Children with cancer in Europe: challenges and perspectives
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ottobre-Dicembre 2013 • Vol. 43 • N. 172 • Pp. 233-237 ONCologia pediatrica
Children with cancer in Europe: challenges and
perspectives
Kathy Pritchard-Jones
University College London, Institute of Child Health, 30 Guilford Street, London, UK
Summary
Cancer in children and adolescents is rare and biologically different from cancer in adults. In high-income countries, survival from childhood cancer has
reached 80% through a continuous focus on the integration of clinical research into front-line care for nearly all children affected by malignant disease.
Further improvements must entail new biology-driven approaches since optimization of conventional treatments has in many cases reached its limits. This
will be achieved by the access to drugs thar are less toxic and more targeted than those currently used and through international collaborative research,
since rare cancers are being subdivided into increased smaller subgroups. Finally the long-term effect of anticancer treatment on quality of life must also
be taken into account because more than one in 1000 adults in high-income countries are thought to be survivors of cancer in childhood or adolescence.
Riassunto
I tumori del bambino e adolescente sono malattie relativamente rare e biologicamente differenti dai tumori dell’età adulta. Nei paesi con risorse economiche
elevate, la sopravvivenza dei tumori infantili ha raggiunto oggi l’80%. Ciò si è realizzato attraverso l’arruolamento dei pazienti in protocolli clinici come
standard di cura di prima linea. Il progressivo miglioramento è probabile possa essere ottenuto con approcci innovativi basati sulle conoscenze biologiche
e molecolari, poiché l’ottimizzazione dei trattamenti con i farmaci convenzionali ha raggiunto ormai il massimo delle sue potenzialità. L’accesso a farmaci
meno tossici e diretti contro target molecolari più specifici dei chemioterapici convenzionali e la collaborazione internazionale per far fronte all’identificazio-
ne e trattamento di gruppi di pazienti sempre più piccoli, sono due degli aspetti da cui dipenderà l’ulteriore miglioramento della sopravvivenza dei pazienti.
Infine l’impatto a lungo termine dei trattamenti chemio-radioterapici sulla qualità di vita è divenuto sempre più rilevante, considerando che si stima che
circa 1 adulto su 1000 sia stato affetto da tumore in età pediatrica.
Key words: childhood cancer, clinical research, SIOP Europe
Parole chiave: cancro infantile, ricerca clinica, SIOP Europa
Introduction tion is incorporated, whereby tumours are risk-stratified according
to their molecular subtype, then each childhood cancer category be-
Cancer in children is a significant health challenge for our society,
comes individually rarer still. Hence, it is essential that clinical trials
even though it is relatively rare, affecting about 1 in 600 children
specific to the cancers that affect children and adolescents are con-
before their 15th birthday, and comprises only 1% of all cancers in
ducted in a timely and efficient manner if we are to continue to make
high income countries (Pritchard-Jones et al., 2013). In this setting,
progress at a European level. These inevitably require multi-national
overall survival has increased to approximately 80% at 5 years. This
co-operation due to the small numbers of cases in each country.
means that current estimates of the proportion of the young adult
population (aged 18-40 years) who has survived childhood cancer
stands at 1 in a thousand. This proportion is set to continue to rise Since the beginning of the new millenium, the rate of improvement
rapidly. in overall survival rates has slowed for most childhood cancers (Fig.
