COVID Oximetry@home Webinar on Primary Care - led pulse oximetry and remote monitoring - Barnet CEPN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
COVID Oximetry@home
Webinar on Primary Care – led pulse oximetry and remote
monitoring
26 January 2021
3:30-5pm
Hosted by NHS London Respiratory Clinical Network, NHS London COVID Remote
Monitoring Cell and London Academic Health Science Networks (AHSNs)
This work is informed and enabled by National NHSE/I, NHS X and NHS D remote
monitoring initiatives.
Supported by Healthy London Partnership and NEL Healthcare Consulting
1. Welcome and why this is important
Dr Jo Sauvage
GP and Clinical Chair of NCL CCG
Clinical Lead for London COVID Remote Monitoring Cell, NHS London
Dr Irem Patel
Consultant Respiratory Physician, Integrated Care;
Clinical Co-Director NHSE London Respiratory Clinical Network;
Joint Director of Clinical Strategy, King’s Health Partners
2
London 23rd December 2020….
The problem…..
• Rapid uptick in Covid 19 cases since early December 2020
• Variation in availability of Covid Oximetry @ home pathways across London
• Variation in availability of Covid Virtual Ward pathways across London
• Variation in application of Standard Operating Procedures (SOPs)
• Visibility and interoperability complex as pathways involve multiple providers and interfaces in each
ICS
The proposed solution needed to ensure patients able to consistently access the care they needed for
their stage of disease in timely manner
Operational pressures (London Ambulance Service (LAS), Emergency Departments (EDs) and the
General and Acute (G&A) bed base)
• given the increased demand for services
• impact of infection control social distancing measures
• transportation challenges
3
Aims of our webinar today – COVID Oximetry@home
1. Describe the collective why – responding to the impact of current COVID
surge on Londoners and the services caring for them
2. Describe the cohort of people who will benefit from the COVID Oximetry
@home primary care led model
3. Share learning from General Practice/Primary Care across London in delivering
this model of care and how it works in practice
4. Outline what is required next to ensure all Londoners have equal access to
the same standard of provision and how NHS London is enabling and assuring
implementation
4
COVID Oximetry@home – agenda
# Item Speaker Timing
1 Welcome and why this is important Dr Jo Sauvage and Dr 15:30 – 15:35 (5 min)
Sarah Elkin
2 Sli.do interactive session Sophie Bulmer 15:35 – 15:40 (5 min)
3 COVID Oximetry@home - National context and London approach Dr Jo Sauvage 15:40 – 15:55 (15 min)
to delivering great care
4 Patient cohorts for COVID Oximetry@home – who benefits? Dr Kuldhir Johal 15:55 – 16:10 (15 min)
5 Operationalising COVID Oximetry@home – learning from local Dr Katie Coleman and Dr 16:10 – 16:25 (15 min)
implementation Stephanie Coughlin
• Supporting general practices to implement the pathway
• How we worked with ED, NHS 111, LAS and EA
6 Slido interactive session with audience on three questions Sophie Bulmer 16:25 – 16:30 (5 min)
7 Next steps to enabling implementation Fiona Howgego 16:30-16:40 (10 min)
• Role of NHS London COVID Remote Monitoring Cell
• Next steps and support available
8 Facilitated audience Q&A Catherine Dale 16:40 – 17:00 (20 min)
5
2. Sli.do - Hearing from our audience
Sophie Bulmer
Network Development Lead , UCLP
Participate on
On your phone: slido app
On your web browser: slido.com
Part 1 event code: #95657
6
3. COVID Oximetry@home - National context and London
approach to delivering great care
Dr Jo Sauvage
GP and Clinical Chair of NCL CCG
Clinical Lead for London COVID Remote Monitoring Cell, NHS London
7
National guidance: informing our approach in London
The National NHS@home team launched COVID Oximetry@Home
SOP on 12th November 2020, with clear guidance around:
• Entry criteria
• Staffing and oversight
• Patient journey
• Oximeter supply and safe re-use
• Care homes
• Coding, record keeping and data
requirements
Visit www.ahsnnetwork.com/covid-oximetry for more information:
• Sign up to the National Learning Network
• Find tools and resources to help implementation
• Contact your local Patient Safety Collaborative, who are
supporting COVID Oximetry@home and COVID Virtual Wards
8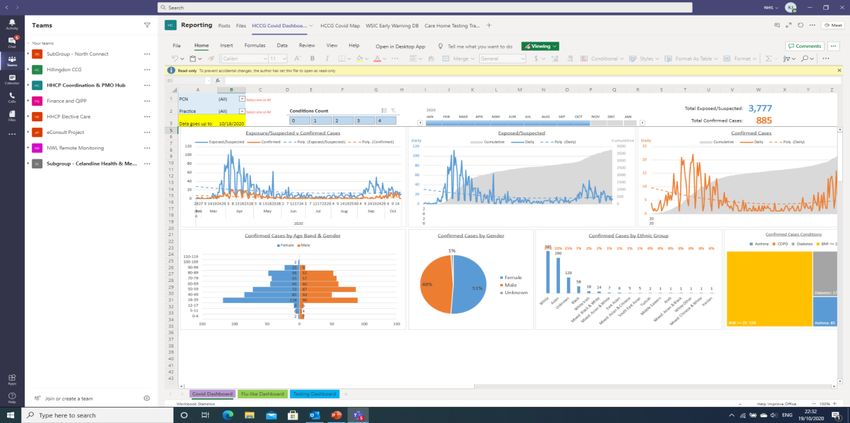
9

10
Aligning COVID pathways across care settings to
standardise access to great COVID care
Understanding the difference between COVID
Oximetry@home and COVID Virtual ward
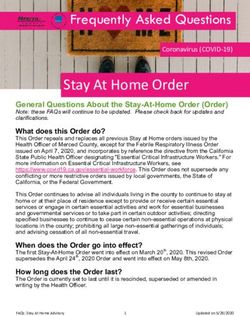
Building on NHS National COVID 19 assessment and
treatment pathways, NHS London has produced the 4
Actions paper to provide clarity on the difference
between primary care-led COVID Oximetry@home and
COVID Virtual Ward care models.
