it e-newsletters and the NHS Choices website.
was it wasn’t actually realised [Interviewee 06] Interviewees seemed unclear what ‘public’ engagement
One interviewee [07] felt that London 2012 Games was the meant and whether it was appropriate.
wrong time to try out new technologies and pathways due to I’m not sure about public engagement. . .if you break that
existing disruption to services. down does that mean campaigns for the public, and if so,
which members of the public, is it at-risk groups or is it
10
more generic groups? I think that probably the aim should
have been around good stakeholder engagement which
8
includes public engagement and I think there was good
stakeholder engagement [Interviewee 09].
Frequency
6
Interviewees felt that a range of professionals were engaged,
4
in particular service providers and the third sector:
‘I think they tried very hard to reach out to sexual health
2 services’ [Interviewee 01]
I really did see some fantastic voluntary sector collabora-
0
Yes, very Yes to Not sure No not No not tions. I would say that was good legacy [Interviewee 09]
much so some extent really at all
Do you think the Programme transformed services and Professionals felt to be less well engaged included commis-
relationships between partners and stakeholders for lasting benefit sioners, senior leadership decision-makers and perhaps the
in line with QIPP?
Fig. 3 Survey response regarding achievement of transformation. wider public health community.S E X UA L H EA LT H P L A N NI N G FO R T H E LO N DO N 2 0 1 2 O LY M P I CS 7
There was a unanimous view that MBARC were ‘great’ and to be a challenge to get buy-in, ownership, involvement and
‘really good’ at engaging young people. ‘Sex Factor Ideas participation from the necessary stakeholders – when
2012’ competition may provide a model for engagement funding did materialise (it took time) there was insufficient
in the future rolled out and localized as a ‘toolkit for local time to build/re-build the necessary coalition to take the
engagement’. work forward [Survey 16].
Other challenges from progress reports included problems
Legacy: some potential but unclear with technology, e.g. NHS staff accessing YouTube for ‘Sex
Survey participants were split 50/50% regarding the pro- Factor 2012’; lack of prioritization of Games time provision
gramme’s legacy. Some felt it was too early to conclude. Some by commissioners and worsening financial climate impacting
felt legacy was limited due to NHS reorganization and lack of sponsorship.
a clear plan and commitment from the NHS. Potential legacy
opportunities were: the planning work that was done; trans-
formation ideas; relationship building and continuing the Discussion
changes implemented in the resilience work. The transform- Main findings of this study
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
ation models ( pharmacy pilots, self-testing, condom distribu-
Results suggest that the aims of the programme were
tion and ‘Sex Factor’) provide groundwork and potential
correct, although perhaps overambitious given the resources
legacy if taken forward.
available, in particular transformation aims. They appeared
some softer stuff around relationships which is worth only to be achieved in part due to ‘over-promise’ and exter-
recording as part of the legacy. I think it brought providers nal factors.
and commissioners together in common purpose Results highlighted that the evidence base for the decision
rather than what is sometimes a more adversarial role to plan for an anticipated increase in demand for sexual
[Interviewee 05] health services may have been insufficient. Despite stake-
holders reporting no increase in demand for services, the
I think the legacy is getting existing services doing some-
Olympic Games provided an opportunity for sexual health
thing slightly different, and know[ing] that they can do it
services to try new ways of working, engage with stakeholders
and it’s not going to be onerous [Interviewee 09]
and develop new relationships.
Aims to transform services and relationships were relatively
Challenges unsuccessful, attributed to lack of time to achieve sufficient
Awaiting sign off by senior staff was a key documented delay- buy-in and confounded by NHS restructuring.
ing factor. Governance and communication seemed very thorough.
Respondents felt that major restructuring and reform of One of the key problems mentioned in this evaluation was the
the NHS during the programme had a major impact on its issues with private sector involvement.
success, particularly in engaging NHS stakeholders and Successful engagement was reported, although many parti-
restricting funding. cipants felt aiming to engage the public was inappropriate and
There were much bigger issues that people in the NHS overambitious.
were grappling with so this programme probably ended up Although unclear, the main potential legacy opportunities
being much less of a priority for people. . .. [Survey 4] were the planning work that was done; the groundwork for
transformation ideas; relationship building and continuing the
Progress reports and respondents also identified the difficult changes implemented in the resilience work.
relationship with the private sector as a challenge (see health
promotion above).