3). It is becoming clear that we have reached the limits of optimising
Despite these good overall survival rates, there remain subgroups currently available treatments through dose intensification or rapid
of childhood cancers with much worse outcomes, such as high risk scheduling, and that new approaches are needed (Pritchard-Jones
neuroblastoma, high grade gliomas and metastatic sarcomas. Also, et al., 2013). These can include introduction of biomarkers to im-
for those children who are cured with current treatments, many will prove the accuracy of risk-stratification or response assessment,
have received unpleasant, prolonged therapy that disrupts schooling and use of new, molecularly targeted drugs that have mostly been
and family life and may cause permanent side effects that compro- developed for adult cancers (Vassal et al., 2013). Indeed, there are
mise normal functioning in adult life. Hence, clinical research that now more than 400 biologically targeted drugs available for clinical
aims to improve survival rates and quality of survival for the total use in adult cancers, but few of these have yet been tested for their
population afflicted by childhood cancer remains an important goal safety or efficacy in childhood cancers, even though there may be a
for our society. strong biological rationale if the same molecular target is disrupted
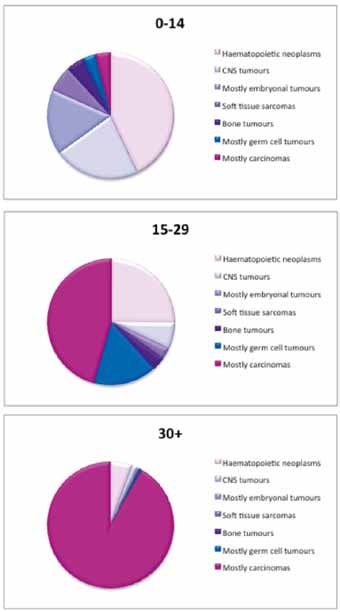
The spectrum of the mainly embryonal cancer types seen in chil- in cancer in both age groups.
dren is very different from the predominantly epithelial types seen
in adults and from the spectrum of cancers seen in adolescents and The other major challenge is the inequality in survival rates seen
young adults (Fig. 1). However, the number of major subtypes is just between different geographical regions of Europe. The differences
as complex as in adult cancer (Fig. 2). Once biological risk stratifica- measured by comparative cancer registry research in the 1990s
233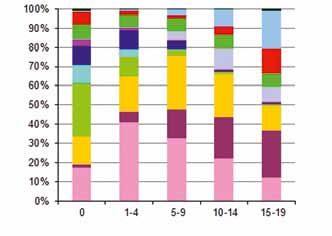
K. Pritchard-Jones
Age groups (years)
Figure 2.
Proportion of the 12 main tumor groups in children and adolescents in Eu-
rope (with permission of Lancet Oncology, Pritchard-Jones et al., 2013).
Mortality
Years
Figure 3.
Child cancer mortality (per million person-years) (aged 0-14 years) in
Figure 1. three European countries (Ireland, Netherlands and UK (combined) (blue
Cancer incidence by type in three age groups (with permission of Lan- line) and the USA (red line) (modified from Lancet Oncology, Pritchard-
cet Oncology, Pritchard-Jones and Sullivan, 2013). Jones et al., 2013).
showed an approximately 15-20% difference in survival rates, ENCCA was created at relatively short notice in 2009 by the collabora-
even though the rate of improvement was similar in Eastern and tive efforts of a relatively limited number of specialist centres active in
Western European regions (Fig. 4). Whilst there is recent evidence treatment and clinical research into childhood and/or adolescent can-
that this difference is decreasing in the 2000s (Gatta et al, 2013), cers. However, it was always planned from the very beginning that EN-
it must be remembered that this improvement is only known with CCA would unite the multinational clinical trial groups and national child-
any confidence in those countries with cancer registration in place hood cancer organisations into the building blocks of a future «virtual
at a population level. There may be persisting outcome differences institute» of paediatric haemato-oncology research, that would involve
in countries without specific cancer control resources in place. For every major treatment and research centre across Europe.
these reasons, outcomes research must also focus on the broader
aspects of health services delivery and models of care. To summarise the need in numbers, every year there are 15,000
new cases of cancer in children and adolescents in Europe. Whilst
80% can be cured with current multidisciplinary treatments, 3,000
The Europe perspective will die. There are more than 60 different disease types histologi-
To address the challenges faced by children and young people with cally and clinically, from newborns to teenagers. There are hundreds
cancer at a European level, the ENCCA project (European Network for of subtypes when biomarkers are considered. These children and
Cancer research in Children and Adolescents) was developed with fund- young people receive their diagnosis and treatment at one of about
ing from the 7th framework programme of the European Commission 250 public specialised treatment centres in the EU, each seeing only
(www.encca.eu). Due to the requirements of European grant funding, a handful of each individual cancer type each year.
234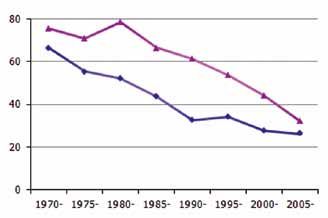
Childhood cancer in Europe: problems and perspective
agreeing common goals and priorities and then working in partner-
ship to deliver these in a timely fashion. Everyone will benefit from
such sharing of resources – most importantly the patients who will
see the fruits of the research being applied in clinical care more
quickly and with greater confidence from the robust sample size
involved in each trial question.