This will help to ensure the right cohorts of the population
are triaged into the right level of remote monitoring and
safety netting according to their specific requirements.
COVID Severity assessment – consistency matters
Aligning criteria to grade the severity of clinical risk
enables UEC (LAS,111) partners to escalate treatment to
the right place, at the right time. This helps to create
consistency in access to great COVID care across our
Capital, regardless of the person’s geographical location.
11January 2021: Our opportunity to deliver best care for
Londoners
• Increased role out of COVID Oximetry@ home across London at scale and pace
• Optimise uptake of remote monitoring to safety net to improve early detection of
deterioration in COVID-19
• Help people to be able to self manage their condition safely at home and know when
and how to get help
• Implementation of systems and processes that ensures appropriate identification
of the right patients who need face to face assessment by a senior clinician, some
who may require diagnostics.
• Senior specialist support as required through COVID Specialist Advice line
• Optimise management of operational pressures in NHS services in London
• Increase clinician knowledge and confidence in clinical management
• Improve pathway interoperability through greater visibility of local services
• Increase clinician understanding of local services and how to refer/use
• Growing and maturing MDT working
• Improve consistency in service provision as well as enhanced clinical care, safety
& patient experience
• Develop a blue print and legacy for remote monitoring of LTCs for the future
12Supporting flow in COVID UEC pathway for London: the
contribution of COVID remote monitoring through 4 actions
The purpose of this document is to ensure:
1. Consistent criteria are applied that maintains patient safety in the community and helps identify
patients most at risk wherever they present
2. Each ICS system able to consider the most appropriate model for them with best utilisation of space
and workforce
3. Benefits to flow and capacity as managed by LAS handover and ED length of stay are realised
COVID Oximetry @Home monitoring
Action 1 Rapid implementation and scaling of community-led Oximetry @Home for
safety netting and management of lower risk patients in the community,
including links to ED and out of hours services to support admission avoidance
London SPOC
Action 2 Development of secondary care led acute-led COVID Virtual Ward services to
mandated delivery
provide early supported discharge after ED attendance or hospital admission
of Actions 1 and 2
8 January 2021.
Best utilisation of available space and staffing – either/both to be implemented
Action 3 Consideration of optimal utilisation of any free clinical space within the ICS locations to:
Option 1: Provide a red same day emergency care COVID assessment and diagnostic unit And/ Or
Option 2: Provide a clinically monitored cohort area for COVID patients awaiting G&A bed admission
13The London COVID Oximetry@Home Interactive Map:
improving the visibility of local services London ICS
• This interactive map can be used to provide information
on the COVID Oximetry@Home provision within each
locality of London and also the referral routes into the
clinical settings that ‘onboard’ patients into these
pathways from alternative care settings
• Each area has an overview slide, which has a map of the
service provision available, with key contacts and
documents embedded
Downstream referral routes into COVID
Oximetry@Home pulse oximetry provision
• There is also a slide for each of the four care settings for 111/IUC/999 E-CAS/CCAS
outlined below to provide a Pan London view of the Downstream referral routes for 999 crews
(via MIDOS) into COVID Oximetry
service provision available for clinicians within these @Home pulse oximetry provision
services to refer patients into so that they can be Downstream referral routes into COVID
effectively ‘onboarded’ onto pulse oximetry pathways. Oximetry@Home provision for secondary
care
Referral routes into COVID
Oximetry@Home pulse oximetry provision
for primary care (In Hours/Out of Hours)
14 |NCL – High level overview of COVID Oximetry@Home
care provision
Overview of NCL Oximetry@home model:
Clinical Lead: Katie Coleman
Patients are onboarded into COVID Oximetry@home pathway via their GP and Extended Access Hubs. Operational Leads: Shafeeq Tejani, Meena Mahil
Advice and Guidance Line: In place
Who does the monitoring? Local GPs and GP Federations. GP Federations provide senior clinical triage
and home visiting where needed. Pulse oximetry monitoring over weekends provided by Extended Access
NCL Number of patients managed with Oximetry
hubs and LCW (Out of Hours) at Home (11.01): 512-1101*
Number of oximeters sent: 6,500 * Figure of 512 based on return from 93 GP practices. 1101
extrapolated figure for all NCL practices.
Key Points:
• COVID Oximetry@Home being led by GP
in-hours and Extended Access Hubs. No
digital solution in place.
• Integrated model established between
LCW and NCL Primary Care to ensure out
of hour pulse oximetry provision is in
place.
Any Exceptions:
• The specialist NCL COVID-19 service,
COVID Hot Hub set up in Islington, does not onboard
Specialist COVID services patients onto local pulse oximetry
Secondary care pathways. Patients are passed back to
All GP Practices in NCL their GP for onboarding.
supporting COVID demand
15 | GP OOH in all boroughs4. Patient cohorts for COVID Oximetry@home – who benefits?
Dr Kuldhir Johal
General Practitioner and NWL Remote monitoring COVID19 – Primary care clinical lead.