What is already known on this topic
A number of interviewees cited limited resources as
Although a study of the Sydney Olympics demonstrated
restricting health promotion and engagement, particularly the
increased use of sexual health services and STIs,4 other eva-
reduced funding (also documented in progress reports), al-
luations of the London and Sydney Games have found little
though the programme was generally seen as successful
change in routine activity in other services9 and no major
within the finite resources. Time was also limited, particularly
public health incidents.2,10 In addition, the evidence base for
for achieving transformation.
the decision to plan for an anticipated increase in demand was
Funding and therefore legitimacy were always neglected with limited across public health services.2 Black et al.2 found that
this work programme – without funding it was always going initially NHSL anticipated minimal impact on health services,8 J O U R NA L O F P U B L IC H E A LT H
but, as the Games approached, planning for increased messages. Future programmes should be cautious about
demand increased, perhaps due to anxiety about responsibility attempting transformation of services during the event, al-
among NHSL and doubt as to the relevance of data from pre- though opportunities for transformation should be recognized.
vious Olympics. Extensive, diverse, regular stakeholder engagement, in
Similarly to this evaluation, Black et al.’s evaluation also particular commissioners, is crucial and can provide an excel-
found that systemic improvements to public health, rather than lent opportunity for collaboration; however, public engage-
a health legacy, were seen, such as changes to service delivery ment should be focussed to avoid wasting resources. Third
and relationships.2 Lack of clarity regarding legacy was also sector organizations are vital in ensuring engagement with
identified, attributed to unclear definitions, lack of funding, hard-to-reach groups and in achieving outcomes. Young
‘deprioritization’, unsustainability and lack of measurement.2 people are often enthusiastic and the ‘Sex Factor Ideas 2012’
Participants’ concerns about the lack of consistency in lead- competition model could be used for future events and en-
ership and accountability (due to MBARC taking over after the gagement with young people in sexual health.
programme had started and delay in appointing a programme Participants were divided as to whether sexual health
manager) appears legitimate, as Tsouros et al. cite strong and should have been dealt with separately to other health issues.
consistent leadership as a critical factor in public health This is perhaps part of a wider debate, for example in the
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
planning for Olympic Games.8 The relationship between NHS sexual health used to be commissioned by specialist
NHSL and LOCOG was also problematic in Black et al.’s services and is now predominantly commissioned as part of
evaluation, particularly differences in culture and priorities.2 public health (by local authorities).11 The pros and cons of
Successful engagement is known to be key, for example in including sexual health as part of general health promotion
Black et al.’s evaluation where connections between the NHS or developing separate programmes should be considered at
and stakeholders were a key factor in successful delivery of future events.
the public health planning for the Games.2
The NHS reforms did have a significant impact on sexual Limitations of this study
health services11 and their commissioning and were not As the evaluation was commissioned after the programme
without controversy.12 The impact of the NHS reforms on was completed we were unable to compare results before and
the programme echo those seen in the Athens Games due to after and relied on LSHP and MBARC to recommend who
a change of government 5 months before the start.8 we should invite to participate. Commissioning the evaluation
as part of the initial planning for the programme may have
What this study adds prevented delays.
As the first ever host city to have a sexual health programme, Response rates were low, which may be due to NHS
the plans and documentation can provide support, process reform occurring during the evaluation period, meaning that
lessons and data for future events, e.g. Rio in 2016, the many potential respondents had other priorities and had
Commonwealth Games in Glasgow in 2014 and potentially perhaps changed jobs. The results of the evaluation should
the Gay Games in London in 2018. thus be used with caution as the evaluation sample is unlikely
This study confirms that a clear vision, evidence-based aims to be representative of all stakeholders.