Mortality
Through the ENCCA project and its workstreams, many high-level
research teams dedicated to paediatric tumour biology have forged
stronger links and are sharing tissue samples and genomic analy-
sis data. A series of ‘biology-driven drug development workshops’
have been held to bring together experts in drug development, the
relevant tumour biology and clinical trial groups and representatives
Years
of parents and regulators (http://www.ema.europa.eu/docs/en_GB/
document_library/Regulatory_and_procedural_guideline/2013/02/
Figure 4. WC500139182.pdf;http://www.ema.europa.eu/docs/en_GB/docu-
Child cancer mortality (per million person-years) (aged 0-14 years) in ment_library/Regulatory_and_procedural_guideline/2013/02/
former socialist economies (red line) compared with other European WC500139183.pdf; Perotti et al., 2013).
countries (blue line) (modified from Lancet Oncology, Pritchard-Jones Here the discussion has been about understanding the driver bio-
et al., 2013). logical targets or pathways for each tumour type or subtype and
prioritising the drugs for testing in early phase trials in high risk
tumours. The ultimate output of each workshop is a proposal for a
The challenges of clinical research model ‘Paediatric investigation plan’ that can stimulate more appro-
Since the 1970’s, there have been networks conducting clinical tri- priate drug development plans that match the clinical unmet needs
als across many institutions, all working to a common protocol with of children with these forms of cancer.
standards for diagnosis, pathology review, response assessment
and event free and overall survival. Many of these clinical trial groups Working with the clinical trial groups and the innovative therapies for
started as national entities, often conducting single arm studies that children with cancer consortium (www.itcc-consortium.org), several
laid the evidence base for the standard of care. However, soon either workpackages within ENCCA are prioritising this biology-driven ap-
the numbers required for statistically meaningful trial design, or the proach to new drug development, aiming to open at least one trial
of a suitably targeted new agent. The resources to run the trial do
intellectual rigor and pleasure of working with like-minded individu-
not come from ENCCA, rather it provides the catalyst that has al-
als with a common understanding and passion for improvement in
lowed groups to bid successfully for further funding or to present a
outcomes, led to most clinical trial groups working across national
united front to an industry partner to make the drug and sometimes
boundaries. By the late 1990s, approximately 40% of patients were
sponsorship available.
treated within trials (phase I to III), a further 40% were treated ac-
cording to recognised standards within prospective studies, but less
This partnership approach to improving outcomes for children and
than 5% were enrolled in pharma-sponsored trials of new drugs.
young people with cancer across Europe requires us all to think in a
However, since the introduction of the well-intentioned EU Clinical
different way to the traditional institutional and national loyalties we
Trials Directive (EU-CTD), the proportion of children treated in clini-
were brought up with. We need to agree on the best structures and
cal trials or prospective studies has dropped dramatically. This is not relationships in order to build a sustainable, safe and high quality
because the trials are no longer needed, but rather because the time network for clinical care and research that benefits all of the chil-
taken and expense incurred to open a trial has increased massively dren and young people with cancer in Europe. This is the only way
due to new bureacracy and need for formal sponsorship with insu- we can truly tackle the unacceptable variation we find now in ac-
rance (Pritchard-Jones, 2008). cess to ‘state of the art’ treatment and best outcomes. SIOP Europe
has therefore created a ‘European Clinical Research Council’ (ECRC)
How to make progress to be the common, harmonised voice for advocacy and lobbying at
the European level on paediatric and adolescent cancer clinical and
The challenge for childhood cancer in the current millenium must research activities. The ECRC comprises representatives of each of
be to gain a better understanding of the biological basis of the dif- the National Paediatric Haemato-Oncology Societies (NAPHOS) and
ferent childhood cancers and to work in partnership with the phar- of the multi-national clinical trial groups.