Governing Body Member of NHS Hillingdon CCG
16Slides will be shared following this event • Templates – codes – SNOMED CO@home aligned codes • NHSD data – pillar 1, 2 and 4 data set made available to you and how to use • EMIS, S1 and SNOMED alignment – London agreed approach • (Templates and searches will be cascaded accordingly)
Coding into your current systems – Primary Care • Suspected COVID19 – 1240761000000102 • Disease COVID19 - 1240751000000100 • Ethnicity • Height • Weight • Saturations - O2 • PDS – check postcode, telephone number – SCR alignment • For every case of Positive Pillar 2 result – • add in code for “Disease COVID19” • You already have this information at practice level – • aggregate at PCN/Borough/CCG/Region • “Code” – use the “same language” • SNOMED Codes – UK National - any healthcare setting
Log of suggested codes • Dr Kuldhir Johal following discussions with Dr Tony Willis, Dr Simon Gordon, Dr Afsana Safa in NWL – EMIS and S1 alignment – 19/01/2021 • Following discussion with Dr Katie Coleman – NCL – alignment 21/01/2021 • London COVID Remote Monitoring Programme Board –22/01/2021 – agreed adoption of codes and rollout across London
Patient referral, decision to Virtual ward monitoring and
Daily reviews Discharge
add to Virtual ward on-boarding
GP practice/111 book CEC telephone
appointment via SystmOne/EMIS for
• Nurse/HCA calls patient 3 times a day • Patient no longer requires telehealth
suspected COVID-19 patient
to retrieve the vital signs and update monitoring
these on S1/EMIS • GP informs patient of discharge plan
• Nurse/HCA deploys sats probe and
CEC GP carries out virtual hub appointment • Nurse identifies escalations and books • GP gives safety netting advice and codes
ensures that patient is added to task
using S1/EMIS (telephone/video/F2F/HV) appropriately timed same day virtual offboarding from virtual ward
group/ caseload and has follow up
appointments in place on S1/EMIS for appointment with GP Coding (on template):
GP offers Virtual Ward monitoring – daily GP reviews via task on S1/EMIS • Discharge from virtual ward (708252004
identifies whether patient is for app or not GP consultation – Patient data in S1/EMIS / XaXnm / 8HgE)
and adds to virtual ward record. GP reviews and makes clinical plan
Coding (on template):
• Admission to virtual ward
(784431000000109 / XaXpP / 8Hv)*
• Nurse reviews Medopad dashboard
three times a day. Liaises with patients
GP adds patient to same day nurse/HCA on- not using correctly (under- / over-using)
boarding slot and informs patients they will • Patient no longer requires telehealth
get a call that day for this process • Nurse/HCA sends the Medopad monitoring
Coding (on template): onboarding SMS, talks patient through • Nurse transfers Medopad data to • GP informs patient of discharge plan
• Telehealth monitoring invitation the app set up (including setting S1/EMIS record • GP gives safety netting advice and
(922451000000105 / XabY5 / 8AB4) OR reminders for observation recording) and informs nurse
Coding (on template):
• Telehealth monitoring declined confirms onboarding
• Step up change in telehealth monitoring
(750451000000101 / XaWzf / 8AB2) OR (722299009 / XacXO / 8AB7) • Nurse discharges patient from S1/EMIS
• Telehealth monitoring not appropriate and speaks to patient to off board from
(750451000000101 / XaWzf / 8AB2) app and virtual ward
• Nurse/HCA adds patients to task group • Nurse identifies escalations and books
and codes Telehealth monitoring on appropriately timed same day virtual Coding (on template):
Key: • Ending of telehealth monitoring
S1/EMIS appointment with GP
GP, S1/EMIS (726871000000107 / XaWNH / 8AB0)
Coding (on template):
AND
• Starting of telehealth monitoring GP practice/111 book CEC telephone
Nurse, S1/EMIS • Discharge from virtual ward (708252004
(726861000000100 / XaWNG / 8AB1) appointment via SystmOne/EMIS for / XaXnm / 8HgE)
suspected COVID-19 patient
Nurse, Medopad
*Codes shown as SNOMED / CTV3 (S1) / READv2 (EMIS) Proxy codes alignment in Wave 1 of the
COVID19 Pandemic NWL April/May 2020 – Proxy codesPatient referral, decision to add to
COVID Oximetry@home – GP CO@home monitoring and on-
Practice and GP Practice as site for Daily reviews Discharge
boarding
CO@home
GP practice/111 book telephone appointment via
SystmOne/EMIS for suspected COVID-19
patient/confirmed/high risk • Nurse/HCA deploys sats probe and • Nurse/HCA calls patient 3 times a day • Patient no longer requires CO@home
ensures that patient is added to task to retrieve the vital signs and update monitoring
Coding (on template): Referral to telehealth pulse group/ caseload and has follow up • GP informs patient of discharge plan
these on S1/EMIS
oximetry monitoring service
(1325251000000106/Y2a44/EMISNQRE644)
appointments in place on S1/EMIS for • Nurse identifies escalations and books • GP gives safety netting advice and codes
daily GP reviews via task on S1/EMIS appropriately timed same day virtual offboarding from virtual ward
appointment with GP Coding (on template):
GP carries out appointment using S1/EMIS
(telephone/video/F2F/HV) Discharge from telehealth pulse oximetry
Coding (on template): Provision of pulse monitoring service
GP consultation – Patient data in S1/EMIS
oximeter (132561000000102/Y2a46/EMISNQDI271)
record. GP reviews and makes clinical plan
(1325211000000107/YA796/EMISNQPR508)
GP offers CO@home monitoring – identifies
whether patient is for app or not and adds
to HUMA APP • Nurse reviews Medopad aka HUMA
dashboard three times a day. Liaises with
GP adds patient to same day nurse/HCA on- patients not using correctly (under- /
• Nurse/HCA sends the Medopad aka over-using)
boarding slot and informs patients they will • Patient no longer requires CO@home
HUMA onboarding SMS, talks patient
get a call that day for this process monitoring
through the app set up (including setting
Coding (on template): • Nurse transfers Medopad/HUMA data to • GP informs patient of discharge plan
reminders for observation recording) and
Discussion about telehealth pulse oximetry S1/EMIS record • GP gives safety netting advice and
confirms onboarding
monitoring informs nurse
Coding (on template):
(1325281000000100/Y2a4b/EMISNQDI273) Coding (on template): Provision of pulse • Step up change in telehealth monitoring
Telehealth pulse oximetry monitoring not oximeter (1325211000000107/YA796/ (722299009 / XacXO / 8AB7) • Nurse discharges patient from S1/EMIS
appropriate EMISNQPR508) and speaks to patient to off board from
(1325221000000101/Y2a49/EMISNQTE34) app and CO@home