and consistency in leadership and accountability are important Given more time and resources we would have liked to
for the success of programmes of public health planning interview a wider range of stakeholders, in particular those
for mass gatherings.8 The governance and communication who were not actively engaged in the programme, to evaluate
processes in this programme should inform future similar its wider impact.
programmes. Careful planning, timely reporting and commu-
nication strategies are crucial10 and programmes may need to
Conclusion
allow extra time for approvals needed from senior staff, espe-
cially if other external factors may influence their priorities. This evaluation provides recommendations for sexual health
Decisions regarding potential increase in demand should services during future events. Sexual health services were not
be made on a local basis, although a programme to cope with disrupted by the 2012 Olympic and Paralympic Games, and
potential extra demand for services can provide assurance to demand did not appear to increase. Although services were
stakeholders and ensure preparedness. Signposting users away not transformed as intended, the programme resulted in a
from GUM and a SARC residual risk response may be useful. number of legacy opportunities to improve sexual health ser-
The Games may not have been the best time to attempt vices in London, particularly engagement, relationship build-
transformation, in particular amongst so many competing ing and resilience of services.S E X UA L H EA LT H P L A N NI N G FO R T H E LO N DO N 2 0 1 2 O LY M P I CS 9
Acknowledgements 4 McNulty AM, Rohrsheim R, Donovan B. Demand for sexual health
services during the Olympic Games: both sides of the Sherman
Dr Lorenc and Prof Robinson would like to thank all the effect. Int J STD AIDS 2003;14(5):307 –8.
survey and interview participants, as well as MBARC for their 5 Deering KN, Chettiar J, Chan K et al. Sex work and the public health
cooperation. impacts of the 2010 Olympic Games. Sex Transm Infect
2012;88(4):301– 3.
6 Brennan RJ, Keim ME, Sharp TW et al. Medical and public health
Ethical approval services at the 1996 Atlanta Olympic Games: an overview. Med J Aust
1997;167(11 – 12):595– 8.
Ethical approval was given by London South Bank University
7 Enock KE, Jacobs J. The Olympic and Paralympic Games 2012: lit-
Research Ethics Committee in October 2012, reference UREC
erature review of the logistical planning and operational challenges
1268. for public health. Public Health 2008;122(11):1229 – 38.
8 Tsouros A, Stergachis A, Barbeschi M et al. The Athens 2004
Olympic Games and public health: main conclusions and lessons
Funding
learned. In: Tsouros AD, Efstathiou P. (eds). Mass Gatherings and
This work was supported by the London Sexual Health Public Health. The Experience of the Athens 2004 Olympic Games.
Downloaded from http://jpubhealth.oxfordjournals.org/ by guest on September 30, 2015
Copenhagen: WHO, 2007.
Programme (LSHP).
9 Williams K, Sinclair C, McEwan R et al. Impact of the London 2012
Olympic and Paralympic Games on demand for microbiology gastro-
intestinal diagnostic services at the Public Health Laboratory
References London. J Med Microbiol 2014;63(Pt 7):968 – 74.
1 Hadjichristodoulou C, Mouchtouri V, Soteriades ES et al. Mass gath- 10 Jorm LR, Thackway SV, Churches TR et al. Watching the games:
ering preparedness: the experience of the Athens 2004 Olympic and public health surveillance for the Sydney 2000 Olympic Games. J
Para-Olympic Games. J Environ Health 2005;67(9):52– 7. Epidemiol Community Health 2003;57(2):102 – 8.
2 Black G, Kononovas K, Taylor J et al. Healthcare planning for 11 FPA. What does the Health and Social Care Bill mean for sexual
the Olympics in London: a qualitative evaluation. PLoS One health services in England? 2012. http://wwwfpaorguk/sites/
2014;9(3):e92338. default/files/health-and-social-care-bill-and-sexual-health-services-
3 Abubakar I, Gautret P, Brunette GW et al. Global perspectives for march-2012 pdf (1 July 2014, date last accessed).
prevention of infectious diseases associated with mass gatherings. 12 Maynard A. NHS reform: the risks of jumping on the spot again. J R
Lancet Infect Dis 2012;12(1):66– 74. Soc Med 2013;106(5):164 – 6.You can also read