maceutical industry to obtain better access to molecularly targeted
drugs that may offer chances for improved or safer cure (Vassal et Many EU member states have established NAPHOS that have links
al., 2013, Pritchard-Jones, 2008). This will require extensive trans- to health policy makers and have introduced quality standards
lational research, with comprehensive tissue banking from current for specialist centres to care for children with cancer and for the
patients linked to their clinical diagnosis, treatment and outcome training of the staff who work there. In the UK, for example, there
data. Only in this way can biomarkers for risk prediction, response are 17 specialist centres designated to provide services for a total
assessment and signposting to existing therapies be developed and population of about 60 million. Quality standards were published in
assessed prior to routine use in standard care. 2005 (http://www.nice.org.uk/nicemedia/pdf/C&YPManual.pdf) and
How do we achieve all of this with the limited resources available to centres have been externally quality assessed since 2012. However,
us? The answer has to lie in much wider and stronger collaboration, not all countries in Europe have yet achieved this, and the degree
235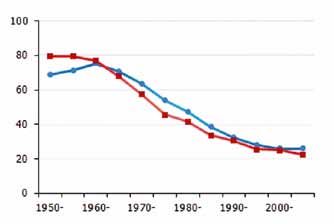
K. Pritchard-Jones
Table I.
The 7 priority areas for a Virtual Institute of Paediatric Haematology Oncology to make progress in:
Introducing safe and effective innovative treatments (new drugs, new technologies) in multidisciplinary standard care.
Driving therapeutic decision by improved risk classification and use of molecular characteristics (tumour, patient) – personalized medicine
Increasing knowledge on tumour biology and speeding up translation to the patients
Increasing equal access across Europe to standard care and clinical research
Addressing the specific needs of adolescents and young adults jointly with adult oncology
Addressing long-term toxicity and cancer treatment consequences including the genetic background/risk – quality of survivorship
Understanding the causes of paediatric cancers and setting prevention where possible
Table II.
Challenges and proposed solutions to make progress in childhood cancers.
Summary of Challenges Proposed Solutions
Increasing complexity of risk stratification We have to work together across Europe to design and implement clinical
trials – the European Clinical Trials Council, co-ordinated by SIOPE
– single countries only have a handful of cases in each category e.g. very
high risk Wilms: 5 pts and 1-2 relapses/yr in Italy
Optimisation of intensive use of present treatments has reached its limits European virtual institute for translational research in childhood and
adolescent cancer to promote a biology-driven approach
- Need for biology-driven approach to risk stratification and response
assessment in front line treatment
Unaffordable & unnecessarily complex regulatory bureaucracy for Professionals, parents and patients need to establish a “Therapeutic
international investigator-led clinical trials Alliance” with industry & regulators
- Need to influence revision of EU CTD to a Regulation
Insufficient commercial interest from Phama Professionals, parents and patients need to establish a “Therapeutic
Alliance” with industry & regulators
of development of standards and quality assurance remains vari- learning and improving through clinical research and well designed
able. Hence, an important project has been launched through SIOP prospective studies and audit.
Europe, the European Standards of Care for children with cancer
(http://www.siope.eu/european-research-and-standards/stand-
ards-of-care-in-paediatric-oncology/). This is now being dissemi- Conclusions
nated through a partnership with EPAAC (European Partnership for SIOP Europe and ENCCA are currently working on creating a sus-
Action Against Cancer). It should be noted that a key component of tainable solution to the challenges we face together in continuing
the expected standard for any childhood cancer treatment centre is to make improvements for children and young people with cancer
the ability to offer patients participation in clinical trials and to con- in Europe. This group has identified 7 priority areas that we need
tribute clinical data to cancer registration processes. This is based to focus on (Tab. I). Whilst the challenges are immense, solutions
on the clear observation that patients who are treated within clinical have been identified (Tab. II). We now need to coordinate our ef-
trials or at institutions that are active in research have better out- forts in each country so that we can work together most effectively
comes (Stiller et al., 2012). The life threatening diseases that make to ensure we are ready to win the opportunities that we expect to
up childhood cancer and the serious side effects of the necessary be available in Horizon 2020 and other funding sources in the near
treatments mandate that the clinical teams should be constantly future.