Telehealth pulse oximetry declined • Nurse/HCA adds patients to task group • Nurse identifies escalations and books
(132541000000108/Y2a4a/EMISNQTE35) appropriately timed same day Coding (on template):
and codes CO@home on S1/EMIS Telehealth pulse oximetry monitoring
appointment with GP
Key: GP, S1/EMIS ended
GP Coding (on template): Telehealth pulse
Practice (1325201000000105/Y2a47/EMSINQTE33)
oximetry monitoring started GP practice/111 book telephone AND
(1325191000000108/Y2a48/EMISNQTE32) appointment via SystmOne/EMIS for • Discharge from telehealth pulse oximetry
CO@home Nurse, S1/EMIS suspected COVID-19 patient monitoring service
CO@home Nurse, HUMA • (132561000000102/Y2a46/EMISNQDI271)
*Codes shown as SNOMED / CTV3 (S1) / READv2 (EMIS) updated 18/01/2021 TO Reflect COVID
Oximetry@home National Codes alignmentPatient referral, decision to add to CO@home monitoring and on-
COVID Oximetry@home – Hot site
Daily reviews Discharge
boarding
GP practice/111 book telephone appointment via
SystmOne/EMIS for suspected COVID-19
patient/confirmed/high risk
• Nurse/HCA deploys sats probe and • Nurse/HCA calls patient 3 times a day • Patient no longer requires CO@home
Coding (on template): Referral to telehealth pulse ensures that patient is added to task to retrieve the vital signs and update monitoring
oximetry monitoring service group/ caseload and has follow up these on S1/EMIS • GP informs patient of discharge plan
(1325251000000106/Y2a44/EMISNQRE644)
GP carries out virtual hub appointment appointments in place on S1/EMIS for • Nurse identifies escalations and books • GP gives safety netting advice and codes
using S1/EMIS (telephone/video/F2F/HV) daily GP reviews via task on S1/EMIS appropriately timed same day virtual offboarding from virtual ward
appointment with GP Coding (on template):
GP offers CO@home monitoring – identifies Discharge from telehealth pulse oximetry
whether patient is for app or not and adds Coding (on template): Provision of pulse monitoring service
GP consultation – Patient data in S1/EMIS
to virtual ward oximeter (132561000000102/Y2a46/EMISNQDI271)
record. GP reviews and makes clinical plan
(1325211000000107/YA796/EMISNQPR508)
Coding (on template):
Referral by telehealth pulse oximetry
monitoring service • Nurse reviews Medopad aka HUMA
(1325261000000109/Y2a45/EMISNQRE643) HUMA APP
dashboard three times a day. Liaises with
GP adds patient to same day nurse/HCA on- patients not using correctly (under- /
• Nurse/HCA sends the Medopad aka over-using)
boarding slot and informs patients they will • Patient no longer requires CO@home
HUMA onboarding SMS, talks patient
get a call that day for this process monitoring
through the app set up (including setting
Coding (on template): • Nurse transfers Medopad data to • GP informs patient of discharge plan
reminders for observation recording) and
Discussion about telehealth pulse oximetry S1/EMIS record • GP gives safety netting advice and
confirms onboarding
monitoring informs nurse
Coding (on template):
(1325281000000100/Y2a4b/EMISNQDI273) Coding (on template): Provision of pulse • Step up change in telehealth monitoring
Telehealth pulse oximetry monitoring not oximeter (1325211000000107/YA796/ (722299009 / XacXO / 8AB7) • Nurse discharges patient from S1/EMIS
appropriate EMISNQPR508) and speaks to patient to off board from
(1325221000000101/Y2a49/EMISNQTE34) app and CO@home
Telehealth pulse oximetry declined • Nurse/HCA adds patients to task group • Nurse identifies escalations and books
(132541000000108/Y2a4a/EMISNQTE35) appropriately timed same day virtual Coding (on template):
and codes CO@home on S1/EMIS Telehealth pulse oximetry monitoring
GP appointment with GP
Key: Practice GP, S1/EMIS ended
Coding (on template): Telehealth pulse
(1325201000000105/Y2a47/EMSINQTE33)
Hot Site GP, S1/EMIS oximetry monitoring started GP practice/111 book CEC telephone AND
(1325191000000108/Y2a48/EMISNQTE32) appointment via SystmOne/EMIS for • Discharge from telehealth pulse oximetry
Hot Site Nurse, S1/EMIS suspected COVID-19 patient monitoring service
Hot Site Nurse, Medopad • (132561000000102/Y2a46/EMISNQDI271)
*Codes shown as SNOMED / CTV3 (S1) / READv2 (EMIS) updated 18/01/2021 TO Reflect COVID
Oximetry@home National Codes alignmentPatient referral, decision to add to
CVW monitoring and on-
HOSPITAL COVID VIRTUAL WARD Daily reviews Discharge
(CVW) boarding
Respiratory team adds to hospital CVW
Codes for source of referral • Nurse/HCA deploys sats probe and
ensures that patient is added to task • Nurse/HCA calls patient 3 times a day • Patient no longer requires CVW
group/ caseload and has follow up to retrieve the vital signs and update monitoring
Coding (on template):Admission to virtual ward
appointments in place on Hospital these on S1/EMIS • GP informs patient of discharge plan
((784431000000109 / XaXpP / 8Hv)*
record/S1/EMIS for daily Dr/HCA/Nurse • Nurse identifies escalations and books • GP gives safety netting advice and codes
reviews appropriately timed same day offboarding from CVW
appointment with Dr Coding (on template):
Hospital team – identifies whether patient Discharge from virtual ward (708252004 /
is for app or not and adds to (CVW) virtual Coding (on template): Provision of pulse Dr consultation – Patient data in Hospital XaXnm / 8HgE)
ward oximeter (1325211000000107) record/S1/EMIS record. Dr reviews and
makes clinical plan
HUMA APP • Nurse reviews Medopad aka HUMA
dashboard three times a day. Liaises with
Dr adds patient to same day nurse/HCA on- patients not using correctly (under- /
• Nurse/HCA sends the Medopad aka over-using)
boarding slot and informs patients they will • Patient no longer requires CVW
HUMA onboarding SMS, talks patient
get a call that day for this process monitoring
through the app set up (including setting
Coding (on template): • Nurse transfers Medopad data to • Dr informs patient of discharge plan
reminders for observation recording) and
Discussion about telehealth pulse oximetry Hospital record/S1/EMIS record • Dr gives safety netting advice and
confirms onboarding
monitoring (1325281000000100 informs nurse
Coding (on template):
Telehealth pulse oximetry monitoring not Coding (on template): Provision of pulse • Step up change in telehealth monitoring
appropriate (1325221000000101 oximeter (1325211000000107) (722299009 / XacXO / 8AB7) • Nurse discharges patient from Hospital
Telehealth pulse oximetry declined IT/ S1/EMIS and speaks to patient to off
(132541000000108) board from app and CVW
• Nurse/HCA adds patients to task group • Nurse identifies escalations and books
and codes CVW monitoring on Hospital appropriately timed same day Coding (on template):
Key: Hospital Hospital system Telehealth pulse oximetry monitoring
team IT/S1/EMIS appointment with Dr
CVW Hospital IT ended (1325201000000105/
Coding (on template): Telehealth pulse
Site
Nurse, Hospital oximetry monitoring started
Hospital • AND
record (1325191000000108
• Discharge from virtual ward (708252004 /
Hospital Nurse, Medopad XaXnm / 8HgE)
*Codes shown as SNOMED / CTV3 (S1) / READv2 (EMIS) updated 18/01/2021Understanding the whole picture GP Practice only – All patients – Isolation leaflet Referral to telehealth pulse oximetry monitoring service (1325251000000106/Y2a44/EMISNQRE644) CO@home – GP Practice Discharge from telehealth pulse oximetry monitoring service (132561000000102/Y2a46/EMISNQDI271) CO@home – Hot Site Referral by telehealth pulse oximetry monitoring service (1325261000000109/Y2a45/EMISNQRE643) Discharge from telehealth pulse oximetry monitoring service (132561000000102/Y2a46/EMISNQDI271)
Moving from Reactive care to Proactive care for
Early Identification
Capturing the clinical information and
code alignment – in the different settings
ITU
Inpatient
CO@home CVW
111/999 OOHs
Secondary
Primary care Community
CareGenerate reports and CSV files – for NHSD/London PRM 111/999 alignment
The NWL COVID-19 Virtual Ward tech-enabled experience
was designed to be as simple as possible for clinicians and
patients
A step-by-step guide to the tech-enabled COVID-19 Virtual Ward remote monitoring experience
1
Patient referred
to Hot Hub with 2 3 4 5 6
COVID-19 symptoms
Staff member onboards Patient downloads Patient reports vital Staff member reviews Clinician calls priority
patient to app with link vital sign and symptom signs and symptoms patient population RAG patients for follow-up
and unique code reporting app through app daily dashboard and appropriate action
Text message and Observations collected and assessed 3 x a day All patients received a GP
leaflet sent to patient • Oxygen saturation and heart rate consultation 1 x a day to ensure
(via provisioned pulse oximeter), temperature clinical safety and test accuracy of
Breathlessness rating and symptom profile 1 x a day observation monitoring as method
to accurately pick up deterioration
Green tick on app
The dash board – allows for
Use of tools, telephone, indicates the clinician
viewing of all the patients in one
SMS, AccuRx, pdf, has seen the record, or
view – rather than having to go into
paper – recorded in if diary – readings are
each individual record – helps as
clinical system added into clinical
the number of cases goes up
record either way
GP Practice – Cross-
organisational booking –
into Escalated care clinicClinical parameters over time give an idea of trend for
each individual case – in the primary care setting it is
about identifying early and empowering the patient and
clinician to do this confidently and know what to do next…
• The guidance recommends assessing • “I recently had covid.
patients for hospital admission when they • I was relieved when I had no fever on day 5. But on day 9 the fever came
continue to have oxygen levels at 93%- back with breathlessness and loss of smell.
94% (when this is lower than usual for them). • I was very scared - scared of having to go to a hospital and leave my
daughters all alone - every single parent's nightmare.
• If a patient has oxygen levels of 92% or • I called 111 and they referred my case to Soho CEC -that changed everything
lower they are considered in for me! I got all the monitoring of a hospital ward, right here at home.
the severe category and to need urgent • The doctors and staff were very kind and had a very comforting bedside
admission to hospital. manner. They were very attentive, decisive and comforting. The doctors even
arranged for the medicine to be delivered to my residence when the
connection with my surgery/boots didn't work. I couldn't have asked for
• Patients with oxygen levels of 95% or above more when locked all alone and unable to go out and help myself.
are considered 'mild' but to require • The medopad app became a friend and was very easy to use. On day 15, I
monitoring. They are recommended to had chest pains that I fed into the medopad app - I had a call from the Soho
CEC doctor within a few minutes. She spent time with me on the phone
have exercise testing and to be considered trying to assess the source of the pain and was very assuring and efficient.
for admission to hospital if their levels drop
• I beat covid with the wonderful Soho CEC by my side and am getting stronger
by 3% or more on exertion. with each passing day.
• A huge thank you to all the staff and wonderful doctors who supported me
through my ordeal. THANK YOU for this service
• Thanks”5. Operationalising COVID Oximetry@home – learning from
local implementation
Dr Katie Coleman, NCL Clinical lead Primary care Development
Dr. Stephanie Coughlin, NEL COVID Oximetry@home lead
31Our journey to date: two system-wide perspectives
NCL: Dr Katie Coleman NEL: Dr Stephanie Coughlin
• All practice implementation total triage • Majority boroughs operating through central
• Early adoption of using Sats probes (Pulse Federation run model. 2/7 boroughs utilising
oximeters) - mixed model via hot hubs/via GP a practice-led approach
practice • Different levels of maturity
• Upskilling of general practice around IPC and • One borough had in place pulse oximetry
confidence building to see COVID +ve patients monitoring service since April 2020
• Hot hubs stood down, implementation NCL • Hot hubs in place in each of the boroughs
wide COVID support service + general practice • NEL Digital support solution – OneContact
delivery of COVID Oximetry@home
• Third wave – rapid role out NHSE CO@H SOP
32Essential criteria for successful delivery of COVID
Oximetry@home
Enough pulse oximeters
Clearly defined pathway
GP leadership and good engagement
Provider leadership and engagement
Patient information in variety of formats and languages
Managing interfaces between local, system and
London – level services
Proactive care delivery
33Having a clear patient pathway is key
1. Clear inclusion criteria
2. COVID Oximetry@home register
• a. Which people are for active follow up:
• When required while on pathway
• At 6 weeks (NCL)
• b. Agree method of follow up:
• Text
• Email
• Phone
4. Location of pulse oximeter
5. Patient resources in all relevant languages
6. Clear Treatment Escalation Plan (TEP) for clinical review
7. Process for capturing patients onboarded via:
• ED
• NHS 111
• Extended Access
• LAS
• In-patients
• COVID virtual ward
34Engaging effectively with our GP colleagues
means….