236Childhood cancer in Europe: problems and perspective
Box di orientamento
Che cosa si sapeva prima
I tumori pediatrici, rappresentando solo l’1-2% di tutti i casi registrati di tumore, sono un evento relativamente raro. Nonostante ciò, queste malattie
hanno un grande impatto sui pazienti, sulle loro famiglie e sulla società in generale, e costituiscono la seconda causa di morte in età infantile dopo
traumi ed avvelenamenti. La diminuzione del tasso di mortalità dei tumori pediatrici (in particolare leucemie, malattia di Hodgkin e sarcomi) è stato
uno dei successi più importanti della medicina negli ultimi 30 anni. Tale risultato è stato ottenuto principalmente grazie all’arruolamento dei pazienti
in protocolli clinici di diagnosi e trattamento, come standard di cura, al miglioramento delle terapie di supporto e ai risultati del trapianto di cellule
staminali emopoietiche.
Cosa sappiamo adesso
Nei paesi con elevate risorse economiche, il trend di miglioramento ha raggiunto una stabilità ed è difficile prevedere che un ulteriore successo pos-
sa avvenire con l’ottimizzazione dei chemioterapici fino ad ora utilizzati. La genomica sta progressivamente modificando il paradigma di cura verso
l’utilizzo di farmaci diretti contro le alterazioni genetiche dei diversi tipi di tumore. L’aspettativa è quella di poter disporre di farmaci meno tossici e
più efficaci, perché diretti principalmente contro la cellula tumorale. Un ulteriore aspetto di novità è costituito dai “guariti” o “lungo sopravviventi” (si
stima che circa 1 adulto su 1000 sia stato affetto da tumore in età pediatrica) e dalla necessità di sviluppare risposte a nuove domande di salute, di
inserimento sociale e di qualità di vita.
Quali ricadute sulla pratica clinica
Il successo terapeutico dei tumori in età pediatrica rende ancora più necessario il diretto coinvolgimento del Pediatra e Medico di famiglia nel percorso
di diagnosi e cura per poter divenire senza soluzione di continuità il referente diretto di nuovi bisogni di salute che il bambino/adolescente “guarito”
esprimerà a conclusione del suo percorso terapeutico.
References Pritchard-Jones K, Sullivan R. Children with cancer: driving the global agenda.
Lancet Oncol 2013;14:189-91.
Dixon-Woods M, Naafs-Wilstra M, Valsecchi MG. Improving recruitment to clini-
cal trials for cancer in childhood. Lancet Oncology 2008;9:392-9. Stiller C, Kroll M, Pritchard-Jones K. Population survival from childhood cancer
in Britain during 1978-2005 by eras of entry to clinical trials. Annals Oncology
Gatta G, Botta L, Rossi S et al. The EUROCARE Working Group. Childhood can- 2012;23:2464-9.
cer survival in Europe 1999-2007: results of EUROCARE-5 - a population-based
study. Lancet Oncol 2013;Dec5 (Epub ahead of print). Vassal G, Zwaan C, Ashley D, et al. New drugs for children and adolescents with
cancer: the need for novel development pathways. Lancet Oncol 2013;14:117-
Perotti D, Hohenstein P, Bongarzone I, et al. Is Wilms Tumor a Candidate Neo- 24.
plasia for Treatment with WNT/β-Catenin Pathway Modulators? A Report from
the Renal Tumors Biology-Driven Drug Development Workshop. Mol Cancer Ther
2013;12:2619-27. http://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and_
Pritchard-Jones K, SIOP Europe. Clinical Trials for children with cancer in Europe procedural_guideline/2013/02/WC500139182.pdf
– still a long way from harmonization: a report from SIOP Europe. Eur. J Cancer http://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and_
2008;44:2106-11. procedural_guideline/2013/02/WC500139183.pdf
Pritchard-Jones K, Dixon-Woods M, Naafs-Wilstra M, et al. Improving recruit- http://www.siope.eu/european-research-and-standards/standards-of-care-in-
ment to clinical trials for cancer in childhood. Lancet Oncol 2008;9:392-9. paediatric-oncology/
Pritchard-Jones K, Pieters R, Reaman G, et al. Sustaining innovation and im- http://www.nice.org.uk/nicemedia/pdf/C&YPManual.pdf.
provement in the treatment of childhood cancer: lessons from high-income
countries. Lancet Oncol 2013;14:95-103.
Corrispondenza
Kathy Pritchard-Jones, University College London, Institute of Child Health, 30 Guilsford Street, London, UK. E-mail: k.pritchard-jones@ich.ucl.ac.uk
237You can also read