1. Consistent and recurrent messaging and communication
2. Training events
3. Webinars
4. GP bulletins
5. Resources:
• Process map
• Templates
• Searches
• Data collecting spreadsheets
• PILs and videos
• Follow up methods
• Clinical escalation check list
• Caller scripts
35London overview: the interface of alternative care settings
with COVID Oximetry@Home
Referrals from LAS
999 crews
Referrals from COVID@Home Referrals from
111/IUC/999 E- Pulse Oximetry Secondary Care
CAS/CCAS Pathway settings
Referrals from
Primary Care
36 |Engaging effectively with our provider colleagues
means….
• Ensure conversations with all providers including:
• Acute providers
• Community providers
• Mental health providers
• London Ambulance Service (LAS)
• NHS 111
• Extended access
• Local Authority
• Consistent resources primary/secondary/community care
• Need to consider demand and capacity so services not
overwhelmed
37Managing interfaces between care providers
It is helpful to consider a number of interfaces to ensure safe treatment escalation/de-escalation
across the COVID Oximetry@home pathway
Two-way interfaces Other interfaces
SDEC GP
GP ED
COVID VW GP
GP NHS 111
Care Homes GP
GP LAS
Prison Service
38Enabling proactive care
1. Daily searches for covid +ve patients
identified via national testing
Group 1 65 andChallenges and emerging solutions to these
1. Variation vs consistency
2. Service capacity
3. Phased approach to opening up/management of interfaces
4. Impacts across multiple pathways – homeless/asylum seekers, maternity care etc
5. General public purchase of pulse oximeters but not onboarded to service
6. Data collection/quality
7. Vulnerable groups – further support required
406. SLIDO - Hearing from our audience
Sophie Bulmer
Network Development Lead , UCLP
Participate on
On your phone: slido app
On your web browser: slido.com
Part 2 event code: #94091
417. Next steps to enabling implementation
Fiona Howgego
Cell Director, COVID Remote Monitoring, NHS London
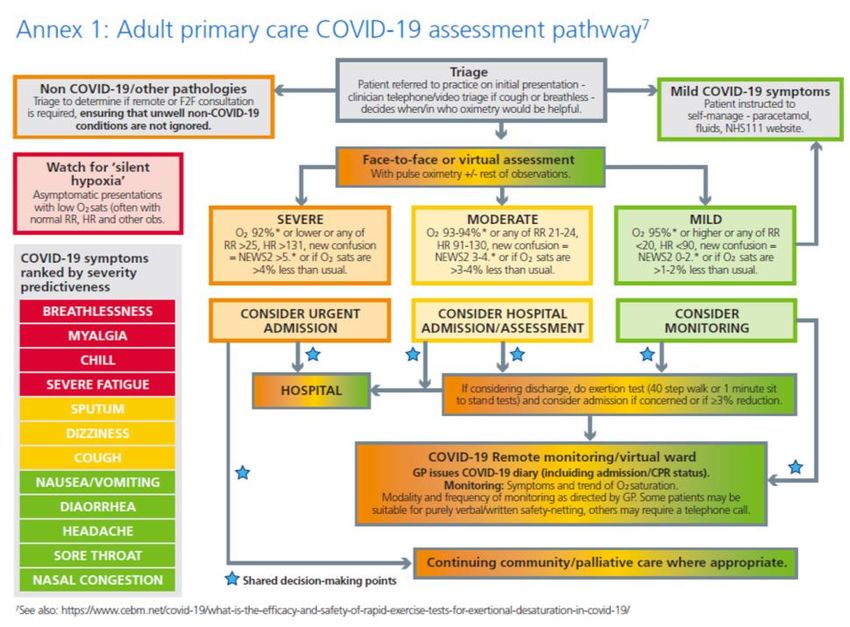
42NHS London COVID Remote Monitoring Cell
– enabling implementation
Programme Board
Forum designed to share and understand challenges and key achievements across the region and provide senior
decision making and governance to the programme
ICS Implementation Indicators
A tool to aid discussion between ICS area leads and ICS Clinical and Operational leads to understand any variation in
provision and how this can be improved locally
Interactive Map
Provides an interactive summary of the COVID Oximetry@home service provision in place across each ICS. This will
increase visibility of local services in place to enhance interoperability across service providers
London specific Futures site
A repository to share and store key London specific documents and useful information for COVID Oximetry@home and
COVID Virtual Wards, sits alongside national Futures site
Data Automation
To lessen the data burden on the systems, the team are working closely with ICS leads and NHS Digital colleagues to
automate the various data asks for this programme
London and Local education and training events
To strengthen knowledge of key leadership roles and local integration we are working with key partners to co-design and
deliver two Regional webinars. These will be followed by local system-level webinars supported by local GP training
hubs and AHSN colleagues – dates to be agreed.
43 |Live issues being explored by London team
COVID specialist
advice line
Out of area
Maternity
support and
indicators
mapping
Clinical engineer
input
Mental health
inpatient Homeless
interaction with access to
pathway pathway
Data
streamlining
44 |Key next steps in enabling implementation
1. Strengthening Implementation across London to reduce variation in outcomes:
• We ask that each ICS to work closely with their assigned area lead to understand how the region can support to
minimise variation in service provision for each COVID Remote Monitoring pathway.
• Working with your ICS training hubs and AHSNs arrange local webinars to strengthen local implementation with
key local providers
2. Data collection to capture our collective achievements:
There are currently two manual data requests the system are required to submit. The regional team continue to work
on setting up automated reporting mechanisms to lessen the data burden on the systems.
1. Number of patients on each COVID Remote Monitoring pathway
• Submission to the regional team twice weekly; Tuesday and Friday by 5pm
• Revised template circulated 26 January 2021
• All submissions sent to: england.londoncovidoximetry@nhs.net
2. Management Information report to NHS Digital
• Weekly data submission sent directly to NHS Digital team
• London organisations are not required to complete the Service Evaluation section of the circulated template
and are asked only to report, via SDCS, on:
o Number of oximeters available
o Number of oximeters sent out for use
o Number of oximeters returned and able to be re-used
45 |8. Audience Q&A
Facilitated by Catherine Dale
Programme Director for Patient Safety and Experience at the Health Innovation Network
Academic Health Science Network (AHSN) for south London
46Supporting local implementation – immediate next
steps
Future NHS site: London Covid Oximetry @home and Covid Virtual Ward resources
A repository for information for those in the London region to share documents to support
development and running of Covid Oximetry @home and Covid Virtual Ward services.
https://future.nhs.uk/NEWS2CN/view?objectId=24446896
Local system Date and time Key contact
NCL 1-2 pm 3rd February Michael Fox
mfox@nhs.net
SWL 12-1pm 11th February Catherine Dale
catherine.dale3@nhs.net
*SEL 5.30pm Mondays and Thursdays
NWL TBC Kenny Ajay
kenny.ajayi@imperialcollegehealthpartners.com
NEL TBC – wc 8 February Sule Kangulec sule.kangulec@communitymatters.co.uk
*Mobilisation meetings – some of these will be extended as learning sessions, beginning this Thursday 28th January
47 |Appendix 1: Speaker Biographies
Speaker Biographies
Name Current role and organisation Bio
Dr Jo Sauvage London Clinical Lead for COVID Jo was elected to the role of Chair of North Central London Clinical Commissioning Group (CCG) in February 2020. She is also
(co-chair) Oximetry @home and remote clinical lead for the emerging Integrated Care System in North Central London working, a role where she seeks to support closer
monitoring. working between partner organisations including the NHS, Local Authority & voluntary sector, to improve the health & wellbeing of
our residents.
Clinical Lead for the Sustainability Within Islington she is Co-Chair of the Fairer Together borough Partnership championing collaborative working at borough level.
Network, supporting London’s For London, She is a London region representative on the board of NHS Clinical Commissioners and the commissioner member of
Integrated Care Systems the London People Board. She is a clinical member of the London Health Board, chaired by the London Mayor.
contribute to a Greener NHS. She has worked as a GP in Old Street EC1 for over 21 years.
Dr Sarah Elkin Consultant in Respiratory and Dr Sarah Elkin is Joint-Clinical Director of the London region Respiratory network - NHSE/I. She is a Consultant in Respiratory
(co-chair) General Medicine, Imperial medicine at Imperial college NHS trust where she is Clinical Director for Integrated care. She works both in the acute trust
College Hospital managing respiratory & medical emergencies and in the community leading a large integrated respiratory team. She works closely
Clinical Co-Director London with GPs in NW London, as chair of the clinical reference group, running and developing respiratory pathways from early diagnosis
Respiratory Clinical Network, to advanced care, running community based clinics, advice and guidance and supporting the pulmonary rehabilitation, oxygen and
NHSE/I supported discharge programs.
Dr Kuldhir General Practitioner and NWL Frontline GP for over 22 years – interested in aligning the “real world” from the GP practice level to population level – through the
Johal Remote monitoring COVID19 – use of enabling technologies with patient care at the centre. Has been involved in clinical commissioning for over 10 years. Clinical
Primary care clinical lead. Lead for IT locally and contribute to IT programmes locally, NWL and regional level. Previously first regional lead for 111 – London
Governing Body Member of NHS – when introduced and currently work closely with the London Ambulance Service (Chair LAS/CCG CQRG). Previously a GP
Hillingdon CCG trainer with the London Deanery and also hold a Masters in Health Informatics (awarded with Distinction) from City University.
Dr Stephanie GP Partner in Hackney, East Stephanie is the clinical lead for system-wide transformational programme focusing on integrated care and the broader
Coughlin London. determinants of health in City & Hackney
Local COVID 19 clinical and the During the pandemic she has set up national networks for primary care teams across the country enabling quick and easy access
NEL lead for COVID to essential support and resources. Stephanie is also Clinical Lead for Innovation at the RCGP. In this role she supports GP
Oximetry@home. practice teams with the implementation of new ways of working and digital solutions that can reduce workload and improve patient
care. Person-centred care, continuity of care, AI, digital technologies, and genomics have been some of the key programmes of
work.
Dr Katie GP, Islington. Katie has been a GP in Islington for 22 years. She is a strong advocate of patient empowerment, ensuring that people are
Coleman NCL Clinical Lead for Primary supported to identify what is important to them when engaging with health and care providers.
Care Development, During the course of the pandemic she has supported the NCL system in ensuring patients with Covid-19 experience integrated
Personalisation, Long Term care through multidisciplinary working.
Conditions and Enhanced Health
in Care Homes.Speaker Biographies – continued
Name Current role and organisation Bio
Dr Irem Patel Consultant Respiratory Dr Irem Patel is Joint Clinical Director of the NHSE London Respiratory Network. She is an integrated Respiratory Consultant and
Physician, Integrated Care; Joint Director of Clinical Strategy at King's Health Partners. She heads a multidisciplinary specialist team spanning hospital and
Clinical Co-Director NHSE community delivering integrated respiratory care in South East London and leads on running and developing respiratory pathways
London Respiratory Clinical for airways disease, community spirometry, oxygen therapy, tobacco dependence and pulmonary rehabilitation. She works
Network; closely with GP colleagues as respiratory clinical lead for SEL ICS. She is also a clinical advisor to the British Lung Foundation
Joint Director of Clinical Strategy, and Associate Editor of NPJ-Primary Care Respiratory Journal.
King’s Health Partners
Fiona Programme Director for London Fiona has been supporting the London region in their COVID response for the last 12 months– leading on ventilator provision for
Howgego COVID Remote Monitoring Cell wave 1, the UEC restoration programme and now the COVID remote monitoring work for London.
She is an expert in health service turnaround, with twenty years of experience helping stabilise organisations in distress;
identifying then designing, implementing and monitoring a range of recovery programmes. Her extensive NHS experience is built
from work in both commissioners and providers, alongside significant consulting experience. She has a masters in medical
anthropology and her substantive role is as a director within a national team at NHSEI supporting the most challenged
organisations within the NHS.
Catherine Dale Programme Director for Patient Catherine has over twenty years’ experience in the NHS in London, including more than fifteen years in quality improvement and
Safety and Experience at the transformation roles. Catherine co-leads the National Patient Safety Improvement programme on Managing Deterioration.
Health Innovation Network the Catherine has a Masters in Business Psychology and is an expert on co-designing improvements with patients and applying
Academic Health Science behavioural insights to healthcare.
Network for south London
Kara Renno RGN, Assistant Director NEL Kara joined the NHS in 2000 and worked as a Community Respiratory Nurse Specialist in Camden (2001-2008) and Tower
Healthcare Consulting Hamlets (2008-2013). She joined NEL CSU in Nov 2013 as a Healthcare Consultant, leading teams to provide consultancy and
transformational change expertise within the NHS across a variety of Regional and ICS-level programmes. Since March 2019,
NHS London Respiratory Kara has been working within NHS London Respiratory Strategic Clinical Network providing Respiratory SME and programme
Strategic Clinical network management expertise to progress the ambitions of the Long Term Plan, and more recently the Response to COVID 19. She is
now working alongside the COVID Remote Monitoring Cell supporting the implementation of the 4 key actions through her
Respiratory Clinical Network role.Appendix 2: COVID Oximetry@home leads across London
Working with our ICS Leads
COVID Ox@Home and Virtual Ward
COVID Ox@home System Leads Virtual Ward System Leads
PMO Area and AHSN Leads
ICS
PMO Area Lead AHSN Lead Clinical Lead Operational Lead/s Clinical Lead/s Operational Lead/s
NWL Isabel del Arbol Stewart Kenny Ajayi-ICHP Kuldhir Johal June Farquharson TBC TBC
isabel.delarbolstewart@nhs kenny.ajayi@imperialcollegehea kuldhirjohal@nhs.net
.net lthpartners.com Ashley Plummer SRO
ashley.plummer@nhs.net Jane Wheeler
jane.wheeler2@nhs.net
NCL Chris Larkin John Illingworth- UCLP Katie Coleman (Katie is in Meena Mahil Melissa Heightman Meena Mahil
chris.larkin2@nhs.net john.illingworth@uclpartners.co post for now but NCL is m.mahil@nhs.net melissa.heightman1@nhs.n m.mahil@nhs.net
m recruiting Clinical Lead) et
Support: katie.coleman@nhs.net Shafeeq Tejani Shafeeq Tejani
Sarah Sandiford Valentina Karas- UCLP S.Tejani@nhs.net S.Tejani@nhs.net
s.sandiford@nhs.net Valentina.Karas@uclpartners.co
m SRO
Sarah Mcdonnell Davies
sarah.mcdonnell1@nhs.net
NEL Chris Larkin John Illingworth- UCLP Steph Coughlin Selina Douglas WEL clinical leads: Selina Douglas
chris.larkin2@nhs.net john.illingworth@uclpartners.co stephaniecoughlin@nhs.ne selina.douglas@nhs.net Waleed Mohammed selina.douglas@nhs.net
m t Simon Green
Support: Paul Calaminus Clare Dow Paul Calaminus
Sarah Sandiford Valentina Karas- UCLP paul.calaminus@nhs.net paul.calaminus@nhs.net
s.sandiford@nhs.net Valentina.Karas@uclpartners.co BHR clinical lead:
m Teddy Abrokwa Jagan John jagan.john- Teddy Abrokwa
teddy.abrokwa@nhs.net barkdagccg@nhs.net teddy.abrokwa@nhs.net
SWL Matt Dodwell Catherine Dale- HIN Rachel Tunbridge Andrew McMylor Yogini Raste Alex Lang
m.dodwell@nhs.net catherine.dale3@nhs.net rachel.tunbridge@nhs.net Andrew.mcmylor@swlondon. yoginiraste@nhs.net Alex.Lang@swlondon.nhs.u
nhs.uk k
SEL Matt Dodwell Catherine Dale- HIN Jonty Heaversedge Holly Eden Irem Patel David Reith
m.dodwell@nhs.net catherine.dale3@nhs.net Jonty.heaversedge@nhs.n Holly.eden@nhs.net irempatel@nhs.net David.reith@nhs.net
et
Area Grace Coombs
52 | Leads grace.coombs@nhs.net
SupportNHS London COVID Remote Monitoring Cell – key roles
Name Programme Role
Helen Pettersen SRO
Fiona Howgego Programme Director
Emma Jopling Lead Programme Manager
Isabel del Arbol Stewart Area Lead: NWL
Workstream Lead: Equipment
Workstream Lead: Digital
Matt Dodwell Area Lead: SWL and SEL
Chris Larkin Area Lead: NCL and NEL
Sarah Sandiford Area Lead Support: NCL and NEL
Joe Fraser Workstream Lead: Data
Workstream Lead: Integrated Pathways
Kara Renno Workstream Lead: Respiratory Clinical Network and training
Tyler Smith Project Support: PMO
Grace Coombs Project Support: Area leads
Rob Ballantine Workstream Lead: interactive map and 111/IUC/999 onboarding to pathway
Luca Cicalese Data analyst
53 |You can also read